Peritalar Injury | TN + TC Joints | Medial 80% | Urgent Reduction | AVN Risk
- Two joints involved: Talonavicular AND talocalcaneal (tibiotalar intact)
- Medial most common (85%): Foot inverted and adducted = 'acquired clubfoot'
- Urgent reduction: Skin tension causes necrosis within hours
- Associated fractures: CT after reduction - 40% have occult fractures
- AVN risk: Talus has tenuous blood supply - prolonged dislocation increases risk
- “Named by direction of FOOT relative to talus (medial = foot goes medial)
- “Medial dislocation = adducted/inverted = 'acquired clubfoot' appearance
- “Lateral dislocation = abducted/everted = 'acquired flatfoot' appearance
- “CT mandatory after reduction to detect associated fractures
- “Open dislocations have significantly worse outcomes
Critical Exam Points - Subtalar Dislocations:
- JOINTS INVOLVED: Talonavicular + Talocalcaneal (NOT tibiotalar)
- MEDIAL IS MOST COMMON (85%): Foot displaced medial = acquired clubfoot appearance
- URGENT REDUCTION REQUIRED: Skin tension causes necrosis - reduce within hours
- CT AFTER REDUCTION: 40% have occult fractures - always scan after reduction
- REDUCTION TECHNIQUE: Knee flexed, traction, accentuate deformity then reverse
- OPEN INJURIES: Much worse prognosis - higher complication rates
- Medial Dislocation (85%)
- Adducted and inverted
- Lateral Dislocation (15%)
- Abducted and everted
- Medial Dislocation (85%)
- Acquired clubfoot
- Lateral Dislocation (15%)
- Acquired flatfoot
- Medial Dislocation (85%)
- Inversion force (most common)
- Lateral Dislocation (15%)
- Eversion force
- Medial Dislocation (85%)
- Traction + EVERSION
- Lateral Dislocation (15%)
- Traction + INVERSION
- Medial Dislocation (85%)
- Talar head on navicular/EHL
- Lateral Dislocation (15%)
- Talar head on cuboid/peroneal tendons
- Medial Dislocation (85%)
- Lower
- Lateral Dislocation (15%)
- Higher (worse prognosis)
PERITALARPERITALAR - Key Features
Hook:PERITALAR dislocations involve Paired joints, require Emergency reduction, and need CT to detect Associated fractures
MEDIALMEDIAL - Medial Dislocation Features
Hook:MEDIAL is Most common and needs Eversion to reduce
Overview
Subtalar Dislocations - Peritalar Dislocations
Subtalar dislocations are rare but dramatic injuries characterized by simultaneous dislocation of the talonavicular and talocalcaneal joints while the tibiotalar joint remains intact. Also called "peritalar dislocations," they represent approximately 1% of all dislocations and require urgent reduction to prevent skin necrosis and long-term complications.
Epidemiology
- Rare injury - approximately 1% of all dislocations
- 1-2% of major joint dislocations
- Predominantly young males (70-80%)
- Usually high-energy mechanism
- Motor vehicle accidents (40%)
- Falls from height (30%)
- Sports injuries (20%) - basketball, football
- Direct trauma (10%)
- Most common in 20-40 year age group
- Rare in children and elderly
- Associated with active lifestyle/sports
Anatomy and Pathophysiology
Subtalar Complex Anatomy
The Subtalar Complex
- Talonavicular joint (ball and socket)
- Talocalcaneal joint (subtalar joint proper)
- Tibiotalar joint - remains intact (talus stays in mortise)
This is why the injury is also called "peritalar dislocation" - the dislocation occurs AROUND the talus.
Blood Supply to the Talus
- Posterior tibial artery: Main supply via artery of the tarsal canal
- Anterior tibial artery: Supplies talar neck and head dorsally
- Peroneal artery: Supplies via artery of the tarsal sinus
- 60% of talus is covered by articular cartilage (no periosteal vessels)
- Tenuous retrograde blood supply
- Prolonged dislocation can compromise vessels
- Risk of AVN, especially with delayed reduction
The talus has no muscle attachments and 60% articular cartilage coverage, making it dependent on intraosseous blood supply through the tarsal canal and sinus. Prolonged dislocation with stretched vessels significantly increases AVN risk.
Mechanism of Injury
- High-energy inversion force
- Foot forced into plantarflexion and inversion
- Common scenarios: falls, MVA, sports (basketball - "basketball foot")
- Calcaneus, navicular, and forefoot displace medially under talus
- High-energy eversion force
- Foot forced into dorsiflexion and eversion
- Usually requires greater force than medial
- Higher association with open injuries and fractures
The dislocation is named by the direction of the FOOT relative to the talus:
- Medial dislocation: Foot goes MEDIAL = adducted, inverted = "acquired clubfoot"
- Lateral dislocation: Foot goes LATERAL = abducted, everted = "acquired flatfoot"
The talus remains in the ankle mortise in both types.
