Chronic Childhood Inflammatory Arthritis
ILAR Classification
Critical Must-Knows
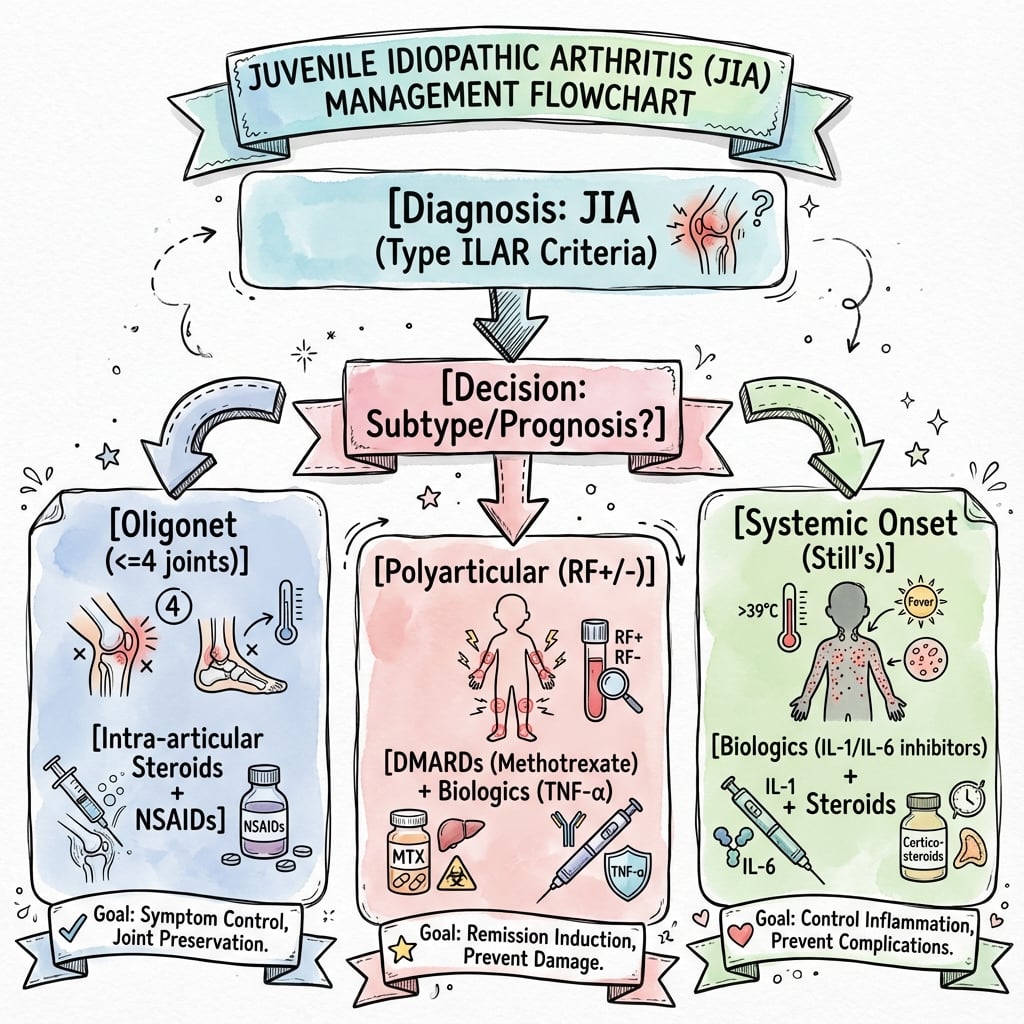
- Oligoarticular: Most common type. 4 or fewer joints.
- Polyarticular: 5 or more joints. More severe.
- Systemic (Still's): Fever, rash, serositis.
- Growth Disturbance: Initial overgrowth, then undergrowth.
- Biologics: Revolutionized medical treatment.
Clinical Pearls
- "Oligoarticular most common
- "Knee overgrowth then undergrowth
- "Biologics are first-line
- "Surgery after medical optimization
Growth Disturbance
JIA causes characteristic growth disturbance in the affected limb.
