Avascular Necrosis of Lunate | Progressive Wrist Arthritis | Ulnar Variance Key
- Negative Ulnar Variance: Present in 78% - ulna shorter than radius increases lunate loading
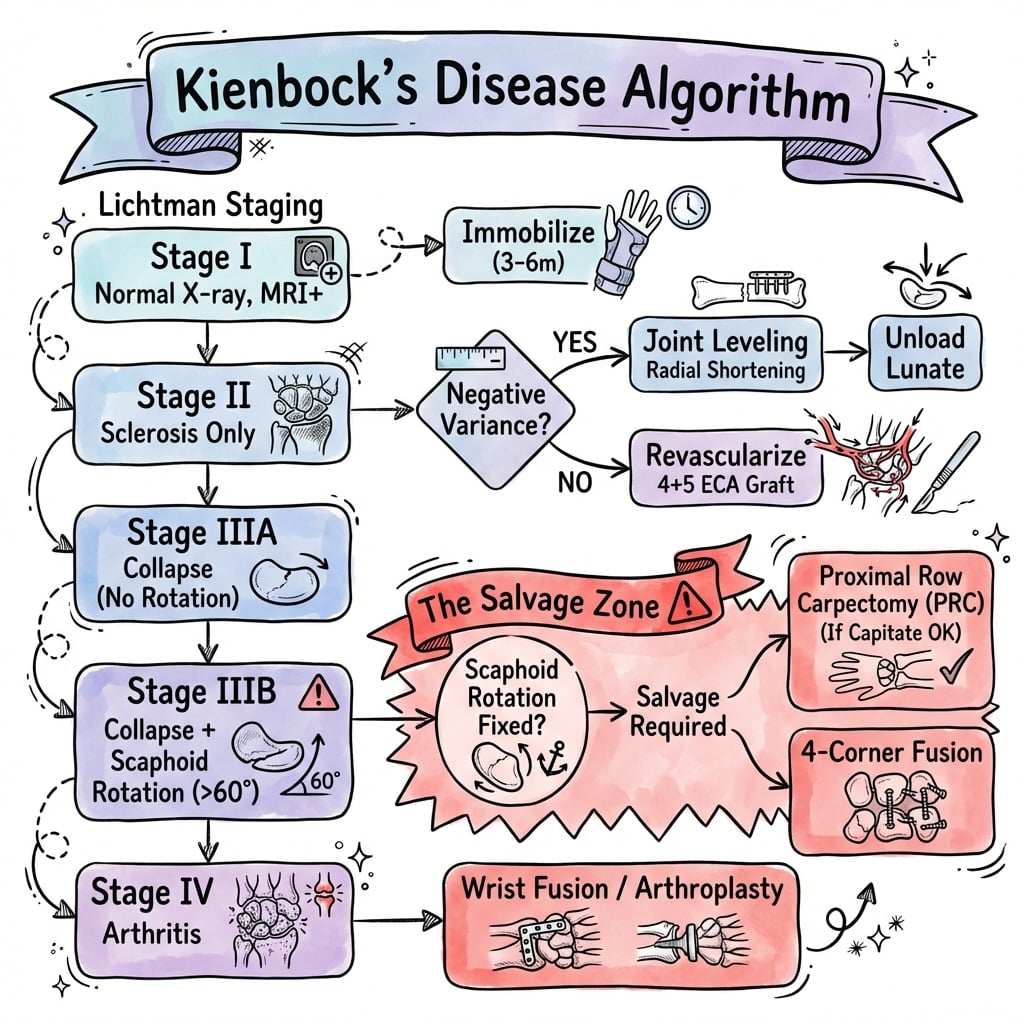
- Lichtman Stage IIIB: Scaphoid rotation = critical prognostic divider - salvage surgery required
- MRI Gold Standard: Detects Stage I disease before X-ray changes appear
- Joint Leveling: Radial shortening or ulnar lengthening for Stage II-IIIA with negative variance
- PRC: Proximal row carpectomy - motion-preserving salvage for Stage IIIB-IV without arthritis
- “Negative ulnar variance = lunate takes excessive load
- “Stage IIIB (scaphoid rotation) = point of no return
- “MRI shows bone marrow edema before X-ray changes
- “Radial shortening decreases lunate loading by 45%
Lichtman Stage IIIB is the critical divider. Scaphoid rotation indicates lunate collapse severe enough to destabilize the carpus. Stages I-IIIA may benefit from joint leveling; IIIB-IV require salvage procedures.
Negative ulnar variance in 78% of cases. Ulna 2-4mm shorter than radius increases lunate loading. Radial shortening osteotomy decreases lunate force by 45%.
Stage I disease is MRI-only. Bone marrow edema and low T1 signal precede X-ray sclerosis by months. Early detection may allow non-operative treatment.
PRC vs Fusion trade-offs. Proximal row carpectomy preserves 50% motion but requires intact capitolunate articulation. Fusion eliminates motion but relieves pain reliably.