Structures That Can Block Reduction
- Talar head buttonholes through extensor retinaculum
- EHL tendon may wrap around talar head
- Tibialis posterior tendon occasionally blocks
- Talonavicular capsule interposition
- Peroneal tendons wrap around talar neck
- Talar head buttonholes through extensor retinaculum
- FHL tendon may block
- Posterior tibial tendon occasionally involved
BLOCKBLOCK - Structures Blocking Reduction
Hook:If closed reduction BLOCKED, suspect soft tissue interposition - may need open reduction
Classification
Classification
Medial Subtalar Dislocation
Most Common Type (85%)
- High-energy inversion force
- Plantarflexion and inversion
- Falls, MVA, sports (basketball)
- Displaced MEDIALLY
- Adducted and inverted
- "Acquired clubfoot" appearance
- Prominent DORSOLATERALLY
- Palpable and visible
- Skin tension over prominence
- Knee flexed (relax gastrocnemius)
- Longitudinal traction
- Accentuate plantarflexion and inversion
- Then EVERT and dorsiflex to reduce
- Extensor retinaculum (buttonholed)
- EHL tendon wrapping talar head
- Tibialis posterior tendon
- Talonavicular capsule
- Better than lateral type
- 60-90% good-excellent outcomes (pure dislocation)
- Lower open injury rate
- Lower complication rate
Medial is most common, has better prognosis, and is easier to reduce.
Clinical Assessment
Initial Assessment
Presentation
-
Medial: Foot appears adducted and inverted ("acquired clubfoot")
- Talar head prominent DORSOLATERALLY
- Heel in varus
-
Lateral: Foot appears abducted and everted ("acquired flatfoot")
- Talar head prominent DORSOMEDIALLY
- Heel in valgus
- Significant swelling
- Severe pain
- Unable to weight bear
- Skin tension - may be tented over talar head
- Open wounds (check carefully)
Skin Assessment - Critical
Skin tension over the talar head is an EMERGENCY
The prominent talar head causes extreme skin tension that can lead to:
- Necrosis within hours
- Full-thickness skin loss
- Open conversion of closed injury
- Infection risk
Immediate reduction is mandatory to relieve skin tension.
Neurovascular Examination
- Dorsalis pedis pulse (may be displaced)
- Posterior tibial pulse
- Capillary refill
- Sensory examination (if patient can cooperate)
- Superficial peroneal (dorsum of foot)
- Deep peroneal (first web space)
- Tibial nerve (plantar foot)
- Sural nerve (lateral foot)
- Changes in vascular status
- Sensory changes
- Motor function once pain controlled
Associated Injuries to Assess
- Open wounds (check carefully between toes)
- Associated fractures (malleoli, talus, calcaneus, navicular, cuboid)
- Ankle mortise integrity
- Skin condition
- High-energy mechanism - assess for polytrauma
- Spine injuries
- Other extremity injuries
- Head injury
Differential Diagnosis
The deformed, swollen hindfoot has several mimics. The single most discriminating step is establishing whether the tibiotalar (ankle) mortise is intact and which articulations have lost congruity.
- Distinguishing feature
- TN + TC joints dislocated, tibiotalar INTACT
- Key discriminator
- Talus stays in mortise; foot displaced under talus
- Distinguishing feature
- Talus dislocated from tibiotalar AND subtalar joints
- Key discriminator
- Talus extruded/rotated out of mortise; very high AVN and infection risk
- Distinguishing feature
- Talus displaced relative to tibia/fibula; mortise disrupted
- Key discriminator
- Malleolar fractures and incongruent mortise on AP/mortise view
- Distinguishing feature
- Fracture line through talar neck, joints may be congruent
- Key discriminator
- Cortical break at talar neck rather than pure joint malalignment
- Distinguishing feature
- TN +/- calcaneocuboid disruption, talocalcaneal INTACT
- Key discriminator
- Subtalar joint congruent; dislocation is distal to talus only
- Distinguishing feature
- Broadened, shortened heel after axial load
- Key discriminator
- Boehler angle change on lateral; subtalar congruity often preserved
The top differential above - total talar dislocation - is the catastrophic end of the peritalar spectrum and a favourite exam contrast, so be ready to distinguish it from the subtalar dislocation managed in this topic.
- The difference: in a subtalar dislocation the talus stays in the ankle mortise while the foot dislocates beneath it; in a total talar dislocation the talus is extruded from all three of its articulations (tibiotalar, talocalcaneal and talonavicular), commonly rotated and often pushed out through a wound (open in the great majority).
- Why it is far worse: the already tenuous talar blood supply is essentially completely stripped, so AVN is near-universal and, because most are open, deep infection is the dominant early threat.