- Initial: Inflammation → hyperemia → physeal overgrowth (limb lengthening).
- Later: Physeal damage → premature closure → undergrowth (limb shortening).
- Net Effect: Often leg length discrepancy.
- Knee most affected: Valgus deformity common.
JIA Subtypes
| Type | Joints | Features |
|---|---|---|
| ≤4 | Most common, uveitis risk | |
| ≥5 | Symmetric, moderate | |
| ≥5 | Similar to adult RA | |
| Variable | Fever, rash, serositis |
At a Glance Table
| Aspect | Details |
|---|---|
| Definition | Chronic arthritis in children under 16, lasting over 6 weeks |
| Most Common Subtype | Oligoarticular (4 or fewer joints) |
| Key Feature | Joint inflammation with growth disturbance |
| Growth Pattern | Initial overgrowth (hyperemia) then undergrowth (physeal damage) |
| Treatment Revolution | Biologics (TNF inhibitors, IL-1/IL-6 blockers) |
| Surgery | Reserved for refractory contractures or end-stage joints |
JIA TJIA Types
| O | Oligoarticular ≤4 joints, most common |
| P | Polyarticular ≥5 joints |
| S | Systemic Fever, rash |
| E | Enthesitis-Related HLA-B27 associated |
| P | Psoriatic Psoriasis |
| O | Oligoarticular ≤4 joints, most common | E | Enthesitis-Related HLA-B27 associated |
| P | Polyarticular ≥5 joints | P | Psoriatic Psoriasis |
| S | Systemic Fever, rash |
Hook:OPSEP - Oligo, Poly, Systemic, Enthesitis, Psoriatic.
OUGrowth Changes
| O | Overgrowth Early hyperemia |
| U | Undergrowth Late physeal damage |
| O | Overgrowth Early hyperemia |
| U | Undergrowth Late physeal damage |
Hook:OU - Overgrowth first, Undergrowth later.
OAFYUveitis Risk Factors
| O | Oligoarticular Highest risk subtype |
| A | ANA Positive Antinuclear antibody |
| F | Female Girls more affected |
| Y | Young Onset Earlier onset higher risk |
| O | Oligoarticular Highest risk subtype | F | Female Girls more affected |
| A | ANA Positive Antinuclear antibody | Y | Young Onset Earlier onset higher risk |
Hook:OAFY - Oligo, ANA+, Female, Young.
Overview/Epidemiology
Juvenile Idiopathic Arthritis (JIA) is chronic inflammatory arthritis in children.
- Definition: Arthritis in children under 16, lasting greater than 6 weeks, with no other cause.
- Incidence: 1-4 per 10,000 children.
- Classification: ILAR classification (7 subtypes).
Pathophysiology and Mechanism
Pathophysiology of Joint Damage
- Chronic synovitis leads to pannus formation.
- Pannus erodes cartilage and subchondral bone.
- Joint destruction progresses if inflammation uncontrolled.
Growth Disturbance Mechanism
- Early Phase: Chronic inflammation causes hyperemia around physis.
- Hyperemia increases blood flow → physeal overgrowth → limb lengthening.
- Late Phase: Prolonged inflammation damages physeal chondrocytes.
- Physeal damage → premature closure → limb shortening.
- Net Effect: Often initial lengthening followed by shortening.
Common Joint Involvement
- Knee: Most commonly affected. Valgus deformity, flexion contracture.
- Hip: Flexion-adduction contracture, coxa valga.
- Cervical Spine: C1-C2 instability in severe polyarticular JIA.
Classification Systems
ILAR Classification (International League of Associations for Rheumatology)
- Oligoarticular: ≤4 joints in first 6 months. Most common (50%). Uveitis risk.
- Polyarticular RF-negative: ≥5 joints, RF negative. Moderate severity.
- Polyarticular RF-positive: ≥5 joints, RF positive. Similar to adult RA. Worst prognosis.
