MT2 Marching Fracture | MT5 High-Risk Zones | Female Athlete Triad | MRI Gold Standard | Activity Modification
- Second metatarsal is most common site (marching fracture) - usually low-risk, conservative treatment
- Fifth metatarsal Zone 2-3 are HIGH-RISK locations - 50%+ nonunion rate, often need surgery
- MRI is gold standard for early diagnosis - X-rays negative for 2-3 weeks after symptom onset
- Female athlete triad (energy deficiency, amenorrhea, low BMD) increases stress fracture risk
- Activity modification is cornerstone - address training errors, biomechanics, nutrition
- “MT2 stress fracture = 'marching fracture' - most common, usually conservative, good prognosis
- “MT5 Zone 2-3 stress fractures = high nonunion risk = surgical fixation in athletes
- “X-ray delay: symptoms appear 2-3 weeks before radiographic changes (MRI earlier)
- “Bone scan vs MRI: MRI more specific, shows fracture line and edema pattern
- “Return to sport: 6-8 weeks for low-risk, 10-12 weeks for high-risk (MT5 Zone 2-3)
MT5 Zone 2-3 = HIGH-RISK - 50%+ nonunion, need surgery. MT2 = low-risk, usually conservative
X-rays negative for 2-3 weeks - MRI gold standard for early diagnosis before radiographic changes
Female athlete triad, training errors, biomechanics, nutrition - must address underlying causes
Low-risk (MT2-4): Activity mod. High-risk (MT5 Zone 2-3): Surgical fixation in athletes
- Risk Level
- Low risk
- Treatment
- Activity modification, CAM boot 4-6 weeks
- Key Pearl
- Most common, excellent prognosis with rest
- Risk Level
- Moderate risk
- Treatment
- NWB 6-8 weeks, bone stimulator
- Key Pearl
- Weight-bearing importance - lower threshold for surgery
- Risk Level
- HIGH RISK
- Treatment
- Surgical fixation (IM screw) in athletes
- Key Pearl
- 50%+ nonunion rate - watershed blood supply
- Risk Level
- High risk
- Treatment
- Comprehensive workup, address systemic causes
- Key Pearl
- Female athlete triad, nutrition, biomechanics
MARCHINGMARCHING - MT2 Stress Fracture Features
Hook:MARCHING fractures are the most common - Most common site, Activity modification, Rapid recovery, Conservative treatment, High success, Inferior cortex, No surgery, Gradual return
ZONEZONE - Fifth Metatarsal Risk Zones
Hook:ZONE classification determines risk - Zone 1 low risk, Zone 2-3 HIGH RISK, Nonunion risk high, Early surgery for athletes
Overview and Epidemiology
Metatarsal stress fractures are among the most common stress fractures in athletes and military recruits. The second metatarsal ("marching fracture") is the most frequent site, typically low-risk with excellent prognosis. However, fifth metatarsal Zone 2-3 stress fractures have high nonunion rates (50%+) due to watershed blood supply, requiring surgical fixation in athletes. Understanding site-specific risk and treatment algorithms is critical for exam success.
- Athletes: Runners, dancers, military recruits
- Age: Peak in young adults (late teens to 30s)
- Sex: Overall incidence similar in male and female athletes; female-specific risk is mediated by the triad (low energy availability, menstrual dysfunction, low BMD)
- Sports: Track, basketball, ballet, marching
- Training interruption: 6-12 weeks
- High-risk sites: 50%+ nonunion without surgery
- Recurrence risk: If underlying causes not addressed
- Career impact: Professional athletes need early surgery
Anatomy and Pathophysiology
The metadiaphyseal junction (Zone 2) and proximal diaphysis (Zone 3) of the fifth metatarsal represent a watershed zone where nutrient artery supply meets periosteal supply. This creates a relative avascular zone with poor healing potential, explaining the 50%+ nonunion rate in these locations. This is why Zone 2-3 stress fractures require surgical fixation in athletes.