- Management differs: treat as an open-fracture emergency - early IV antibiotics, urgent thorough irrigation and debridement. The long-standing teaching to discard the extruded talus (talectomy) has largely shifted toward reimplantation of the talus even when fully extruded (after meticulous cleaning), because primary talectomy gives poor function and reimplantation can succeed despite AVN; primary fusion (tibiocalcaneal/blair) or delayed reconstruction is reserved for the unsalvageable or infected talus.
- Counsel for a guarded outcome: AVN, infection and post-traumatic arthritis are the rule rather than the exception.
Exam point: a subtalar dislocation keeps the talus in the mortise (good prognosis with prompt reduction), whereas a total talar dislocation extrudes the talus from all three joints - an open-fracture emergency with near-universal AVN and high infection risk, now usually managed by debridement and reimplantation rather than talectomy.
Investigations
Imaging Protocol
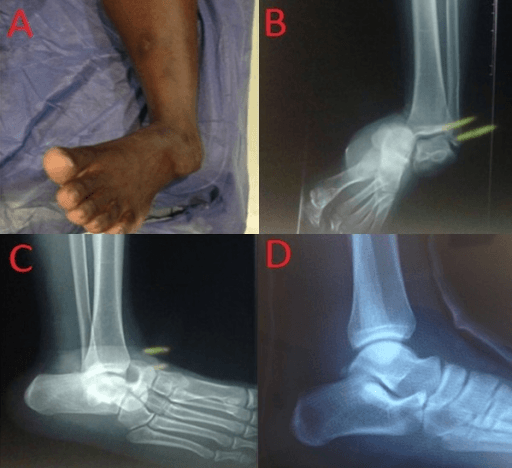
Pre-Reduction X-rays
- AP foot
- Lateral foot
- AP ankle
- Lateral ankle
- Confirm subtalar dislocation (TN and TC disrupted)
- Confirm tibiotalar joint intact
- Identify obvious fractures
- Determine direction of dislocation
If skin is compromised, reduce emergently based on clinical findings and whatever imaging is immediately available.
Post-Reduction Imaging
X-rays:
- Confirm congruent reduction of TN and TC joints
- Check ankle mortise alignment
- Assess any fractures now visible after reduction
CT Scan - MANDATORY:
Always get CT after successful reduction of a subtalar dislocation:
- 40% of subtalar dislocations have associated fractures
- Many are occult on plain X-rays
- May change management if large fragments present
- Identifies loose bodies
- Assesses congruency of reduction
CT Assessment:
- Talar dome and neck fractures
- Posterior process fractures
- Calcaneal fractures (sustentaculum, anterior process)
- Navicular fractures
- Cuboid fractures
- Loose bodies
- Reduction congruency
MRI (Rarely Indicated Acutely)
Potential Indications:
- Suspected chondral injury
- Soft tissue interposition preventing reduction
- Late presentation with concerns for AVN
- Usually delayed investigation
Management
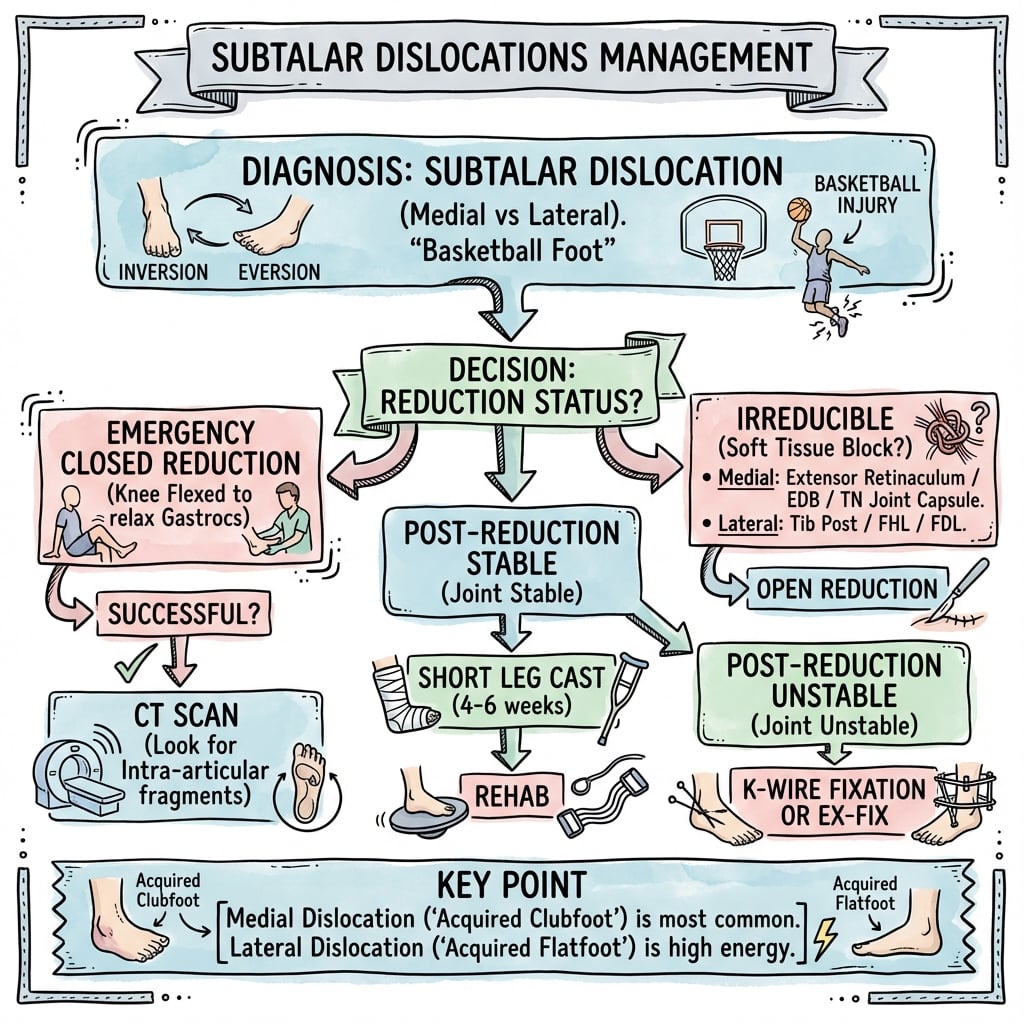
Management Algorithm
Initial Emergency Department Management
- Neurovascular examination and documentation
- Skin assessment - tented skin is emergency
- Check for open wounds
- Pain control
- AP and lateral foot X-rays
- AP and lateral ankle X-rays
- Do NOT delay reduction if skin compromised
- Imaging confirms diagnosis and direction
- Skin tension over talar head = URGENT reduction
- Can occur within hours of injury
- Risk of skin necrosis and full-thickness loss
- May convert closed to open injury
- Patient supine
- Procedural sedation or regional anesthesia
- Assistant for counter-traction
- Fluoroscopy helpful but not mandatory
