Common Pediatric Foot Deformity
Bleck Classification (Heel Bisector)
Critical Must-Knows
- Heel Bisector Method (Bleck) for severity classification
- Flexibility determines treatment (Observation vs Casting)
- Hindfoot is Neutral/Valgus - differentiates from Clubfoot (Varus)
- Association with DDH (10-15%) - must check hips
- Kidney Bean shape foot with deep medial crease
Clinical Pearls
- "Differentiate from Skewfoot (Z-deformity) and Clubfoot (Hindfoot Varus)
- "Rigid deformity greater than 6 months needs casting
- "Surgery is rare - avoid performing too early (less than 5 years) due to physeal injury risk
- "Benign natural history in flexible cases
Differentiation is Key
In the exam, immediately distinguish Metatarsus Adductus from Skewfoot (Z-deformity) and Clubfoot (TEV). In Metatarsus Adductus, the hindfoot is neutral or in slight valgus, whereas in Clubfoot it is in varus, and in Skewfoot, it is in valgus with uncorrected forefoot adduction. Always check the hips for DDH!
Metatarsus Adductus: Quick Reference
| Category | Key Points | |
|---|---|---|
| Most common congenital foot deformity | 1:1000 live births | 50% bilateral |
| Adduction of metatarsals at Lisfranc joint | Normal or Valgus Hindfoot | Medial soft tissue tightness |
| Bleck (Heel Bisector): Mild (3rd toe), Mod (3-4 web), Severe (4-5 web) | Flexibility: Flexible vs Rigid | |
| Flexible: Observation (90% resolve) | Rigid/Late: Serial casting (standard treatment) | Resistant (greater than 4 years): Osteotomies |
| DDH (10-15%) - Mandatory Hip Exam | Torticollis (Packaging disorder) |
MHTPackaging Disorders
| M | Metatarsus Adductus Foot deformity |
| H | Hip Dysplasia (DDH) 10-15% association |
| T | Torticollis Neck deformity |
| M | Metatarsus Adductus Foot deformity |
| H | Hip Dysplasia (DDH) 10-15% association |
| T | Torticollis Neck deformity |
Hook:M-H-T: The Packaging Pack. Check all three!
33/44/5Bleck Severity
| 3 | 3rd Toe Mild |
| 3/4 | 3rd-4th Webspace Moderate |
| 4/5 | 4th-5th Webspace Severe |
| 3 | 3rd Toe Mild |
| 3/4 | 3rd-4th Webspace Moderate |
| 4/5 | 4th-5th Webspace Severe |
Hook:Heel bisector moves laterally with severity (3 to 4 to 5)
MSCDifferential Diagnosis
| M | Metatarsus Adductus Hindfoot Neutral |
| S | Skewfoot Hindfoot Valgus |
| C | Clubfoot Hindfoot Varus |
| M | Metatarsus Adductus Hindfoot Neutral |
| S | Skewfoot Hindfoot Valgus |
| C | Clubfoot Hindfoot Varus |
Hook:Look at the hindfoot to distinguish the diagnosis!
Overview/Epidemiology
Metatarsus Adductus is a benign, self-limiting congenital foot deformity caused by intrauterine packaging. It is characterized by adduction of the forefoot at the tarso-metatarsal joints while the hindfoot remains normally aligned (or in slight valgus). This condition is distinct from Clubfoot (Talipes Equinovarus) where the hindfoot is in varus and equinus.
Aetiology: The exact aetiology is multifactorial but strongly linked to mechanical factors in utero.
- Intrauterine Packaging: The most widely accepted theory. Increased pressure in a growing fetus, particularly in firstborns or in oligohydramnios, forces the feet into an adducted position against the uterine wall. This mechanical compression explains the strong association with other "packaging disorders" like muscular torticollis (sternocleidomastoid contracture) and Developmental Dysplasia of the Hip (DDH).
- Genetics: Familial tendency (polygenic inheritance). There is a higher incidence in siblings of affected patients (approx 1 in 20).
- Muscular Imbalance Theory: Some theories propose an imbalance between the abductor hallucis (which is found to be hypertrophied and tight) and the peroneal muscles (which are weak/lengthened). However, it is debated whether this is a primary cause or secondary to the deformity. The tibialis posterior tendon is also typically shortened.
