Zone I Extensor Tendon Injury
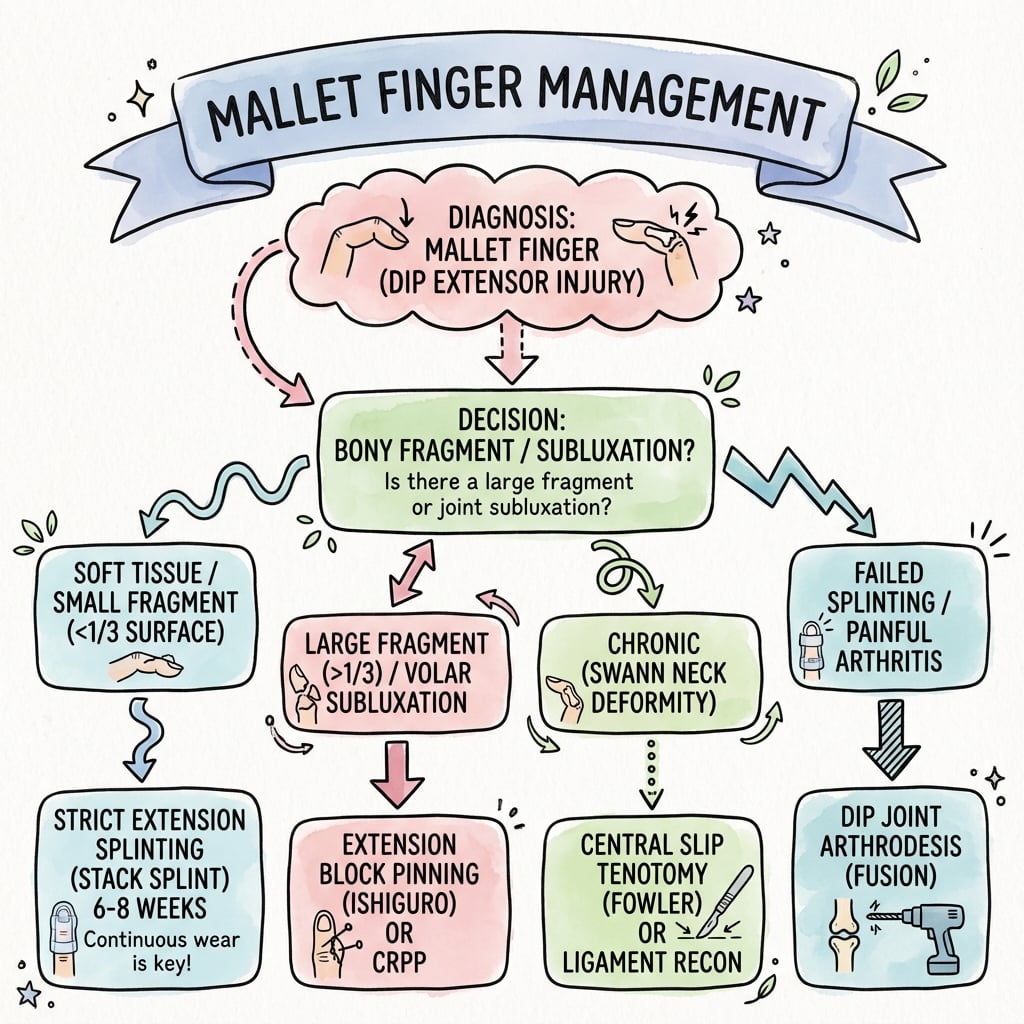
- Conservative management (Splinting) is effective for MOST cases, including Bony Mallet.
- Surgery is indicated for DIPJ subluxation (volar) or large fragments (greater than 30-50%).
- Splinting must be CONTINUOUS. If the finger flexes once, the clock resets.
- Swan Neck Deformity develops due to proximal retraction of the central slip (Fowler's mechanism).
- Ishiguro Extension Block Pinning is the standard minimal invasive technique for bony mallet.
- “A lag of less than 10 degrees is functionally acceptable.
- “Dorsal skin necrosis is the most common complication of splinting (check the fit!).
- “Antibiotics are required for open injuries (Type II/III).
Skin Necrosis The dorsal skin over the DIPJ is extremely thin. Tight splints (especially dorsal splints or taped Stacks) can cause pressure necrosis. This turns a closed simple injury into a complex soft tissue defect.
