Radiological Assessment of Osteoporosis, Paget's, Hyperparathyroidism and Renal Osteodystrophy
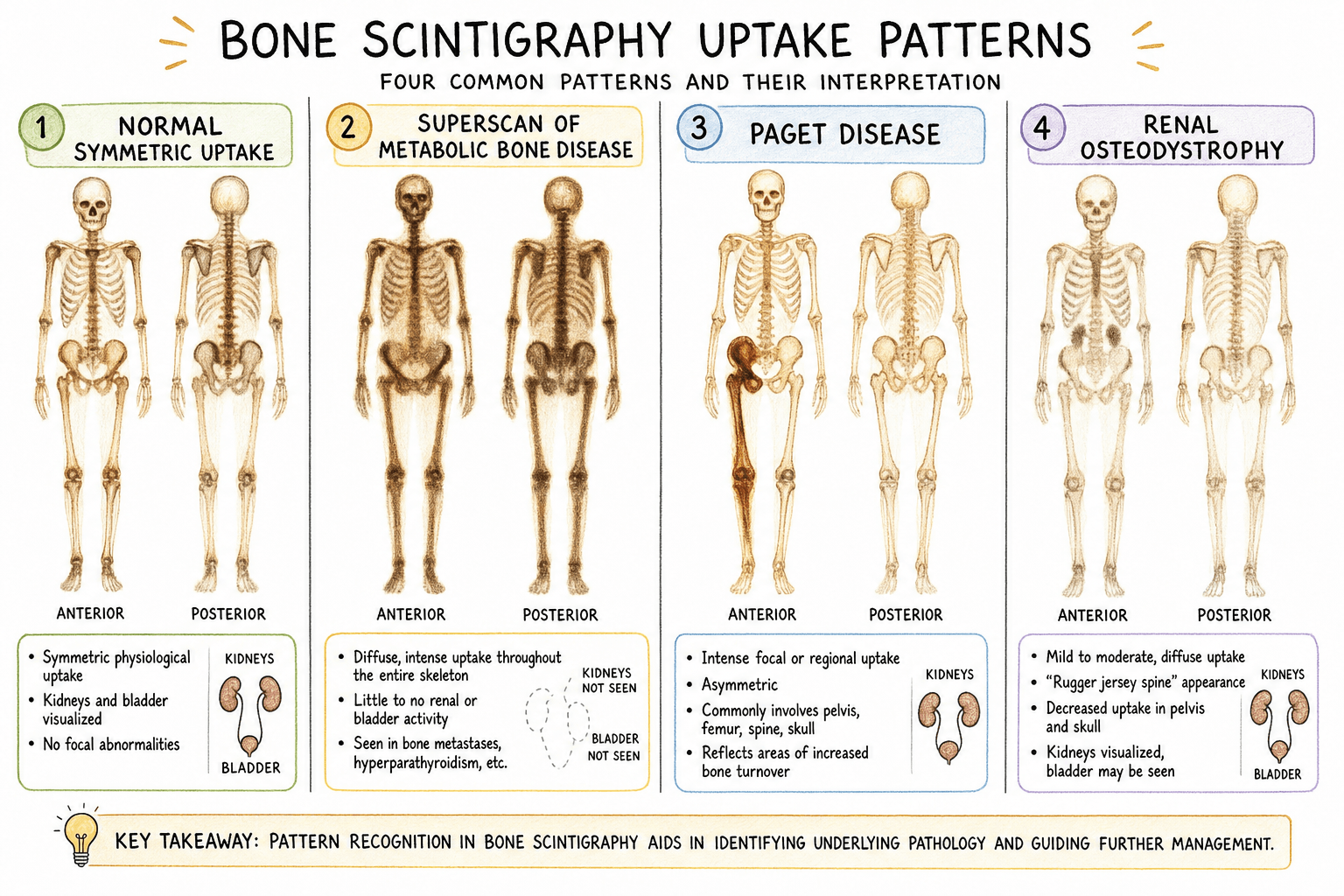
Superscan: Diffuse uptake, no kidneys (metastases or metabolic)
Paget's: Intense uptake, enlarged bone, monostotic or polyostotic
HPT: Diffuse uptake + focal brown tumours
Key: Superscan with uniform uptake favours metabolic; heterogeneous favours metastases
- Osteoporosis: Decreased density, vertebral fractures, cortical thinning
- Paget's: Enlarged bone, coarse trabeculae, mixed lytic/sclerotic
- Hyperparathyroidism: Subperiosteal resorption, brown tumours, chondrocalcinosis
- Osteomalacia: Looser zones (pseudofractures), generalised osteopenia
- Bone scan superscan in diffuse metabolic disease
- “Rugger jersey spine: Renal osteodystrophy
- “Picture frame vertebra: Paget's
- “Cotton wool skull: Paget's (lytic then sclerotic phases)
- “Salt and pepper skull: Hyperparathyroidism
- “Codfish vertebrae: Osteoporosis with biconcave fractures
Metabolic bone disease imaging is commonly tested. Know the classic radiographic signs: Looser zones (osteomalacia), subperiosteal resorption (HPT), picture frame vertebra (Paget's). Understand how to differentiate metabolic superscan from metastatic superscan on bone scan.
QMRRThe Four Mechanisms
Hook:Renal osteodystrophy combines defective mineralisation + excess resorption + sclerosis, which is why its radiographs show mixed features.
Overview
Metabolic bone disease encompasses systemic disorders that disturb the normal balance of bone formation, resorption and mineralisation. Because the abnormality is metabolic rather than focal, the imaging signs are usually generalised and bilateral, with characteristic regional accentuation that points to a specific diagnosis. The radiologist's task is to recognise the dominant abnormality — reduced quantity of mineralised bone (osteoporosis), defective mineralisation of osteoid (osteomalacia/rickets), excessive resorption driven by parathyroid hormone (hyperparathyroidism), disordered remodelling (Paget's disease), or the mixed picture of chronic kidney disease (renal osteodystrophy).
