Non-dissociative carpal instability (CIND) with abnormal motion between the proximal and distal carpal rows
- Pathognomonic: painful catch-up clunk during ulnar deviation under load
- Palmar MCI = reducible VISI (scapholunate angle under 30 degrees)
- Midcarpal shift test (Lichtman) reproduces symptoms
- Diagnosis is clinical plus dynamic fluoroscopy; static films often normal
- Conservative first; dorsal capsulodesis / soft-tissue reefing for refractory cases
- “Non-dissociative: intrinsic SL and LT ligaments are INTACT
- “Distinguish from static VISI of lunotriquetral dissociation (dissociative)
- “Beighton score quantifies the underlying constitutional laxity
- “No randomised or comparative trials exist; treatment is individualised
Epidemiology and Natural History
MCI is uncommon, accounting for a small minority of carpal instabilities, and is widely regarded as under-diagnosed - many patients are initially labelled with wrist "sprain", ganglion, or TFCC pathology, with diagnostic delays often measured in many months. There is a clear female predominance (around 4:1) and a young age at presentation (second to fourth decades). Generalised ligamentous laxity (positive Beighton score) is present in 60-70%, and a subset have bilateral symptoms, supporting a constitutional rather than purely traumatic aetiology. A discrete antecedent injury (dorsiflexion / ulnar-deviation loading) is reported in a minority. Untreated, the course is typically chronic with mechanical pain, clunking and grip weakness; progression to frank midcarpal arthritis is less frequent than after dissociative instabilities such as scapholunate dissociation. Spontaneous resolution is rare in adults but may occur in adolescents with maturity.
Anatomy and Carpal Kinematics
Two-Row Carpal System
The proximal row (scaphoid, lunate, triquetrum) is an intercalated segment with no direct tendon attachments - its position is controlled entirely by ligamentous balance between the radius and the distal row (trapezium, trapezoid, capitate, hamate). In normal kinematics the proximal row extends with radial deviation and flexes (palmar-flexes) with ulnar deviation, a smooth transition governed by the palmar and dorsal carpal ligaments.
Key Stabilisers