- Blood Supply
- Dual supply (medial/lateral plantar)
- Stress Fracture Risk
- Moderate (weight-bearing importance)
- Clinical Significance
- Lower threshold for surgery due to load
- Blood Supply
- Adequate nutrient artery supply
- Stress Fracture Risk
- Low (MT2 most common but low-risk)
- Clinical Significance
- Excellent healing with activity modification
- Blood Supply
- Periosteal supply adequate
- Stress Fracture Risk
- Low (tuberosity avulsion different)
- Clinical Significance
- Conservative treatment successful
- Blood Supply
- Watershed zone (poor supply)
- Stress Fracture Risk
- VERY HIGH (50%+ nonunion)
- Clinical Significance
- Surgical fixation required in athletes
- MT2: Longest, most rigidly fixed at TMT joint
- Load concentration: Inferior cortex of MT2 shaft
- Repetitive loading: Running, jumping, marching
- Fatigue failure: Microfractures exceed repair capacity
- Bone remodeling: Osteoclast activity exceeds osteoblast activity with overuse
- Microfracture accumulation: Exceeds repair capacity
- Cortical breach: Starts on tension side (inferior cortex)
- Complete fracture: If activity continues
Classification Systems
Metatarsal Stress Fracture Sites
- Risk Level
- Low
- Nonunion Risk
- Under 5%
- Treatment
- Activity modification, CAM boot 4-6 weeks
- Risk Level
- Moderate
- Nonunion Risk
- 10-15%
- Treatment
- NWB 6-8 weeks, consider bone stimulator
- Risk Level
- HIGH
- Nonunion Risk
- 50%+
- Treatment
- Surgical fixation in athletes
- Risk Level
- HIGH
- Nonunion Risk
- 50%+
- Treatment
- Surgical fixation + bone graft if delayed
MT2 stress fracture (marching fracture) is the most common but has low nonunion risk - excellent prognosis with conservative treatment. MT5 Zone 2-3 stress fractures are less common but have HIGH nonunion risk (50%+) - require surgical fixation in athletes. Site determines risk, not frequency.
The classic marching fracture is in the MT2 shaft (low-risk), but a distinct and easily-missed entity is the proximal second-metatarsal-base stress fracture, characteristically seen in ballet dancers - and it behaves very differently:
- Why MT2 is loaded here: the second metatarsal base is recessed and rigidly keystoned into the cuneiforms (the Lisfranc "mortise"), so it is the least mobile metatarsal; in the en pointe / demi-pointe position the load concentrates at this proximal base.
- Why it matters: unlike the benign shaft marching fracture, the proximal MT2-base stress fracture is higher-risk and slow to heal (it lies in the relatively avascular proximal metaphyseal region near the Lisfranc complex), is frequently missed because attention is on the shaft, and can progress to delayed/nonunion if the dancer keeps loading it.
- Recognition: pain and tenderness at the proximal MT2/midfoot (not the shaft) in a dancer with a training/pointe-work spike; look specifically at the MT2 base on imaging and use MRI early (radiographs lag and the base is hard to read).
- Management: a more cautious course than the shaft fracture - genuine offloading/relative rest with prolonged restriction from pointe work and a graded return; surgery is occasionally needed for nonunion.
Exam point: in a dancer with proximal forefoot/midfoot pain, think base-of-second-metatarsal stress fracture (loaded because MT2 is keystoned and immobile) - it is higher-risk and slower-healing than the MT2-shaft marching fracture and needs early MRI and a cautious, prolonged return.
Clinical Assessment
- Onset: Gradual, insidious (weeks to months)
- Mechanism: Repetitive loading, training errors
- Pain: Initially with activity, progresses to rest pain
- Training changes: Recent increase in volume/intensity
- Risk factors: Female athlete triad, nutrition, biomechanics
- Point tenderness: Over specific metatarsal
- Swelling: Localized, minimal in early stages
- Tuning fork test: Vibration over fracture site causes pain
- Hop test: Single-leg hop reproduces pain
- Neurovascular: Usually intact
Fifth metatarsal Zone 2-3 stress fractures may present with minimal symptoms initially but have 50%+ nonunion risk. Any athlete with MT5 base pain and training history should have early MRI to assess Zone 2-3 involvement. Delayed diagnosis leads to nonunion requiring bone graft.