- Calcium
- Normal
- Phosphate
- Normal
- ALP
- Normal
- PTH
- Normal
- Calcium
- Low / normal
- Phosphate
- Low
- ALP
- High
- PTH
- High (secondary)
- Calcium
- High
- Phosphate
- Low
- ALP
- High
- PTH
- High
- Calcium
- Low / normal
- Phosphate
- High
- ALP
- High
- PTH
- High
- Calcium
- Normal
- Phosphate
- Normal
- ALP
- Very high (isolated)
- PTH
- Normal
Systematic Approach to the Metabolic Bone Radiograph
A disciplined search pattern converts a vague impression of low density into a specific diagnosis. Work through the DENSITY checklist (above): density, endplates/trabeculae, notches/resorption, soft tissue, insufficiency fractures/Looser zones, tumours, and then yield to biochemistry.
- Highest-Yield Radiograph
- Hands (PA), distal clavicles
- Looking For
- Subperiosteal resorption on radial phalangeal margins, acro-osteolysis
- Highest-Yield Radiograph
- Pelvis, proximal femora, scapulae, ribs
- Looking For
- Looser zones (bilateral, perpendicular lucent bands)
- Highest-Yield Radiograph
- Lateral thoracolumbar spine + DXA
- Looking For
- Vertebral fractures (Genant grade), low BMD
- Highest-Yield Radiograph
- Affected long bone, skull, pelvis
- Looking For
- Bone enlargement, coarse trabeculae, blade-of-grass front
- Highest-Yield Radiograph
- Hands, lateral spine
- Looking For
- Subperiosteal resorption, rugger jersey spine, soft-tissue calcification
DENSITYSearch Pattern for Metabolic Bone Disease
Hook:Decide first whether the dominant abnormality is QUANTITY (osteoporosis), MINERALISATION (osteomalacia), RESORPTION (HPT) or REMODELLING (Paget's) — then confirm with the targeted signs and biochemistry.