Skin tension is the primary driver of urgency.
The topic notes that K-wire stabilisation is "rarely needed" and that its role is "unclear" - but a viva will press you on how you decide, so make the assessment explicit rather than reflexive.
After any reduction (closed or open), test stability directly:
- Confirm a concentric reduction of both the talonavicular and talocalcaneal joints on fluoroscopy.
- Stress the hindfoot under image intensifier through the arc that produced the injury (inversion/eversion, dorsi/plantarflexion). A pure dislocation that reduces with a clear "clunk" is usually intrinsically stable once the capsuloligamentous sleeve is back in place, and a simple below-knee cast/backslab suffices.
Instability that warrants supplementary fixation is the exception and clusters in predictable settings:
- Associated fractures that remain displaced or render a joint incongruent after reduction (e.g. talar neck, large talar head/navicular fragments) - fix the fracture (ORIF) and the dislocation usually becomes stable.
- Re-dislocation or gross subluxation on stress despite a concentric reduction.
- After open reduction where the stabilising capsule, retinaculum and ligaments have been extensively disrupted, or in open injuries with severe soft-tissue loss.
What to use when it is unstable:
- Temporary percutaneous K-wire transfixion across the unstable joint (talonavicular and/or across the subtalar joint), removed at about 4 to 6 weeks before mobilising the subtalar joint.
- A spanning external fixator for grossly unstable, highly comminuted, or soft-tissue-compromised/open injuries, which also allows wound access.
- Avoid prolonging immobilisation unnecessarily - the original DeLee and Curtis teaching is that prolonged casting worsens subtalar stiffness, so remove temporary fixation and begin range of motion as soon as stability allows.
Exam point: most pure subtalar dislocations are stable after a concentric reduction and need only a cast; reserve temporary K-wire transfixion or a spanning external fixator for instability on fluoroscopic stress, an incongruent/unfixed associated fracture, re-dislocation, or extensive soft-tissue disruption after open injury - then remove it early to limit stiffness.
Surgical Technique
Surgical Approaches for Open Reduction
Indications for Open Reduction
- Irreducible closed reduction (soft tissue interposition)
- Open dislocation requiring debridement
- Large displaced fracture-dislocation requiring fixation
- Failed closed reduction under GA with complete muscle relaxation
- Associated fractures requiring ORIF
- Persistent instability after closed reduction (rare)
- 80-90% of subtalar dislocations reduce with closed technique
- 10-20% require open reduction
- Most failures due to soft tissue interposition
Note: Most subtalar dislocations can be successfully reduced with proper technique and adequate analgesia/muscle relaxation.