- Systemic (Still's Disease): Quotidian fever, salmon-pink rash, hepatosplenomegaly. IL-1/IL-6 driven.
- Enthesitis-Related Arthritis: HLA-B27 associated. Axial involvement. Related to ankylosing spondylitis.
- Psoriatic Arthritis: Arthritis with psoriasis or dactylitis.
- Undifferentiated: Does not fit other categories.
Clinical Assessment
History:
- Joint pain, swelling, stiffness.
- Morning stiffness (improves with activity).
- Systemic symptoms (fever, rash in systemic JIA).
- Eye symptoms (uveitis - especially oligoarticular).
Physical Exam:
- Joints: Swelling, warmth, effusion, ROM limitation.
- Gait: Antalgic.
- Leg Length: Discrepancy.
- Contractures: Hip, knee flexion.
- Eyes: Refer for slit lamp (uveitis).
Investigations
Blood:
- ESR, CRP: Elevated.
- ANA: Positive in oligoarticular (uveitis risk).
- RF: Positive in RF+ polyarticular.
- HLA-B27: Enthesitis-related.
Imaging:
- X-ray: Soft tissue swelling, osteopenia, erosions (late).
- MRI: Synovitis, effusion.
Management Algorithm
Medical Management
- NSAIDs: First-line for mild disease.
- Intra-articular Steroids: For oligoarticular.
- DMARDs: Methotrexate for polyarticular.
- Biologics: TNF inhibitors (etanercept, adalimumab), IL-1/IL-6 inhibitors for systemic JIA.
- Goal: Remission, prevent joint damage.
Surgical Techniques
Soft Tissue Releases
Indications: Fixed contractures not responding to physio/splinting.
Knee:
- Posterior capsular release.
- Hamstring lengthening.
- Post-op: Aggressive physio, night splinting.
Hip:
- Iliopsoas, rectus, adductor release.
- May need open release for severe contracture.
Complications
| Complication | Context | Management |
|---|---|---|
| Uveitis | Oligoarticular, ANA+ | Regular slit lamp screening |
| Growth Disturbance | Chronic inflammation | Control disease, address LLD |
| Joint Destruction | Uncontrolled synovitis | Early biologic therapy |
| Flexion Contractures | Chronic inflammation | Physio, splinting, release |
| Cervical Instability | Severe polyarticular | Cervical spine precautions |
Postoperative Care
- Aggressive Physiotherapy: Essential to maintain gains.
- Splinting: Night splints to prevent recurrence.
- Continue Medical Therapy: Do not stop biologics/DMARDs.
- Rheumatology Co-management: Essential.
- Monitor for Recurrence: Contractures can recur.
Outcomes/Prognosis
- Biologics Era: Dramatically improved outcomes.
- Oligoarticular: Best prognosis.
- RF+ Polyarticular: Worse prognosis, similar to adult RA.
- Systemic: Variable, can be severe.
Controversies and Areas of Uncertainty
- Classification in flux: A PRINTO consensus is moving toward a biology-based system (e.g. systemic JIA, RF-positive arthritis, enthesitis/spondylitis-related, early-onset ANA-positive arthritis) that may eventually replace the descriptive ILAR categories. Exam answers should acknowledge ILAR as current standard while noting the proposed revision.
- Systemic JIA as an autoinflammatory disease: Increasingly viewed as IL-1/IL-6-driven autoinflammation rather than classic autoimmune arthritis, supporting first-line IL-1/IL-6 blockade and a possible "window of opportunity" for early biologics.
- When to start biologics: Debate between early aggressive biologic use to prevent damage versus a step-up strategy after methotrexate failure, balancing cost, access and long-term safety.
- Treatment de-escalation: Optimal timing and method of tapering biologics after sustained remission remain unresolved; flare risk on withdrawal is significant.
- Surgical timing and choice: Diminishing role of synovectomy and arthroplasty in the biologic era; uncertainty over epiphysiodesis timing for inflammation-driven leg-length discrepancy that may partially self-correct once disease is controlled.