The palmar midcarpal ligaments - principally the triquetrohamate-capitate ligament (ulnar arm of the arcuate/deltoid ligament) and the scaphotrapeziotrapezoid (STT) complex - act as a sling from the distal row to the proximal row, restraining excessive palmar flexion. The dorsal radiocarpal (DRC) ligament provides important secondary restraint, and DRC insufficiency is increasingly recognised as a driver of palmar MCI.
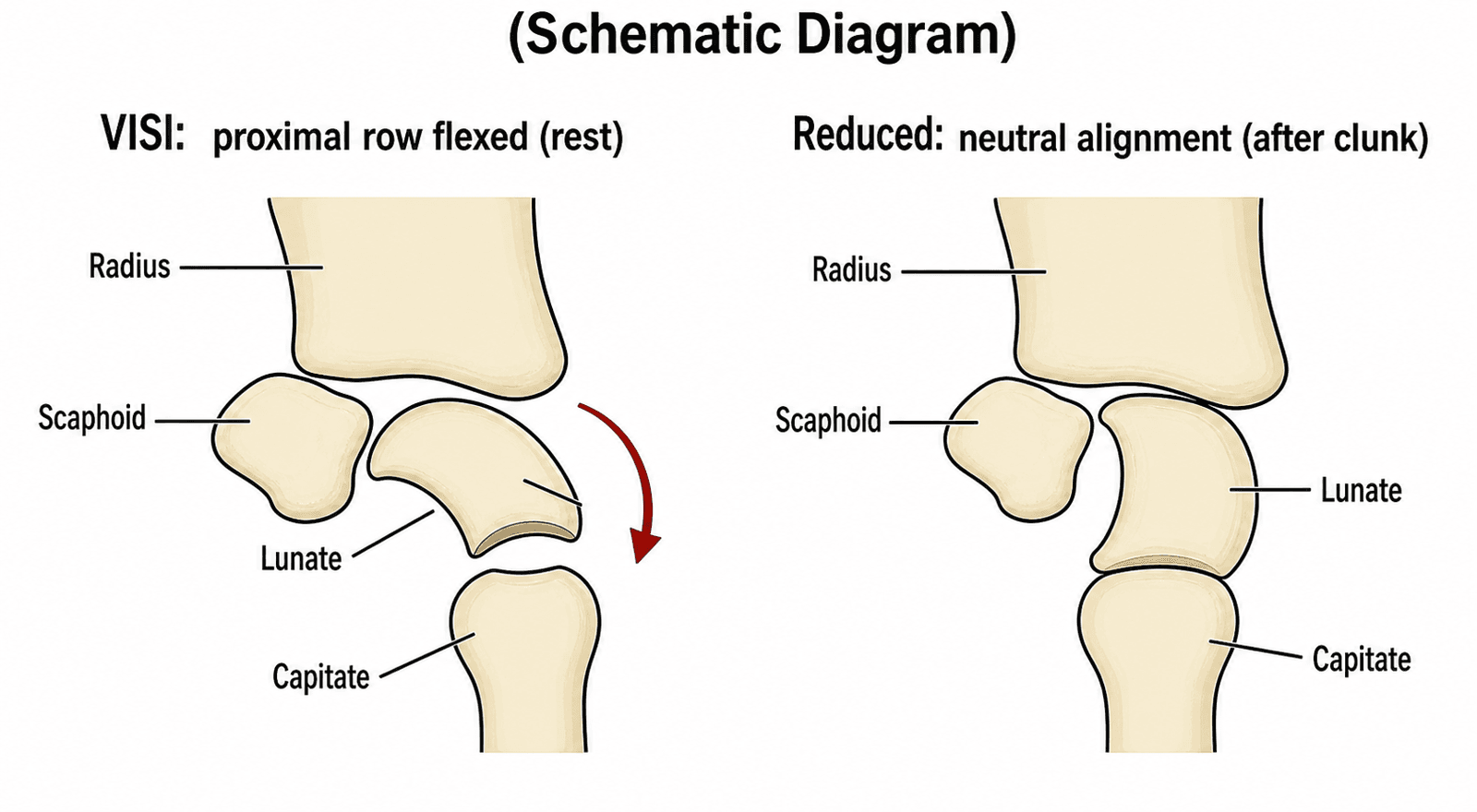
The Catch-Up Clunk Explained
- At rest the lax palmar midcarpal ligaments allow the proximal row to drop into VISI (palmar flexion).
- As the wrist moves from radial toward ulnar deviation under load, force builds across the midcarpal joint.
- The lax ligaments eventually yield and the proximal row suddenly "catches up" - snapping from VISI to neutral/slight extension with reduction of the palmarly subluxed capitate.
- This abrupt shift is the audible/palpable clunk that reproduces the patient's symptoms.
Classification
Lichtman Classification of Palmar Midcarpal Instability
The Lichtman system, based on the degree and reducibility of VISI, remains the most widely cited framework.
- Description
- VISI only with provocative load; often minimally symptomatic
- Imaging
- Normal resting film; clunk on fluoroscopy
- Treatment emphasis
- Conservative / proprioceptive rehab
- Description
- VISI at rest, corrects with radial deviation or grip
- Imaging
- VISI on lateral view, reducible
- Treatment emphasis
- Conservative then soft-tissue stabilisation
- Description
- Persistent VISI not fully correctable
- Imaging
- Fixed VISI on all views
- Treatment emphasis
- Soft-tissue stabilisation / capsulodesis
- Description
- VISI with established midcarpal degeneration
- Imaging
- Arthritis on radiograph
- Treatment emphasis
- Salvage - limited fusion
Anatomic and Functional Subtypes
- Palmar MCI (80-90%) - palmar midcarpal / DRC ligament laxity producing reducible VISI. The classic clunking presentation.
- Dorsal MCI (rare, under 10%) - dorsal capsular laxity allowing the capitate to sublux dorsally out of the lunate (the "chronic capitolunate instability" described by Johnson and Carrera), tending toward a DISI-type attitude.
- Combined / global - both directions, typically in severe constitutional laxity.
- Extrinsic vs intrinsic - radiocarpal (extrinsic) vs midcarpal (intrinsic) ligament laxity; mostly combined in practice, so the distinction is largely conceptual. Hargreaves has proposed a functional staging scheme (graded by the extent of palmar translation of the distal row on stress testing) as an alternative that better reflects the dynamic nature of the disorder.
