Ulna Fracture with Radial Head Dislocation
- Line through radial head must bisect capitellum on ALL views
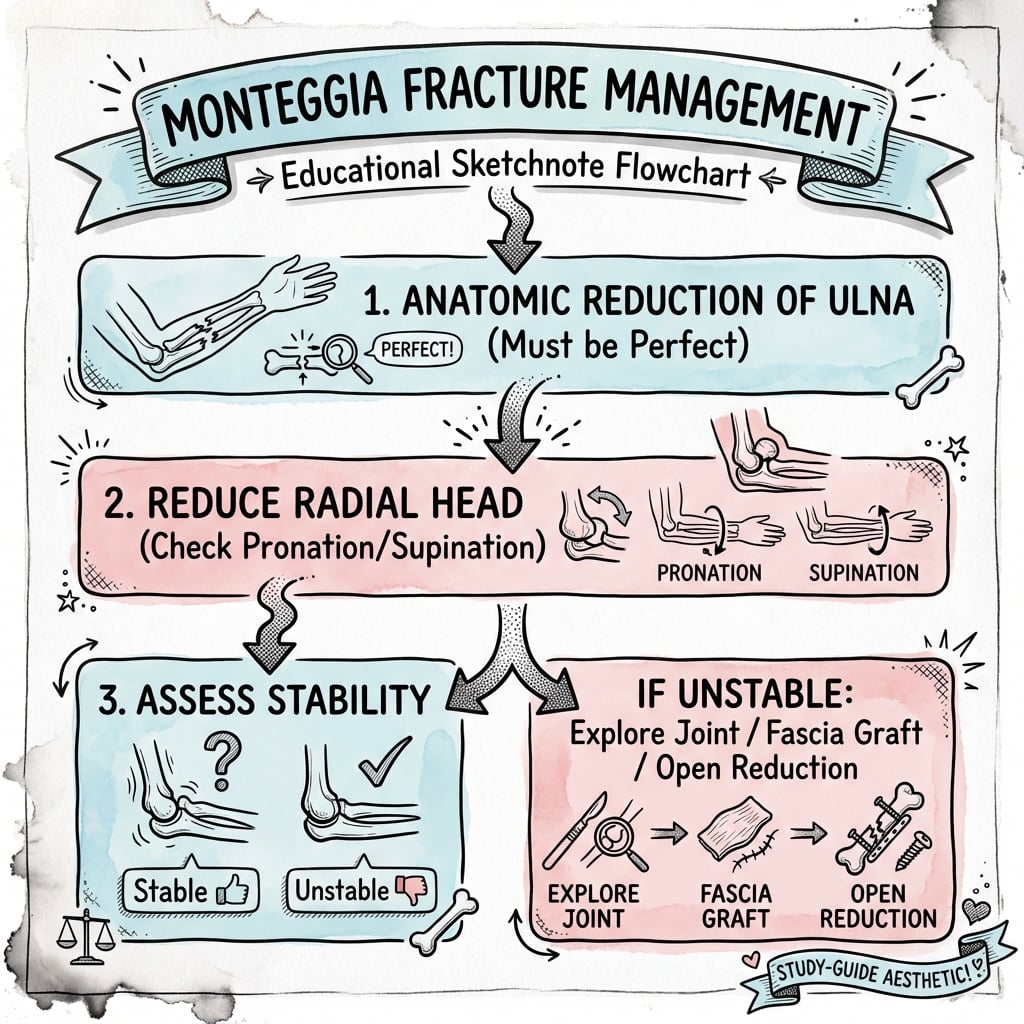
- Fix the ulna - radial head reduces spontaneously
- Adult Type II most common - posterior angulation
- Chronic - requires open reduction and annular ligament reconstruction
- “Always get elbow X-ray with forearm fracture
- “Radiocapitellar line - most missed injury in orthopaedics
- “Type II most common in adults, Type I in children
- “Ulna length and alignment critical - use contralateral comparison
Monteggia is one of the most commonly missed forearm injuries. ALWAYS check the radiocapitellar line on every forearm X-ray.
Type II (posterior) is most common in adults. Type I (anterior) is most common in children. Treatment principles differ significantly between these groups.
Fix the ulna anatomically - the radial head typically reduces spontaneously in acute injuries. If it doesn't reduce, suspect interposed tissue (annular ligament).
If more than 4 weeks: annular ligament reconstruction (Bell Tawse) is required. Results deteriorate significantly with delay—early diagnosis is critical.