- X-ray Findings
- Normal X-ray, MRI positive
- Treatment
- Immobilization 3-6 months
- Key Pearl
- May arrest progression if caught early
- X-ray Findings
- Sclerosis, no collapse
- Treatment
- Radial shortening or revascularization
- Key Pearl
- Joint leveling decreases lunate loading
- X-ray Findings
- Collapse, NO scaphoid rotation
- Treatment
- Consider joint leveling if lunate viable
- Key Pearl
- Last chance for joint-preserving surgery
- X-ray Findings
- Collapse WITH scaphoid rotation
- Treatment
- PRC or limited fusion
- Key Pearl
- Scaphoid rotation = carpal instability
- X-ray Findings
- Generalized arthritis
- Treatment
- Total wrist fusion or arthroplasty
- Key Pearl
- End-stage disease
LUNATERisk Factors for Kienböck's Disease
Hook:LUNATE = the bone that dies! Remember the risk factors that predispose to AVN.
PRC-FSalvage Surgery Options
Hook:PRC-F = Proximal Row and Carpal Fusions - the salvage spectrum from motion-preserving to stable fusion!
Overview and Epidemiology
Kienböck's disease is a rare but disabling condition affecting young, active patients. Understanding staging and treatment algorithms is essential for hand surgery exams and clinical practice.
Kienböck's Disease is avascular necrosis (AVN) of the lunate bone, leading to progressive collapse, carpal instability, and wrist arthritis.
- Age: 20-40 years (peak incidence)
- Gender: Male predominance 2:1
- Occupation: Manual laborers, athletes
- Bilateral: Rare (less than 5%)
Typically affects dominant hand of young workers.
- Early (I-II): May stabilize with treatment
- Mid (IIIA): Progressive collapse likely
- Advanced (IIIB-IV): Irreversible arthritis
- Timeline: Years to decades of progression
Early diagnosis is critical to prevent collapse.
Pathophysiology and Etiology
The lunate has tenuous blood supply with two main patterns: Type I (Y-pattern from radial and ulnar arteries, 80%) and Type II (single vessel, 20%). Interruption leads to AVN, particularly in Type II anatomy.
Etiology is multifactorial:
Risk Factors
-
Negative Ulnar Variance (78% of cases)
- Ulna 2-4mm shorter than radius
- Increases lunate loading by transmitting more force
- Present in normal population at only 23%
-
Repetitive Microtrauma
- Manual labor, jackhammer use
- Gymnastics, racquet sports
- Cumulative stress to lunate
-
Vascular Anatomy
- Single vessel supply (Type II) at higher risk
- Intraosseous anastomoses limited
- Watershed areas vulnerable
-
Systemic Associations
- Corticosteroid use
- Systemic lupus erythematosus
- Gout, sickle cell disease
- Hypothyroidism
Pathophysiology Cascade:
- Vascular insult or repetitive trauma
- Ischemia and bone marrow edema
- Osteocyte death and sclerosis
- Structural collapse of lunate
- Scaphoid rotation and carpal instability
- Progressive radiocarpal and midcarpal arthritis
Negative ulnar variance increases lunate loading. In a neutral wrist, 60% of axial load transmits through radius and 40% through ulna. With 2mm negative variance, lunate bears 95% of radiocarpal load.
Radial shortening osteotomy redistributes load to ulna.
AVN weakens subchondral bone. Repeated loading causes microfractures, progressive height loss, and eventual fragmentation. Once collapse begins (Stage III), progression is difficult to arrest.
Early intervention aims to prevent collapse.
Classification Systems
Lichtman Classification (Modified 2010)
The gold standard staging system, based on radiographic appearance and treatment implications.
- Radiographic Findings
- Normal X-ray; MRI shows AVN
- Lunate Status
- Structurally intact
- Treatment Approach
- Immobilization, observation
- Radiographic Findings
- Sclerosis on X-ray
- Lunate Status
- Intact, no collapse
- Treatment Approach
- Joint leveling, revascularization
- Radiographic Findings
- Collapse, no scaphoid rotation
- Lunate Status
- Collapsed, some viability
- Treatment Approach
- Joint leveling if viable, or PRC
- Radiographic Findings
- Collapse WITH scaphoid rotation
- Lunate Status
- Collapsed, carpal instability
- Treatment Approach
- PRC, partial fusion
- Radiographic Findings
- Generalized carpal arthritis
- Lunate Status
- Fragmented, arthritic
- Treatment Approach
- Total wrist fusion or arthroplasty
Stage IIIB is the critical prognostic divider: scaphoid rotation indicates fixed carpal collapse beyond salvage with joint-preserving techniques.
Staging determines treatment strategy and prognosis.
I See Carpal ArthritisLichtman Staging Progression
Hook:I See Carpal Arthritis = the natural progression of untreated Kienböck's disease from invisible to end-stage!