- Key Features
- Point tenderness, insidious onset, training history
- Distinguishing Factor
- MRI shows fracture line and edema
- Key Features
- Diffuse forefoot pain, no point tenderness
- Distinguishing Factor
- No fracture on imaging
- Key Features
- Interdigital pain, Mulder's click
- Distinguishing Factor
- Between metatarsals, not over bone
- Key Features
- MT2 head avascular necrosis
- Distinguishing Factor
- X-ray shows collapse, not stress fracture
Forefoot stress injury is not only metatarsal - a sesamoid stress fracture is a classic, easily-missed cause of plantar first-ray pain in runners, dancers and sprinters, and it is a recognised high-risk (poor-healing) site:
- Which one: the medial (tibial) sesamoid is more often affected (it bears more load); pain is plantar under the first metatarsal head, worse on push-off/dorsiflexion of the hallux.
- Why it heals poorly: the sesamoids have a tenuous, often single-vessel blood supply, so stress fractures are prone to delayed union, nonunion and osteonecrosis - a high-risk pattern despite the small bone.
- The mimic: a bipartite sesamoid (present in a notable minority, frequently bilateral) is the key trap - it has smooth, well-corticated, rounded margins and is often bilateral, whereas a fracture has sharp irregular non-corticated edges, focal tenderness and marrow oedema on MRI; get the contralateral film and MRI/CT if unsure (bone scan is sensitive).
- Management: non-operative first - strict offloading (stiff-soled shoe/boot with a dancer's pad to unload the sesamoid), then graded return; for nonunion the options are partial sesamoidectomy or bone grafting - avoid total excision of both sesamoids (or a tibial sesamoidectomy that destabilises the hallux), which causes a cock-up or hallux valgus/varus deformity.
Exam point: plantar first-MTP pain on push-off is a sesamoid stress fracture until proven otherwise - it is a high-risk poor-vascularity site, distinguish it from a bipartite sesamoid (bilateral, corticated), offload it, and if surgery is needed do a partial sesamoidectomy/graft, never routine total excision.
Investigations
Imaging Protocol
Initial X-rays often negative - stress fractures take 2-3 weeks to show radiographic changes.
Views: AP, lateral, oblique foot
Early findings: None (X-ray negative period)
Later findings:
- Periosteal reaction (2-3 weeks)
- Fracture line (3-4 weeks)
- Callus formation (4-6 weeks)
Best for early diagnosis - shows changes within days of symptom onset.
Findings:
- Bone marrow edema (T2 hyperintensity)
- Fracture line (T1 hypointense line)
- Periosteal reaction
Advantages: High sensitivity, shows extent, guides treatment
Sensitive but less specific than MRI.
Findings: Increased uptake at fracture site
Use: If MRI unavailable, but MRI preferred for specificity
X-rays are negative for 2-3 weeks after symptom onset. If clinical suspicion is high (point tenderness, training history), order MRI immediately rather than waiting for radiographic changes. Early diagnosis allows prompt treatment and prevents progression to complete fracture.

Management Algorithm
Conservative Management
Goal: Pain-free healing with activity modification
Treatment Steps
Activity modification: Stop running/jumping activities
Weight-bearing: CAM boot, weight-bearing as tolerated
Pain control: NSAIDs, ice
Address risk factors: Training errors, nutrition, biomechanics
If pain-free: Progress to walking, then light jogging
Monitor: No return of pain with activity
Cross-training: Swimming, cycling to maintain fitness
Follow-up: X-ray at 6 weeks to confirm healing
Criteria: Pain-free, no tenderness, X-ray shows healing
Progression: Gradual increase in intensity
Prevention: Address underlying causes (training, biomechanics)
MT2 stress fractures (marching fracture) have excellent prognosis with conservative treatment. Success rate over 95% with proper activity modification. Surgery rarely needed unless displaced or nonunion.