- Macrophage activation syndrome (MAS): A life-threatening complication of systemic JIA; thresholds for diagnosis and the role of anakinra in treatment continue to evolve.
Evidence Base
- Landmark double-blind RCT: 69 children with methotrexate-refractory polyarticular JIA
- 74% responded in open-label phase; on withdrawal, disease flare in 28% (etanercept) vs 81% (placebo)
- Median time to flare over 116 days vs 28 days with placebo (less than 0.001)
- Defines the seven mutually exclusive ILAR categories used worldwide
- Arthritis onset under 16 years, persisting over 6 weeks, no other cause
- Categories: oligo (persistent/extended), poly RF-neg, poly RF-pos, systemic, ERA, psoriatic, undifferentiated
- Authoritative review of heterogeneous JIA arthritides of unknown cause
- Prognosis greatly improved by anticytokine agents for conventional-therapy-resistant disease
- Subtype-specific presentation, genetics and outcome
- Post hoc radiographic analysis of two RCTs (systemic and polyarticular-course JIA)
- Wrist/hand films scored by adapted Sharp-van der Heijde and Poznanski methods over 104 weeks
- Most patients showed no structural progression on IL-6 blockade
- Validated criteria for inactive disease, clinical remission on and off medication
- Built from 34-country Delphi survey and chart review of 437 JIA patients
- Patients reaching off-medication remission stayed disease-free longest
- 29 TKAs in 19 patients aged 20 years or younger (JIA the leading diagnosis)
- Implant survivorship 96% at 5 years and 94-95% at 10 years
- TKA volume for inflammatory arthritis has fallen with biologic therapy
- ACR recommendations on initiation and safety monitoring of JIA therapeutics
- Treatment by disease group and prognostic features rather than ILAR category alone
- Escalation to DMARDs/biologics for poor-prognosis or refractory disease
- Standard reference for ILAR classification detail
- Orthopaedic manifestations and growth disturbance
- Multidisciplinary management principles
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Leg Length Discrepancy in JIA
"10-year-old with oligoarticular JIA affecting the left knee. 3cm left leg lengthening noted."
This is characteristic **growth disturbance in JIA**. The chronic inflammation causes **hyperemia and physeal overgrowth** initially, leading to leg lengthening. If it continues, the physis may be damaged and undergo premature closure, causing eventual shortening. Management: Ensure **medical management is optimized** (DMARDs/biologics) to control inflammation. For the leg length discrepancy, use a **shoe raise** for now. If significant and ongoing, consider **epiphysiodesis** of the longer leg at appropriate timing.
Knee Flexion Contracture
"Same patient has a 30-degree knee flexion contracture despite physiotherapy."
A persistent knee flexion contracture despite conservative measures may need **soft tissue release**. First, ensure **medical treatment is optimized** (no active synovitis). Physiotherapy and serial casting/splinting should be tried. If still contracted, **posterior capsular release** with hamstring lengthening may be needed. Post-op, aggressive physiotherapy is essential.
Cervical Spine in JIA
"Teenager with long-standing polyarticular JIA needs tonsillectomy. What are the anaesthetic concerns?"
Patients with **polyarticular JIA** can have **cervical spine involvement** with C1-C2 instability. Before any surgery requiring intubation, I would obtain **flexion-extension lateral cervical spine X-rays** to assess for atlantoaxial instability. If unstable, **awake fibreoptic intubation** or **manual inline stabilization** during intubation is required. I would also ensure **TMJ function** is adequate as some JIA patients have limited mouth opening. I would communicate with the anaesthetist and document the cervical spine status.
MCQ Practice Points
Type MCQ
Q: What is the most common JIA subtype? A: Oligoarticular (≤4 joints).
Growth MCQ
Q: What causes initial leg lengthening in JIA? A: Hyperemia from inflammation causes physeal overgrowth.
Eye MCQ
Q: What eye complication is associated with oligoarticular JIA? A: Uveitis (especially if ANA positive).