Clinical Presentation
History
Patients describe ulnar-sided wrist pain, often with an audible or palpable clunk/snap and a sense of the wrist "giving way". Symptoms are mechanical and activity-related, provoked by forceful grip with ulnar deviation (racquet sports, golf, weight-bearing through the hand, push-ups) and by repetitive loading (gymnasts, yoga). Daily tasks such as opening jars, lifting and pushing up from a chair are affected. A subset can voluntarily reproduce the clunk.
Examination
- Inspection / palpation: usually minimal swelling; dorsal and palmar midcarpal tenderness; a dorsal capitate prominence may be felt in the VISI position.
- Range of motion: typically full; grip strength is commonly reduced relative to the contralateral side.
- Generalised laxity: formal Beighton score (thumb-to-forearm, fifth-MCP and elbow/knee hyperextension, forward flexion).
- Midcarpal shift test (Lichtman) - the key manoeuvre: with the forearm pronated and stabilised, the examiner applies a palmar-directed (volar) force on the dorsal capitate while axially loading and ulnarly deviating the wrist; reproduction of the painful clunk is positive.
- Adjuncts: the catch-up clunk on passive radial-to-ulnar deviation; the supination lift test (pain/giving-way lifting against resistance with the forearm supinated); a dorsal-palmar shear test across the midcarpal joint.
Always compare with the asymptomatic contralateral wrist, since baseline laxity is common.
Provocative Test Battery in Detail
The midcarpal shift is the headline manoeuvre, but the topic names two further adjuncts - the supination lift test and the dorsal-palmar shear test - that are often left undefined. They are performed and interpreted together, always against the asymptomatic side, because no single test is diagnostic.
Supination Lift Test
With the forearm fully supinated and the hands placed flat beneath a fixed table, the patient is asked to push up against the undersurface of the table (or lift a heavy fixed object) so the extended wrist loads against resistance. Reproduction of dorsal/ulnar-sided wrist pain or a sense of the wrist giving way is positive; it stresses the ulnar midcarpal and ulnocarpal region under supinated load. Importantly it is not specific to MCI - it is also positive in TFCC and distal radioulnar joint pathology - so it supports rather than makes the diagnosis.
Dorsal-Palmar Shear (Shuck) Test
The examiner stabilises the distal row/capitate and translates it dorsally and palmarly relative to the fixed proximal row and radius. Excessive translation, a painful clunk, or apprehension indicates midcarpal laxity. It is the clinical analogue of the arthroscopic midcarpal "bounce"/trampoline assessment.
Grading and Interpretation
Provocative manoeuvres are judged by the magnitude of the shift and - decisively - whether a painful clunk that reproduces the patient's symptoms is elicited. A small, painless shift is common in lax but asymptomatic wrists and does not constitute pathology.
No single manoeuvre is diagnostic. The examiner combines the midcarpal shift, supination lift and shear tests, and then confirms that the elicited clunk is both symptomatic and reducible on dynamic fluoroscopy before labelling the wrist unstable. A positive test in a painless hypermobile wrist is laxity, not disease.
Investigation
Radiographs
Standard PA, lateral and oblique views are frequently normal. The lateral may show VISI - capitolunate angle over 15 degrees with palmar lunate tilt and scapholunate angle under 30 degrees - but only if the wrist is genuinely relaxed and neutral; inadvertent radial deviation masks it. Reference angles: capitolunate normally under 15 degrees, scapholunate normally 30-60 degrees, radiolunate around 0 degrees.
Dynamic Video Fluoroscopy (Key Confirmatory Test)
Real-time imaging through full radial-to-ulnar deviation under load captures the catch-up clunk as the proximal row shifts abruptly from VISI to neutral. It also demonstrates reducibility, the feature that separates MCI from fixed dissociative VISI. Side-by-side comparison with the opposite wrist aids interpretation in subtle cases. 4D (dynamic) CT has been described as an emerging adjunct, characterising lunate triggering and capitate subluxation along the radius-lunate-capitate axis.
MRI and Arthroscopy
MRI is usually normal in isolated MCI because the lesion is ligamentous attenuation, not rupture; its main value is excluding TFCC tears, lunotriquetral dissociation and occult fracture. Arthroscopy allows direct grading of midcarpal laxity (a "trampoline"/bounce assessment with the probe) and identification of associated pathology, and can be therapeutic (capsular shrinkage). However, neither MRI nor arthroscopy reliably confirms MCI on its own - the diagnosis remains clinical and fluoroscopic.