STRESSSTRESS - Risk Factors and Management
Hook:STRESS fractures need STRESS management - Site-specific risk, Training errors, Risk factors, Early MRI, Surgery for high-risk, Systematic approach
Surgical Technique
MT5 Zone 2-3 Stress Fracture Fixation
Indication: High-risk stress fractures (MT5 Zone 2-3) in athletes
Surgical Steps
Supine on radiolucent table
C-arm: Positioned for AP and lateral views
Limb: Free draped, accessible for screw insertion
Location: Tip of fifth metatarsal tuberosity
Landmark: Palpable prominence at base of MT5
Incision: Small (1-2cm) longitudinal over tuberosity
Protect: Sural nerve branches
Insertion: Under fluoroscopy guidance
Path: Down medullary canal, across fracture
Endpoint: Engage far cortex (distal)
Confirm: AP and lateral views show correct position
Size: Minimum 5.5mm diameter (larger better)
Length: Measure from guidewire, engage far cortex
Compression: Partially threaded or fully threaded with compression
Final check: Fluoroscopy confirms compression and position
Indication: Torg Type II-III (sclerotic canal, delayed/nonunion)
Technique: Curettage of sclerotic bone, autograft from iliac crest
Placement: Around fracture site, then screw fixation
Alternative: Allograft bone chips if autograft not desired
Layers: Subcutaneous, skin
Dressing: Sterile, non-adherent
Splint: Posterior splint for comfort (remove in 1-2 weeks)
- Screw size matters: 5.5mm minimum, larger diameter better outcomes
- Entry point critical: Tip of tuberosity, not too medial
- Engage far cortex: Essential for compression and stability
- Fluoroscopy: Confirm position before final tightening
- Undersized screw: Less than 5.5mm increases failure risk
- Wrong entry point: Too medial risks peroneal tendon injury
- Incomplete engagement: Screw not engaging far cortex
- Missed sclerosis: Torg Type II-III need bone graft
Screw size is critical - minimum 5.5mm diameter recommended. Studies show better outcomes with larger screws (5.5-6.5mm) compared to 4.5mm. Entry at tip of tuberosity, engage far cortex for compression. For Torg Type II-III, add bone graft after curettage of sclerotic canal.
Complications
- Incidence
- 50%+ (MT5 Zone 2-3 conservative)
- Risk Factors
- High-risk site, continued activity, Torg Type II-III
- Management
- Surgical fixation + bone graft
- Incidence
- 10-20% (all sites)
- Risk Factors
- Inadequate rest, poor nutrition, biomechanics
- Management
- Extended NWB, bone stimulator, address causes
- Incidence
- 20-30%
- Risk Factors
- Underlying causes not addressed
- Management
- Comprehensive risk factor management
- Incidence
- Rare (if displaced)
- Risk Factors
- Inadequate reduction, continued weight-bearing
- Management
- Osteotomy if symptomatic
- Incidence
- 5-10% (surgical)
- Risk Factors
- Undersized screw, poor technique
- Management
- Revision surgery if symptomatic
Fifth metatarsal Zone 2-3 stress fractures have 50%+ nonunion rate with conservative treatment due to watershed blood supply. Athletes should have early surgical fixation to prevent nonunion. Non-athletes may attempt conservative trial but must be counseled about high failure rate and need for eventual surgery.