Complications
Acute Complications
Skin Necrosis
Most Urgent Acute Complication:
- Occurs with prolonged dislocation
- Skin tented over talar head
- Can develop within 6-12 hours
- Full-thickness skin loss possible
- May convert closed to open injury
- Prevention: Urgent reduction
Neurovascular Injury
5-10% of cases
- Superficial peroneal nerve (most common)
- Deep peroneal nerve
- Tibial nerve
- Usually neurapraxia from stretch
- Most recover with time
- Dorsalis pedis artery injury rare
- Posterior tibial artery injury rare
- Compartment syndrome (very rare)
Inability to Reduce
Failed Closed Reduction (10-20%):
- Soft tissue interposition
- Buttonholed extensor retinaculum
- EHL tendon (medial dislocation)
- Peroneal tendons (lateral dislocation)
- Requires open reduction
Compartment Syndrome
Very Rare but Possible:
- High-energy injuries
- Associated fractures
- Prolonged dislocation
- Monitor closely first 48 hours
- High index of suspicion needed
Chronic Complications
Post-Traumatic Arthritis
- Pure closed medial: 30-40%
- Fracture-dislocation: 50-70%
- Open or lateral: 60-80%
- May take 5-10 years to develop
- Progressive symptoms
- Joint space narrowing on X-ray
- Subtalar crepitus and pain
- Activity modification
- Orthotics and supportive footwear
- NSAIDs for pain
- Corticosteroid injections
- Subtalar fusion if severe (good pain relief, further stiffness)
- Fusion provides reliable pain relief
- Further loss of inversion/eversion
- Often well-tolerated
Avascular Necrosis (AVN)
- Pure dislocation: 5-10%
- Fracture-dislocation: 15-20%
- Open injury: 20-30%
- Higher with delayed reduction
- Delayed reduction (over 6 hours)
- High-energy mechanism
- Associated talar neck fracture
- Open injury
- Need for open reduction
- Initially asymptomatic
- Pain develops as collapse occurs
- Progressive deformity
- Eventually arthritis
- Hawkins sign at 6-8 weeks (subchondral lucency = good blood supply)
- Absence of Hawkins sign concerning for AVN
- MRI most sensitive for early detection
- X-ray changes later (sclerosis, collapse)
- Protected weight bearing if detected early
- Core decompression rarely beneficial
- Usually progresses to fusion if symptomatic
- May require talonavicular or triple fusion
Subtalar Stiffness
- 50-70% loss of subtalar motion typical
- Inversion more affected than eversion
- Often well-compensated by ankle and midfoot
- Stiffness may protect against arthritis pain
- Walking on flat ground usually normal
- Difficulty on uneven terrain
- Difficulty on slopes/inclines
- May need orthotic support
- Aggressive physical therapy for ROM
- Orthotic devices for support
- Ankle-foot orthosis if severe
- Most patients adapt well
Chronic Pain
10-40% depending on injury severity
- Post-traumatic arthritis
- Subtalar stiffness
- Nerve injury (neuroma, dysesthesia)
- Complex regional pain syndrome (rare)
- Multimodal pain management
- Physical therapy
- Psychological support
- Orthotics
- Surgical options if structural cause
Malunion/Nonunion (with Associated Fractures)
- Alters hindfoot alignment
- Accelerates arthritis
- May need osteotomy or fusion
- Rare with adequate immobilization
- May occur with talar neck fractures
- Usually requires surgical fixation
Prevention of Complications
Early Reduction
Single Most Important Factor:
- Reduces skin necrosis risk
- Reduces AVN risk
- Improves overall outcomes
- Target: Reduction within 6 hours
CT Scanning
Detects Occult Fractures:
- Changes management in 20% of cases
- Allows appropriate fixation
- Prevents displacement during healing
- Improves long-term outcomes
Adequate Immobilization
Prevents Redislocation:
- 4-6 weeks immobilization typical
- Non-weight bearing essential
- Progressive loading protocol
- Serial X-rays to monitor
Aggressive Rehabilitation
Optimizes Function:
- ROM exercises after immobilization
- Strengthening program
- Proprioception training
- Return to activity protocol
Postoperative Care
Rehabilitation Protocol
Phase 1: Protection (0-6 Weeks)
- Below-knee backslab or cast
- Strictly non-weight bearing
- Crutches or knee scooter
- Elevation and ice
- DVT prophylaxis (rivaroxaban or enoxaparin)
- Monitor for compartment syndrome (first 48h)
- Transition to CAM boot or short leg cast
- Continue non-weight bearing
- Begin ankle ROM exercises (if tibiotalar stable)
- Gentle active dorsiflexion/plantarflexion
- Do NOT invert/evert (protect subtalar healing)
- Post-reduction (immediate)
- 2 weeks
- 6 weeks
- MANDATORY after reduction to detect occult fractures
- Usually performed within 24-48 hours of reduction
Phase 2: Progressive Loading (6-12 Weeks)
- X-rays to confirm healing
- Begin partial weight bearing in CAM boot (25-50%)
- Progressive increase based on pain
