Congenital localized gigantism of digits following nerve territory distribution - staged surgical management
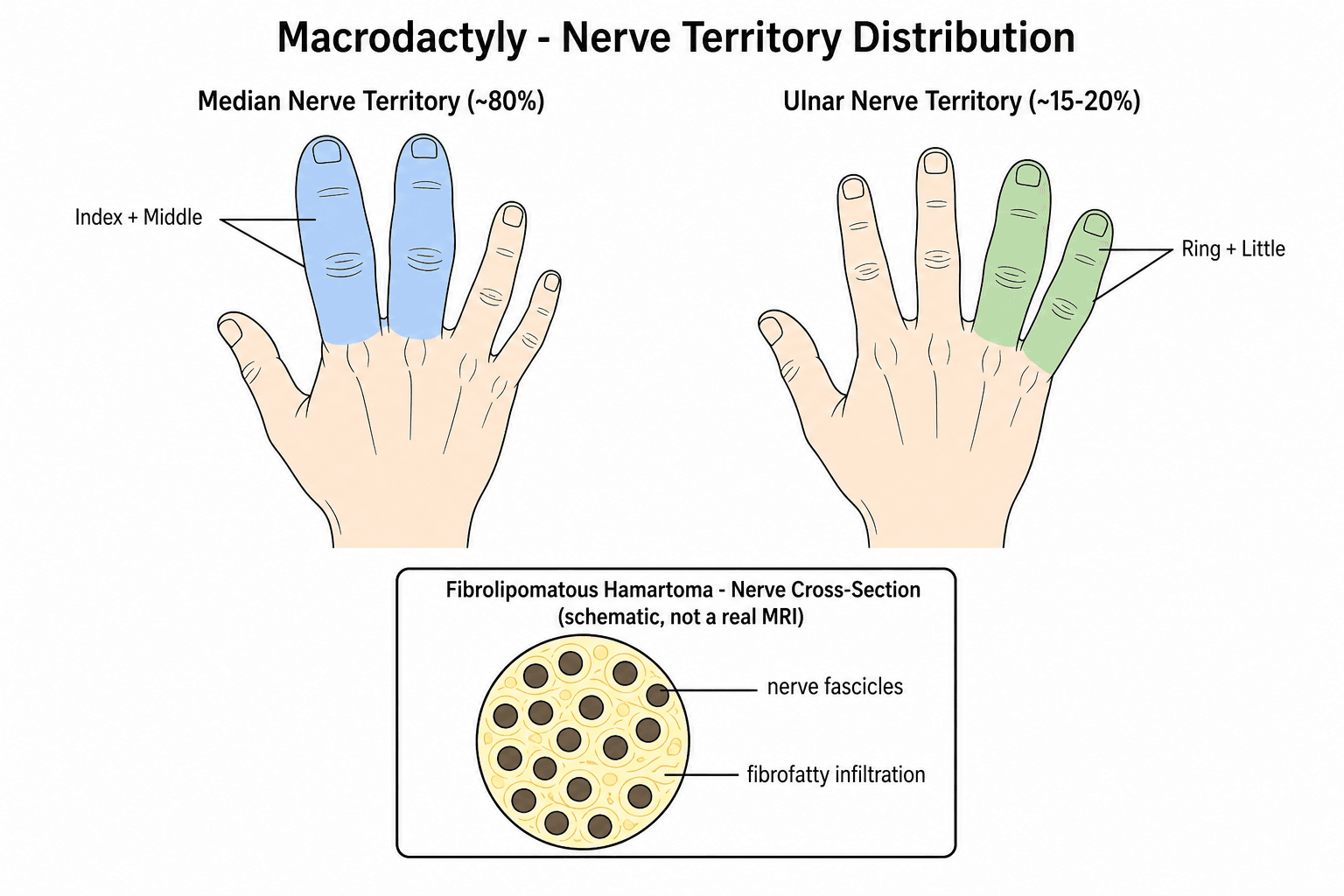
- Nerve territory distribution is PATHOGNOMONIC - median nerve 80%, ulnar 15-20%
- All mesenchymal elements enlarged (bone, nerve, fat, skin, vessels)
- Two types: Static (proportional growth) vs Progressive (accelerated growth)
- Staged debulking preferred - preserve neurovascular structures
- Epiphysiodesis before skeletal maturity to prevent further length discrepancy
- “Index and middle finger = median nerve; ring and small = ulnar nerve
- “MRI shows intraneural lipomatosis (high T1 signal in enlarged nerve)
- “Ray amputation may be best option for severe, non-functional digits
- “Progressive type has higher recurrence and worse functional outcomes
Macrodactyly
Epidemiology and Clinical Significance
Incidence and Demographics
Classic operative experience in macrodactyly
- Foundational operative series establishing macrodactyly as a rare overgrowth of all digital tissue elements (bone, nerve, fat, skin)
- Macrodactyly accounts for roughly 1% of congenital upper-limb anomalies
- Described staged debulking combined with osteotomy and epiphysiodesis to control size and length
Macrodactyly is exceptionally rare, with an estimated incidence of 1 in 100,000 live births. The condition shows no gender predilection and affects all ethnic groups equally. Approximately 70% of cases are unilateral, with the index and middle fingers most commonly involved when the median nerve territory is affected.