Postoperative Care and Rehabilitation
Rehabilitation Timeline
Activity: Complete rest from running/jumping
Weight-bearing: CAM boot, weight-bearing as tolerated
Pain control: NSAIDs, ice
Cross-training: Swimming, cycling (if pain-free)
If pain-free: Progress to walking without boot
Activity: Light activities of daily living
Monitor: No return of pain
Continue: Address risk factors (training, nutrition)
Activity: Light jogging if pain-free
Progression: Gradual increase in distance/intensity
Stop if: Pain returns
Follow-up: X-ray at 6 weeks
Criteria: Pain-free, no tenderness, X-ray shows healing
Sport-specific: Gradual return to full activity
Prevention: Maintain risk factor management
Outcomes and Prognosis
- Conservative Success
- 95%+ (6-8 weeks)
- Surgical Success
- N/A (rarely needed)
- Return to Sport
- 6-8 weeks
- Conservative Success
- 85-90% (8-10 weeks)
- Surgical Success
- 95%+ (if needed)
- Return to Sport
- 8-10 weeks
- Conservative Success
- Under 50% (high nonunion)
- Surgical Success
- 90%+ (8-10 weeks)
- Return to Sport
- 8-10 weeks surgical
Site is the strongest predictor: MT2 has excellent prognosis (95%+), MT5 Zone 2-3 has poor prognosis without surgery (under 50%). Early diagnosis and treatment improve outcomes. Addressing risk factors prevents recurrence. Athletes with MT5 Zone 2-3 should have early surgery for reliable healing and timely return.
Guidelines, Registries & Global Practice
- Foot stress fractures: Among the commonest overuse bony injuries in runners, jumpers, dancers and military recruits worldwide
- Track and field: Overall stress fracture incidence ~21% over 12 months in competitive athletes; foot fractures cluster in sprint/jump events (Bennell et al, AJSM 1996)
- Military: Metatarsal stress fractures are a leading cause of recruit attrition during basic training globally
- Site pattern: MT2/MT3 shaft commonest overall; proximal MT5 (Zone 2-3) is uncommon but high-risk
- High-resource: Early MRI, CAM boot/orthoses, cannulated screw fixation, DEXA and sports-nutrition/endocrine pathways readily available
- Limited-resource: Diagnosis often clinical or delayed-radiograph based; activity modification and casting are mainstays; surgery reserved for clear high-risk/failed cases
- Athlete level: Elite/professional athletes are managed more aggressively (early fixation) to protect career timelines regardless of region
- Focus
- Proximal MT5 (Jones / Zone 2-3)
- Key Position
- Intramedullary screw fixation favoured in athletes for reliable union and earlier return to sport
- Focus
- Metatarsal & foot injuries
- Key Position
- Low-risk shaft fractures managed non-operatively; high-risk MT5 referred for surgical consideration
- Focus
- Bone stress injury & RED-S
- Key Position
- Risk-stratify by site (high vs low risk); screen and treat low energy availability / Triad as a root cause
- Focus
- Operative technique
- Key Position
- Canal-filling intramedullary screw with compression; graft sclerotic canals (Torg II-III)
Unlike arthroplasty, metatarsal stress fractures are not tracked in national joint registries. The best comparative evidence comes from systematic reviews and athlete cohorts (e.g. Mallee et al, BJSM 2014), which consistently show earlier return to sport with surgery for the proximal fifth metatarsal but at low overall evidence quality - so management is individualised by site, athlete level and resources rather than dictated by a single guideline.
- Document risk-factor assessment (training load, nutrition, energy availability, menstrual status, biomechanics)
- Counsel explicitly about the high nonunion rate of MT5 Zone 2-3 with conservative care and the surgical alternative
- Record the treatment rationale (site- and athlete-specific) and any multidisciplinary referrals (sports medicine, dietetics, endocrinology)
Controversies and Areas of Uncertainty
Optimal screw diameter and design (solid vs cannulated, partially vs fully threaded) remain debated. The principle is a canal-filling screw with compression across the fracture; oversizing risks lateral cortex blow-out, undersizing risks refracture. No randomised trial defines a single best implant.
Routine fixation of every proximal MT5 stress fracture in low-demand patients is not established. A conservative trial (non-weight-bearing) is reasonable, with surgery for delayed union, nonunion or those wanting faster, more reliable return.
The role of bone stimulators, vitamin D optimisation, teriparatide and biologic augmentation is plausible but evidence is limited and largely extrapolated; they should not replace addressing energy availability and mechanical load.
There is no universally validated return-to-sport test battery. Radiographic union can lag clinical recovery, and re-fracture after early return (especially in cavovarus feet) drives interest in CT confirmation and gradual load progression.