- Continue ankle ROM
- Begin gentle subtalar ROM
- Progress to full weight bearing
- Wean from CAM boot to supportive shoe
- Physical therapy 2-3x per week
- Focus on proprioception and balance
- Strengthening exercises
Phase 3: Return to Function (3-6 Months)
- Full weight bearing in regular shoes
- Progress strengthening
- Sport-specific training if applicable
- Continue balance and proprioception work
- Return to sports/full activity
- May have persistent subtalar stiffness
- Monitor for signs of post-traumatic arthritis
Monitoring for Complications
- Hawkins sign on X-ray at 6-8 weeks (subchondral lucency = good blood supply)
- Absence of Hawkins sign may indicate AVN
- MRI if high clinical suspicion
- Peak incidence 12-24 months post-injury
- May not manifest for years
- Serial X-rays if symptomatic
- Consider subtalar fusion if symptomatic arthritis develops
- Universal to some degree
- Often well-tolerated
- Physical therapy for ROM
- May protect against arthritis pain
Long-Term Follow-Up
- 6 weeks, 12 weeks, 6 months, 12 months
- Then as needed if symptomatic
- Pain levels
- ROM (especially subtalar inversion/eversion)
- Gait pattern
- Return to work/sport
- X-ray changes (arthritis, AVN)
Outcomes and Prognosis
Prognostic Factors
Factors Associated with Better Outcomes
- Younger age (under 40 years)
- Higher activity level pre-injury
- Non-smoker
- Healthy BMI
- Medial dislocation (vs lateral)
- Closed injury (vs open)
- Pure dislocation (no associated fractures)
- Early reduction (within 6 hours)
- Successful closed reduction (vs open)
Factors Associated with Worse Outcomes
Injury Factors:
- Lateral dislocation (much worse than medial)
- Open injury (infection, AVN, arthritis rates all higher)
- Associated fractures (fracture-dislocation)
- Delayed reduction (over 12 hours)
- Need for open reduction
- High-energy mechanism
Expected Outcomes by Injury Type
Pure Closed Medial Dislocation
Best Prognosis Group
60-90%
- Most return to work
- Many return to sport (may be delayed)
- Subtalar stiffness common but often asymptomatic
- Post-traumatic arthritis: 30-40%
- AVN: 5-10%
- Persistent stiffness: Common (often well-tolerated)
- Chronic pain: 10-20%
- Sedentary work: 2-3 months
- Manual labor: 4-6 months
- Contact sports: 6-9 months
- May never regain full subtalar motion
Fracture-Dislocation (Closed)
Moderate Prognosis
40-60%
- Post-traumatic arthritis: 50-70%
- AVN: 15-20%
- Persistent pain: 30-40%
- Size and location of fracture
- Quality of reduction
- Successful fixation if needed
Lateral or Open Dislocations
Poor Prognosis
20-40%
- Post-traumatic arthritis: 60-80%
- AVN: 20-30%
- Infection (open injuries): 10-30%
- Chronic pain: 40-60%
- Need for salvage procedure: 20-40%
- Subtalar fusion (most common)
- Triple arthrodesis
- Below-knee amputation (severe cases)
Functional Outcomes
Subtalar Motion
- Inversion: 20-30 degrees
- Eversion: 10-20 degrees
- Expect 50-70% loss of motion
- Inversion more affected than eversion
- Often well-compensated by ankle and midfoot
- Stiffness may protect against arthritis pain
Activities of Daily Living
Most Patients:
- Normal walking on flat ground
- Difficulty on uneven terrain
- Difficulty with slopes/stairs
- May need orthotic support
Return to Sport
Low Impact (walking, cycling): 3-4 months typical Moderate Impact (running): 6-9 months typical High Impact (basketball, football): 9-12 months typical Elite Athletes: May not return to pre-injury level
Guidelines, Registries & Global Practice
Global Epidemiology
Subtalar dislocation is rare worldwide, accounting for approximately 1% of all traumatic foot injuries and 1-2% of all dislocations, almost always from high-energy trauma (Prada-Cañizares et al, 2015). Pooled data from large systematic reviews give a consistent demographic and directional profile:
- Hoexum 2014 (n=528)
- 76%
- Lugani 2022 (n=389)
- Male predominant
- Hoexum 2014 (n=528)
- 33.8 years
- Lugani 2022 (n=389)
- Young, active adults
- Hoexum 2014 (n=528)
- 71.5%
- Lugani 2022 (n=389)
- 68.1%
- Hoexum 2014 (n=528)
- 26.0%
- Lugani 2022 (n=389)
- 27.7%
- Hoexum 2014 (n=528)
- 22.5%
- Lugani 2022 (n=389)
- Bone exposure 44.5% (lateral-heavy)
- Hoexum 2014 (n=528)
- 61.4%
- Lugani 2022 (n=389)
- Associated lesions 44.5%
- Hoexum 2014 (n=528)
- 14.0%
- Lugani 2022 (n=389)
- Open reduction 48.2% (lateral-heavy)
- Hoexum 2014 (n=528)
- 52.3%
- Lugani 2022 (n=389)
- Lateral subgroup worst
The classic teaching of "medial 85%" derives from small historical series (e.g. DeLee and Curtis, 1982). Modern pooled reviews of several hundred cases place the medial proportion nearer 68-72%. Both figures are defensible in a viva; cite the modern systematic-review denominators if pressed for precision.