Hygiene & Fit Instruct the patient to clean the finger daily while supported in extension. Check the splint for blanching points. Use a slightly looser splint with perforation for aeration.
- Pathology
- Tendon Rupture
- Treatment
- Splint 6-8w
- Prognosis
- Good
- Pathology
- Avulsion #
- Treatment
- Splint 6w (Bony union fast)
- Prognosis
- Good (Remodels)
- Pathology
- Volar Subluxation
- Treatment
- Surgery (Ishiguro)
- Prognosis
- Variable (OA risk)
- Pathology
- Scarred/Long
- Treatment
- Re-splint or Tenotomy
- Prognosis
- Fair
VOLTSwan Neck Component
Hook:It takes VOLTage to snap into Swan Neck.
Overview
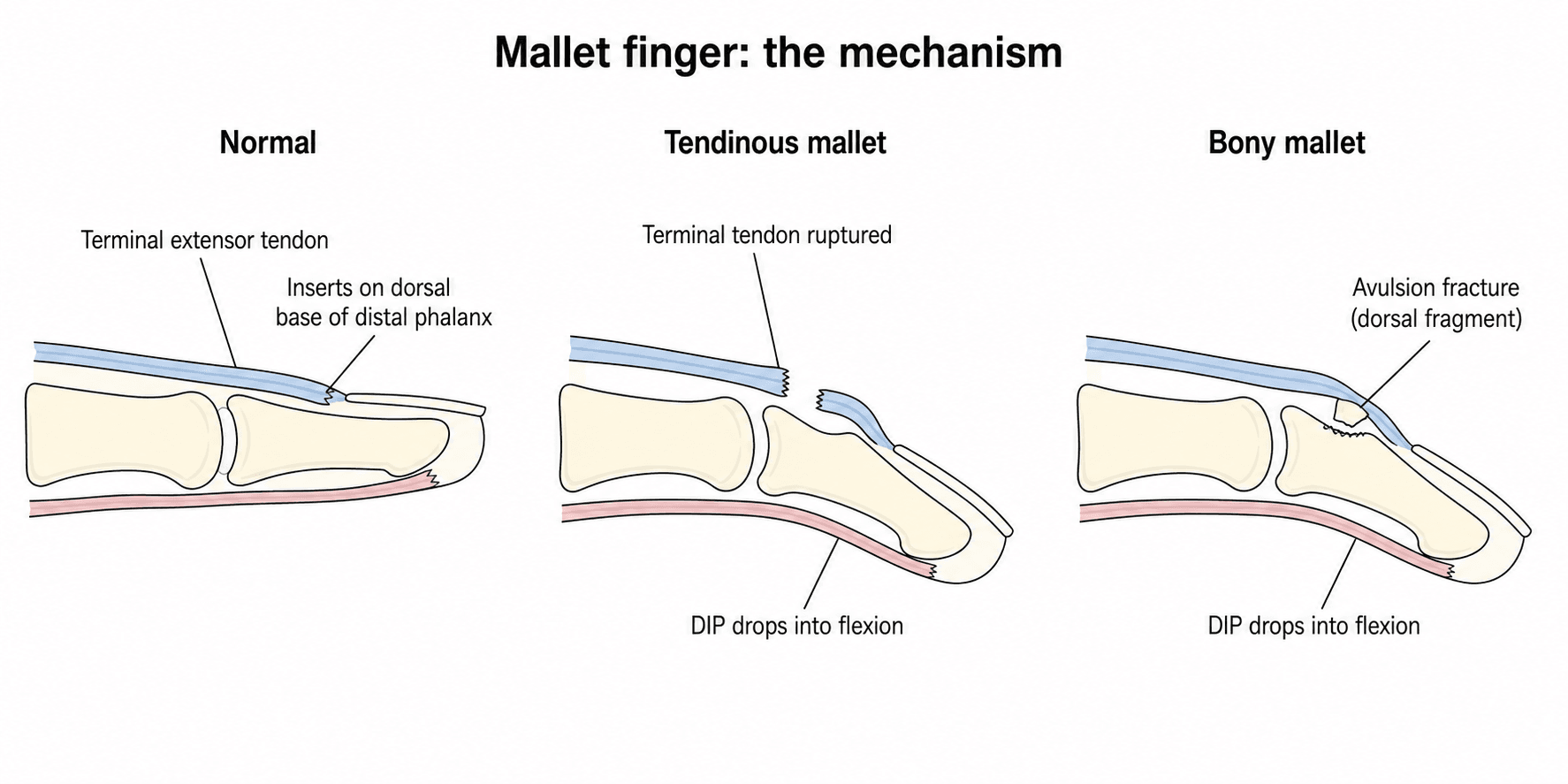
Mallet Finger is the disruption of the terminal extensor tendon at its insertion into the base of the distal phalanx (Zone I). It results in the inability to actively extend the DIPJ (extensor lag), while passive extension remains intact.