Lunate Viability: The Schmitt Perfusion Classification
The Lichtman stage tells you how far the bone has collapsed; the Schmitt contrast-enhanced MRI grade tells you whether the marrow is still alive. A viable or reparable lunate can be unloaded or revascularised; a completely necrotic lunate with no repair zone will not respond to grafting and points toward salvage.
The 2016 integrated algorithm (Lichtman, Pientka & Bain) and several European centres pair the osseous Lichtman stage with the Schmitt perfusion/viability classification — the very axis those cards reference — yet plain radiographs cannot show it. Schmitt and Kalb described that a necrotic lunate remodels in band-shaped zones that are only demonstrable on gadolinium-enhanced MRI.
On contrast-enhanced MRI the lunate separates into:
- Proximal necrotic zone — dead marrow, no enhancement
- Intermediate reparative zone — hypervascular granulation/repair tissue that enhances avidly
- Distal viable zone — preserved marrow with normal perfusion
Intravenous gadolinium is mandatory: only a perfusion study reliably separates the non-enhancing necrotic zone from the enhancing repair zone.
- A lunate with a substantial viable or reparative component is a candidate for unloading or revascularisation (radial shortening, pedicled graft, medial femoral condyle flap).
- A globally necrotic, non-enhancing lunate is effectively a "compromised lunate" — reconstruction is unlikely to succeed, so PRC or fusion is the more honest choice.
- This perfusion axis underlies the 2016 "intact / compromised lunate / compromised wrist" framework.
Practical protocol. High-resolution CT best shows the osseous detail that stages the disease — proximal coronal fractures (Lichtman IIIA) and pancarpal arthritis (Stage IV) — while contrast-enhanced MRI grades marrow viability. Used together, CT plus contrast-enhanced MRI classify Kienböck's disease by both morphology and perfusion, which plain films cannot do.
- Contrast-enhanced MRI resolves the lunate into a proximal necrotic, middle reparative and distal viable zone
- Intravenous gadolinium is mandatory to separate necrotic from reparative tissue on perfusion imaging
- CT is more sensitive than radiographs for proximally located (stage IIIA) fractures and stage IV osteoarthritis
- Synoptic clinical, biomechanical and imaging assessment distinguishes Kienböck's from mimics in over 80% of cases
- Contrast-enhanced MRI differentiates up to three band-shaped zones: necrotic (proximal), hypervascular repair (intermediate) and viable (distal)
- Intravenous gadolinium is recommended to distinguish necrotic from repair tissue
- High-resolution CT best depicts osteosclerosis, insufficiency fractures and advanced osteoarthritis
- Combined HRCT and contrast-enhanced MRI allow exact classification of osteonecrosis by morphology AND viability
Clinical Assessment
- Pain: Dorsal wrist pain, worse with activity
- Weakness: Grip strength reduced 30-50%
- Stiffness: Progressive loss of motion
- Occupation: Manual labor, repetitive wrist use
- Trauma: History of wrist injury in 30%
- Dominant hand: Usually affected
Insidious onset over months is typical.
- Inspection: Dorsal swelling over lunate
- Palpation: Tenderness over lunate fossa
- ROM: Decreased flexion and extension (50% of normal)
- Strength: Grip weakness (30-50% reduction)
- Provocative: Pain with axial loading of 3rd metacarpal
- Watson test: May be positive (scaphoid instability)
Physical findings are non-specific; imaging confirms diagnosis.
- Pain
- Mild, activity-related
- Motion Loss
- Minimal (10-20%)
- Grip Strength
- Near normal
- Pain
- Moderate, constant
- Motion Loss
- Moderate (30-50%)
- Grip Strength
- Reduced 30-40%
- Pain
- Severe, rest pain
- Motion Loss
- Severe (over 50%)
- Grip Strength
- Reduced over 50%
Dorsal/central wrist pain in a young adult has several mimics. MRI is the single best discriminator: AVN of the lunate shows diffuse low T1 marrow signal, whereas the alternatives below have characteristic alternative patterns.
- Typical features
- Insidious dorsal pain, young manual worker, grip loss
- Key imaging discriminator
- Diffuse low T1 signal throughout lunate; later collapse
- Distinguishing point from Kienböck's
- AVN is global to the lunate, not focal
- Typical features
- Trauma history, dorsal SL tenderness, positive Watson
- Key imaging discriminator
- SL gap (Terry-Thomas sign), DISI; lunate marrow normal
- Distinguishing point from Kienböck's
- Lunate signal is normal; instability is ligamentous
- Typical features
- Ulnar-sided pain, positive ulnar variance, click
- Key imaging discriminator
- Ulnar-positive variance, ulnar lunate/triquetral cysts
- Distinguishing point from Kienböck's
- Pain is ulnar-sided; usually ulnar-POSITIVE variance
- Typical features
- Ulnar pain on loading/grip
- Key imaging discriminator
- Subchondral cysts at ulnar lunate, positive variance
- Distinguishing point from Kienböck's
- Opposite ulnar variance to classic Kienböck's
- Typical features
- Acute trauma, focal tenderness
- Key imaging discriminator
- Discrete fracture line; focal not diffuse marrow change
- Distinguishing point from Kienböck's
- Single fracture line rather than diffuse AVN
- Typical features
- Localised swelling, dorsal lump
- Key imaging discriminator
- Cyst or osteophyte; lunate normal
- Distinguishing point from Kienböck's
- Structural lesion, normal lunate marrow

Investigations
Investigation Protocol
PA, lateral, and clenched-fist views. Look for: lunate sclerosis (Stage II), collapse with decreased height (Stage III), scaphoid rotation on lateral (IIIB), carpal arthritis (IV). Measure ulnar variance on neutral rotation PA view.