Pattern of Involvement
The distribution of macrodactyly consistently follows nerve territories, which is pathognomonic for the condition. The median nerve territory is affected in approximately 80% of cases, typically involving the index and middle fingers. Ulnar nerve territory involvement occurs in 15-20% of cases, affecting the ring and small fingers. Radial nerve territory involvement is exceptionally rare, representing fewer than 5% of cases.
Associated Conditions
Macrodactyly may occur as an isolated finding or in association with other conditions. Recognized associations include neurofibromatosis type 1 (requiring careful evaluation for café-au-lait spots and family history), Proteus syndrome (asymmetric overgrowth with connective tissue nevi), and Klippel-Trenaunay-Weber syndrome (capillary malformations with venous and lymphatic anomalies). Approximately 10-15% of patients have associated syndactyly of the affected digits.
Pathophysiology and Anatomy
Molecular Basis (PIK3CA / PROS)
Isolated macrodactyly is now recognised as part of the PIK3CA-Related Overgrowth Spectrum (PROS). The driver is a somatic, mosaic gain-of-function mutation in PIK3CA (the gene encoding the p110-alpha catalytic subunit of PI3K), which constitutively activates the PI3K-AKT-mTOR pathway and produces unregulated tissue growth. Because the mutation is post-zygotic and mosaic, overgrowth is segmental and follows the affected cell lineage rather than a Mendelian inheritance pattern. The same pathway underlies the broader PROS family (CLOVES, fibroadipose hyperplasia, hemihyperplasia-multiple lipomatosis), and recognising macrodactyly as a forme fruste of PROS prompts screening for associated overgrowth and vascular anomalies.
Somatic PIK3CA mutations drive isolated macrodactyly
- Mosaic activating PIK3CA mutations detected in 10 of 12 patients with isolated macrodactyly
- Recurrent oncogenic hotspot variants (H1047R, H1047L, E545K, E542K) at low mutant allele fraction (7-27%)
- Adipose tissue had the highest mutation-detection rate, followed by nerve and skin
Tissue Changes
All mesenchymal tissue elements undergo disproportionate growth in macrodactyly. Histological examination reveals characteristic features including extensive fibrofatty proliferation within and around peripheral nerves (lipomatous macrodystrophy), hypertrophy of all digital tissues, and increased vascularity with tortuous vessels. The bone shows accelerated growth with widened medullary canals and early physeal closure in some cases.
Nerve Involvement
The peripheral nerve involvement is pathognomonic for macrodactyly. The affected nerve appears grossly enlarged, with a diameter that may be 3-5 times normal size. Microscopic examination shows adipose tissue infiltration between nerve fascicles (intraneural lipomatosis), increased epineurial connective tissue, and normal myelinated axons interspersed with excessive perineural fat. This neural lipomatous infiltration distinguishes macrodactyly from other causes of localized gigantism.