Osteoporosis
- Description
- Decreased bone density, increased lucency
- Location
- Diffuse
- Description
- Thin cortices, endosteal scalloping
- Location
- Long bones
- Description
- Loss of horizontal trabeculae, vertical streaking
- Location
- Vertebrae
- Description
- Wedge, biconcave, or crush morphology
- Location
- Spine
- Description
- Loss of trabecular groups in proximal femur
- Location
- Hip
WBC FracturesVertebral Fracture Morphology
Hook:Greater than 20% height loss or greater than 4mm absolute loss indicates vertebral fracture. Compare with adjacent vertebrae.
Paget's Disease
- Pathophysiology
- Osteoclast predominance
- X-ray Appearance
- V-shaped lytic lesion (blade of grass), osteoporosis circumscripta (skull)
- Pathophysiology
- Osteoclast and osteoblast activity
- X-ray Appearance
- Coarse trabeculae, bone enlargement, cortical thickening
- Pathophysiology
- Osteoblast predominance
- X-ray Appearance
- Dense sclerotic bone, ivory vertebra, cotton wool skull
Hyperparathyroidism
- Description
- Lacy, irregular periosteal margin
- Location
- Radial aspect of middle phalanges (classic)
- Description
- Resorption of terminal tufts
- Location
- Distal phalanges
- Description
- Well-defined lytic lesions
- Location
- Mandible, pelvis, femur, ribs
- Description
- Calcification in cartilage
- Location
- Knee menisci, TFCC, pubic symphysis
- Description
- Diffuse granular demineralisation
- Location
- Skull vault
- Description
- Sclerotic endplates, lucent centre
- Location
- More common in renal osteodystrophy
Subperiosteal Resorption SitesHPT Classic Sites
Hook:Look at the radial aspect of the 2nd and 3rd middle phalanges - subperiosteal resorption here is virtually pathognomonic of HPT
Osteomalacia and Rickets
- Description
- Lucent bands perpendicular to cortex, bilateral, symmetric
- Significance
- PATHOGNOMONIC
- Description
- Decreased bone density
- Significance
- Non-specific
- Description
- Fuzzy, indistinct trabeculae
- Significance
- Unmineralised osteoid
- Description
- Codfish vertebrae
- Significance
- Softened bone
- Description
- Protrusio, triradiate pelvis
- Significance
- Severe disease
- Description
- Concave metaphyseal margin
- Location
- Wrist, knee (most obvious)
- Description
- Irregular, brush-like margin
- Location
- Growth plates
- Description
- Increased physeal width
- Location
- Active growth plates
- Description
- Enlarged costochondral junctions
- Location
- Anterior ribs
- Description
- Genu varum or valgum
- Location
- Lower limbs
Renal Osteodystrophy
- Cause
- Sclerotic endplates, lucent centre
- Appearance
- Horizontal banding like rugby jersey
- Cause
- Secondary HPT
- Appearance
- As in primary HPT
- Cause
- High calcium-phosphate product
- Appearance
- Vascular, periarticular
- Cause
- Secondary HPT
- Appearance
- Lytic lesions
- Cause
- Dialysis-related
- Appearance
- Bone cysts, erosions
Osteopetrosis (Marble Bone Disease)
The differential table cites "osteopetrosis (sandwich vertebra)" as the mimic to exclude for rugger jersey spine, but the disease itself is never developed. Osteopetrosis is a sclerosing bone disorder caused by FAILURE of osteoclast-mediated resorption, producing diffusely dense bone that is paradoxically BRITTLE.