Guidelines and Society Guidance
No high-level (Level I/II) guideline or randomised evidence exists for this rare injury - management rests on consistent narrative/systematic reviews and expert consensus. The table summarises how the major bodies frame hindfoot trauma principles relevant to subtalar dislocation.
- Relevant principle
- Emergent reduction of dislocations to protect skin and neurovascular status; post-reduction CT for hindfoot trauma
- Evidence level
- Expert consensus (Level V)
- Relevant principle
- Open dislocations follow open-fracture pathway: early IV antibiotics, combined ortho-plastics, debridement and early coverage
- Evidence level
- Consensus standard
- Relevant principle
- Senior decision-making, CT for complex foot/hindfoot trauma, early definitive care in specialist centres
- Evidence level
- Guideline (consensus-based)
- Relevant principle
- Direction-based reduction manoeuvre, accentuate-then-reverse technique, CT to define associated fractures
- Evidence level
- Expert/teaching consensus
- Relevant principle
- Recognises subtalar dislocation as high-energy injury needing urgent reduction and associated-injury work-up
- Evidence level
- Narrative consensus
Registry Evidence
There is no dedicated joint registry for subtalar dislocation; national arthroplasty registries (AOANJRR, NJR, AJRR) do not capture this injury. Where late post-traumatic subtalar arthritis proceeds to subtalar or triple arthrodesis, those fusion procedures are captured only indirectly in some national trauma/procedure datasets, and outcome evidence remains limited to single-centre series.
Practice Variation
Reported management varies chiefly in three areas with no consensus standard (Byrd et al, 2013): adjunctive percutaneous K-wire fixation (used selectively for residual instability vs not at all), immobilisation type (below-knee cast vs CAM boot), and duration of immobilisation (under 4 weeks vs around 6 weeks). Several series report good results with shorter immobilisation and early subtalar range of motion, consistent with DeLee and Curtis's original recommendation against prolonged casting.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old basketball player presents after a fall landing on an inverted foot. The foot is markedly deformed with an adducted and inverted position. The skin is tented over a prominent bony structure dorsolaterally. How would you manage this?”
“You are unable to reduce a subtalar dislocation despite adequate sedation. What would you do next?”
“Post-reduction CT of a subtalar dislocation shows a talar neck fracture involving 30% of the joint surface. How does this change your management?”
MCQ Practice Points
High-Yield Exam Facts
Q: What defines a subtalar dislocation? A: Simultaneous dislocation of the Talonavicular and Talocalcaneal joints, while the Tibiotalar joint remains intact.
Q: Which type is most common? A: Medial (85%) - caused by inversion (basketball foot), foot displaced medially ("acquired clubfoot").
Q: Why is skin tension an emergency? A: Tented skin over the talar head can necrose within hours. Immediate reduction is mandatory before imaging if skin is compromised.
Q: What is the reduction maneuver? A: Knee flexed (relax gastroc), Traction, Accentuate Deformity, then Reverse Deformity. Medial needs Eversion; Lateral needs Inversion.
Q: What is the critical imaging step after reduction? A: CT Scan is MANDATORY. 40% of cases have occult fractures not visible on X-ray, which may change management.
Q: What is the most common long-term complication? A: Post-traumatic arthritis (30-40% in pure dislocations, higher in fracture-dislocations).
Q: Which factors predict a worse outcome? A: Lateral dislocation, Open injury, Associated fractures, and Delayed reduction.
Q: What structure commonly blocks reduction in medial dislocations? A: The Extensor Retinaculum (buttonholing) or the EHL tendon.
Q: How do you distinguish Subtalar from Total Talar dislocation? A: In Subtalar, the Tibiotalar joint is intact. In Total Talar, the talus is dislocated from the tibia as well (extruded).