Original surgical series defining palmar MCI - fusion outperformed soft-tissue repair
- 13 patients, 15 procedures for palmar MCI, mean follow-up 48 months, 100% follow-up
- All 6 limited midcarpal arthrodeses were successful
- 6 of 9 soft-tissue reconstructions FAILED
- The most successful soft-tissue option was distal advancement of the ulnar arm of the arcuate ligament combined with dorsal capsulodesis (stable in 3 of 5)
Carpal instability non-dissociative (CIND) - large series, modest results
- 45 patients with proximal-row instability and intact intrinsic interosseous ligaments (arthrographically/surgically confirmed)
- Mean follow-up 5.8 years; 7 treated non-operatively, 38 operatively
- Only 56% good/excellent overall, with NO significant difference between surgical and non-surgical groups
- Best results were in ulna-minus CIND treated by joint-levelling osteotomy (83% good/excellent)
Chronic capitolunate (dorsal midcarpal) instability and the dorsal stress test
- 12 young patients with vague pain, weakness and clicking after a remote dorsiflexion injury, with normal plain films
- A fluoroscopically controlled dorsal-displacement stress test reproduced dorsal capitate subluxation out of the lunate with apprehension and a painful click
- Attributed to radiocapitate (palmar) ligament attenuation; 11 underwent volar ligament tightening
- Results: 6 excellent, 3 good, 1 fair, 1 poor; mean loss 15 degrees extension and 19 degrees flexion
Differential Diagnosis
The differential for ulnar-sided wrist pain with mechanical symptoms is wide; the table below highlights the discriminators most often tested.
- Key feature
- Catch-up clunk on ulnar deviation, intact intrinsics
- Carpal alignment
- Reducible VISI
- Discriminating test/finding
- Positive midcarpal shift; clunk reproduced/reduced on dynamic fluoroscopy
- Key feature
- Ulnar focal pain, often post-trauma
- Carpal alignment
- VISI (may be fixed)
- Discriminating test/finding
- LT ballottement/shear positive; LT ligament tear on MRI/arthroscopy (dissociative)
- Key feature
- Dorsal radial pain, weak grip
- Carpal alignment
- DISI
- Discriminating test/finding
- Watson shift positive; SL gap/SL angle over 70 degrees; SL ligament tear
- Key feature
- Ulnar pain on rotation/loading
- Carpal alignment
- Normal
- Discriminating test/finding
- Fovea sign, ulnocarpal stress test; TFCC tear and ulnar-positive variance
- Key feature
- Painful snap with supination/ulnar deviation
- Carpal alignment
- Normal
- Discriminating test/finding
- Snap palpable over ECU groove; tendon subluxes on circumduction
- Key feature
- Pain over pisiform
- Carpal alignment
- Normal
- Discriminating test/finding
- Pisotriquetral grind; tenderness localised to pisiform
The trap is to fixate on the VISI radiograph. VISI is a pattern, not a diagnosis. Both LT dissociation and palmar MCI cause VISI - separate them by whether the intrinsic ligaments are torn (dissociative) and whether the deformity is reducible (MCI is).
Management
Non-Operative Treatment (First-Line)
Conservative care is first-line for all grades and may be definitive in dynamic (Grade I-II) disease. The core is a structured hand-therapy programme: strengthening of the dynamic stabilisers (extensor carpi ulnaris, flexor carpi ulnaris, hypothenar muscles) and proprioceptive / dart-thrower's-motion retraining, progressed with closed-chain work. Splinting/orthoses that block terminal palmar flexion and ulnar deviation (a slight radial-deviation/extension posture) reduce provocation; a custom "ulnar boost" orthosis that supports the pisotriquetral complex has been described specifically for CIND. Activity modification avoids loaded ulnar deviation. NSAIDs give only short-term relief, and corticosteroid injection has no role and may weaken already-attenuated ligaments.
Function-preserving orthosis for non-dissociative MCI
- Describes a custom orthotic design and therapy plan for carpal instability non-dissociative aimed at restoring pain-free, symptom-free movement
- Supports the ulnar/pisotriquetral side to counter the proximal-row collapse driving the clunk
- Positions therapy and orthotic management as the primary, mobility-preserving intervention
Indications and Cautions for Surgery
Surgery is considered when a genuine, supervised conservative trial (typically 3-6 months) fails, symptoms meaningfully limit function or sport, and dynamic imaging confirms reducible instability. Caution / relative contraindications: very severe generalised laxity (e.g. Beighton over 7) predicts recurrence; active workers' compensation or litigation, psychiatric comorbidity and unrealistic expectations all predict poorer outcomes. Counsel candidly - the literature is Level IV and soft-tissue procedures have historically been unreliable.