RF+ MCQ
Q: Which JIA subtype has the worst prognosis? A: RF-positive polyarticular - similar to adult rheumatoid arthritis.
Systemic JIA MCQ
Q: What is the characteristic rash in systemic JIA? A: Salmon-pink, evanescent rash that appears with fever spikes.
Cervical Spine MCQ
Q: What cervical spine concern exists in polyarticular JIA? A: C1-C2 instability - requires pre-operative assessment before intubation.
Guidelines, Registries & Global Practice
Global epidemiology
- JIA is the most common chronic inflammatory rheumatic disease of childhood. Population-based studies show wide variation: incidence roughly 1.6-23 per 100,000/year and prevalence 3.8-400 per 100,000.
- Oligoarticular onset predominates in European/North American cohorts; systemic and polyarticular onset are relatively more common in parts of Asia, Africa and Latin America.
- Female predominance overall (especially ANA-positive oligoarticular and uveitis); enthesitis-related arthritis is more common in older boys.
Major guidelines — side by side
| Body | Scope | Core position |
|---|---|---|
| ACR (US) | Treatment by disease group + prognostic features | Stepwise escalation: NSAIDs/intra-articular steroid → methotrexate → biologic for poor-prognosis or refractory disease |
| EULAR/PReS (Europe) | Points to consider, systemic JIA & non-systemic | Treat-to-target to inactive disease; early biologic in systemic JIA; window-of-opportunity concept |
| BSPAR / NICE (UK) | Biologic eligibility & uveitis screening | Structured ophthalmology screening schedule; biologics for inadequate methotrexate response |
| ILAR (global) | Classification | Seven-category framework underpinning all guidelines |
Registry & long-term data
- Pharmacovigilance registries (e.g. German BiKeR, UK BSPAR-ETN/BCRD, US CARRA Registry, Pharmachild/PRINTO) track biologic safety — malignancy and serious-infection signals have been reassuring at population scale.
- Joint-replacement registries show end-stage arthroplasty for JIA is now uncommon; when performed, survivorship is good but technically demanding (small implants, deformity, osteopenia).
High- vs limited-resource practice variation
- Well-resourced settings: early methotrexate, prompt biologic access, protocolised slit-lamp uveitis screening, MDT (rheumatology, ophthalmology, physiotherapy, orthopaedics, psychology), structured adolescent transition to adult services.
- Limited-resource settings: delayed diagnosis, reliance on NSAIDs/steroids and methotrexate due to biologic cost/availability, higher burden of established deformity, contractures and growth disturbance at presentation — raising the relative role of orthopaedic soft-tissue and reconstructive surgery.
- Universal priorities: control inflammation early, screen the eyes, preserve growth and function, and assess the cervical spine and TMJ before any anaesthetic in polyarticular disease.
JUVENILE IDIOPATHIC ARTHRITIS
Clinical summary
TYPES
- •Oligoarticular (most common)
- •Polyarticular RF+/-
- •Systemic (Still's)
- •Enthesitis-related
GROWTH
- •Initial overgrowth (hyperemia)
- •Later undergrowth (physeal damage)
- •Leg length discrepancy
- •Valgus knee common
UVEITIS RISK
- •Oligoarticular subtype
- •ANA positive
- •Female
- •Young onset
TREATMENT
- •NSAIDs for mild
- •DMARDs (methotrexate)
- •Biologics (TNF, IL-1/6)
- •Physio essential
SURGERY
- •After medical optimization
- •Contracture release
- •Epiphysiodesis for LLD
- •Arthroplasty (rare)
CERVICAL SPINE
- •C1-C2 instability risk
- •Pre-op imaging
- •TMJ may limit mouth opening
- •Communicate with anaesthesia
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Septic Arthritis | Acute, single joint, febrile, elevated WCC |
| Reactive Arthritis | Post-infectious, self-limiting |
| Lyme Arthritis | Endemic area, tick bite, Borrelia serology |
| Leukemia | Night pain, bone pain, abnormal blood film |
| Transient Synovitis | Hip, resolves within 2 weeks, normal bloods |