T1 and T2 sequences. T1 shows low signal (bone marrow replacement), T2 shows variable signal depending on stage. Detects Stage I disease before X-ray changes. Also assesses lunate viability and cartilage integrity.
For surgical planning. Defines extent of collapse, fracture lines, and articular involvement. Useful before salvage procedures to assess capitate head (for PRC) or plan fusion surfaces.
Rarely used. Increased uptake in lunate. Less specific than MRI. Historical interest; MRI has replaced it.
Key Radiographic Measurements
- Technique
- PA view, neutral rotation, difference in radial-ulnar heights
- Normal Value
- 0 to +2mm
- Kienböck's Finding
- Negative variance in 78%
- Technique
- Lateral view, capitate to radius distance / lunate to 3rd MC length
- Normal Value
- 0.54 ± 0.03
- Kienböck's Finding
- Decreased in Stage III+
- Technique
- Lateral view, angle between scaphoid and lunate
- Normal Value
- 30-60 degrees
- Kienböck's Finding
- Over 60° in Stage IIIB (DISI)
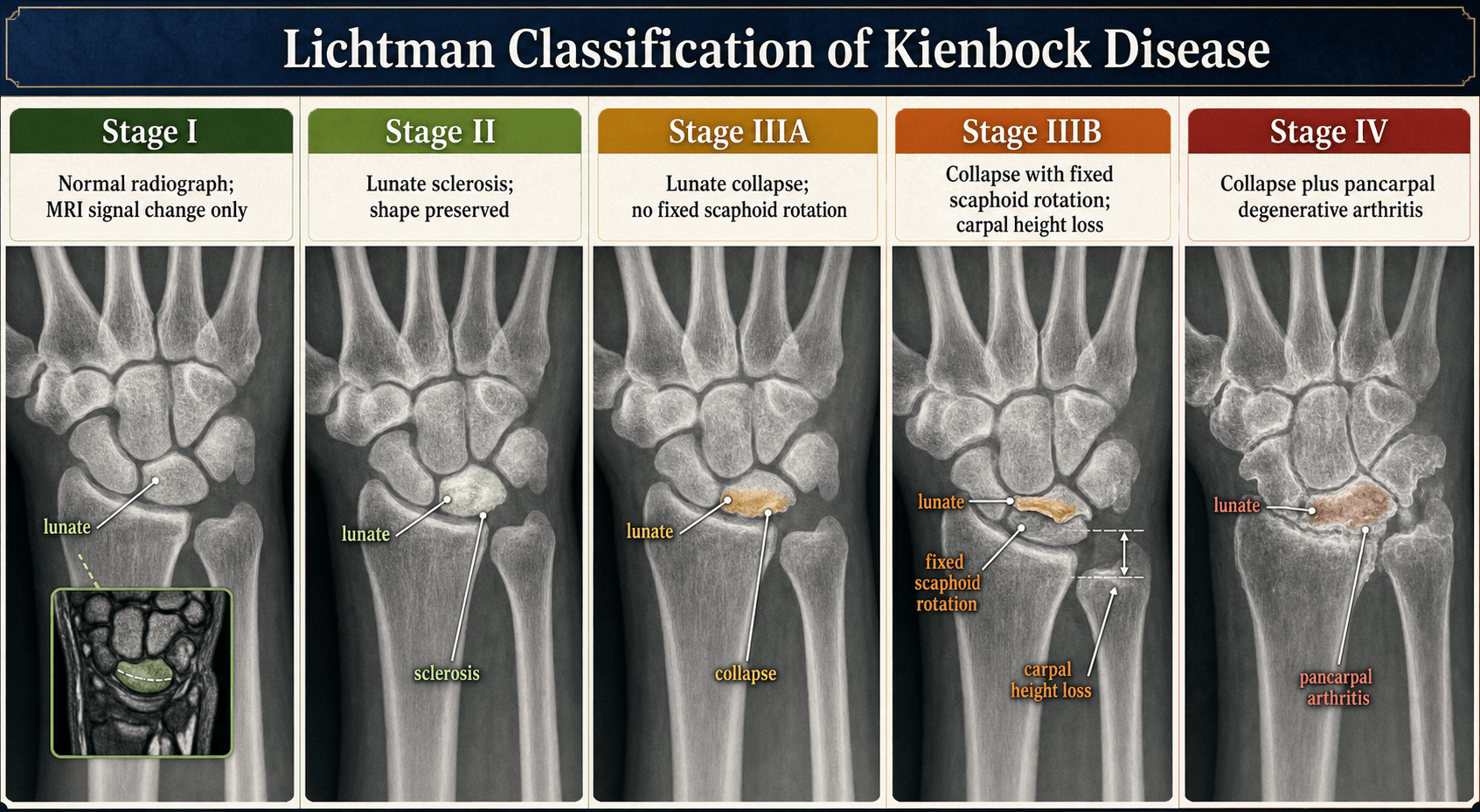
Radiographic Stages
Normal X-ray (diagnosis requires MRI)
Increased density (sclerosis) of lunate, normal shape and height
Lunate collapse with height loss, scapholunate angle normal (less than 60°)
Lunate collapse PLUS scaphoid rotation - scapholunate angle over 60° (DISI pattern)
Generalized carpal arthritis - radiocarpal, midcarpal, or both
Management Algorithm
Conservative Management
Indications: Stage I disease, patient refuses surgery, medical comorbidities
Conservative Treatment Steps
Short-arm cast or splint for 3-6 months. Aim is to unload lunate and allow revascularization. Success rate 30-50% in Stage I. Monitor with serial MRI every 3-4 months.
Avoid heavy manual work. Reduce impact loading. Ergonomic assessment. Consider job modification or retraining.
Bisphosphonates (experimental). Limited evidence. Iloprost (prostacyclin analog) may improve vascularity. NSAIDs for pain control.
Outcomes: Conservative treatment rarely effective beyond Stage I. Progression common without surgical intervention.
Conservative management is temporizing in most cases.
- Preferred Treatment
- Immobilization 3-6 months
- Alternative
- Observation
- Outcomes
- 50% arrest progression
- Preferred Treatment
- Radial shortening (if -UV)
- Alternative