- Description
- Generalised dense bone with loss of corticomedullary differentiation
- Note
- Symmetric — the hallmark
- Description
- Sharply defined, very dense sclerotic endplate bands
- Note
- Distinguish from the INDISTINCT rugger jersey spine of renal osteodystrophy
- Description
- A miniature bone within the bone
- Note
- Vertebrae, pelvis, phalanges, carpals/tarsals
- Description
- Undertubulated, flared metaphyses
- Note
- From defective metaphyseal remodelling
- Description
- Dense bone that fractures like brittle chalk
- Note
- Brittle despite the high density
Bone Scan Patterns
- Pattern
- Diffuse uptake, no kidneys
- Key Features
- Uniform, symmetric, all bones
- Pattern
- Diffuse uptake, no kidneys
- Key Features
- Heterogeneous, asymmetric foci
- Pattern
- Intense focal uptake
- Key Features
- Enlarged bone, entire bone involved
- Pattern
- Diffuse + focal
- Key Features
- Brown tumours show focal uptake
- Pattern
- Pseudofractures show uptake
- Key Features
- Looser zone sites positive
Differential Diagnosis
The classic radiographic signs of metabolic bone disease overlap with focal pathology. The decisive discriminators are distribution (generalised/symmetric vs focal), the accompanying biochemistry, and whether the affected bone is enlarged.
- Metabolic Cause
- Osteoporosis / osteomalacia
- Mimic to Exclude
- Diffuse marrow infiltration (myeloma, leukaemia)
- Discriminating Feature
- Osteomalacia has coarse trabeculae + Looser zones; myeloma shows punched-out lytic lesions and a paraprotein
- Metabolic Cause
- Brown tumour (HPT)
- Mimic to Exclude
- Metastasis, plasmacytoma, GCT
- Discriminating Feature
- Brown tumour only in proven hyperparathyroidism; check calcium and PTH
- Metabolic Cause
- Paget's disease
- Mimic to Exclude
- Sclerotic (blastic) metastasis
- Discriminating Feature
- Paget's ENLARGES bone and coarsens trabeculae; metastasis does not enlarge bone
- Metabolic Cause
- Metabolic / renal osteodystrophy
- Mimic to Exclude
- Diffuse osteoblastic metastases
- Discriminating Feature
- Metabolic uptake is uniform and symmetric; metastatic is heterogeneous and patchy
- Metabolic Cause
- Looser zone (osteomalacia)
- Mimic to Exclude
- Stress/fatigue fracture
- Discriminating Feature