Growth Patterns
- static
- Full manifestation present
- progressive
- Mild or subtle findings
- static
- Proportional to body growth
- progressive
- Accelerated, disproportionate
- static
- More common (60-70%)
- progressive
- Less common (30-40%)
- static
- Clearly defined distribution
- progressive
- May cross nerve territories
- static
- Elective, staged procedures
- progressive
- Earlier intervention needed
- static
- Better functional outcomes
- progressive
- Higher recurrence, worse function
Classification
Barsky Classification (by growth pattern)
The most exam-relevant classification. It divides macrodactyly by growth behaviour, which directly informs surgical timing and prognosis.
- Type I - Static (60-70%): Full manifestation at birth; the enlarged digit grows proportionally with the child. Better prognosis; elective staged procedures.
- Type II - Progressive (30-40%): Accelerated, disproportionate growth, often worsening during growth spurts. Higher recurrence, worse function; earlier and more aggressive intervention.
Viva pearl: confirm static versus progressive from the growth history and serial measurements - it is the single most useful prognostic discriminator.
Clinical Presentation
History and Physical Examination
Parents typically present with concerns about digital enlargement noticed at birth or during early childhood. For static macrodactyly, the disproportion is evident from birth but grows proportionally with the child. Progressive macrodactyly shows accelerated growth that becomes increasingly apparent with age, particularly during growth spurts.
Physical examination reveals characteristic findings including disproportionate enlargement of one or more digits, with involvement of all tissues (skin, subcutaneous tissue, bone, nail). The affected digit feels doughy due to excessive subcutaneous fat. Skin folds may be prominent with redundant tissue. The nerve territory distribution should be carefully documented, as this is pathognomonic for the diagnosis.
Systematic Assessment: Examine from fingertip to forearm to identify extent of involvement
Nerve Territory Mapping: Document which digits are affected and correlate with median/ulnar/radial nerve distribution
Functional Testing: Assess grip strength, pinch, range of motion, and activities of daily living
Comparative Measurement: Use digital caliper measurements and compare to contralateral normal digits
Associated Findings: Look for syndactyly, café-au-lait spots (neurofibromatosis), vascular malformations
Growth Monitoring: Serial measurements and photographs to document progression
Functional Impairment
Functional deficits vary with the degree of enlargement and digits involved. Common functional problems include difficulty with fine motor tasks, reduced grip strength due to abnormal digit mechanics, impaired pinch when the thumb or index finger is involved, and psychosocial concerns related to appearance. As the child grows, the enlarged digit may interfere with activities such as writing, using utensils, and keyboard use.
Nerve Function
Despite the massive enlargement of the peripheral nerve, neurological function is typically preserved. Sensory examination usually reveals normal two-point discrimination, though some patients may report hyperesthesia or altered sensation. Motor function of intrinsic muscles supplied by the affected nerve is generally normal unless there has been prior surgical intervention.
Investigations
Radiographic Evaluation
Original description and radiographic classification of macrodactyly
- Defined the static versus progressive growth dichotomy that remains the standard classification
- Radiographic hallmarks: soft-tissue enlargement, widened/thickened phalanges, splayed epiphyses
- Advanced skeletal maturation of the affected digit relative to adjacent normal digits
Plain radiographs of the hand are essential for initial assessment and surgical planning. Anteroposterior and lateral views demonstrate characteristic features including soft tissue prominence, widened phalanges with cortical thickening, splayed epiphyses, and occasionally advanced skeletal maturation in the affected digit compared to adjacent normal digits.
Serial radiographs allow monitoring of growth velocity and timing of epiphysiodesis. The bone age of the affected digit may be advanced compared to the chronological age, particularly in progressive macrodactyly. Measurement of phalangeal width, length, and angulation should be documented for comparison over time.
Advanced Imaging
Magnetic resonance imaging (MRI) provides detailed soft tissue characterization and surgical planning information. MRI demonstrates the extent of fibrofatty infiltration, nerve enlargement with intraneural lipomatosis (characteristic high signal on T1-weighted images), vascular anatomy, and relationship of enlarged structures to joints and tendons.
MRI is particularly valuable when considering debulking procedures, as it allows precise delineation of neurovascular bundles and planning of tissue excision. Fat-suppressed sequences help differentiate lipomatous tissue from other soft tissue elements.