- Revascularization
- Outcomes
- 60-80% pain relief
- Preferred Treatment
- Joint leveling or revascularization
- Alternative
- Consider PRC
- Outcomes
- Variable, 40-70% success
- Preferred Treatment
- PRC or four-corner fusion
- Alternative
- STT fusion
- Outcomes
- 80% pain relief, limited motion
- Preferred Treatment
- Total wrist fusion
- Alternative
- Wrist arthroplasty (selected)
- Outcomes
- Excellent pain relief, no motion
Surgical Technique
Radial Shortening Osteotomy
Surgical Steps
Supine, arm table, tourniquet. Volar approach to distal radius: longitudinal incision between FCR and radial artery. Protect superficial radial nerve branches.
Retract FCR ulnarly, radial artery radially. Expose pronator quadratus and incise longitudinally. Subperiosteal elevation of distal radius.
Mark osteotomy 2-3cm proximal to radial articular surface. Perform transverse osteotomy with oscillating saw. Remove 2-4mm bone wedge (based on pre-op ulnar variance measurement). Shorten radius.
Compress osteotomy and apply dorsal locking plate. Ensure stable fixation. Check DRUJ stability and rotation.
Repair pronator quadratus (protects plate). Skin closure, splint in neutral.
- Pre-op planning: measure exact ulnar variance and plan shortening amount
- Avoid excessive shortening (over 4mm) - causes DRUJ symptoms
- Compress osteotomy fully to minimize nonunion risk
- Use locking plate for secure fixation in osteopenic bone
- Inadequate shortening - fails to unload lunate
- Excessive shortening - DRUJ pain and stiffness
- Nonunion if inadequate fixation or bone contact
Radial shortening decreases lunate loading biomechanically.
Scaphotrapeziotrapezoid (STT) Arthrodesis
STT (triscaphe) arthrodesis is an alternative limited intercarpal fusion for collapsing Kienböck's: fusing the scaphoid to the trapezium and trapezoid stabilises the radial column, holds the scaphoid extended and shifts axial load off the lunate onto the radioscaphoid column while maintaining carpal height. Popularised by Watson, its stated indication is Lichtman stage IIIA/IIIB.
Both the treatment table and the intraoperative image on this page reference STT fusion, so it is worth knowing its mechanism, its results and its signature complication — none of which the staging tables convey.