Surgical Options
- indication
- Reducible Grade II-III palmar MCI after failed rehab
- technique
- Reef/advance dorsal capsule (and ulnar arcuate ligament) to limit proximal-row palmar flexion
- outcomes
- Motion-preserving; results variable and historically inconsistent
- indication
- Focal palmar (or radiocapitate) ligament deficiency
- technique
- Tendon-graft reconstruction of the deficient restraint
- outcomes
- Technically demanding; limited durable data
- indication
- Dynamic (Grade I-II) instability, often with DRC tensioning
- technique
- Radiofrequency shrinkage of redundant capsule, sometimes + open DRC reefing
- outcomes
- Less invasive; early reports favourable but recurrence a concern
- indication
- Grade IV with arthritis, or salvage of failed stabilisation
- technique
- Fuse capitate-hamate-lunate-triquetrum (often with scaphoid excision)
- outcomes
- Reliable pain relief and stability; sacrifices roughly half the motion arc
Soft-Tissue Stabilisation
The shared aim is to limit excessive palmar flexion of the proximal row while preserving motion. Dorsal capsulodesis advances a distally based dorsal capsular flap and reefs the dorsal restraints; described variants tension the dorsal radiocarpal ligament and/or advance the ulnar arm of the arcuate (triquetrohamate-capitate) ligament, the most successful soft-tissue option in Lichtman's original series. Realistic expectations are essential: roughly 10-20 degrees of flexion-extension is traded for stability, and recurrence is well recognised, particularly in markedly lax wrists.
Arthroscopic thermal shrinkage with open DRC tensioning - modern minimally-invasive option
- 9 patients with palmar MCI (mean age 32), mean symptom duration 15.3 months, mean follow-up 16.8 months
- Combined arthroscopic thermal capsular shrinkage with open dorsal radiocarpal (DRC) ligament suture tensioning
- Significant improvement in pain (VAS), grip strength and QuickDASH/modified Mayo scores with maintained radiocarpal stability
- Mild ROM limitation only; all patients returned to previous work and activities
Limited Wrist Arthrodesis (Salvage)
Four-corner fusion (capitate-hamate-lunate-triquetrum, usually with scaphoid excision) is reserved for Grade IV MCI with established midcarpal arthritis or as salvage of failed stabilisation. It gives reliable pain relief and durable stability at the cost of roughly half the flexion-extension arc. Total wrist arthrodesis is a last resort for pan-carpal arthritis or repeated failures, eliminating motion but providing a stable, pain-free wrist.
Complications
After Soft-Tissue Stabilisation
- Recurrent instability - the most frequent problem, more likely with severe generalised laxity or premature return to loaded ulnar deviation; manage by re-confirming the diagnosis, excluding missed pathology, and considering revision reefing, ligament augmentation or salvage fusion.
- Stiffness - some loss of flexion-extension (around 10-20 degrees) is expected and generally well tolerated; excessive stiffness needs directed therapy.
- Persistent pain - suggests inadequate correction, an unrecognised co-existing lesion (TFCC, LT), or progression to arthritis.
- Dorsal ganglion at the capsulodesis site, often asymptomatic.
- Neurovascular injury - dorsal sensory branches of the radial and ulnar nerves are at risk during dorsal exposure; protect them. Wound infection is uncommon.
After Limited Fusion
Non-union, hardware prominence/loosening, dorsal impingement and adjacent (radiolunate) degeneration, in addition to the inherent and substantial loss of motion.
Outcomes and Prognosis
Outcomes are variable and grade-dependent, and the evidence is Level IV throughout. Limited midcarpal fusion is the most reliable operation for pain relief but costs motion; soft-tissue stabilisation preserves motion but historically carries meaningful recurrence (Lichtman: 6 of 9 soft-tissue reconstructions failed; Wright: only 56% good/excellent overall with no surgical advantage). Modern minimally-invasive approaches report encouraging early results in small series but lack long-term and comparative data. Poor-prognosis markers: severe generalised laxity (Beighton over 7), workers' compensation/litigation, bilateral disease, high-demand sport, and unrealistic expectations.