- Key Feature
- Anterior ulna angulation
- Radial Head Status
- Anterior RH dislocation
- Treatment
- Anatomic ulna ORIF - RH reduces
- Key Feature
- Posterior ulna angulation - most common adult
- Radial Head Status
- Posterior RH dislocation
- Treatment
- Plate fixation ulna - check RH reduction
- Key Feature
- Ulna metaphyseal fracture
- Radial Head Status
- Lateral RH dislocation
- Treatment
- Ulna fixation - may need RH ORIF
- Key Feature
- Both bone fractures
- Radial Head Status
- Anterior RH dislocation
- Treatment
- Fix both radius and ulna
- Key Feature
- Missed or delayed presentation
- Radial Head Status
- RH remains dislocated
- Treatment
- Open reduction + annular ligament reconstruction
- Key Feature
- Plastic deformation possible
- Radial Head Status
- Check radiocapitellar line
- Treatment
- Closed reduction if acute, open if chronic
Overview/Epidemiology
Demographics and Distribution
- Bimodal pattern: peaks in childhood (4-10 years) and middle age (40-60 years)
- Pediatric cases: predominantly Type I (anterior)
- Adult cases: predominantly Type II (posterior)
- Elderly patients: often have more comminuted patterns
- Children: Falls from height, playground injuries
- Adults: High-energy trauma, sports injuries, direct blows
- Elderly: Low-energy falls with osteoporotic bone
The bimodal age distribution reflects different mechanisms: children fall with hyperextended arm (Type I), while adults sustain direct blows or axial loading (Type II).

Anatomy/Biomechanics
Relevant Anatomy
- Radial head articulates with radial notch of ulna
- Annular ligament encircles radial head (4/5 of circumference)
- Quadrate ligament provides secondary restraint
- Interosseous membrane connects radius and ulna throughout forearm
- Strong fibrous band attached to anterior and posterior margins of radial notch
- Forms 4/5 of fibro-osseous ring around radial head
- Lined with cartilage on inner surface
- Prevents radial head migration during rotation
- Fibers run obliquely from radius to ulna (proximal-lateral to distal-medial)
- Central band is the thickest and strongest portion
- Transmits forces from radius to ulna
- Disruption leads to proximal migration of radius
The interosseous membrane is often disrupted in Monteggia injuries. This affects load transfer and forearm stability. Assess for tenderness along the entire interosseous space.
Biomechanical Principles
Why Does the Radial Head Dislocate?
The ulna and radius are linked as a functional unit:
- Ulna is the fixed bone (stable at elbow via olecranon)
- Radius rotates around ulna for pronation/supination
- When ulna angulates, radial head must dislocate to accommodate
Key Concept: Radiocapitellar Line
The radiocapitellar line is a line drawn through the center of the radial shaft and head. On any view:
- This line MUST pass through the center of the capitellum
- If it doesn't, the radial head is subluxated or dislocated
- Check on AP, lateral, AND oblique views
Classification Systems
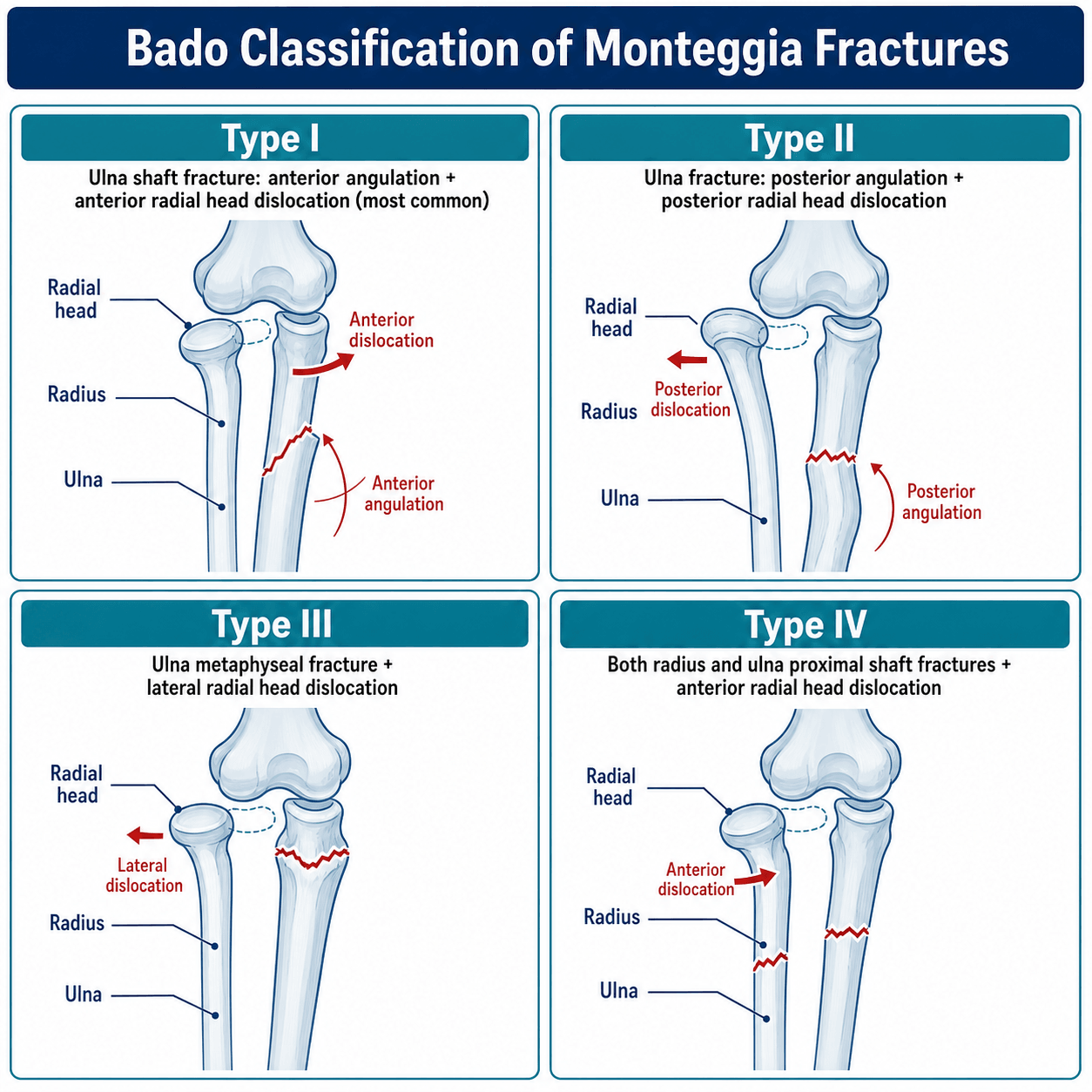
Bado Classification
- RH Dislocation
- Anterior
- Ulna Pattern
- Anterior apex angulation
- Mechanism
- Fall on hyperextended arm
- Frequency Adult
- 15%
- RH Dislocation
- Posterior/Posterolateral
- Ulna Pattern
- Posterior apex angulation
- Mechanism
- Direct blow to flexed elbow
- Frequency Adult
- 70%
- RH Dislocation
- Lateral
- Ulna Pattern
- Metaphyseal fracture (valgus)
- Mechanism
- Varus force on extended arm
- Frequency Adult
- 10%
- RH Dislocation
- Anterior
- Ulna Pattern
- Both bone fractures (same level)
- Mechanism
- Hyperpronation injury
- Frequency Adult
- 5%
Jupiter Type II Subclassification
- Pattern
- Ulna fracture at coronoid level
- Implications
- Most common subtype
- Pattern
- Fracture distal to coronoid
- Implications
- Standard plating approach
- Pattern
- Fracture at diaphysis
- Implications
- May need longer plate
- Pattern
- Fracture at ulna diaphysis + radius fracture
- Implications
- Both bone fixation required
Jupiter classification helps predict difficulty - proximal fractures near coronoid (IIA) may require different approach and have higher complication rates.
Pathomechanics
Forced hyperpronation with hyperextension
- Fall on outstretched hand
- Forearm in pronation
- Biceps pulls radial head anteriorly
- Most common in children (greenstick pattern)
Proper technique and attention to detail ensure optimal outcomes.
Clinical Assessment
Key Examination Points
Check finger extension (EDC, EIP) specifically. PIN palsy occurs in 10-20% of Monteggia injuries. Wrist extension preserved (ECRL/ECRB) as these are innervated proximal to PIN.
Investigations
Essential Imaging
Standard Views:
- AP and lateral forearm - MUST include elbow and wrist joints
- AP and lateral elbow - confirm radial head relationship
- Contralateral comparison if ulna length questionable
The radiocapitellar line must bisect the capitellum on EVERY view (AP, lateral, oblique). Any deviation indicates radial head subluxation/dislocation.