- Fuse scaphoid, trapezium and trapezoid with K-wires, staples, a circular plate or a memory-alloy concentrator, plus local bone graft
- The scaphoid is fixed in a corrected, extended position, redistributing load through the radioscaphoid column and away from the diseased lunate
- Carpal height is preserved, unlike lunate excision alone
- Frequently combined with debridement or excision of the necrotic lunate in advanced disease
- Reliable pain relief, with grip recovering to roughly 60 to 65 percent of the opposite side and most patients returning to their original occupation
- Wrist motion is reduced, radial and ulnar deviation especially, because the radial column is locked
- Radioscaphoid arthrosis is the characteristic late complication (around one quarter of cases at long follow-up)
- Nonunion is the main early risk; union typically takes about 7 to 11 weeks
STT fusion competes with radial shortening (for negative variance) and with the salvage options (PRC, four-corner fusion). It is most attractive when a joint-preserving load-shift is still wanted but candidates must accept the loss of deviation and the risk of later radioscaphoid wear. For the fusion techniques it sits alongside, see the dedicated four-corner-fusion and proximal-row-carpectomy topics.
- 26 patients with Lichtman stage IIIA/IIIB Kienböck's treated by STT arthrodesis; union in 25, mean follow-up 35 months
- Pain reduced to 72% of preoperative value at rest and 60% under stress; grip recovered to 60% of the opposite hand
- 80% returned to their original occupation; 20 of 26 would undergo the operation again
- The procedure both decreases load to the lunate AND maintains carpal height
- 30 STT fusions (23 for Kienböck's disease); all united at an average of 11.2 weeks, mean follow-up 84 months
- Radioscaphoid arthrosis developed in 23% (7 of 30) — the characteristic late complication of the procedure
- Grip strength improved from 18 kgf preoperatively to 27 kgf postoperatively
- 26 of 30 patients returned to their previous activities
Complications
- Early Complications
- Infection, CRPS
- Late Complications
- Nonunion (5%), DRUJ pain
- Management
- Bone graft, revision fixation
- Early Complications
- Pedicle injury, hematoma
- Late Complications
- Graft failure, lunate collapse
- Management
- Consider salvage procedure
- Early Complications
- Stiffness, CRPS
- Late Complications
- Capitate-radius arthritis (20% at 10 years)
- Management
- Convert to fusion
- Early Complications
- Nonunion (5-10%), hardware irritation
- Late Complications
- Adjacent joint arthritis
- Management
- Hardware removal, convert to total fusion
General Complications
- Stage I to IV over 3-10 years
- Inevitable without intervention in most cases
- Collapse and arthritis are endpoint
- Occurs after 2-5% of wrist surgeries
- Risk factors: female, prolonged immobilization
- Prevention: early motion, vitamin C supplementation
- Management: multidisciplinary pain team
- Common after any wrist surgery
- Worse with prolonged immobilization
- Prevention: early therapy, limit casting to 6 weeks max
Postoperative Care
Postoperative Protocol by Procedure
Short-arm splint. Finger and elbow ROM immediately. X-ray at 2, 6 weeks to assess union.
Wean splint, begin wrist ROM. Therapy for strengthening. Full activities at 12 weeks if healed.
Short-arm cast. Strict immobilization to allow graft incorporation. No motion.
Removable splint, begin ROM. Protected strengthening. Full activities 12-16 weeks.
Bulky dressing. Finger ROM immediately. Wound check, transition to removable splint at 2 weeks.
Removable splint, begin wrist ROM at week 3. Early motion prevents stiffness. Strengthen grip.
Wean splint, progressive strengthening. Return to normal activities by 3 months.
- Desk work: 2-4 weeks (depending on procedure)
- Light manual work: 8-12 weeks
- Heavy manual labor: 12-16 weeks or job modification
- Annual X-rays for first 3 years to detect progression
- MRI if symptoms worsen or new pain
- Salvage planning if joint-preserving procedure fails
Outcomes and Prognosis
- Pain Relief
- 50% improvement
- Motion Preservation
- Maintained if stable
- Durability
- Variable, monitoring needed
- Pain Relief
- 60-80% good outcome
- Motion Preservation
- Maintained
- Durability
- Good 5-10 years
- Pain Relief
- 40-70% improvement
- Motion Preservation
- Maintained if successful
- Durability
- Variable, graft-dependent
- Pain Relief
- 80% good pain relief
- Motion Preservation
- 50% motion vs normal
- Durability
- Durable 10+ years
- Pain Relief
- 85% pain relief
- Motion Preservation
- 40-50% motion
- Durability
- Good 5-10 years
- Pain Relief
- 95% pain relief
- Motion Preservation
- 0% motion
- Durability
- Excellent long-term
Prognostic Factors:
- Better Outcome
- I-II
- Worse Outcome
- IIIB-IV
- Better Outcome
- Under 30
- Worse Outcome
- Over 50
- Better Outcome
- Sedentary
- Worse Outcome
- Heavy manual labor
- Better Outcome
- Negative (correctable)
- Worse Outcome
- Neutral/positive
Natural History (Untreated):
- Stage I: 50% progress to Stage II within 2 years
- Stage II: 80% progress to Stage III within 3-5 years
- Stage IIIB: 100% progress to Stage IV without treatment
- Timeline: Variable, 3-15 years from onset to end-stage
Early diagnosis and intervention improve outcomes substantially.