A strong viva answer acknowledges that the "50% nonunion" figure for conservatively treated MT5 Zone 2-3 fractures comes from heterogeneous historical series, that the surgery-versus-conservative evidence is low quality (GRADE), and that the decision is individualised by site, Torg type, athlete level, foot alignment (cavovarus) and energy availability rather than a single rule.
MCQ Practice Points
Q: What is the most common site for metatarsal stress fractures? A: Second metatarsal (marching fracture) - most common site but has low nonunion risk with excellent prognosis using conservative treatment.
Q: Which metatarsal stress fracture location has the highest nonunion risk? A: Fifth metatarsal Zone 2-3 (metadiaphyseal junction and proximal diaphysis) - 50%+ nonunion rate with conservative treatment due to watershed blood supply. Athletes require surgical fixation.
Q: When do stress fractures become visible on X-ray after symptom onset? A: 2-3 weeks - X-rays are negative initially. MRI is gold standard for early diagnosis, showing changes within days of symptom onset.
Q: What is the minimum recommended screw diameter for MT5 Zone 2-3 stress fracture fixation? A: 5.5mm - Studies show better outcomes with larger screws (5.5-6.5mm) compared to 4.5mm. Screw size matters for reliable healing.
Q: What is the typical return to sport timeline for MT5 Zone 2-3 stress fractures treated surgically? A: 8-10 weeks - Surgical fixation allows reliable healing and earlier return compared to conservative treatment (which has 50%+ nonunion risk and 15+ weeks if it fails).
Q: What increases the risk of metatarsal stress fractures in female athletes? A: Female athlete triad / RED-S - low energy availability, menstrual dysfunction and low bone mineral density are the key female-specific risk factors (Bennell et al, AJSM 1996). Also training errors, nutrition, prior stress fracture, and biomechanical factors.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old female runner presents with 3 weeks of gradually worsening pain in her midfoot. Pain started after increasing her weekly mileage from 20 to 40 miles. Examination shows point tenderness over the second metatarsal shaft. X-rays are normal. What is your assessment and management?”
“A 19-year-old college basketball player presents with 6 weeks of pain at the base of his fifth metatarsal. He continued playing through the pain initially. Examination shows tenderness over MT5 base, pain with hop test. X-ray shows a fracture line at the metadiaphyseal junction extending into the 4-5 intermetatarsal articulation, with some medullary sclerosis. What is your assessment and management?”
“A 20-year-old female cross-country runner presents with her third metatarsal stress fracture in 18 months (previous MT2, MT3, now MT4). She has been compliant with activity modification each time. What is your approach?”
Key Anatomy
- MT2 = most common site (marching fracture) - low risk, excellent prognosis