Epidemiology:
- Incidence: Approximately 1 in 1000 live births. However, mild cases are often underdiagnosed or resolve so quickly they are not recorded in birth registries.
- Gender: Generally reported as equal Male = Female, though some series show a slight female predominance (similar to DDH).
- Laterality: Bilateral in approximately 50-60% of cases. In unilateral cases, the left foot is slightly more commonly affected, ostensibly due to the common position of the fetus (Left Occiput Anterior).
- Birth Order: Significantly more common in firstborn children due to the "tight" nulliparous uterus (known as the "primigravida effect").
History of Treatment:
Historically, treatment involved forceful manipulation and strapping, or aggressive soft tissue releases (Heyman-Herndon). Long-term follow-up studies (Rushforth, Farsetti) demonstrated the benign natural history, leading to a shift towards observation for flexible cases and serial casting for rigid ones. Surgical intervention is now strictly reserved for older children with persistent rigid deformity causing symptoms.
Pathophysiology and Biomechanics
Pathoanatomy: The deformity is primarily located at the Lisfranc Joint (Tarsometatarsal joint).
- Metatarsals: All metatarsals are adducted (deviated medially) relative to the cuneiforms and cuboid. The 1st metatarsal is often the most severely affected.
- Cuneiforms: The medial cuneiform is often misshapen (trapezoidal or wedge-shaped with the base lateral). This bony deformity helps maintain the adduction of the 1st ray.
- Navicular: Usually laterally subluxated on the talus head in Clubfoot, but in Metatarsus Adductus, the navicular position is relatively normal or slightly lateral.
- Hindfoot (Subtalar Joint): CRITICAL FEATURE. The calcaneus and talus are in a normal divergent relationship or in slight valgus. The talocalcaneal angle is normal. This is the key differentiator from Clubfoot (where the hindfoot is in varus and equinus) and Skewfoot (where the hindfoot is in distinct valgus).
- Soft Tissue Contractures:
- Medial: Tightness of the abductor hallucis muscle, tibialis posterior tendon, and the medial tarsometatarsal joint capsules.
- Lateral: Attenuation (lengthening) of the peroneal muscles (peroneus brevis and longus) and the lateral soft tissues.
Associated Anatomy:
- Acetabulum: Due to the association with DDH, the hip anatomy may be abnormal (dysplastic). Careful screening is mandatory.
- Sternocleidomastoid: May be contracted (Torticollis), leading to head tilt and rotation.
Biomechanics of Gait: If untreated, the adducted forefoot leads to an intoeing gait (pigeon-toed). Children often compensate by externally rotating the tibia or hip to bring the foot progression angle to neutral. This can lead to complex rotational profiles later in life ("squinting patellae" if femoral anteversion is also present). However, functional limitation is rare, and the condition is largely cosmetic in adulthood unless severe.
Classification Systems
Bleck Classification (Heel Bisector Method)
This is the most clinically useful classification. It is based on the relationship of the Heel Bisector Line to the toes.
Technique: With the patient prone and knees flexed 90 degrees, imagine a line bisecting the elliptical heel pad and extend it distally to the toes.
- Normal: The line passes between the 2nd and 3rd toes.
- Mild: The line passes through the 3rd toe.
- Moderate: The line passes through the 3rd-4th webspace.
- Severe: The line passes through the 4th-5th webspace.
This classification correlates well with the prognosis and need for treatment.
Clinical Assessment
History:
- Onset: Note when the deformity was first noticed (birth vs later). Late onset suggests localized pathology or mimicking conditions.
- Family History: Ask about foot deformities, hip dysplasia, or "packaging" issues in siblings/parents.
- Pregnancy History: Breech presentation, oligohydramnios, first obstetric event.
- Gait: If walking, describe the foot progression angle (Intoeing). Parents often report the child "trips over their own feet".
Physical Examination:
-
Inspection:
- Forefoot Adduction: "Kidney Bean" shape.
- Lateral Border: Convex.
- Medial Crease: Deep crease in midfoot suggests rigidity.
- Hindfoot: Neutral or slight valgus (NOT varus - that suggests Clubfoot).
- Base of 5th: Prominent styloid.