Dart-Thrower's Motion and Proprioceptive Rehabilitation
The conservative programme repeatedly invokes dart-thrower's-motion retraining, but the concept is the biomechanical foundation of motion-preserving care in MCI and deserves explanation.
The dart-thrower's motion (DTM) is the oblique, diagonal wrist arc running from radial deviation with extension to ulnar deviation with flexion - the plane used to throw a dart, swing a hammer or pour from a jug, and the plane of most functional daily tasks. In-vivo kinematic studies show that during DTM the proximal carpal row (scaphoid and lunate) moves remarkably little relative to the radius, with the majority of the excursion occurring at the midcarpal joint through the distal row.
Relevance to MCI: the symptom-generating movement in palmar MCI is loaded pure coronal-plane radial-to-ulnar deviation with the wrist near neutral flexion - exactly the arc that lets the VISI-postured proximal row abruptly "catch up". Because DTM couples ulnar excursion with flexion, functional loading can be retrained through this diagonal plane while avoiding the terminal coronal ulnar-deviation-under-load position that triggers the clunk. DTM drills are combined with co-contraction training of the dynamic stabilisers (extensor carpi ulnaris, flexor carpi ulnaris, hypothenar muscles) to actively control the proximal row, progressing from unloaded proprioceptive work to closed-chain and sport-specific loading. The goal is a stable, pain-free functional arc, not restoration of full coronal deviation.
In the dart-thrower's plane the proximal row behaves as a near-stationary intercalated segment and the excursion is shared smoothly across the midcarpal joint. Retraining the patient to load through this diagonal arc - rather than through provocative coronal ulnar deviation - removes the exact motion that produces the catch-up clunk while preserving useful wrist function.
Guidelines, Registries & Global Practice
There are no dedicated society guidelines for MCI (AAOS, BOA/BSSH, AO, EFORT, ASSH) given its rarity and the absence of high-level evidence - practice is built on expert case series and review (Lichtman; Wright; Hargreaves). The points below summarise the global, society-agnostic consensus and where practice genuinely varies.
- Widely agreed position
- Clinical (midcarpal shift + Beighton) confirmed by dynamic fluoroscopy; imaging mainly excludes other pathology
- Where practice varies
- Availability of dynamic video fluoroscopy and 4D CT (research/tertiary centres only)
- Widely agreed position
- Supervised proprioceptive rehabilitation and activity-blocking orthosis
- Where practice varies
- Access to certified hand therapists; emphasis on dart-thrower's retraining
- Widely agreed position
- Motion-preserving soft-tissue stabilisation (capsulodesis / DRC tensioning / arthroscopic shrinkage)
- Where practice varies
- Use of arthroscopic thermal shrinkage - popular in some units, abandoned in others over durability
- Widely agreed position
- Limited midcarpal (four-corner) fusion as reliable salvage
- Where practice varies
- Fixation method (circular plate vs screws vs K-wires) and scaphoid excision
Global epidemiology: a rare, under-recognised instability with consistent reports of female predominance (around 4:1), young age, and generalised laxity in 60-70%. High- vs limited-resource settings: in well-resourced units, dynamic fluoroscopy, wrist arthroscopy and certified hand therapy are routine, enabling motion-preserving surgery; in limited-resource settings the diagnosis is often missed or made clinically, conservative care predominates, and surgical management - if undertaken - is more likely to be a definitive fusion than a technically demanding soft-tissue reconstruction. No implant registry captures MCI procedures specifically, reflecting the predominance of soft-tissue rather than arthroplasty surgery.
Controversies and Areas of Uncertainty
- What is the primary lesion? Historically attributed to triquetrohamate / ulnar arcuate ligament laxity, but contemporary work implicates dorsal radiocarpal (DRC) ligament insufficiency as a key driver of palmar MCI - which is why DRC tensioning features in modern procedures. The true biomechanical culprit remains debated.
- Which classification? The radiograph-based Lichtman grades coexist with Hargreaves' functional staging; because MCI is a functional instability often with normal static films, no single system is universally accepted.
- Does dynamic instability need surgery at all? A positive midcarpal shift occurs in many asymptomatic hypermobile people, so the threshold for intervention - and the reliability of provocative tests - is contested.
