Milch Classification of Lateral Condyle Fractures
Do not use Milch as a treatment threshold by itself. The exam distinction is anatomical: Milch I is lateral to the trochlear groove and stable; Milch II enters the groove/trochlea and is unstable. Treatment then follows displacement: less than 2 mm in all views can be immobilised with strict early follow-up; greater than 2 mm, articular incongruity, or rotation requires operative fixation.
The Milch Classification
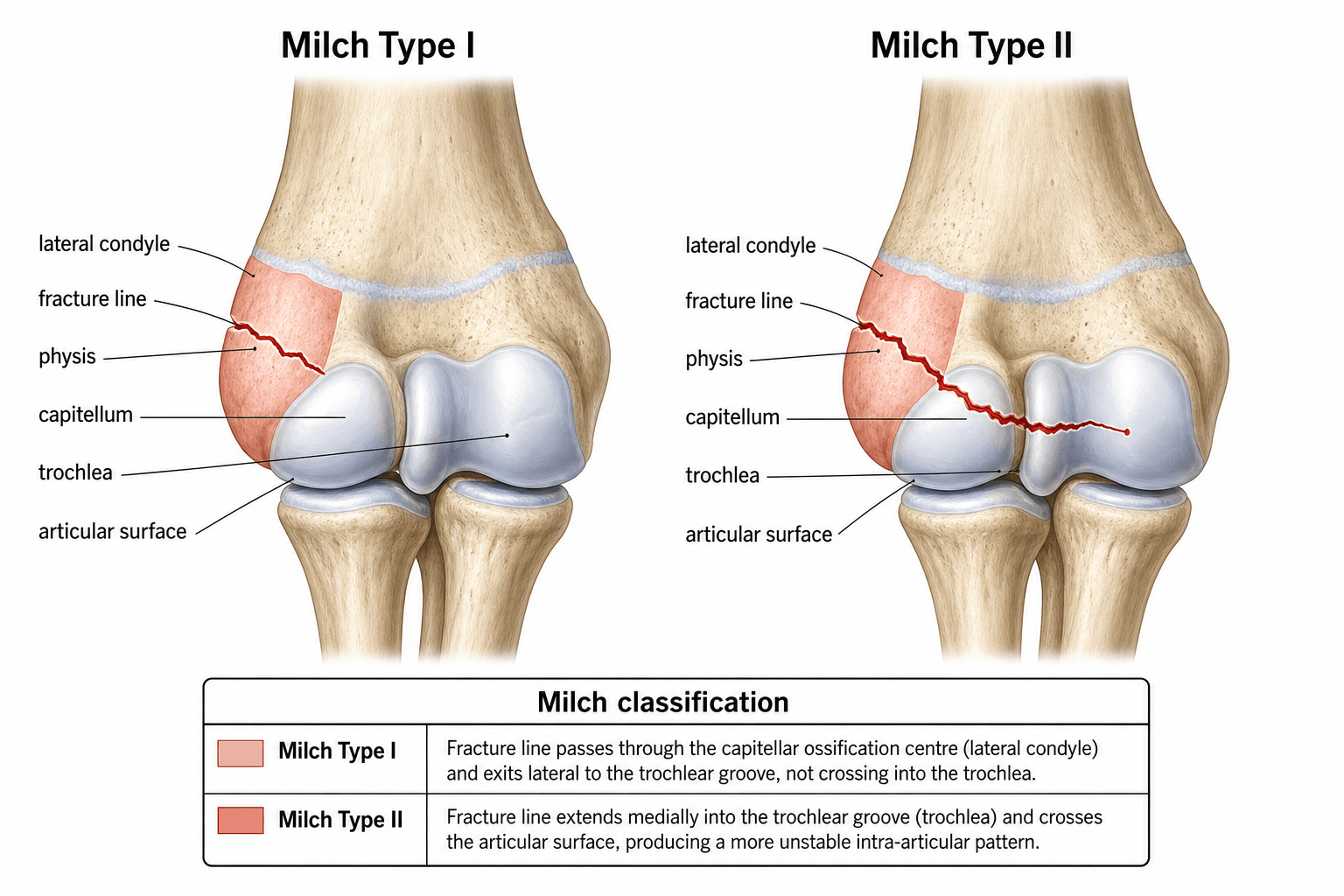

Milch is a map of the fracture line through the distal humeral epiphysis. It is most useful when the examiner asks whether the elbow remains stable and whether the trochlear ridge has been violated.