Vascular Studies
Ultrasound Doppler examination or MR angiography may be considered when vascular anomalies are suspected or when extensive debulking is planned. These studies identify the course of digital arteries, assess for arteriovenous malformations, and help predict vascular complications during surgery.
Differential Diagnosis
Localised digital/limb gigantism has a focused differential. The discriminating feature for true macrodactyly is enlargement of all tissue elements in a nerve-territory distribution with intraneural lipomatosis.
- clue
- All tissues enlarged; nerve-territory distribution; doughy fat
- keyTest
- MRI - intraneural lipomatous nerve (high T1); somatic PIK3CA in tissue
- distinguisher
- Enlarged tortuous nerve is the hallmark
- clue
- Cafe-au-lait macules, axillary freckling, plexiform neurofibromas, family history
- keyTest
- NF1 gene; whorled neurofibroma on MRI/histology
- distinguisher
- Plexiform neurofibroma, not simple fatty overgrowth
- clue
- Bluish/warm, compressible, bruit or thrill, may enlarge with dependency
- keyTest
- Doppler ultrasound, MR angiography
- distinguisher
- Flow voids/feeding vessels; tissue not uniformly fatty
- clue
- Diffuse pitting/non-pitting swelling, no bony enlargement
- keyTest
- Lymphoscintigraphy; normal bone on X-ray
- distinguisher
- No phalangeal widening or bone overgrowth
- clue
- Asymmetric segmental overgrowth crossing nerve territories, connective-tissue/cerebriform nevi
- keyTest
- Clinical criteria; AKT1 (Proteus) mutation
- distinguisher
- Crosses nerve territories; disproportionate, progressive, mosaic
- clue
- Capillary (port-wine) stain, varicosities, limb overgrowth
- keyTest
- Imaging of venous/lymphatic anomaly
- distinguisher
- Capillary-venolymphatic malformation with limb hypertrophy
Macrodactyly of the Foot and Toes
Although the classic teaching centres on the hand, macrodactyly of the foot is a distinct clinical problem that this topic's own evidence base repeatedly invokes - the enlargement follows the plantar nerve territories (medial plantar more often than lateral plantar), and the second toe is the most commonly affected, frequently with adjacent-toe involvement. The functional priorities differ fundamentally from the hand: the goal is not fine dexterity but a plantigrade foot that fits into a normal shoe and allows painless weight-bearing. A grotesquely enlarged toe causes footwear difficulty, ambulation problems, ulceration over pressure points and psychosocial distress rather than loss of pinch or grip.
Because the functional cost of losing a toe is far lower than losing a finger, surgeons hold a lower threshold for ray resection/amputation in the foot than in the hand, and preserving a normal-width forefoot is often prioritised over preserving the number of digits. The reconstructive ladder mirrors the hand - staged soft-tissue defatting, epiphysiodesis or physeal ablation to arrest length, shortening/narrowing osteotomies, and terminal (Syme-type) amputation of the distal phalanx - but is deployed with footwear and forefoot width as the endpoints. The same PIK3CA/PROS biology underlies both, and the two-stage defatting-plus-phalangectomy strategy validated in the hand was applied to toes in the same historic series. Microsurgical composite (toenail flap) reconstruction has more recently been described as an alternative to amputation for the severely enlarged toe.
When macrodactyly presents in the foot, restructure your priorities around shoe-fitting and painless ambulation, not dexterity. The second toe is most often involved and the pattern follows the plantar (not median/ulnar) nerves. Ray resection is far better tolerated than in the hand, so a non-salvageable, footwear-limiting toe is a legitimate early candidate for ray amputation rather than repeated debulking; epiphysiodesis is still timed to the expected adult length so the reconstructed forefoot matches the contralateral side.