- Soft tissue vs fusion. Soft-tissue stabilisation preserves motion but is historically unreliable; fusion is reliable but sacrifices motion. There are no comparative or randomised trials to adjudicate, and choice is individualised.
- Role of arthroscopic thermal shrinkage. Once popular, then questioned for durability and chondral/capsular safety; newer combined techniques (shrinkage + DRC tensioning) report better early results but need validation.
MCQ Practice Points
Q: What is the pathognomonic clinical finding in midcarpal instability?
A: The catch-up clunk - a painful clunk during ulnar deviation under axial load as the proximal row suddenly shifts from VISI to neutral/extension, reducing the palmarly subluxed capitate. It reproduces the patient's symptoms and is reducible, distinguishing MCI from fixed dissociative VISI.
Q: Why are static radiographs often normal in MCI, and what is the key confirmatory test?
A: Because MCI is a functional, reducible instability - any VISI corrects with radial deviation or grip, and the lesion is ligament attenuation not rupture. The key confirmatory investigation is dynamic video fluoroscopy through radial-to-ulnar deviation under load, capturing the reducible catch-up clunk.
Q: How is MCI distinguished from lunotriquetral dissociation?
A: Both can show a VISI lateral film, but MCI is non-dissociative (intrinsic SL/LT ligaments intact) and reducible, whereas LT dissociation is dissociative (LT interosseous ligament torn, positive LT ballottement/shear) and may be fixed.
Q: Which ligaments are implicated in palmar MCI?
A: Classically the palmar midcarpal ligaments - triquetrohamate-capitate (ulnar arm of the arcuate ligament) and the STT complex. Contemporary evidence also implicates dorsal radiocarpal (DRC) ligament insufficiency, which is why DRC tensioning is incorporated into modern procedures.
Q: What is the strength of the evidence base for MCI treatment?
A: Uniformly Level IV - small retrospective case series only, with no comparative or randomised trials. Limited midcarpal fusion is the most reliable operation for pain; soft-tissue stabilisation preserves motion but is historically less predictable.
At a Glance
Midcarpal instability (MCI) is a non-dissociative carpal instability (CIND) in which the intrinsic interosseous ligaments are intact but abnormal motion occurs between the proximal and distal carpal rows. The hallmark is a painful catch-up clunk during ulnar deviation, caused by the lax palmar midcarpal ligaments failing to control the proximal row, which sits in VISI (volar intercalated segment instability) at rest and then snaps to neutral as the wrist is loaded. Most patients are young women with generalised ligamentous laxity, and a minority have a clear post-traumatic onset. Diagnosis is primarily clinical (Lichtman midcarpal shift test) confirmed by dynamic video fluoroscopy; static radiographs are frequently normal, and arthroscopy/MRI mainly exclude other pathology. The evidence base is uniformly Level IV - there are no comparative or randomised trials. Management begins with proprioceptive rehabilitation and splinting; refractory cases are treated with soft-tissue stabilisation (dorsal capsulodesis, ligament reefing, thermal shrinkage) or, with established arthritis, limited (e.g. four-corner) fusion.
CLUNKMCI Features - CLUNK
Hook:The CLUNK reminds you of the catch-up clunk
Core Exam Knowledge
- Defining feature: painful catch-up clunk on ulnar deviation under load - sudden proximal-row shift from VISI to neutral
- Instability type: non-dissociative (both rows move as units; the lesion is between the rows, not within them)
- Anatomic basis: attenuation of the palmar midcarpal ligaments (triquetrohamate-capitate / ulnar arm of the arcuate ligament; STT complex). The dorsal radiocarpal (DRC) ligament is also implicated as a secondary restraint
- Association: generalised ligamentous laxity (positive Beighton score) in 60-70%
- Diagnosis: clinical (midcarpal shift test) confirmed by dynamic video fluoroscopy; static films often normal
- Treatment principle: limit excessive palmar flexion of the proximal row - rehabilitation first, then soft-tissue stabilisation; partial fusion is reliable but sacrifices motion
MCI vs lunotriquetral dissociation. Both can show a VISI lateral radiograph, but MCI is non-dissociative and reducible (intrinsic ligaments intact, VISI corrects with radial deviation/grip) whereas LT dissociation is dissociative and may be fixed (LT interosseous ligament torn). Demonstrating reducibility on dynamic fluoroscopy is the key.