Guidelines, Registries & Global Practice
Global epidemiology. Kienböck's disease is rare worldwide; most hand surgeons see only a handful of cases per year. It clusters in men aged 20-40, frequently in manual or vibration-exposed occupations (construction, drilling, mining). Negative ulnar variance is over-represented compared with the general population, though it is a predisposing rather than causal factor. There is no high-quality population incidence figure, and there is no implant registry for Kienböck's surgery because most procedures are osteotomies, fusions or carpectomies rather than arthroplasty.
No single global guideline — practice is built on cohort evidence and consensus. No society publishes a formal Kienböck's treatment guideline equivalent to a fracture protocol. Practice converges on staging-driven algorithms.
- Staging emphasis
- Lichtman radiographic + arthroscopic cartilage grading
- Early disease (Stage I-II)
- Unloading osteotomy or vascularized graft; MFC free flap in selected young patients
- Advanced (IIIB-IV)
- PRC favoured if capitate/lunate fossa intact
- Staging emphasis
- Lichtman plus Schmitt MRI perfusion grade
- Early disease (Stage I-II)
- Radial shortening for negative variance; conservative trial common in Stage I
- Advanced (IIIB-IV)
- PRC or four-corner fusion per surgeon preference
- Staging emphasis
- Strong interest in capitate shortening and combined revascularization
- Early disease (Stage I-II)
- Capitate shortening when variance is non-negative; vascularized pedicled graft
- Advanced (IIIB-IV)
- Limited carpal fusion; arthroplasty in low-demand only
- Staging emphasis
- Plain radiographs only (MRI often unavailable)
- Early disease (Stage I-II)
- Immobilization, activity modification; osteotomy where fixation available
- Advanced (IIIB-IV)
- Wrist fusion as reliable, low-cost salvage
Registry and high- vs limited-resource practice. Where MRI is freely available, Stage I disease is detected early and unloading or revascularization is offered before collapse. Where MRI is scarce, diagnosis is later and total wrist fusion becomes the dependable salvage because it needs no specialist implant and reliably abolishes pain. Vascularized bone grafting and medial femoral condyle free flaps are concentrated in microsurgical referral units. Documenting the neutral-rotation ulnar variance on every wrist radiograph remains a universal, resource-independent standard because it determines whether radial shortening or capitate shortening is the appropriate unloading procedure.
Consent essentials (universal). For salvage surgery, counsel explicitly on the motion-versus-pain-relief trade-off (PRC preserves roughly half of wrist motion; total fusion removes motion but most reliably relieves pain), and on progression risk if early-stage disease is managed non-operatively.
Controversies and Areas of Uncertainty
Kienböck's disease has no Level I evidence and no consensus guideline. A strong candidate acknowledges the uncertainty rather than overstating any single procedure.
The Shin et al systematic review (JBJS Am 2018) found radial osteotomy did not slow Lichtman-stage progression versus nonoperative care, despite better pain and motion. Whether we are modifying disease or only managing symptoms remains genuinely unsettled.
Negative ulnar variance, single-vessel supply and repetitive load are predisposing factors, not proven causes. Modern reviews reframe historic "causal" factors as markers of a pre-existing vulnerable lunate.
No reliable way to predict which MRI-only cases progress. Choice between immobilization with surveillance and early unloading/revascularization is shared decision-making, not protocol.
When variance is neutral or positive, radial shortening is biomechanically wrong. Capitate shortening osteotomy is the rational alternative (Motaghi et al 2025), but evidence is Level IV only.
Long-term outcomes are comparable (Chim & Moran). PRC is technically simpler with no nonunion risk; four-corner fusion may suit very heavy demand. No randomised comparison exists.
Medial femoral condyle free flap can reconstruct a compromised but salvageable lunate, but is confined to microsurgical units and lacks comparative trials against simpler unloading.
MCQ Practice Points
Q: What Lichtman stage represents the critical prognostic divider in Kienböck's disease? A: Stage IIIB - scaphoid rotation (scapholunate angle over 60°) indicates fixed carpal collapse and instability. Joint-preserving surgery (leveling, revascularization) is ineffective beyond this point; salvage procedures required.
Q: What percentage of Kienböck's disease patients have negative ulnar variance? A: 78% - compared to 23% in the general population. Negative variance increases lunate loading by shifting axial load away from the ulnocarpal joint.
Q: What is the investigation of choice for detecting Stage I Kienböck's disease? A: MRI - detects bone marrow edema and low T1 signal before radiographic changes appear. X-rays are normal in Stage I.
Q: By what percentage does radial shortening osteotomy decrease lunate loading? A: 45% - shortening the radius 2-4mm redistributes axial load from radiocarpal (lunate) to ulnocarpal articulation, unloading the lunate.
Q: What are the key requirements for successful proximal row carpectomy in Kienböck's disease? A: Intact capitate head cartilage AND intact lunate fossa (radiocarpal) cartilage. Any arthritis at these articulation sites is a contraindication; fusion would be preferred.