- Coronoid fracture assessment
- Complex proximal ulna fractures
- Chronic Monteggia - assess radial head shape changes
- Suspected interosseous membrane disruption (Essex-Lopresti variant)
- Chronic injuries - assess cartilage integrity
- Soft tissue interposition planning
Differential Diagnosis
- Ulna
- Proximal/shaft fracture or plastic bowing
- Radial Head / PRUJ
- Dislocated (radiocapitellar line disrupted)
- Discriminating Feature
- Ulna fracture WITH radial head dislocation - check the line on every view
- Ulna
- Mid-shaft fracture, often transverse
- Radial Head / PRUJ
- Located normally (line intact)
- Discriminating Feature
- No radial head dislocation - the classic Monteggia trap if the line is not checked
- Ulna
- Normal, no fracture
- Radial Head / PRUJ
- Chronically dislocated; convex/dome-shaped radial head, hypoplastic capitellum
- Discriminating Feature
- Bilateral, no trauma, dysmorphic radial head - do NOT mistake for acute injury
- Ulna
- Fracture
- Radial Head / PRUJ
- Radius fractured but radial head located
- Discriminating Feature
- Both bones broken without PRUJ dislocation (vs Bado IV which adds RH dislocation)
- Ulna
- Intact
- Radial Head / PRUJ
- Radial HEAD fracture + IOM + DRUJ disruption
- Discriminating Feature
- Longitudinal forearm instability and DRUJ disruption, not proximal RU dislocation
- Ulna
- Olecranon fracture
- Radial Head / PRUJ
- PRUJ intact; ulnohumeral subluxation
- Discriminating Feature
- Forearm translates with the proximal ulna; radiocapitellar relationship preserved
A pulled or angulated ulna shaft fracture is a Monteggia until proven otherwise. The single discriminator is the radiocapitellar line - a normal-looking "isolated ulna fracture" with a disrupted line IS a Monteggia.
Proximal Ulna Dorsal Angulation (PUDA) and the Straight-Plate Pitfall
The topic's central mantra is "fix the ulna anatomically and the radial head follows", and it shows (Ring 2004) that malalignment after a posterior Monteggia is usually due to inadequate fixation - but it never explains the specific geometric trap that causes this: the proximal ulna is not straight.
- The proximal ulna dorsal angulation (PUDA). The proximal ulna carries a normal dorsally-directed (apex-posterior) angulation of roughly 6 degrees, located about 5-6 cm distal to the tip of the olecranon, together with a variable proximal radioulnar convergence in the coronal plane. It is a genuine anatomical bow, not a straight tube.
- The straight-plate pitfall. Applying a straight or generically pre-contoured plate to the dorsal proximal ulna flattens this normal PUDA, subtly shortening and malaligning the proximal ulna - which then levers the radial head into subluxation or redislocation even when the shaft looks "reduced". This is the mechanism behind the malaligned posterior Monteggia fractures that Ring salvaged with a dorsal contoured plate.
- Avoiding it. Template the PUDA against the contralateral uninjured ulna, contour the plate (or use a dedicated pre-contoured proximal-ulna plate) to the patient's own geometry, and confirm a concentric radiocapitellar line on fluoroscopy before leaving theatre. "Anatomic" means restoring the ulna's length AND its native sagittal bow - not making it straight.
Q: Why can a posterior Monteggia redislocate even after the ulna shaft is "reduced" and plated? A: The proximal ulna has a normal dorsal angulation (PUDA, about 6 degrees) ~5-6 cm distal to the olecranon tip. A straight plate flattens it, shortening/malaligning the proximal ulna and levering the radial head out - the mechanism Ring salvaged with a dorsal contoured plate. Template the contralateral ulna, contour the plate to the native PUDA, and confirm a concentric radiocapitellar line. Restore the ulna's length AND its bow.
Management Algorithm
- Anterior (Type I) or posterior (Type II) radial head dislocation
- Presentation within 4 weeks of injury
- Most common scenario in both children and adults
- Closed reduction attempt - may provide temporary stability
- Anatomic ulna ORIF - restore length and alignment
- Intraoperative fluoroscopy - confirm radiocapitellar line
- Radial head reduces spontaneously in 95% of cases
- Fix the ulna first - radial head follows
- Must restore ulna length - compare to contralateral
- 3.5mm LCP plate, 6-8 holes minimum
- If RH doesn't reduce - explore for interposed tissue
Anatomic ulna fixation is the key - radial head reduces spontaneously in acute injuries. If it doesn't, suspect interposed tissue (annular ligament, capsule, or biceps).