- Fracture Line
- Lateral to the trochlear groove; through the capitellum-lateral condyle mass
- Physeal Pattern
- Classically Salter-Harris IV because the fracture crosses metaphysis, physis and epiphysis
- Elbow Stability
- Usually stable because the medial trochlear ridge is preserved
- Fracture Line
- Through the trochlear groove and into the trochlea
- Physeal Pattern
- Salter-Harris II pattern in the Milch teaching scheme
- Elbow Stability
- Unstable; the elbow may sublux or dislocate because the lateral crista of the trochlea is disrupted
I = Outside the groove • II = Into the grooveThe two Milch lines
Hook:One stays Outside the groove (I); twO goes intO the groove (II) — and losing the groove loses elbow stability.
I is Intact • II is InstabilityStability
Hook:I = Intact ridge, stable; II = Instability — the trochlear buttress is breached.
Milch maps • Jakob measures • displacement decidesTreatment logic
Hook:Milch maps, Jakob measures, displacement decides — never cast vs fix on Milch alone.
The visible ossified fragment underestimates the real fracture in younger children because much of the lateral condyle and trochlea is cartilage. If the joint surface or hinge is uncertain on plain radiographs, use an internal oblique view and consider arthrogram, MRI, or intra-operative assessment.
Score Interpretation and Action
Jakob staging is the practical companion to Milch because it grades displacement and rotation.
- Radiographic Pattern
- Undisplaced or less than 2 mm displacement on all views
- Articular Hinge
- Cartilaginous hinge intact
- Recommended Action
- Above-elbow cast, elbow at about 90 degrees, weekly radiographs for the first 2 to 3 weeks
- Radiographic Pattern
- Moderate displacement, typically greater than 2 mm, without rotation
- Articular Hinge
- May be intact but is unreliable on plain radiographs
- Recommended Action
- Reduction and fixation if displacement is greater than 2 mm; closed or mini-open technique may be considered if the articular surface is reducible
- Radiographic Pattern
- Completely displaced or rotated fragment
- Articular Hinge
- Hinge disrupted
- Recommended Action
- Open reduction and internal fixation with K-wires or a screw, preserving posterior soft tissues
- Treatment
- Long-arm cast and close surveillance
- Key Technical Point
- Radiograph at 5 to 7 days and then weekly early; convert to fixation if it displaces
- Follow-up Risk
- Late displacement, non-union
- Treatment
- Fixation after confirming/reducing the articular surface
- Key Technical Point
- Two divergent lateral K-wires are common; cannulated screw can be used in larger children when compression is desired
- Follow-up Risk
- Loss of reduction, stiffness, lateral overgrowth
- Treatment
- Open reduction and internal fixation
- Key Technical Point
- Anterolateral approach; do not strip posterior attachments because they carry fragment blood supply
- Follow-up Risk
- Avascular necrosis, fishtail deformity, cubitus valgus

A displaced lateral condyle fracture is an intra-articular injury bathed in synovial fluid and pulled by the common extensor origin. Treating a displaced fracture in plaster risks non-union, progressive cubitus valgus, and late tardy ulnar nerve palsy.
The topic's complications are named — here is what examiners want you to DO about them:
- Established non-union with a viable, minimally-displaced fragment: the principle is in-situ fixation (a compression screw) plus bone grafting WITHOUT mobilising/dissecting the fragment — disturbing the posterior soft-tissue attachments to reduce the non-union risks osteonecrosis of the already-tenuous fragment. Accept a small malposition rather than devascularise it.
- Why fix a non-union at all: to halt the progressive cubitus valgus that follows (the un-tethered lateral physis keeps growing / the elbow drifts into valgus) and the resulting traction tardy (delayed) ulnar neuropathy.
- Established cubitus valgus + tardy ulnar nerve palsy: treat the nerve with anterior ulnar nerve transposition (decompress/relocate it out of the stretched cubital tunnel), and correct the deformity with a distal humeral (supracondylar) corrective osteotomy when the valgus/function warrants it.
- The whole cascade — displaced fracture cast in plaster → non-union → cubitus valgus → tardy ulnar palsy — is the classic "why you must not cast a displaced lateral condyle fracture" story.
Limitations and Modern Context
- Milch has limited reliability on plain radiographs. The key line often passes through unossified cartilage, so the apparent bony fracture may not show whether the trochlear groove or cartilaginous hinge is intact.
- Milch does not grade displacement. A Milch I fracture displaced greater than 2 mm still requires fixation, while a truly undisplaced Milch II pattern may initially be observed only if the joint is congruent and follow-up is reliable.
- Jakob and modern displacement-based systems are more treatment-facing. Stage I injuries are casted, Stage II injuries sit at the reduction/fixation threshold, and Stage III injuries require open reduction.