Q: What is the most common motion-preserving salvage procedure for Stage IIIB Kienböck's disease? A: Proximal row carpectomy (PRC) - provides 80% pain relief and preserves 50% wrist motion. Durable for 10+ years if cartilage is intact.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old male manual laborer presents with 6 months of wrist pain. X-rays show lunate sclerosis with no collapse. MRI confirms AVN with intact lunate architecture. Ulnar variance is negative 3mm.”
“A 45-year-old presents with chronic wrist pain and stiffness. X-rays show lunate collapse with scapholunate angle of 70 degrees. CT shows intact capitate head cartilage. What is your assessment and management?”
“A 28-year-old woman has wrist pain for 3 months. X-rays are normal but MRI shows low T1 signal in the lunate with bone marrow edema. Ulnar variance is neutral. How do you manage this Stage I disease, and what does the evidence say about early intervention?”
Key Anatomy
- Lunate = keystone of proximal carpal row
- Vascular supply: Y-pattern (80%) or single vessel (20%)
- Type II anatomy (single vessel) = higher AVN risk
- Ulnar variance: negative in 78% vs 23% normal population
Lichtman Staging (Modified)
- Stage I: Normal X-ray, MRI shows AVN
- Stage II: Sclerosis, no collapse
- Stage IIIA: Collapse, scaphoid angle less than 60°
- Stage IIIB: Collapse + scaphoid rotation over 60° (CRITICAL)
- Stage IV: Generalized carpal arthritis
Investigations
- MRI: Gold standard, detects Stage I before X-ray
- X-ray: Measure ulnar variance on neutral PA view
- CT: Surgical planning, assess capitate head for PRC
- Scapholunate angle: over 60° = Stage IIIB (DISI)
Treatment Algorithm
- Stage I: Immobilization 3-6 months, serial MRI
- Stage II: Radial shortening if negative UV (60-80% success)
- Stage IIIA: Joint leveling or consider PRC
- Stage IIIB: PRC (if intact cartilage) or four-corner fusion
- Stage IV: Total wrist fusion (gold standard for pain)
Surgical Pearls
- Radial shortening: Decrease lunate loading 45%
- 4+5 ECA graft: Vascularized from distal radius
- PRC: Requires intact capitate and radiocarpal cartilage
- PRC outcomes: 80% pain relief, 50% motion, durable 10+ years
Evidence Base
- Reviews the four-stage radiographic Lichtman classification and its treatment algorithm
- Stage IIIB (fixed scaphoid rotation) marks the transition from joint-preserving to salvage surgery
- Emphasises that a reproducible staging system underpins surgical decision-making
- Anticipates perfusion- and cartilage-based classifications as adjuncts to plain radiographs
- Arthroscopic classification grading the number of non-functional lunate and adjacent articular surfaces
- Disease typically begins at the proximal lunate surface before involving the radial lunate facet
- Procedure is matched to grade: synovectomy/radial shortening, PRC, radioscapholunate fusion, or wrist fusion
- Adds intra-articular cartilage assessment that plain radiographs cannot provide
- Integrates the Lichtman (osseous), Schmitt (perfusion/viability) and Bain (cartilage) classifications into one algorithm
- Frames management around 'intact', 'compromised lunate', 'compromised wrist' and unreconstructable end-stage
- Compromised lunate may be reconstructed with medial femoral condyle graft or proximal row carpectomy
- Stresses that patient factors (age, demand, comorbidity) and surgeon factors modify the final decision
- 17 long-term studies (mean follow-up at least 10 years): 12 radial osteotomy, 5 nonoperative
- Radial osteotomy did NOT slow Lichtman-stage progression compared with nonoperative care
- More-than-moderate pain at final follow-up: 5.7% after radial osteotomy vs 23.2% nonoperative
- Total wrist arc was greater after radial osteotomy (107° vs 89°)
- 144 consecutive proximal row carpectomies, mean follow-up 13.4 years
- Good pain relief with preservation (not improvement) of motion; 12% required revision
- A preoperative diagnosis of Kienböck's disease was associated with improved pain, function and survival
- Radiocapitate arthrosis developed in 45% but did not correlate with clinical outcome or revision
- Six studies, 147 patients with at least 10-year follow-up after proximal row carpectomy
- No significant change between pre- and long-term postoperative motion; mean grip 68.4% of contralateral
- Outcomes comparable to four-corner arthrodesis; 14.3% failure rate requiring re-operation
- Heavy manual labourers fare worse; trauma and early-stage Kienböck's fare better
- 13 studies, 293 patients with neutral or positive ulnar variance (radial shortening biomechanically inappropriate)
- Isolated capitate shortening osteotomy (125 patients) gave reliable relief: persistent pain 10.4%, revision 5.6%
- Combined decompression plus revascularization appeared most useful in Stage IIIA disease
- Evidence is predominantly Level IV case series with marked heterogeneity