It is commonly caused by a "jamming" injury (e.g., basketball hitting the tip of the extended finger). The force force-flexes the DIPJ against extensor resistance, snapping the tendon or avulsing bone.
Pathophysiology and Mechanisms

Extensor Apparatus
- Terminal Tendon: Formed by the confluence of the two lateral bands. Inserts into the dorsal lip of the distal phalanx.
- Central Slip: Inserts into the middle phalanx.
- Triangular Ligament: Prevents lateral bands from subluxing volarly.
- Oblique Retinacular Ligament (ORL): Links PIPJ extension to DIPJ extension.
The terminal tendon is wide and wafer thin (less than 1mm).
Classification Systems
Doyle Classification
- Type I: Closed tendinous injury. (Most common).
- Type II: Open injury (Laceration).
- Type III: Open injury with loss of skin/tendon substance.
- Type IV: Mallet Fracture.
- IVa: Pediatric (Salter-Harris Physeal injury).
- IVb: Adult, less than 30% articular surface.
- IVc: Adult, greater than 30% articular surface / Subluxed.
Type IVc is the most debated category regarding surgical management.
COATDoyle Classification
Hook:Wear a COAT for the cold finger.
Clinical Presentation
The classic presentation is a patient who jammed the tip of an extended finger and now cannot straighten the last joint. The fingertip droops into flexion and will not actively lift, although it can be passively pushed straight.
- Typical patient: young athlete after a ball-sport injury, or an older adult after a trivial knock (e.g. tucking in a bedsheet).
- Hallmark sign: extension lag at the DIPJ with preserved passive extension.
- Acute features: dorsal swelling, tenderness and bruising over the DIPJ; in bony mallet a palpable step or fragment.
- Red flags: any skin breach (open/Type II-III), a flexed bleeding fingertip in a child (Seymour fracture), or a developing swan-neck posture at the PIPJ.
History
History Factors
- Mechanism: Jamming vs Laceration.
- Timing: Acute (less than 4 weeks) vs Chronic (greater than 4 weeks).
- Occupation: Surgeon/Musician (needs perfect glide) vs Labourer (needs stable union).
Late presentation (greater than 4 weeks) can still be treated with splinting.
Examination
Physical Exam
- Look: Drooping DIPJ. Erythema/Swelling (acute).
- Move:
- Active: Loss of active extension (Lag).
- Passive: Full passive extension (rules out locked joint/fracture block).
- Swan Neck: Check for PIPJ hyperextension.
- Open: Check for laceration (don't miss a Type II).
Always document the rotational alignment of the finger.
Investigations
Radiology
- Views: PA and True Lateral.
- Findings:
- Avulsion: Triangular fragment from dorsal base of P3.
- Subluxation: Volar subluxation of P3 relative to P2 head. (Surgical Indication).
- Apposition: Gap between fragment and bone.
A "True Lateral" is essential to assess joint congruency.
Mallet Thumb
The thumb has its own, much rarer, version of the injury - mallet thumb - which examiners like to contrast with the finger lesion.
- The tendon is different: extension of the thumb IP joint is driven by the terminal insertion of the extensor pollicis longus (EPL). A mallet thumb is therefore an EPL terminal disruption (closed avulsion, laceration, or a bony avulsion of the dorsal distal phalanx) producing an IP-joint extension lag.
- Lower splinting success: unlike the finger's thin terminal slip, EPL has a strong, more proximal muscle belly with greater excursion that tends to retract a ruptured tendon, so closed extension splinting is less reliable and there is a lower threshold for primary repair - particularly for open injuries and displaced bony fragments.
- Same principles otherwise: a true lateral radiograph, attention to joint congruency/subluxation, and IP extension immobilisation for stable closed or undisplaced bony injuries.
A mallet thumb is a terminal extensor pollicis longus injury at the IP joint, not the finger's thin terminal slip. Because EPL has a powerful, more proximal muscle belly that retracts a ruptured tendon, closed splinting is less reliable than in the finger and there is a lower threshold for primary repair or fixation of a displaced bony fragment.