Complications and Management
Common Complications
- Incidence
- 10-20%
- Prevention/Management
- Usually neurapraxia - observe 3 months. Explore if no recovery.
- Incidence
- 5-10%
- Prevention/Management
- Anatomic ulna reduction, check intraoperative fluoro
- Incidence
- 2-5%
- Prevention/Management
- Single incision, careful soft tissue handling
- Incidence
- 10-15%
- Prevention/Management
- Early ROM, static progressive splinting
- Incidence
- Under 5%
- Prevention/Management
- Compression plating, bone graft if needed
- Incidence
- 5%
- Prevention/Management
- Gentle surgery, consider prophylaxis if prior HO
Nerve Injury
Associated Injuries
What is Essex-Lopresti?
- Radial head fracture + interosseous membrane disruption + DRUJ injury
- Rare but devastating combination
- Can occur with Type IV Monteggia (both bone fractures)
- Tenderness along entire interosseous space
- DRUJ instability on examination
- Positive ulnar variance on X-ray
- Cannot excise radial head (leads to proximal migration)
- Must address DRUJ stability
- Consider radial head replacement if unfixable
If you encounter a Monteggia variant with both bone fractures (Type IV), specifically examine the DRUJ and entire interosseous membrane. Missing this leads to proximal radial migration and chronic wrist pain.
Surgical Technique
Acute Management Principles
Surgical Technique
Approach: Direct posterior (Boyd approach)
- Position: Supine, arm across chest or table
- Posterior incision along subcutaneous border
- Fracture reduction - restore length and alignment
- Plate fixation - 3.5mm LCP, 6-8 holes
- Check radiocapitellar relationship under fluoro
- If RH doesn't reduce - explore for interposition
- Must restore ulna length - compare to contralateral
- Slight bow of ulna important for rotation
- Position plate on tension side (posterior/lateral)
Proper technique and attention to detail ensure optimal outcomes.
Pediatric Considerations
- Adult
- Type II (posterior)
- Pediatric
- Type I (anterior)
- Adult
- Complete fracture
- Pediatric
- Often greenstick/plastic
- Adult
- Operative fixation standard
- Pediatric
- Closed reduction may succeed
- Adult
- Often ruptured
- Pediatric
- Often intact
- Adult
- Poor outcomes
- Pediatric
- Better remodeling potential
Pediatric Monteggia: If ulna greenstick is corrected and radial head reduces concentrically, closed treatment with long arm cast in supination (Type I) may succeed. Follow closely for re-displacement.
Chronic Monteggia
Chronic Monteggia (more than 4 weeks) has significantly worse outcomes. Early diagnosis and treatment essential. Results deteriorate rapidly with delay.

Missed injury more than 4 weeks from injury
- Radial head deformity and overgrowth
- Annular ligament scarring/absence
- Capitellum changes
- Limited remodeling in adults
- Ulna osteotomy - restore length and correct angular deformity
- Open reduction of radial head
- Annular ligament reconstruction (Bell Tawse technique)
- Radial head excision (adults, after skeletal maturity)
Bell Tawse Reconstruction Technique
- Chronic Monteggia with absent/deficient annular ligament
- Most commonly used in pediatric patients
- After successful open reduction of radial head
- Position supine, arm on table
- Posterior approach - harvest 1cm strip of triceps fascia (10-12cm long)
- Kocher approach to radial head
- Reduce radial head - excise any fibrous tissue blocking reduction
- Drill hole through proximal ulna (anterior to posterior)
- Pass triceps strip through hole
- Wrap around radial neck and suture to itself
- Temporary transarticular K-wire for 3-4 weeks
- Good results in 70-80% of pediatric cases
- Results decline with increasing delay from injury
- Adult outcomes less predictable
- May require additional procedures for stiffness
The Bell Tawse technique uses triceps fascia to create a neo-annular ligament. Originally described in 1965, it remains the gold standard for chronic pediatric Monteggia reconstruction.
Radial Head Excision
- Chronic Monteggia in adults with irreducible radial head
- Significant radial head deformity
- Failed reconstruction
- Only after skeletal maturity (contraindicated in children)
- Loss of radiocapitellar articulation
- Potential valgus instability
- Proximal radial migration (if DRUJ unstable)
- Cubitus valgus deformity
- Intact DRUJ
- Intact MCL complex
- No associated Essex-Lopresti injury
Never excise the radial head in a skeletally immature patient. This leads to progressive valgus deformity and proximal migration. Always attempt reconstruction first.