- Looser zones are bilateral, symmetric, on the concave/medial side; stress fractures are unilateral and at typical sport-related sites
- Metabolic Cause
- Rugger jersey spine (renal)
- Mimic to Exclude
- Osteopetrosis (sandwich vertebra)
- Discriminating Feature
- Renal banding is indistinct; osteopetrosis bands are sharply defined and very dense
Guidelines, Registries & Global Practice
Metabolic bone disease is diagnosed and managed worldwide; imaging interpretation is universal, but access to DXA, scintigraphy and biochemistry varies markedly by resource setting.
- Epidemiology
- Most common metabolic bone disease; lifetime fragility-fracture risk roughly 1 in 2 women and 1 in 5 men over 50
- Imaging-Relevant Point
- DXA-defined; FRAX adds clinical risk factors
- Epidemiology
- Estimated 0.4-1% of adults, rising after age 55; marked geographic and declining temporal variation
- Imaging-Relevant Point
- Often incidental on CT/radiographs (Husseini 2022)
- Epidemiology
- Re-emerging with vitamin D deficiency, malabsorption and limited sun exposure; major burden in some low-resource regions
- Imaging-Relevant Point
- Looser zones and metaphyseal change are diagnostic clues
- Epidemiology
- Affects most patients with advanced CKD on dialysis
- Imaging-Relevant Point
- Hand radiographs highest yield (Lacativa 2009)
- Scope
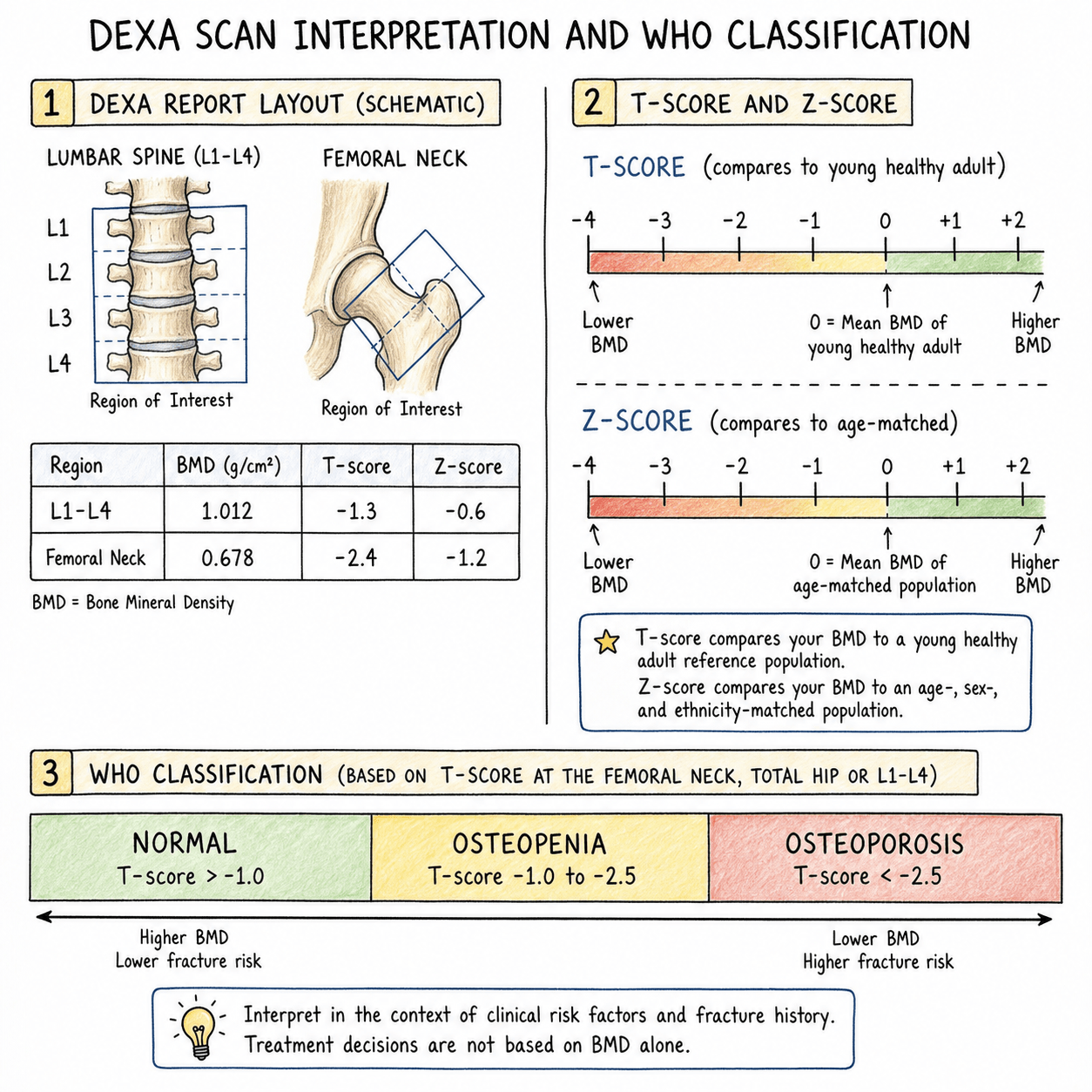
- Osteoporosis definition
- Imaging-Relevant Position
- T-score at or below -2.5 by central DXA defines osteoporosis; -1 to -2.5 osteopenia
- Scope
- Fragility fracture / osteoporosis care
- Imaging-Relevant Position
- Endorses DXA plus fracture-risk assessment and secondary-fracture prevention after fragility fracture
- Scope
- Fracture risk assessment
- Imaging-Relevant Position
- FRAX-based intervention thresholds; DXA where FRAX indicates; vertebral fracture assessment encouraged
- Scope
- Paget's disease
- Imaging-Relevant Position
- Plain radiographs for diagnosis, radionuclide bone scan to map extent, ALP to monitor; treat symptomatic disease
- Scope
- CKD-mineral and bone disorder
- Imaging-Relevant Position
- Cautions against relying on plain radiographs alone; biochemistry and selective imaging guide CKD-MBD diagnosis
Clinical Imaging
No single modality answers every question in metabolic bone disease; the modalities are complementary and each has a defined role.