Fibrolipomatous Hamartoma of Nerve (Macrodystrophia Lipomatosa)
The "grossly enlarged, lipomatous nerve" that this topic calls pathognomonic is itself a named entity: fibrolipomatous hamartoma of nerve (also termed lipofibromatous hamartoma, neural fibrolipoma, or - when it drives bony overgrowth - macrodystrophia lipomatosa). It is a benign, non-neoplastic proliferation of mature fibrofatty tissue within the epineurium and perineurium, infiltrating between and separating the nerve fascicles. The median nerve is by far the most common site (with a predilection for the volar wrist and hand), which is exactly why median-territory macrodactyly predominates. When the process also stimulates overgrowth of the underlying bone and soft tissue in a nerve-territory distribution, the digit becomes macrodactylous.
A key clinical point the topic implies but never states: the infiltrated median nerve can produce a compression neuropathy (carpal tunnel syndrome) as the fatty bulk enlarges within the carpal canal - macrodactyly and nerve compression can coexist. The MRI appearance is effectively diagnostic: on axial images the low-signal nerve fascicles surrounded by high-signal T1 fat give a "coaxial cable" appearance, and on the coronal/longitudinal plane the fascicles running through fat produce a "spaghetti" pattern; the fatty component suppresses on fat-saturated sequences. Because the picture is so characteristic, biopsy is usually unnecessary.
Management is dictated by the intimate involvement of the fascicles: do not attempt complete excision of the mass, because the hamartoma is inseparable from the functioning nerve and radical resection risks devastating sensorimotor loss. Treatment is symptom-directed - carpal tunnel/nerve decompression for compressive symptoms and careful debulking of the fibrofatty tissue while preserving the nerve - which aligns precisely with this topic's core operative principle of nerve preservation over aggressive resection.
An enlarged median nerve with a "coaxial cable" (axial) / "spaghetti" (coronal) fatty appearance on MRI is fibrolipomatous hamartoma of nerve; when it drives digital overgrowth it is macrodystrophia lipomatosa - the substrate of macrodactyly. The MRI is diagnostic, so biopsy is usually not needed, and the nerve must never be radically excised - manage the compressive carpal tunnel syndrome by decompression and debulk fat while preserving fascicles.
Management
Goals and Strategy
Surgical management is challenging and demands meticulous planning. The goals are to improve function, enhance appearance, control progression, and above all preserve neurovascular structures. Core principles:
- Staged, not single-stage: multiple sequenced procedures across childhood outperform one radical operation.
- Function over cosmesis: preserve a sensate, mobile digit where possible.
- Half-at-a-time soft-tissue rule: debulk only one side of a digit per stage to protect the dominant neurovascular bundle and skin perfusion.
- Set expectations early: recurrence is common, particularly in the progressive type.
STEPMacrodactyly Surgical Timeline
Hook:Think of the STEPS through childhood - each stage has its own procedure
Management Algorithm
Complications
Surgical Complications
Neurovascular Injury: Most feared complication during debulking; requires meticulous dissection with loupe magnification
Recurrence: Occurs in 30-50% after soft tissue debulking; plan for staged revisions from outset
Joint Stiffness: Common after extensive soft tissue procedures; aggressive hand therapy essential
Skin Necrosis: Risk with excessive skin excision or tension; plan incisions carefully with tissue viability in mind
Nerve Dysesthesia: May occur after neurolysis; usually temporary but counsel families preoperatively
Early complications include wound healing problems (skin edge necrosis, dehiscence, infection), neurovascular injury (digital nerve or artery damage during dissection), and compartment syndrome (rare but possible with extensive debulking). Late complications include recurrence of soft tissue overgrowth (particularly in progressive type), joint stiffness and contracture, growth disturbance if physes are injured, and chronic pain or hypersensitivity.
Functional Outcomes
Functional outcomes are variable and depend on multiple factors including type (static versus progressive), extent of involvement, number and type of procedures performed, and patient compliance with therapy. Static macrodactyly generally achieves better functional outcomes than progressive type. Early intervention with staged procedures tends to yield better results than delayed single-stage radical debulking.
Long-term studies report that 60-70% of patients achieve good to excellent functional outcomes with preserved sensation, useful range of motion, and acceptable cosmesis. However, recurrence requiring additional procedures occurs in 30-50% of cases, particularly in progressive macrodactyly. Patient and family satisfaction correlates more closely with realistic expectation-setting than with objective functional measures.