Imaging Atlas
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old female gymnast presents with painful clunking in her right wrist that has progressively worsened over a year. The clunk occurs with certain movements and is painful. Examination shows a positive midcarpal shift test. How would you assess and manage her?”
“The same gymnast returns after 6 months of hand therapy and activity modification. She has improved somewhat but still clunks and has pain with gymnastics, which she wants to continue. Grip is 60% of the other side. She asks about surgery. How do you counsel her?”
“A 45-year-old manual worker has chronic ulnar wrist pain and clunking 5 years after a fall. Radiographs show a VISI pattern with midcarpal joint space narrowing and osteophytes. Conservative measures have failed. What is your approach?”
Definition and Pathognomonic Features
- Non-dissociative carpal instability (CIND): intrinsic SL/LT ligaments INTACT; abnormal motion BETWEEN the carpal rows
- Hallmark: painful, reducible catch-up clunk on ulnar deviation under load
- Anatomic basis: palmar midcarpal (triquetrohamate/arcuate, STT) and dorsal radiocarpal ligament insufficiency
- Generalised ligamentous laxity in 60-70%; female predominance ~4:1, young patients
Clinical Diagnosis - Key Test
- Midcarpal shift test (Lichtman): palmar-directed force on dorsal capitate + axial load + ulnar deviation reproduces the clunk
- Adjuncts: supination lift test, dorsal-palmar shear test
- Always assess Beighton score and compare with the asymptomatic side
- A positive shift without symptoms is NOT pathology
Classification
- Lichtman Grade I (dynamic) - VISI only with provocation
- Grade II (static reducible) - VISI at rest, corrects with radial deviation
- Grade III (static irreducible) - persistent VISI
- Grade IV (arthritic) - midcarpal arthritis
- Subtypes: palmar (80-90%, VISI) vs dorsal/capitolunate (rare); Hargreaves functional staging is an alternative
Investigation
- Radiographs often normal; lateral may show reducible VISI (capitolunate over 15 degrees palmar, scapholunate under 30 degrees)
- KEY: dynamic video fluoroscopy capturing the reducible catch-up clunk
- MRI/arthroscopy mainly to EXCLUDE TFCC, LT and SL pathology; 4D CT is an emerging adjunct
Management
- First-line: proprioceptive/dynamic-stabiliser rehabilitation + activity-blocking orthosis, 3-6 months
- Reducible refractory disease: dorsal capsulodesis / arcuate advancement / arthroscopic shrinkage with DRC tensioning (expect ~10-20 degrees motion loss)
- Grade IV arthritis or failed stabilisation: limited (four-corner) fusion; total wrist fusion as last resort
- Evidence is Level IV only - no comparative or randomised trials
Complications and Prognosis
- Recurrent instability is the leading problem after soft-tissue surgery (worse with severe laxity/high demand)
- Expected stiffness ~10-20 degrees; persistent pain suggests missed pathology or arthritis
- Dorsal sensory nerve branches at risk on dorsal exposure
- Fusion: reliable pain relief but ~50% motion loss; risks non-union and adjacent degeneration
- Poor prognosis: Beighton over 7, workers' comp/litigation, bilateral disease, elite sport
Viva Talking Points
- Emphasise NON-dissociative, REDUCIBLE instability between intact rows
- Diagnosis is clinical + dynamic fluoroscopy; static films often normal
- Distinguish from LT dissociation (dissociative, may be fixed)
- Rehab first; motion-preserving soft tissue for reducible disease; fusion for arthritis/salvage
- Be honest that the evidence is Level IV
The Role of Wrist Arthroscopy and Modern Evidence
Contemporary review - role of arthroscopy and grade-matched treatment
- Evidence for MCI management rests solely on case series; established (fusion) treatments cost significant motion
- Treatment should be matched to type and grade using the Hargreaves grading system for palmar MCI
- Arthroscopic thermal capsular shrinkage is appropriate for dynamic instabilities
- Static deformities require soft-tissue reconstruction or partial wrist fusion
Authoritative overview and proposed functional staging
- Palmar MCI is the commonest type and the typical cause of a clunking, painful wrist
- Diagnosis is made on clinical grounds with provocative tests; imaging and arthroscopy mainly EXCLUDE other pathology
- Proposes a functional staging scheme (extent of palmar translation of the distal row) better suited to a functional instability
- Explicitly notes there are NO comparative series or randomised studies given the rarity of the condition