- Primary Role
- Pattern recognition of qualitative signs
- Strengths / Limitations
- Shows Looser zones, subperiosteal resorption, Paget's architecture; insensitive to early density loss
- Primary Role
- Quantify bone mineral density (T-score)
- Strengths / Limitations
- Reference standard for osteoporosis diagnosis; cannot show qualitative signs or assess mineralisation
- Primary Role
- Whole-skeleton survey of turnover
- Strengths / Limitations
- Maps Paget's extent, Looser zones, brown tumours; superscan in diffuse disease; non-specific
- Primary Role
- Cortical detail, fracture and deformity
- Strengths / Limitations
- Defines Paget's cortical thickening, vertebral fractures, brown tumours; higher dose
- Primary Role
- Marrow and occult/insufficiency fractures
- Strengths / Limitations
- Sensitive for sacral and vertebral insufficiency fractures invisible on radiographs
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 70-year-old man presents with a painful, bowed tibia. X-ray shows an enlarged bone with coarse trabeculae, cortical thickening, and mixed lytic and sclerotic areas.”
“A patient with chronic kidney disease has hand X-rays showing irregular erosions along the radial aspect of the middle phalanges and loss of the lamina dura around teeth.”
“A 45-year-old woman with coeliac disease presents with bone pain. X-rays show generalised osteopenia and bilateral symmetric lucent bands perpendicular to the cortex at the medial femoral necks.”
“A 68-year-old woman is referred after a low-trauma wrist fracture. Her lumbar spine DXA reports a T-score of -1.8 but her femoral neck T-score is -2.7. Lateral spine radiograph shows a grade 2 wedge deformity at T8.”
Paget's Disease Signs
- Bone enlargement (pathognomonic)
- Blade of grass (lytic phase)
- Cotton wool skull (sclerotic)
- Picture frame vertebra
- Banana fractures
Hyperparathyroidism Signs
- Subperiosteal resorption (radial middle phalanges)
- Salt and pepper skull
- Brown tumours (lytic lesions)
- Chondrocalcinosis
- Rugger jersey spine (renal)
Osteomalacia Signs
- Looser zones (PATHOGNOMONIC)
- Bilateral, symmetric pseudofractures
- Medial femoral neck, pubic rami, scapula
- Generalised osteopenia
- Rickets: Cupping, fraying, widened physis
Bone Scan Patterns
- Metabolic superscan: Uniform, symmetric
- Metastatic superscan: Heterogeneous
- Paget's: Intense, entire bone
- Looser zones show uptake
Evidence Base
Genant Semiquantitative Vertebral Fracture Grading
- Introduced the semiquantitative (SQ) visual method that grades vertebral deformity by approximate height loss: grade 1 (mild, 20-25%), grade 2 (moderate, 25-40%), grade 3 (severe, over 40%).
- Validated in 57 postmenopausal women aged 65-75 read by three independent observers, showing the SQ approach can be applied reliably for prevalent and incident fractures when well-defined criteria are used.
- Distinguished true osteoporotic fracture morphology (wedge, biconcave, crush) from non-fracture deformity, reducing interobserver variability.
FRAX — Ten-Year Fracture Probability from Clinical Risk Factors
- Developed the WHO FRAX tool integrating clinical risk factors (age, BMI, prior fracture, parental hip fracture, glucocorticoids, rheumatoid arthritis, smoking, alcohol) with or without femoral neck BMD.
- Ten-year hip fracture probability in women varied roughly 100-fold (0.2% at age 50 without risk factors to 22% at age 80 with parental hip fracture history).
- Demonstrated that most patients who fracture do not meet the DXA T-score definition of osteoporosis, so risk-factor integration improves case-finding.