- Toe Splaying: Often a widened gap between the 1st and 2nd toes (resembling a thumb separation).
-
Heel Bisector Test: Perform with child prone. Determine the Bleck grade (Normal, Mild, Mod, Severe).
-
Flexibility Assessment: Stabilize the hindfoot with one hand. Use the other hand to apply valgus pressure to the forefoot. Can you get it to neutral? Past neutral? This dictates management.
-
Lateral Border Stimulation (Tickle Test): Stroke the lateral border of the foot. A flexible foot will actively abduct due to peroneal muscle contraction. A rigid foot will not.
-
Hindfoot Exam: CRITICAL STEP. Verify the hindfoot is neutral or valgus. If it is in varus, suspect Clubfoot. If it is in severe valgus with a rigid adducted forefoot, suspect Skewfoot.
-
Hip Examination: MANDATORY. Perform Ortolani and Barlow maneuvers to rule out DDH. Document hip range of motion.
-
Spine Exam: Rule out spinal dysraphism (hairy patch, dimple) which can cause foot deformities (e.g., cavovarus, but always good to check).
Investigations
Plain Radiographs (Weight Bearing AP/Lateral):
- Infants: Generally NOT indicated. The tarsal bones are largely cartilaginous and not visible. Diagnosis is clinical.
-
- Heel Bisector Line (Bleck): Normal passes through 2nd/3rd toe webspace. In MA, it passes lateral to the 3rd toe (through 4th or 5th toe).
- Metatarsus Adductus Angle: Angle between axis of tarsus and metatarsals (greater than 20 degrees is abnormal).
- Engel's Angle: Angle between the 2nd metatarsal and the intermediate cuneiform. Normal is less than 24 degrees.
- Talocalcaneal Angle (Kite's Angle):
- Normal/MA: 20-40 degrees (divergent).
- Clubfoot: Parallel (less than 15 degrees).
- Skewfoot: Increased (greater than 40 degrees) due to hindfoot valgus.
Ultrasound:
- Hip Ultrasound: Indicated for any infant with Metatarsus Adductus if there are clinical risk factors or uncertain hip exam findings, due to the high association with DDH.
CT/MRI:
- Rarely indicated. May be used for complex tarsal coalition workup if rigidity is unexplained.
Management Algorithm