Guidelines, Registries & Global Practice
Macrodactyly is too rare to feature in arthroplasty registries, and there are no formal society guidelines or randomised trials - practice is guided by expert consensus and case series across centres worldwide.
Global Epidemiology
- Estimated incidence about 1 in 100,000 live births; roughly 1% of congenital upper-limb anomalies.
- No clear sex or ethnic predilection; around 70% unilateral.
- Median-nerve territory predominates (about 80%), index and middle fingers most affected.
Side-by-Side Practice Positions
- focus
- Staged debulking, function over cosmesis, nerve preservation
- position
- Surgery is first-line for the localised digit; ray amputation for non-salvageable border digits
- focus
- Skeletal control - epiphysiodesis and osteotomy timing
- position
- Time length-control to predicted adult digit length; stable fixation in older children
- focus
- Molecular diagnosis and screening
- position
- Test overgrowth tissue for PIK3CA; screen for wider PROS phenotype
- focus
- PI3K-alpha inhibition (alpelisib)
- position
- Reserve targeted drugs for severe/diffuse PROS; not standard for isolated digits
High- versus Limited-Resource Practice
- High-resource settings: multidisciplinary clinics (paediatric hand/plastic surgery, occupational therapy, clinical genetics, psychology), MRI-based planning, access to molecular testing and - selectively - PI3K-inhibitor trials.
- Limited-resource settings: diagnosis is clinical and radiographic; staged debulking and osteotomy remain feasible and effective, while MRI, genetic testing and targeted drugs may be unavailable. Early ray amputation of a non-functional digit can be a pragmatic single-stage solution where repeated staged surgery and long follow-up are impractical.
Long-term follow-up into adolescence and early adulthood is important everywhere for monitoring recurrence and psychosocial outcomes, with planned transition to adult hand services.
Controversies & Areas of Uncertainty
- Optimal first-operation timing: Most advocate early debulking (ages 2-4) to limit functional/psychosocial impact, but earlier surgery carries higher technical difficulty and recurrence; some delay until clearer functional deficit emerges. No randomised data exist - all guidance is Level IV.
- Debulking versus early ray amputation for border digits: Repeated debulking has diminishing returns and a 30-50% recurrence rate; some argue early ray amputation of a non-functional border digit gives a better, single definitive result. Decision remains individualised and value-sensitive.
- Role and timing of nerve management: How aggressively to neurolyse or even resect-and-graft the lipomatous nerve is debated, trading bulk reduction against sensory loss; many now favour preserving the nerve and accepting residual bulk.
- Targeted medical therapy: PI3K-alpha inhibitors (alpelisib) are transformative for diffuse PROS, but their role - if any - in isolated digital macrodactyly, plus long-term safety in growing children and how they integrate with surgery, is unresolved.
- Molecular testing in routine practice: Whether every isolated macrodactyly warrants PIK3CA testing (and on which tissue) versus reserving it for atypical/syndromic cases is not standardised across centres.
Viva Scenarios
At a Glance
Macrodactyly is a rare congenital disorder characterized by localized overgrowth of all mesenchymal elements of a digit or digits, resulting in disproportionate enlargement. The condition typically follows a nerve territory distribution, most commonly affecting the median nerve territory. Management requires careful timing of interventions, with staged debulking procedures and possible ray amputation for severe cases. Early recognition and multidisciplinary planning optimize functional and aesthetic outcomes.