Differential Diagnosis
The "drooped fingertip" is not always a terminal extensor injury. Distinguishing these saves a patient from being splinted for a problem a splint cannot fix.
- Key distinguishing feature
- Extension lag, jamming mechanism
- Passive DIPJ extension
- Full
- Pitfall
- Missing an associated open laceration (Type II)
- Key distinguishing feature
- Avulsion fragment or physeal widening on X-ray
- Passive DIPJ extension
- Full unless blocked
- Pitfall
- Treating a Seymour fracture as a simple closed mallet
- Key distinguishing feature
- Extensor tendon subluxes off MCPJ; lag at MCPJ not DIPJ
- Passive DIPJ extension
- N/A (MCPJ problem)
- Pitfall
- Confusing extensor lag location
- Key distinguishing feature
- Loss of active DIPJ flexion, not extension
- Passive DIPJ extension
- Full
- Pitfall
- Mixing up the flexed-droop with a flexion-loss injury
- Key distinguishing feature
- Pain and mechanical block on passive extension
- Passive DIPJ extension
- Restricted / blocked
- Pitfall
- Forcing a splint onto a joint that cannot passively extend
- Key distinguishing feature
- Palpable cord, no acute injury
- Passive DIPJ extension
- Restricted
- Pitfall
- Attributing chronic contracture to a recent jam
Management Algorithm

Conservative (Splinting)
- Indication: Type I, II, III, IVb (Stable).
- Protocol:
- Initial: 6-8 weeks CONTINUOUS extension. (Reset clock if flexed).
- Weaning: 2-4 weeks night splinting + sports/heavy use.
- Type: Stack Splint (off the shelf) or Custom Thermoplastic.
- Outcome: 80-90% success. 5-10 degree lag is common but functional.
Patient education is the single most important factor in success.
Surgical Considerations
Ishiguro Extension Block Pinning
- Concept: Uses the P2 head as a backstop.
- Step 1: Flex DIPJ. Insert 1.0mm K-wire into distal P2 head, aimed dorsally.
- Step 2: Extend DIPJ. The fragment hits the wire and is reduced onto the P3 base.
- Step 3: Insert a second longitudinal K-wire across DIPJ to lock flexion.
- Pros: Percutaneous. No dissection.
- Cons: Pin track infection. Wire migration.
The blocking wire must be placed dorsal to the fracture fragment.
LOSSSurgical Indications
Hook:Surgery prevents LOSS of the joint.
Chronic Mallet: Beyond Tenodermodesis
Tenodermodesis is one option for the chronic symptomatic mallet, but examiners expect two further named procedures - especially once a swan-neck deformity has developed.
- Fowler central slip tenotomy: for the chronic mallet that has produced (or threatens) a swan-neck deformity with a supple PIP joint. The central slip is divided over the proximal part of the middle phalanx, releasing the proximal extensor tether so that more extensor force is transmitted distally to the terminal tendon - improving the DIP lag while letting the hyperextended PIP drop back. A small (around 10-15 degree) residual PIP extensor lag is accepted; a true boutonniere is the feared over-correction.
- Oblique retinacular ligament (Spinner-Choi) reconstruction: a tendon graft (a lateral band or free graft) routed from the volar proximal phalanx, volar to the PIP axis, to the dorsal distal phalanx. Acting as a dynamic tenodesis, it simultaneously extends the DIP and restrains PIP hyperextension - addressing both components of the mallet-driven swan neck at once.
- Joint-level salvage: a painful, arthritic or grossly unstable chronic DIP is often best treated by DIP arthrodesis rather than soft-tissue reconstruction.
For a chronic mallet that has driven a swan-neck deformity with a supple PIP, the oblique retinacular ligament (Spinner-Choi) reconstruction is attractive because a single dynamic tenodesis both restores DIP extension and blocks PIP hyperextension. The Fowler central slip tenotomy is the simpler alternative that rebalances the extensor mechanism, accepting a small PIP lag while avoiding a boutonniere.
Complications
- Skin Necrosis: From tight splint. Most common.
- Nail Deformity: Ridging from germinal matrix injury (by splint or fracture).
- Recurrence: If splint removed too early.
- Stiffness: Loss of flexion. Often worse than the original 10 degree lag.
- Septic Arthritis: From pin track infection.
- Functional Deficit: Most patients adapt well to a minor lag, but cannot adapt to a stiff, painful joint.