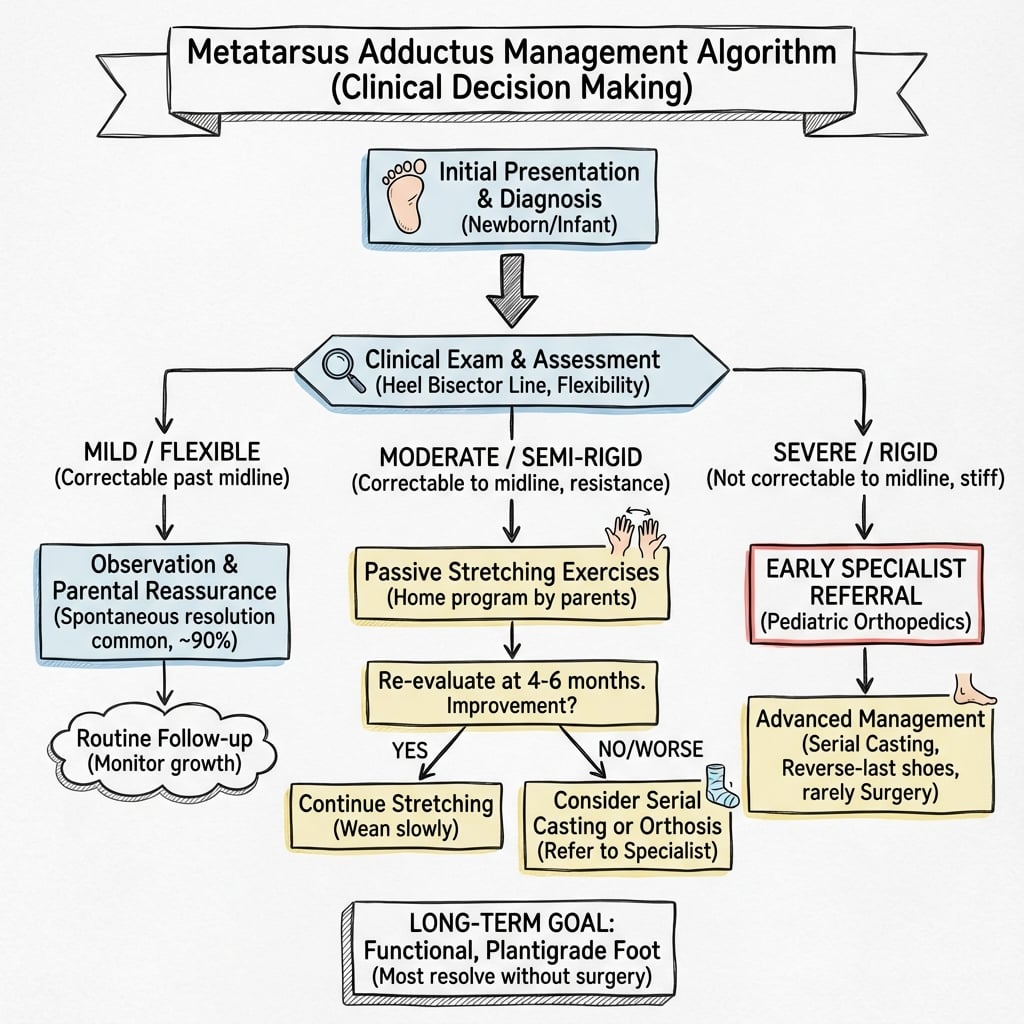
Management of Flexible Deformity
Population: Infants under 6 months, Type I/II flexibility.
- Observation: The mainstay of treatment. Explain to parents that over 90% resolve spontaneously. This requires parental reassurance and patience.
- Stretching:
- Technique: The "abduction stretch". Parents stabilize the heel with one hand and gently push the forefoot into abduction with the other. Hold for 5-10 seconds. Repeat 5 times at each diaper change.
- Evidence: Limited evidence it changes natural history, but empowers parents ("active waiting").
- Follow-up: Review in 3-4 months to ensure resolution. If becoming rigid, escalate.
(Note: Ensure list items are not directly before closing tag)
Surgical Technique
Multiple Metatarsal Osteotomies (Berman-Gartland)
Principles: Realign the forefoot by cutting the metatarsal bases. Doing this in a child over 5 avoids damaging the proximal physis of the metatarsals (especially the 1st).
Initial Setup:
- Supine position, tourniquet control.
- Fluoroscopy available (though often done clinically).
Approach:
- Two or three dorsal longitudinal incisions.
- Incision 1: Between 1st and 2nd ray.
- Incision 2: Between 3rd and 4th ray.
- Protect the superficial peroneal nerve branches and extensor tendons.
Osteotomies:
- 1st Metatarsal: Proximal metaphysis. Often done as an Opening Wedge (medial) to add length and correct adduction. Can insert a small bone graft wedge (from bank or local).
- 2nd, 3rd, 4th Metatarsals: Closing Wedge laterally at the bases. The wedge base is lateral. Closing it swings the metatarsal laterally.
- 5th Metatarsal: Oblique osteotomy.
Fixation:
- Smooth K-wires (1.6mm or similar). Retrograde fixation from the metatarsal head into the tarsus, or crossed pins at the osteotomy site.
- Plate fixation is difficult due to small size but possible in older children.
Closure:
- Layered closure.
- Apply a well-molded short leg cast.
Post-op:
- Non-weight bearing for 6 weeks.
- Pin removal at 6 weeks.
- Walking cast for further 2-4 weeks if needed.