Postoperative Care and Rehabilitation
Post-operative Protocol
- Early motion if stable fixation achieved
- Avoid forced supination in first 4 weeks (protects annular ligament)
- Protect against varus stress if LCL repaired
- Address elbow stiffness aggressively with static progressive splinting
- Focus on forearm rotation as well as elbow flexion/extension
- Desk work: 2-4 weeks
- Manual labor: 3-6 months
- Contact sports: 6 months minimum
- Full unrestricted: When strength and ROM normalized
Managing Stiffness
Outcomes and Prognosis
Expected Outcomes by Type
- Expected ROM
- 80-90% of contralateral ROM
- Union Rate
- 95-98%
- Functional Outcome
- Good to excellent in 85-90%
- Expected ROM
- 70-85% of contralateral ROM
- Union Rate
- 90-95%
- Functional Outcome
- Good to excellent in 70-80%
- Expected ROM
- 60-70% of contralateral ROM
- Union Rate
- N/A (osteotomy)
- Functional Outcome
- Fair to good in 50-60%
- Expected ROM
- Near-normal ROM
- Union Rate
- 98-100%
- Functional Outcome
- Excellent in 90-95%
- Expected ROM
- 70-80% of contralateral ROM
- Union Rate
- N/A
- Functional Outcome
- Good to excellent in 70-80%
Prognostic Factors
The most important prognostic factor is timing of diagnosis and treatment. Acute injuries (under 4 weeks) have excellent outcomes (85-90% good to excellent). Chronic injuries have only 50-60% good outcomes even with reconstruction.
Long-term Outcomes
Key durable endpoints (acute anatomic fixation): ulna union 95-98%, radial head stability 90-95% (re-dislocation 5-10%, higher with non-anatomic reduction), grip and forearm rotation 80-90% of the contralateral side at 1 year. Mild residual stiffness (10-15 degrees) is common but rarely functionally limiting; HO requiring excision and persistent PIN weakness each occur in under 5%.
Counsel patients that while union and stability are reliably achieved, 10-15 degrees of motion loss is common and some loss of grip strength may persist. Most return to full activities by 6 months.
Adult Type II: Outcome is Driven by the Associated Radial Head and Coronoid Injuries
The topic lists associated radial head and coronoid fractures but never crystallises the single most important adult-exam principle from its own evidence (Ring 1998; Xiao 2021): the adult posterior (Bado II) Monteggia is really a proximal-ulna fracture-dislocation, and its outcome is driven by those associated injuries, not the ulnar shaft alone.
- How often, and why it matters. In Ring's adult series, about two-thirds of Bado type II fractures had an associated radial head fracture and many also had a coronoid fracture; the majority of the poor results were type II lesions with these associated injuries. The ulnar shaft heals reliably - it is the radial head and coronoid that determine elbow stability and function.
- Posterior Monteggia is an elbow fracture-dislocation. Bado II sits on a spectrum with the posterior olecranon fracture-dislocation: the injury is centred on the proximal ulna and the ulnohumeral/radiocapitellar articulations, so the coronoid (the anterior buttress against posterior instability) and the radial head (the lateral buttress) must both be restored, not just the ulnar shaft.
- Practical sequence. Plan explicitly for the associated injuries at the index operation: fix or replace the radial head and address the coronoid (its classification and fixation are covered in the coronoid-fractures topic), because coronoid access from the standard posterior approach is difficult and a tenuous coronoid reduction predicts a poor result (Xiao 2021). Under-treating these is why adult type II outcomes lag behind type I and paediatric injuries.
Q: Why are adult Bado type II Monteggia outcomes worse than type I? A: Adult type II is a proximal-ulna fracture-dislocation - in Ring's series ~two-thirds had an associated radial head fracture and many a coronoid fracture, and these (not the ulnar shaft, which heals reliably) drove the poor results. Treat type II as an elbow fracture-dislocation: restore the coronoid (anterior buttress) and radial head (lateral buttress) at the index operation. Coronoid access from the posterior approach is difficult and a tenuous coronoid reduction predicts a poor outcome (Xiao 2021).
Guidelines, Registries & Global Practice
Global Epidemiology
- Monteggia lesions are uncommon: roughly 1-2% of all forearm fractures and under 5% of paediatric elbow/forearm fractures across published series worldwide.
- Bimodal distribution: paediatric peak around 4-10 years (predominantly Bado type I) and an adult peak in middle age and the elderly (predominantly type II).
- There is no single-country pattern - the adult type II predominance and paediatric type I predominance are consistent across North American, European and Asian cohorts.