- MT5 Zone 2-3 = HIGH RISK - watershed blood supply, 50%+ nonunion
- Watershed zone = metadiaphyseal junction where nutrient artery meets periosteal supply
- MT1 = moderate risk due to weight-bearing importance
Classification
- Site-based: MT2 (low), MT1 (moderate), MT5 Zone 2-3 (HIGH)
- Torg classification: Type I (acute), Type II (delayed with sclerosis), Type III (nonunion)
- Severity: Grade I (MRI only), Grade II (periosteal reaction), Grade III (fracture line), Grade IV (displaced)
- Zone classification (MT5): Zone 1 (tuberosity), Zone 2 (metaphyseal-diaphyseal), Zone 3 (proximal diaphysis)
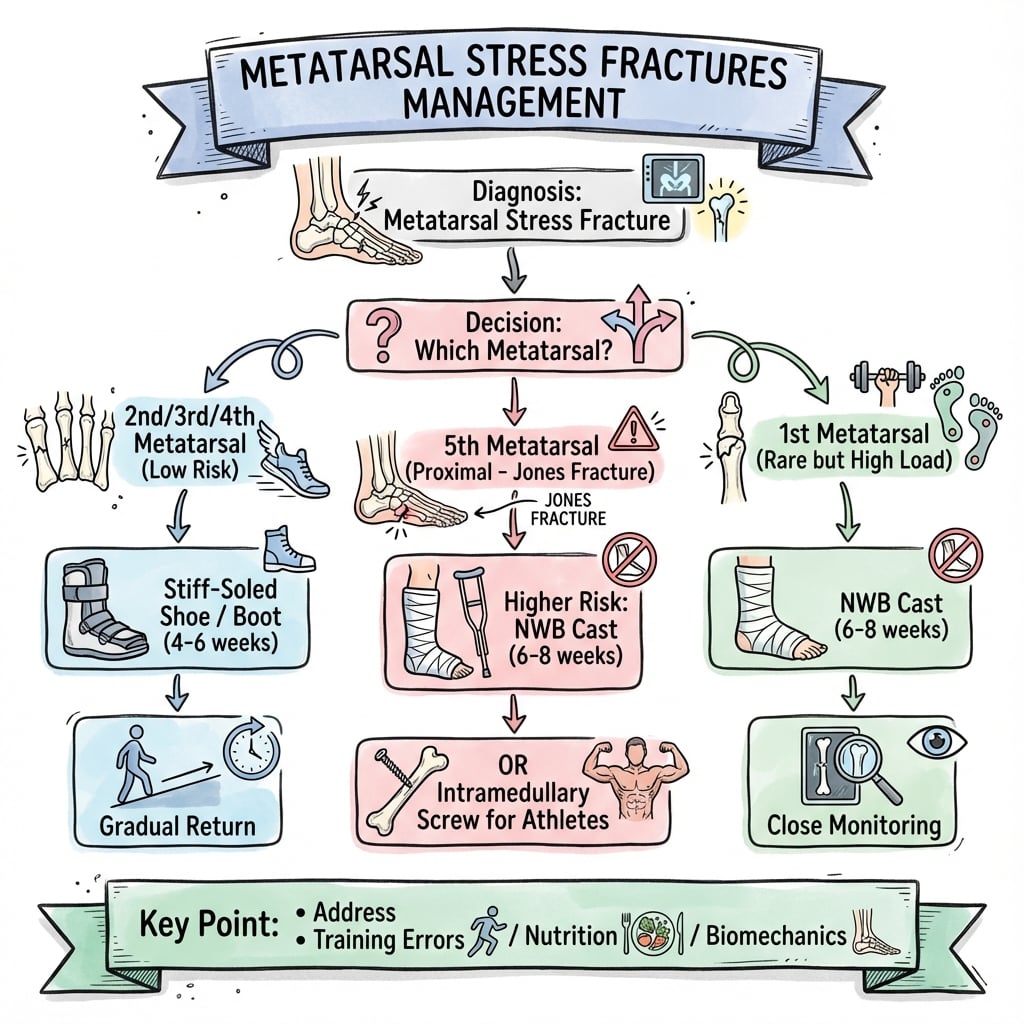
Treatment Algorithm
- Low-risk (MT2-4): Activity modification, CAM boot 4-6 weeks, excellent prognosis
- High-risk (MT5 Zone 2-3): Surgical fixation (IM screw) in athletes, 50%+ nonunion with conservative
- Torg Type II-III: Bone graft + screw fixation for sclerotic canal
- Address risk factors: Training errors, nutrition, female athlete triad, biomechanics
Surgical Pearls
- Entry point: Tip of MT5 tuberosity (not too medial)
- Screw size: Minimum 5.5mm diameter (larger better outcomes)
- Technique: Engage far cortex for compression
- Bone graft: For Torg Type II-III (curettage + autograft)
Complications
- Nonunion: 50%+ risk MT5 Zone 2-3 with conservative treatment
- Delayed union: 10-20% all sites, address risk factors
- Recurrence: 20-30% if underlying causes not addressed
- Hardware issues: 5-10% with undersized screws or poor technique
Evidence Base and Key Trials
Torg Classification - Proximal Fifth Metatarsal Fractures
- Landmark series of 46 proximal fifth metatarsal fractures, mean follow-up 40 months
- Defined three radiographic types: acute (narrow line, no sclerosis), delayed union (widened line, medullary sclerosis), and nonunion (canal obliterated by sclerotic bone)
- 14 of 15 acute fractures treated with non-weight-bearing toe-to-knee cast healed in a mean of 7 weeks
- Only 4 of 10 acute fractures treated with weight-bearing methods united
- 19 of 20 fractures treated with medullary curettage and inlay bone graft healed
Lawrence & Botte Zone Classification of the Proximal Fifth Metatarsal
- Anatomical review separating three proximal fifth metatarsal fracture entities: tuberosity avulsion (Zone 1), Jones fracture at the metaphyseal-diaphyseal junction (Zone 2), and proximal diaphyseal stress fracture (Zone 3)
- Vascular study highlighted a watershed region at the metaphyseal-diaphyseal junction supplied by both the nutrient artery and metaphyseal vessels
- Diaphyseal stress fractures are frequently confused with Jones fractures, obscuring differences in prognosis and treatment
- Most acute fractures heal with immobilisation; displaced intra-articular fractures, delayed unions and nonunions usually need surgery
Risk Factors for Stress Fractures in Track-and-Field Athletes
- 12-month prospective cohort of 111 athletes (53 female, 58 male); stress fracture incidence 21.1%