(Note: Ensure list items are not directly before closing tag)
Complications
| Complication | Risk Factors | Prevention/Management |
|---|---|---|
| Skewfoot (Iatrogenic) | Forced abduction of forefoot against a valgus hindfoot during casting. | Prevention: Proper Casting Technique. Stabilize the hindfoot in neutral/varus while abducting the forefoot. Do not simply "crank" the foot lateral. Management: Surgical correction (calcaneal osteotomy) if rigid. |
| Skin Pressure Sores | Poor cast molding, inadequate padding, tight cast. | Prevention: Careful padding of bony prominences (base of 5th MT, heel). Frequent cast checks. Management: Remove cast, wound care, bivalve next cast. |
| Physeal Arrest | Surgical damage to proximal physis of 1st MT. | Prevention: Perform osteotomies in older children (greater than 5 years). Identify physis on fluoro. Management: Epiphysiodesis if discrepancy significant. |
| Recurrence | Inadequate duration of treatment, failure to use maintenance shoes. | Prevention: Ensure overcorrection (past neutral) before stopping casting. Use reverse-last shoes. Management: Recasting or Osteotomies. |
| Dorsal Bunion | Imbalance of tibialis anterior or FHL; complication of TMT resection. | Prevention: Avoid extensive TMT releases (Heyman-Herndon). Use osteotomies instead. Management: Tibialis anterior transfer or osteotomy. |
| Joint Stiffness | Intrusion into TMT joints during surgery. | Prevention: Extra-articular osteotomies preferred over Capsulotomies. Management: Physiotherapy, analgesia. |
| Metatarsalgia | Altered forefoot mechanics post-osteotomy. | Prevention: anatomic realignment. Management: Orthotics, offloading pads. |
Postoperative Care
Immediate Post-operative Phase (0-2 Weeks):
- Immobilization: Non-weight bearing (NWB) short leg cast or backslab is applied in the operating room.
- Elevation: Strict elevation for the first 48 hours to minimize oedema and pain.
- Neurovascular Monitoring: Routine checks for toe perfusion, sensation, and movement (prevent compartment syndrome, though rare in foot).
Intermediate Phase (2-6 Weeks):
- Wound Check: At 2 weeks, the initial cast/splint is removed to inspect the incisions. Sutures are removed if non-absorbable.
- Re-casting: A definitive fiberglass short leg cast is applied. The foot is held in the corrected position.
- Weight Bearing: Continues to be Non-Weight Bearing to allow osteotomy union without displacement.
Union Phase (6 Weeks):
- Pin Removal: If percutaneous K-wires were used, they are removed in the clinic (or under sedation if buried).
- Radiographs: Check for callus formation and osteotomy union.
- Mobilization: Transition to a weight-bearing walking cast or a stiff-soled shoe (e.g., Darco shoe) for a further 2-4 weeks depending on radiographic consolidation.
Rehabilitation Phase (3 Months onwards):
- Shoe Wear: Return to normal footwear. Broad-toe box shoes recommended.
- Activity: Gradual return to running and sports.
- Follow-up: Annual reviews to monitor for recurrence or growth disturbance until skeletal maturity.
Outcomes/Prognosis
- Natural History: Excellent. In the Iowa long-term cohort (Farsetti/Weinstein/Ponseti, mean 32.5-year follow-up) every passively correctable foot resolved spontaneously and 90% of conservatively treated rigid feet had good results, with no poor results. Even mild residual deformity is compatible with normal function and shoe wear.
- Non-Operative: Serial casting and graded orthosis pathways achieve a greater than 90% success rate for flexible/rigid deformities, best when started in the first year of life.
- Operative: Good cosmetic correction. Functional outcomes are generally good, but there is a risk of midfoot stiffness and metatarsalgia in the long term.
- Adult Sequelae: A long-held teaching links untreated metatarsus adductus to later hallux valgus and lateral-column overload; however the Iowa long-term data found hallux valgus was NOT a common outcome, so this association is now considered weak/debated.
Evidence Base
- 31 patients (45 feet) followed a mean of 32.5 years (Iowa cohort)
- All 16 passively correctable (untreated) feet had good results; 26/29 (90%) conservatively treated feet were good, with no poor results
- Hallux valgus was NOT a common late outcome; residual medial cuneiform-metatarsal obliquity was frequent but asymptomatic
- 2,156 newborns screened; 124 diagnosed with congenital metatarsus varus (prevalence 5/1000), graded by Bleck classification
- 122 flexible/semi-flexible feet treated with manipulation (52 corrected) then Bebax-type braces (70); only 2 rigid feet needed casting
- Only 2 superficial skin ulcerations, all healed within a week
- 25 children (41 feet) randomised to static vs dynamic anti-varus orthosis, scored on the Bleck scale
- Both orthosis types were effective; the best results were achieved with EARLY treatment
- No child had residual deformity interfering with daily activities at minimum 2-year follow-up (IOWA score)
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Worried Parents
"Parents bring six-week-old infant with intoeing. They are worried about clubfoot. How do you assess?"