BONES FatMacrodactyly Tissue Elements
Hook:Remember what gets BIG in macrodactyly - BONES and Fat are the key players
STOP GrowthBarsky Classification
Hook:Static growth STOPs being proportional, Progressive growth doesn't STOP
DEARSSurgical Options for Macrodactyly
Hook:DEARS - staged surgery for our DEAR patients with macrodactyly
Core Exam Knowledge
- Pathognomonic feature: Enlargement follows nerve territory distribution (median nerve in 80% of cases)
- Two clinical types: Static (present at birth, proportional growth) versus progressive (accelerated growth with age)
- Hallmark histology: Fibrofatty proliferation of all tissue elements including bone, nerve, vessels, and subcutaneous tissue
- Critical surgical principle: Staged procedures preferred over single-stage radical debulking to preserve neurovascular structures
- Definitive treatment debate: Debulking versus ray amputation depends on functional deficit and patient age
- Key differential: Distinguish from hemihypertrophy, neurofibromatosis, vascular malformations, and lymphedema
Classification Framework: Know Barsky classification (static versus progressive) and affected nerve territories
Surgical Timing: Multiple staged procedures starting at 2-4 years, with epiphysiodesis before skeletal maturity
Complications to Memorize: Joint stiffness, neurovascular injury, recurrence, growth disturbance, functional loss
Molecular Basis: Isolated macrodactyly is part of the PIK3CA-Related Overgrowth Spectrum (PROS); somatic mosaic activating PIK3CA mutations drive the overgrowth, opening the door to targeted PI3K inhibition
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 3-year-old boy presents with enlargement of the index and middle fingers present since birth. The fingers are functional but parents are concerned about appearance and anticipate functional problems as he grows. How would you assess and manage this patient?”
“A 7-year-old girl with known macrodactyly affecting her ring and small fingers has had two previous debulking procedures. The digits continue to grow disproportionately and now interfere with hand function. Parents ask about further options. How would you counsel them?”
“A 2-year-old has isolated macrodactyly of the index finger. The parents ask whether this is genetic, whether their next child is at risk, and whether there is any 'medicine' rather than surgery. How do you respond?”
Definition and Pathognomonic Features
- Localized gigantism of all mesenchymal tissue elements following nerve territory distribution (median nerve 80%)
- Hallmark histology: fibrofatty proliferation with intraneural lipomatosis
- Incidence: 1 in 100,000 live births
Classification - Barsky Types
- TYPE I (Static, 60-70%): Full manifestation at birth, proportional growth
- TYPE II (Progressive, 30-40%): Accelerated disproportionate growth
- Also classified by nerve territory (median/ulnar/radial) and anatomic extent (digital/metacarpal/forearm)