Guidelines & Society Positions (Side by Side)
- Core Position
- Anatomic reduction and stable plate fixation of the ulna; radial head reduces with correct ulna alignment
- Practical Emphasis
- Restore ulna length, alignment and rotation; intra-op fluoroscopic check of radiocapitellar line
- Core Position
- Treat as a fracture-dislocation - urgent assessment, documented neurovascular exam, early definitive fixation
- Practical Emphasis
- Open injuries follow standard open-fracture pathways; senior-led decision-making
- Core Position
- Operative fixation is standard in adults; emphasis on detecting associated radial head and coronoid injury
- Practical Emphasis
- Address coronoid and radial head fractures at the index procedure
- Core Position
- Closed reduction acceptable for acute, stable (incomplete) paediatric ulna patterns; operate if unstable or chronic
- Practical Emphasis
- Low threshold to fix unstable complete ulna fractures; never excise the radial head in a child
There is no dedicated randomised guideline for Monteggia fractures - guidance is consensus/expert based. The internationally shared principle across AO, BOA, AAOS and paediatric bodies is identical: fix the ulna anatomically and the radial head follows.
Registry & Resource-Setting Variation
- No national arthroplasty/implant registry tracks Monteggia outcomes specifically; evidence is from single-centre and tertiary trauma-centre series rather than registry data.
- High-resource settings: routine fluoroscopy, locking plates, on-table radial head implants, and ready paediatric subspecialty referral.
- Limited-resource settings: missed and chronic (neglected) Monteggia is proportionally far more common because the radiocapitellar line is not checked on the initial film; reconstruction (ulna osteotomy with indirect or open radial head reduction) is therefore a more frequent presentation.
Monteggia fractures are among the most commonly missed injuries.
- Document radiocapitellar line assessment on ALL views
- Note PIN function pre- and post-operatively
- Record stability of radial head after fixation
- Missed diagnosis (most common)
- Delayed treatment leading to chronic Monteggia
- Failure to document pre-existing PIN palsy
- Poor outcomes from chronic reconstruction
Controversies & Areas of Uncertainty
In chronic paediatric cases, ulna osteotomy with indirect reduction can stabilise the radial head without formal reconstruction (Song 2012). When the annular ligament is addressed, repair of the native ligament outperformed reconstruction (Zheng 2020). Many now reserve formal Bell Tawse reconstruction for cases that remain unstable intra-operatively.
Whether to open the radiocapitellar joint or rely on over-correction of the ulna (angulation-translation osteotomy) remains debated; both can succeed and the choice is often driven by chronicity, radial head shape and intra-operative stability.
Trans-capitellar/transarticular K-wires can hold a reduced radial head but carry a real risk of wire breakage and migration. Use is selective, kept short (3-4 weeks), and avoided where stable fixation alone is sufficient.
Most PIN palsies are neurapraxic and recover, so early exploration is generally not indicated. The grey zone is the new, complete post-reduction palsy where nerve entrapment cannot be excluded - timing of exploration and the role of early EMG/nerve ultrasound are not standardised.
Mnemonics for Exam Recall
APLABADO Types by Direction
Hook:A Push Leads to Anterior dislocation (Type I flexion injury)
MISSMISS - Critical Checks
Hook:Don't MISS the Monteggia - check the line!
ULNAULNA - Fixation Goals
Hook:Fix the ULNA and the radial head follows
PINPIN - Nerve at Risk
Hook:PIN is at risk in Monteggia - specifically Posterior Interosseous Nerve
MCQ Practice Points
Q: What radiographic line must be checked on every elbow X-ray to avoid missing a Monteggia fracture?
A: The radiocapitellar line. A line drawn through the center of the radial neck must bisect the center of the capitellum on ALL views (AP, lateral, oblique). Disruption indicates radial head dislocation.
Q: What is the most common Bado type in adults vs children?
A: Adults: Type II (70%) - posterior radial head dislocation with posterior ulna angulation. Children: Type I - anterior radial head dislocation with anterior ulna angulation. This is commonly tested.
Q: After anatomic ulna fixation, the radial head does not reduce. What is your next step?
A: The radial head should reduce spontaneously after anatomic ulna fixation. If it doesn't: 1) Confirm ulna reduction is truly anatomic (length and alignment). 2) If still subluxed, explore through Kocher approach for interposed tissue (annular ligament, capsule, or biceps).
Q: A patient develops finger drop after Monteggia ORIF. What is the likely diagnosis and prognosis?