I would take a history regarding birth (breech, oligohydramnios) and family history. On examination, I would inspect the foot shape (kidney bean), assess the hindfoot (Neutral/Valgus in MA vs Varus in Clubfoot), and test flexibility (midline). I would critically examine the hips for DDH. If flexible and hindfoot neutral, I would diagnose Metatarsus Adductus and reassure the parents that 90% resolve spontaneously. I would demonstrate passive stretching.
The Rigid Presenter
"8-month-old with rigid Metatarsus Adductus. Heel bisector through 4th toe. Stretches failed. Plan?"
This is a rigid, persistent deformity in an older infant. Observation is no longer appropriate. I would recommend serial casting. I would use long-leg casts to control rotation, molding the forefoot into abduction while stabilizing the hindfoot to avoid creating a skewfoot. Changes every 2 weeks, typically 3 casts required. Success rate is high.
The Surgical Candidate
"6-year-old with painful rigid metatarsus adductus. Failing shoe wear. Parents request surgery. Discuss."
I would first confirm the symptoms are due to the deformity (likely lateral border pain). I would counsel the parents that surgery is major, involves bone cuts, and carries risks of stiffness and scarring. If they wish to proceed, I would plan for multiple metatarsal osteotomies. I would avoid soft tissue releases at this age. I would plan for a closing wedge of 2-4 and opening wedge of 1. Post-op NWB cast for 6 weeks.
MCQ Practice Points
Bleck's Classification
Q: What is the radiographic reference line for Metatarsus Adductus severity? A: Heel Bisector Line. Normal = 2nd toe. Mild = 3rd toe. Moderate = 3rd/4th webspace. Severe = 4th/5th toe.
Treatment Timing
Q: When should casting be initiated for rigid Metatarsus Adductus? A: Ideally before 8 months of age. After 1 year, casting is less effective due to bone ossification.
Differential Key
Q: How do you differentiate MA from Skewfoot? A: In MA, the hindfoot is neutral/valgus. In Skewfoot (Serpentine Foot), the hindfoot is in severe valgus AND the forefoot is adducted (Z-deformity).
Diagnosis MCQ
Q: What is the most common differential diagnosis for Metatarsus Adductus? A: Clubfoot (Talipes Equinovarus). Metatarsus Adductus has a neutral or valgus hindfoot.
Bleck Line MCQ
Q: A Heel Bisector Line passing through the 4th/5th toe webspace indicates what severity? A: Severe. Normal is 2nd toe. Mild is 3rd toe. Moderate is 3rd/4th webspace.
Differential Diagnosis
The cardinal exam discriminator is the hindfoot. Examine it first.
The Adducted/Intoeing Foot: Differential Diagnosis
| Condition | Hindfoot | Forefoot | Key Distinguishing Feature |
|---|---|---|---|
| Neutral or slight valgus | Adducted, lateral border convex | Flexible in most; isolated forefoot problem; no equinus | |
| Fixed VALGUS | Rigid adduction + lateral midfoot translation | S-shaped foot; talocalcaneal angle increased; can be iatrogenic from casting | |
| VARUS + equinus | Adducted + cavus | Rigid; calcaneus high and inverted; emptyheel; talocalcaneal angle parallel | |
| Normal | Normal foot shape | Intoeing from rotation, not foot deformity; thigh-foot angle internal | |
| Normal | Normal foot shape | Squinting patellae; intoeing in older toddler; W-sitting | |
| Normal | Isolated great-toe medial deviation | Only the hallux deviates; rest of forefoot normal |
Controversies & Areas of Uncertainty
- Magnitude of the DDH association: The classic teaching of a 10-15% DDH rate derives from small, selected, often historical series. The 60,844-child Norwegian cohort (Håberg 2020) found metatarsus adductus carried only a marginal 1.5% DDH risk, far lower than calcaneovalgus or clubfoot. Whether every infant with isolated flexible MA needs hip ultrasound (versus careful clinical hip exam and selective imaging) is therefore debated — but the hip exam itself is never optional.