- Internal oblique radiographs are essential. Lateral condyle displacement is commonly underestimated on standard AP and lateral views; the internal oblique view profiles the fracture gap and lateral column.
- Operative technique must protect blood supply. The lateral condyle fragment receives important posterior soft-tissue blood supply; aggressive posterior dissection increases the risk of osteonecrosis and fishtail deformity.
- Complications define the long game. Non-union, lateral condylar overgrowth, cubitus valgus, tardy ulnar nerve palsy, fishtail deformity, stiffness, and osteonecrosis must be actively looked for during follow-up.
Because Milch is anatomical and Jakob is dated, two modern displacement/articular-hinge systems now drive treatment and are increasingly the answer examiners want:
- Weiss classification (the practical, treatment-linked one): Type I — under 2 mm displacement → cast/immobilise; Type II — 2 mm or more with an INTACT articular cartilage hinge → closed reduction and percutaneous pinning (CRPP); Type III — 2 mm or more with a DISRUPTED articular surface → open reduction and internal fixation. Weiss also showed the complication rate rises with grade (notably higher in Type III).
- Song classification: a five-stage scheme grading the progression of the fracture gap on the internal oblique radiograph (from a small lateral-gap stage 1 through to a completely displaced, rotated stage 5) — useful for deciding which "minimally displaced" fractures are safe to observe versus pin.
The unifying message is unchanged from Milch/Jakob — the integrity of the articular (cartilage) hinge and the amount of displacement, assessed on the internal oblique view, decide cast vs CRPP vs ORIF — but Weiss/Song state it in directly operative terms.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 6-year-old falls from playground equipment and has lateral elbow swelling. Radiographs show a lateral condyle fracture with the line entering the trochlear groove and 3 mm displacement on the internal oblique view. How do you classify and manage it?”
“A 5-year-old has an apparently undisplaced lateral condyle fracture after a fall. The AP view shows less than 2 mm displacement, but the lateral view is difficult to interpret. What is your investigation and treatment plan?”
Milch anatomy
- Milch I: fracture line lateral to the trochlear groove; medial trochlear ridge preserved; elbow usually stable
- Milch II: fracture line through the trochlear groove into the trochlea; unstable; elbow may sublux or dislocate
- Milch is anatomical, not a stand-alone treatment algorithm
Jakob displacement
- Stage I: undisplaced or less than 2 mm; cast with close radiographs
- Stage II: greater than 2 mm displacement without rotation; reduce and fix if displacement is confirmed
- Stage III: rotated or completely displaced; open reduction and fixation
Treatment thresholds
- Less than 2 mm on AP, lateral and internal oblique views: above-elbow cast and early repeat imaging
- Greater than 2 mm, rotation, incongruity or Milch II instability: ORIF or selected closed reduction with K-wires/screw
- Protect posterior soft-tissue attachments during surgery to reduce osteonecrosis risk
Complications to name
- Non-union with progressive cubitus valgus and tardy ulnar nerve palsy
- Lateral condyle overgrowth, stiffness and loss of motion
- Avascular necrosis and fishtail deformity after excessive dissection or vascular compromise
Evidence Base
Both citations were verified against PubMed. The lateral condyle fracture has no high-level (RCT) evidence base — management rests on review articles and case series. Alvarez Munoz (2024 review) gives the consensus framework: AP/lateral/internal-oblique films are the diagnostic gold standard, the classifications (Milch, Jakob) vary in reproducibility, minimally displaced fractures are immobilised and displaced ones fixed (K-wires or cannulated screw), and the practical message is a growing interest in expanding closed-reduction indications. Li (2026) is an example of that trend — a small Level IV series of single-portal arthroscopic-assisted reduction with excellent Flynn outcomes. The durable exam points (Milch anatomy/stability, the 2 mm displacement threshold, the internal-oblique view, protecting posterior blood supply) are more important than either paper.
Management of Acute Lateral Humeral Condyle Fractures in Children
- Lateral condyle fractures are up to 22 percent of paediatric elbow fractures; AP, lateral and internal-oblique films are the diagnostic standard
- Several classification systems (Milch, Jakob displacement stages) guide management, varying in reproducibility
- Minimally displaced fractures are immobilised; displaced fractures need closed or open reduction with K-wires or cannulated screws
A novel single-portal arthroscopic technique for the management of pediatric humeral lateral condylar fractures
- 18 displaced paediatric lateral condyle fractures treated with arthroscopic-assisted closed reduction via a single portal
- 16 excellent and 2 good outcomes by Flynn criteria; no nonunion, neurovascular injury, or compartment syndrome
- Offers a minimally invasive alternative for displaced fractures not amenable to conventional closed reduction