Clinical Presentation Pearls
- Digital enlargement from birth or early childhood, doughy feel due to subcutaneous fat, follows nerve distribution
- Median territory: index and middle fingers
- Ulnar territory: ring and small fingers
- Function typically preserved despite appearance
Investigation Protocol
- Plain radiographs (AP/lateral): widened phalanges, splayed epiphyses, advanced bone age
- MRI: extent of fibrofatty infiltration, nerve enlargement (high T1 signal), surgical planning
- Vascular studies if planning extensive debulking
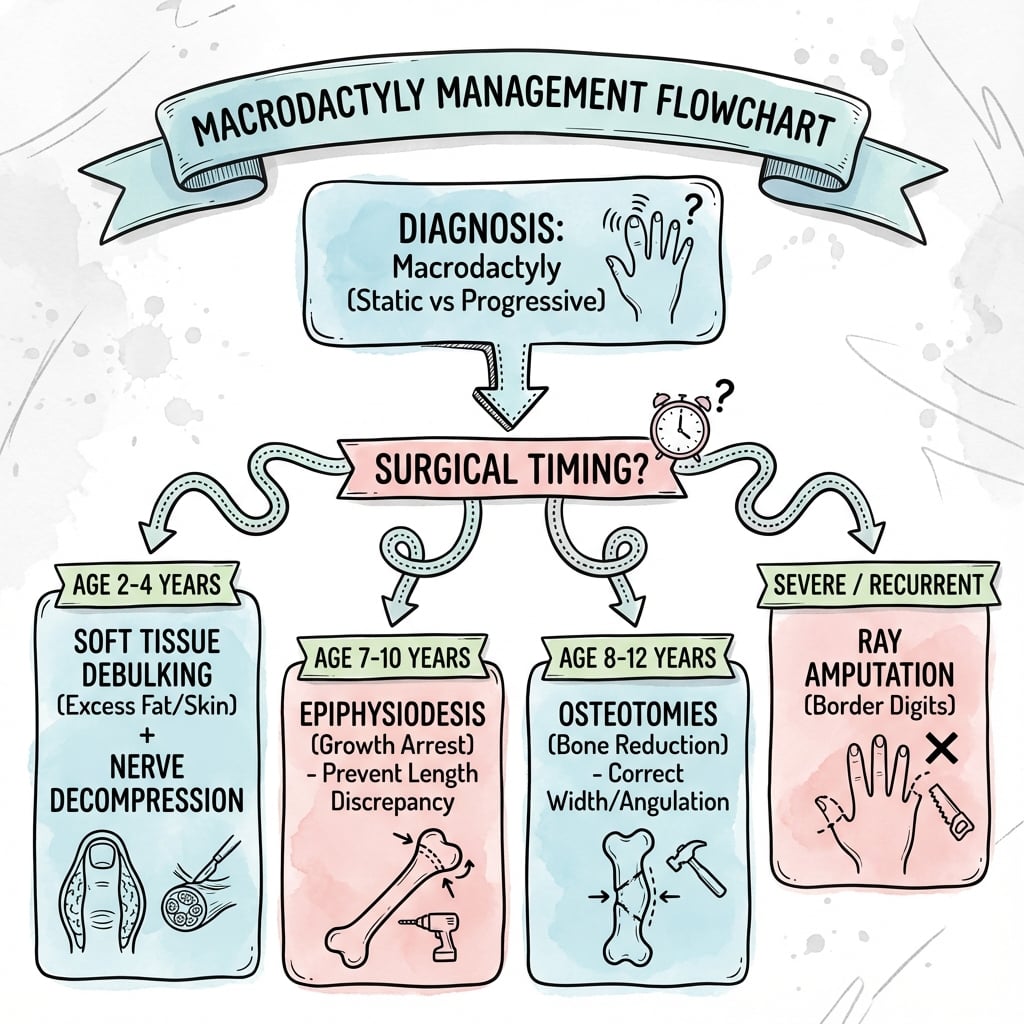
Surgical Treatment Algorithm
- STAGED APPROACH preferred
- Ages 2-4 years: First soft tissue debulking
- Ages 7-10 years: Epiphysiodesis to control length
- Ages 8-12 years: Skeletal procedures (osteotomies)
- RAY AMPUTATION: Severe deformity, border digits, failed debulking, progressive type
Key Complications
- Recurrence (30-50%, especially progressive type)
- Neurovascular injury during debulking
- Joint stiffness post-surgery
- Skin necrosis with excessive excision
- Nerve dysesthesia after neurolysis
- Growth disturbance if physes injured
Differential Diagnosis
- Neurofibromatosis (café-au-lait spots, family history, plexiform neurofibromas)
- Hemihypertrophy (crosses nerve territories)
- Vascular malformations (AVM, lymphatic)
- Proteus syndrome (connective tissue nevi, asymmetric overgrowth)
- Lymphedema (pitting edema, no bone involvement)
Viva Talking Points
- Emphasize nerve territory distribution as pathognomonic
- Discuss staged versus single-stage approach (staged preferred)
- Know epiphysiodesis timing (ages 7-10 years)
- Ray amputation indications (border digits, failed debulking)
- Recurrence common, set realistic expectations
- Multidisciplinary approach essential
Evidence Base & Key Literature
The evidence for macrodactyly is dominated by Level IV case series and expert opinion - there are no randomised trials, reflecting the rarity of the condition. The most important recent shift is the molecular reclassification of macrodactyly within the PIK3CA-Related Overgrowth Spectrum (PROS), which has opened targeted medical therapy as a research direction.
PROS consensus: diagnostic and testing framework
- NIH consensus that unified macrodactyly, CLOVES, FAO and related entities under the umbrella term PROS
- Defined clinical diagnostic features and eligibility criteria for PIK3CA molecular testing
- Recommended testing affected (overgrowth) tissue rather than blood given somatic mosaicism
Systematic review: surgical and pharmacological treatment of PROS
- 16 studies synthesised; surgery beneficial mainly for the localised macrodactyly subgroup of PROS
- PI3K/mTOR pathway inhibition reduced hypertrophy and systemic symptoms across studies
- Overall evidence quality limited (mostly retrospective, medium risk of bias)