- Does stretching change natural history? Parental passive stretching is widely taught for flexible feet, yet high-quality evidence that it alters the (already excellent) natural history is lacking. It is best framed as low-cost "active waiting" and reassurance, not a disease-modifying treatment.
- Casting vs dynamic orthoses for rigid feet: Serial casting is the traditional gold standard, but braces (Bebax, Wheaton) and graded manipulation pathways report comparable correction with fewer skin issues (Rocca 2022). Optimal modality is not settled; early initiation is the consistent predictor of success across studies.
- Surgery threshold and technique: Surgery is rare and reserved for the symptomatic older child. Soft-tissue (Heyman-Herndon) releases have fallen out of favour due to stiffness and dorsal bunion; metatarsal/cuneiform osteotomies are preferred but carry physeal and metatarsalgia risks. Optimal age and bony procedure remain individualised.
- Hallux valgus link: Long quoted as an adult sequela, but the Iowa long-term data found hallux valgus was NOT common, undermining a routine "this will become a bunion" counselling line.
Guidelines, Registries & Global Practice
Global epidemiology:
- Most common congenital foot deformity; reported incidence roughly 1 in 1000 live births, with prospective newborn screening series finding higher prevalence (up to 5 in 1000, Rocca 2022) because mild flexible cases are otherwise underdiagnosed.
- Bilateral in 50-60%; more frequent in firstborns and with intrauterine crowding (oligohydramnios, multiple gestation, breech) — part of the "packaging" cluster with DDH and torticollis.
Side-by-side guidance (where bodies comment):
| Body / Source | Position on flexible MA | Position on rigid MA | Hip screening stance |
|---|---|---|---|
| AAOS / POSNA (US) | Observation + reassurance; natural history excellent | Serial casting; orthoses as adjunct | Examine hips routinely; image if exam abnormal or risk factors |
| BOA / RCH-type UK & Commonwealth pathways | Reassurance, parent stretching as "active waiting" | Casting/bracing in casting clinics (often physio-led) | Clinical hip exam mandatory; selective ultrasound |
| AO / Pediatric trauma-deformity texts | Observe; avoid overtreatment | Three-point molded casting, then maintenance shoes | Screen per national DDH program |
| EFORT / European consensus | Conservative; early treatment favoured if intervening | Graded manipulation then orthosis or cast | Hip surveillance integrated with national DDH screening |
- Registry / cohort signal: Large population data (Norwegian birth cohort, Håberg 2020) reclassify MA as a low-magnitude DDH risk factor relative to other foot deformities — informing more proportionate hip-imaging policy.
High- vs limited-resource practice variation:
- High-resource: Newborn orthopaedic screening, casting clinics, adjustable braces (Bebax/Wheaton), and ultrasound hip surveillance are available; emphasis is on avoiding overtreatment of self-limiting flexible feet.
- Limited-resource: Diagnosis is clinical; mainstays are parental education, manipulation, and simple straight-last/reverse-last footwear. Serial plaster casting is low-cost and effective where braces are unavailable. Rare surgical cases may present late, increasing the role of osteotomy over early conservative care.
Exam Tip
Always examine the hips. Missing a dislocated hip because you focused on the foot is a fail — even though the absolute DDH risk with isolated flexible metatarsus adductus is now known to be low.
METATARSUS ADDUCTUS
Clinical summary
Key Features
- •Kidney Bean Foot
- •Medial Crease
- •Lateral Border Convex
- •Normal Hindfoot (Neutral)
Classification
- •Flexible (Corrects past midline)
- •Partly Flexible (To midline)
- •Rigid (Fixed Adduction)
- •Resistant (Severe)
X-ray Findings
- •Metatarsus Adductus Angle greater than 20
- •Heel Bisector Line (Bleck)
- •Lateral to 2nd toe space
- •Normal Hindfoot Valgus
Management
- •Observation (Flexible)
- •Strethcing (Careful)
- •Serial Casting (Rigid)
- •Operation (Rare, greater than 4yrs)
Associated Conditions
- •DDH (10-15%)
- •Torticollis
- •Plagiocephaly
- •Packaging Disorders