- Hypersensitivity: Common at the fingertip. Desensitization therapy is needed.
Rehabilitation
- Splint: Strict extension (0 degrees). Maintain 24/7 contact with dorsal DIPJ.
- Hygiene: Clean finger while supported in extension - use support finger or splint.
- PIPJ: Active PIPJ ROM (flexion/extension) - prevent stiffness.
- Monitoring: Check splint fit weekly. Look for blanching, pressure marks.
- Education: Explain that ONE flex episode resets the clock.
- Assess: Measure active extension. If lag less than 10 degrees, proceed.
- Active ROM: Start gentle active flexion (20-30 degrees initially).
- Splint: Night splinting continues. Wear for heavy tasks, sports.
- Progression: Increase flexion by 10 degrees per week.
- Full ROM: Expect full DIPJ flexion by 10-12 weeks.
- Strengthening: Putty exercises, grip strengthening.
- Return to Sport: Usually 10-12 weeks for non-contact, 12-16 for contact.
- Full Activity: Unrestricted by 12-16 weeks.
- Lag Management: Slight recurrence of lag (5-10 degrees) is common and acceptable.
- Re-splint Threshold: If lag exceeds 15 degrees, restart 2-week splint protocol.
- Long-term: Scar massage, desensitization if hypersenitive.
Key Rehabilitation Principles:
- Continuous splinting is essential - even brief flexion can undo weeks of healing
- Patient education is the single most important factor in outcome
- Monitor skin - dorsal skin necrosis is avoidable with proper splint fit
- PIPJ exercises prevent stiffness and Swan Neck progression
Prognosis
Outcomes by Treatment Type
- Success Rate: 80-90% achieve good/excellent results
- Residual Lag: Average 5-10 degrees (functionally acceptable)
- Patient Satisfaction: High, especially with compliant patients
- Return to Work: 85% return to pre-injury occupation
- Success Rate: 70-80% (higher complication rate offsets benefits)
- Complications: Nail deformity (15%), infection (5-10%), stiffness (20%)
- Indication: Reserved for subluxed joints or failed splinting
- Compliance: Single most important variable
- Delay to Treatment: Late presentation still responds to splinting
- Age: Younger patients heal faster, elderly have thinner skin (necrosis risk)
- Comorbidities: Diabetes, smoking impair tendon healing
Compliance is the single most important predictor of outcome.
Guidelines, Registries & Global Practice
Global Epidemiology
- Mallet finger is among the most common closed tendon injuries of the hand, with a recognised peak in young men (sport-related forced flexion) and a second peak in older women (low-energy domestic injury, often involving thin dorsal skin).
- Typical mechanisms worldwide: ball-sports (basketball, volleyball, cricket, baseball, netball), bedmaking/tucking sheets, and catching a digit on clothing.
- The long, middle and ring fingers of the dominant hand are most often affected; bony mallet fractures account for a substantial minority of cases.
Side-by-Side Guideline Comparison
- First-line
- Continuous DIPJ extension splint 6-8w
- Surgical threshold
- Open injury, volar subluxation, large displaced fragment
- Notable emphasis
- Hand-therapy-led pathways, patient education
- First-line
- Extension splinting for most closed injuries
- Surgical threshold
- Subluxation or large articular fragment
- Notable emphasis
- Acceptance of small residual lag; shared decision-making
- First-line
- Splint for stable injuries
- Surgical threshold
- Unstable/subluxed fractures - extension block pinning or ORIF
- Notable emphasis
- Closed extension block (Ishiguro) as workhorse technique
- First-line
- Splint-first universally
- Surgical threshold
- Subluxation, open, failed conservative care
- Notable emphasis
- Adapting splint type to local resources
The striking feature is convergence: every major society recommends splint-first management and reserves surgery for volar subluxation, open injury, or selected large fragments. The genuine area of disagreement is the exact articular-percentage threshold (one-third versus one-half).
Registry and Outcome Notes
- There is no dedicated arthroplasty/implant registry for mallet finger, as the injury is rarely implant-based. Outcome evidence derives from RCTs, cohort series and the Cochrane review rather than national registries.
- Reported splinting success rates cluster around 80-90% acceptable outcome, with a residual extension lag of roughly 5-10 degrees that is usually functionally and cosmetically well tolerated.
High- vs Limited-Resource Practice
- Well-resourced settings: custom thermoplastic or perforated splints fabricated by hand therapists, structured education, and ready access to percutaneous pinning for subluxed fractures.