- In men, none of the evaluated risk factors predicted stress fracture
- In women, lower bone density, a history of menstrual disturbance, less lower-limb lean mass, leg-length discrepancy and a lower-fat diet were significant risk factors
- Age at menarche and calf girth were the best independent predictors in women, correctly classifying 80%
Incidence and Distribution of Stress Fractures in Athletes
- Same prospective cohort: 20 athletes sustained 26 stress fractures (21.1%), rate 0.70 per 1000 training hours
- No significant difference in stress fracture rate between men and women
- Sprints, hurdles and jumps were associated with more foot fractures; middle/long-distance running with more long-bone and pelvic fractures
- Tibia (46%), navicular (15%) and fibula (12%) were the commonest overall sites
Intramedullary Screw Fixation of Jones Fractures in Athletes
- Expert review of all three Torg types of proximal fifth metatarsal (Jones) fractures in athletes
- Intramedullary screw fixation that 'fits and fills' the canal with threads across the fracture is the standard operative approach
- Excellent clinical outcomes reported in 80-100% of patients with screw fixation
- Most studies show return to sport at 7-12 weeks after fixation
- Non-operative treatment is rarely used as sole treatment except after re-injury of stable fixation
Surgical vs Conservative Treatment of Proximal Fifth Metatarsal Fractures in Athletes
- 42 athletes with Zone II-III fifth metatarsal fractures; 33 had immediate intramedullary screw fixation, 9 refused surgery and were treated conservatively
- All fractures in the surgical group healed (26 within 8 weeks); 4 of 9 conservative fractures failed to unite by 6 months
- 5 of 9 conservatively treated fractures did not heal; 4 required subsequent osteosynthesis
- 3 surgically treated athletes who resumed intensive training re-fractured and were revised with a stronger screw
Surgical vs Conservative Treatment of High-Risk Lower-Limb Stress Fractures - Systematic Review
- Systematic review of 18 studies covering anterior tibial cortex, navicular and proximal fifth metatarsal stress fractures
- For the fifth metatarsal, weighted mean return to sport was 14 weeks with surgery vs 19 weeks with conservative treatment
- For the navicular, surgery gave earlier return (16 vs 22 weeks); when treated conservatively, weight-bearing should be avoided
- Overall evidence quality was low (GRADE) with a high risk of bias
ACSM Position Stand - The Female Athlete Triad
- Defines the Triad as the interrelationship of energy availability, menstrual function and bone mineral density
- Low energy availability (below ~30 kcal/kg fat-free mass/day) is the central driver of reproductive and skeletal impairment
- Recommends Triad screening at pre-participation and annual health exams and whenever a component (including bone stress injury) presents
- Advocates a multidisciplinary team and prioritises restoring energy availability over pharmacotherapy