DEFINITION
- Dislocation of BOTH talonavicular AND talocalcaneal joints
- Tibiotalar joint remains INTACT
- Also called 'peritalar dislocation'
- Named by direction of FOOT relative to talus
TYPES
- MEDIAL (85%): Foot medial = acquired clubfoot
- LATERAL (15%): Foot lateral = acquired flatfoot
- Anterior and posterior are rare
- Medial has better prognosis than lateral
EMERGENCY
- Tented skin = URGENT reduction needed
- Skin necrosis within hours if unreduced
- Do NOT delay for imaging if skin compromised
- Document neurovascular status before and after
REDUCTION TECHNIQUE
- Flex knee (relax gastrocnemius)
- Longitudinal traction
- ACCENTUATE deformity first
- REVERSE: Medial = evert; Lateral = invert
CT MANDATORY
- 40% have occult fractures on CT
- Plain X-rays miss many injuries
- CT changes management in 20%
- Always scan after successful reduction
Evidence Base
Key Studies and Evidence
Long-Term Outcomes of Subtalar Dislocation
- Retrospective review of 39 subtalar dislocations over a 10-year period, mean follow-up 5.5 years (range 2-10). Medial dislocations predominated (74%) and a large proportion were open (41%); associated fractures were frequent (64%). Using Hardcastle's scoring system, results were 11 good, 7 fair and 21 poor - associated fractures and open injuries were strongly related to poor results, while good results correlated with accurate reduction.
- Key point: only 11 of 39 (28%) achieved a good result; open injuries and associated fractures drove poor outcomes
Role of CT in Subtalar Dislocation
- Retrospective review of nine subtalar joint dislocations over three years. Plain films diagnosed the dislocation in every patient, but post-reduction CT identified additional injuries missed on plain radiographs in 100% of patients, and in 44% the new information dictated a change in treatment.
- Key point: CT is mandatory after reduction - it detected occult associated injuries in all cases and changed management in 44%
Subtalar Dislocation of the Foot (Classic Series)
- Classic series of 17 subtalar dislocations (1 anterior, 12 medial, 4 lateral); 14 closed and 3 open, with 2 of the 4 lateral dislocations being open. Associated talocalcaneal or talonavicular fractures occurred in 8 feet (some seen only on post-reduction polytomography). Associated articular fractures, open dislocations, and the need for immobilisation beyond three weeks produced poor results, with lateral dislocations particularly prone to poor outcomes.
- Key point: lateral dislocations fare worst because of their high open-injury and associated-fracture burden; early range of motion after short immobilisation is favoured
Systematic Review of 528 Subtalar Dislocations (25 years)
- Systematic review of 76 articles reporting 528 cases (1988-2012). Males (76%) and the right foot (61%) predominated; mean age 33.8 years. Mechanism was a traffic accident in 43.7%, a fall in 32.9% and sport in 13.9%. Direction was medial in 71.5%, lateral in 26.0%, posterior in 1.6% and anterior in 0.8%. Open injury occurred in 22.5% and an associated osseous injury in 61.4%. Closed reduction failed (requiring immediate open reduction) in 14.0%. Pooled outcomes were good in 52.3%, fair in 25.2% and poor in 22.5%.
- Key point: the largest pooled dataset confirms medial dominance (~72%), a substantial open-injury rate (~23%), and that roughly one in seven dislocations is irreducible closed
Narrative Review: Subtalar Dislocation Characteristics and Pitfalls
- Narrative review of 47 articles (389 cases) over thirty years. Medial dislocations (68.1%) outnumbered lateral (27.7%). Bone exposure (44.5%), associated lesions (44.5%) and the need for surgical (open) reduction (48.2%) were far more frequent in lateral dislocations than in other directions. Post-reduction CT is recommended in all cases.
- Key point: lateral dislocations concentrate the difficulty - open wounds, associated injuries and irreducibility cluster in this subgroup
Management and Prognosis Review
- Up-to-date review confirming subtalar dislocation represents approximately 1% of all traumatic foot injuries and 1-2% of all dislocations, typically from high-energy trauma. Irreducible injuries have been reported in 0 to 47% of cases. The most frequent associated fractures involve the posterior process of the talus, talar head, lateral and medial malleoli, and the base of the fifth metatarsal. Early closed reduction is advised, proceeding to open reduction without delay if unsuccessful.
- Key point: incidence is ~1% of foot injuries; irreducibility ranges widely (0-47%) and mandates readiness for open reduction
Summary of Evidence
- Most studies are case series and retrospective reviews
- No randomized controlled trials exist
- Injury is too rare for prospective trials
- Medial dislocation is most common (pooled ~68-72% in large systematic reviews; classically quoted as 85%)
- Post-reduction CT detects associated injuries missed on plain films and changes management in a substantial minority (44% in the Bibbo series)
- Open and lateral dislocations have worse outcomes
- Early reduction is critical for skin viability
- Closed reduction is irreducible in roughly 14% of cases (range 0-47% across series), requiring open reduction
- Post-traumatic arthritis is the most common long-term complication
- Optimal immobilization duration not well-defined
- Role of K-wire stabilization unclear
- Rehabilitation protocols not standardized
- Long-term functional outcome studies needed