- Limited-resource or remote settings: off-the-shelf Stack splints, aluminium-foam splints, or simple thermoplastic; telehealth-supervised splinting protocols have been shown to be safe and effective where in-person therapy is scarce.
- Antibiotics for open injuries: open mallet injuries and Seymour fractures are treated as open fractures - urgent debridement plus a first-generation cephalosporin (e.g. cephalexin) with anti-staphylococcal cover, a recommendation consistent across guidelines and supported by the Seymour fracture literature.
Controversies and Areas of Uncertainty
Mallet finger looks simple but several common viva questions sit on genuinely unsettled ground. Knowing what is NOT proven is as important as knowing the protocol.
- The articular-percentage threshold. The "one-third rule" for surgery is a teaching convention, not a validated cut-off. Reviews note that size alone has never reliably predicted who benefits from surgery; congruency (absence of volar subluxation) is the more defensible determinant.
- Surgery versus splinting for displaced bony mallet. The Cochrane review found no high-quality evidence that surgery outperforms splinting, even for larger fragments, while surgery adds infection and nail-deformity risk. Many surgeons still operate on subluxed joints, but the benefit is assumed rather than proven.
- Optimal splint type and duration. No splint design has been shown clearly superior; 6 versus 8 weeks and the weaning schedule are based on tradition and small trials, not robust RCTs.
- Persistent radiographic gap. A residual fracture gap or incomplete reduction frequently coexists with excellent function - a strong argument for treating the patient, not the X-ray.
- Extension block pinning patient selection. Long dorsal-cortex fragments and older patients do worse after extension block pinning, suggesting morphology-based selection rather than a one-technique-fits-all approach.
MCQ Practice Points
Q: What structure balances the lateral bands and prevents volar subluxation? A: The Triangular Ligament.
Q: What is the primary cause of Swan Neck deformity in chronic mallet finger? A: Proximal retraction of the extensor apparatus causing increased tension on the central slip.
Q: What is the most common complication of surgical treatment for mallet finger? A: Nail deformity (ridging) and infection.
Q: A patient wearing a stack splint complains of dorsal pain and white skin. What is the action? A: Adjust/Replace splint immediately (Risk of necrosis).
Q: What percentage of articular surface involvement indicates surgery for bony mallet? A: Greater than 30-50% WITH volar subluxation. Size alone is NOT an indication - congruency is key.
Q: How long should a mallet finger be splinted? A: 6-8 weeks continuous extension, then 2-4 weeks weaning. Clock resets if finger flexes.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old presents 4 months after a mallet injury. He ignored it. Now has a 40 degree lag and finds it catchy. Examination shows a Swan Neck deformity. Management?”
“X-ray shows a mallet fracture with a fragment involving 40% of the articular surface. The joint is congruent (no subluxation). What do you do?”
“A 7-year-old crushes his finger. The nail plate is avulsed proximally (lying on top of the fold). The tip is flexed. X-ray shows a physeal widening.”
“A 65-year-old diabetic presents 3 weeks into splint treatment for a mallet finger. She has a 1cm area of full thickness skin necrosis over the dorsal DIPJ. The underlying tendon is exposed. What is your management?”
Classification
- Type I: Tendon (Splint)
- Type II: Laceration (Wash/Repair)
- Type III: Coverage loss (Flap)
- Type IV: Bony (Splint unless subluxed)
Management
- Splint: 6-8 weeks straight
- Surgery: If Subluxed or greater than 50%
- Tech: Ishiguro Pinning
- Chronic: Tenodermodesis
Complications
- Skin Necrosis (Splint)
- Nail Ridge (Surgery)
- Stiffness
- Recurrence
Evidence Base
Cochrane Review: Interventions for Treating Mallet Finger
- Four randomised/quasi-randomised trials, 278 participants with 283 mallet injuries
- Three trials compared different finger splints versus a standard Stack splint
- One RCT found no significant difference between Kirschner-wire fixation and a Pryor-and-Howard splint, with similar complication rates
- All trials were methodologically flawed; insufficient evidence to define when surgery is indicated
Diagnosis and Management of Mallet Finger Injuries
- Narrative review of epidemiology, diagnosis and management focused on surgical indications
- Non-operative management is advocated for almost all mallet injuries
- Surgery is generally reserved for fractures involving more than one-third of the articular surface and for volar subluxation of the distal phalanx
- A clear advantage of surgery even in these complex cases has not been proven