A: PIN (Posterior Interosseous Nerve) palsy. Occurs in 10-20% of Monteggia injuries. Usually a neurapraxia from traction during injury (not iatrogenic). Excellent prognosis - most recover spontaneously within 3-4 months. Observe unless new post-op or concern for entrapment.
Q: What is the treatment for a Monteggia fracture diagnosed 6 weeks after injury?
A: Chronic Monteggia (greater than 4 weeks) has poor outcomes with simple reduction. Requires: ulna osteotomy (to restore length), open reduction of radial head, and annular ligament reconstruction (Bell Tawse technique using triceps tendon strip). Results are inferior to acute treatment.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old construction worker presents after falling from scaffolding. X-rays show proximal ulna fracture with posterior radial head dislocation.”
“A 7-year-old child presents 6 weeks after a fall. Parents were told the 'wrist fracture healed well' at another hospital. You notice limited forearm rotation and prominent radial head.”
“You fix an acute Type II Monteggia fracture with anatomic ulna reduction and the radial head reduces concentrically. Post-operatively, the patient cannot extend fingers at MCPJs.”
Key Stats
- 1-2% of forearm fractures
- Type II (posterior) = 70% in adults
- Type I (anterior) = most common in children
- PIN palsy 10-20%
- Missed diagnosis rate approximately 5%
Bado Classification
- Type I - Anterior RH dislocation, anterior ulna angulation
- Type II - Posterior RH dislocation, posterior ulna angulation
- Type III - Lateral RH dislocation, ulna metaphyseal fracture
- Type IV - Anterior RH dislocation, both bone fractures
Key Principles
- Radiocapitellar line MUST bisect capitellum on ALL views
- Fix ulna anatomically - RH reduces spontaneously
- If RH doesn't reduce - explore for interposed tissue
- Chronic (more than 4 weeks) - annular ligament reconstruction needed
- PIN palsy - usually recovers, observe 3-4 months
Surgical Steps
- Position supine, arm on table
- Boyd posterior approach to ulna
- Anatomic reduction - restore length/alignment
- 3.5mm LCP plate fixation (6-8 holes)
- Check radiocapitellar line on fluoro
- If RH subluxed - Kocher approach to explore
Must Know for Exam
- Most missed injury - ALWAYS check radiocapitellar line
- Adult vs pediatric types differ (II vs I)
- PIN palsy is neurapraxia - observe
- Chronic has poor outcomes - emphasizes early diagnosis
- Bell Tawse technique for annular ligament reconstruction
Evidence Base and Literature
Key Studies and Papers
Bado Original Classification
- Defined the Monteggia lesion and four types by direction of radial head dislocation and ulna deformity
Annular Ligament Reconstruction (Bell Tawse)
- Described use of a triceps fascia strip to create a neo-annular ligament for chronic radial head dislocation
Monteggia Fractures in Adults
- 48 adults; 38 (79%) were Bado type II; 68% of type II had an associated radial head fracture
- Excellent or good Broberg-Morrey result in 40 of 48 patients (83%) after stable anatomic plate fixation of the ulna
- 6 of 8 unsatisfactory results were type II with concomitant radial head/coronoid fractures
Monteggia Fractures in Children and Adults (Principle Review)
- Stable anatomic reduction of the ulna fracture restores anatomic reduction of the radial head
- Character of the ulna fracture (not the direction of dislocation) guides treatment
- Good non-operative results in children reflect prevalence of incomplete (stable) ulna fractures
Surgical Reconstruction of Missed Monteggia Lesions in Children
- 52 children; median time injury-to-surgery 12.9 weeks; flexion improved from 108 to 140 degrees
- Congruent radiocapitellar alignment maintained in 39 of 52 (75%); 17% redislocated, 8% resubluxated
- Repair of the native annular ligament gave more durable stability than reconstruction or no annular procedure
Indirect Reduction of the Radial Head in Chronic Paediatric Monteggia
- 10 missed paediatric Monteggia treated with angulation-translation ulna osteotomy and closed (indirect) reduction
- Radial head reduction achieved and maintained in 8 of 10 at mean 10-year follow-up
- Annular ligament reconstruction performed in only 2 cases - not required in every case
Surgical Management of Complex Adult Monteggia Fractures
- Jupiter classification subdivides Bado posterior (type II) lesions; coronoid involvement and proximal ulna comminution markedly raise complexity
- Coronoid access is difficult from a posterior approach, risking tenuous reduction and worse function
Salvage of Malaligned Posterior Monteggia Fractures
- 17 patients with malalignment after fixation of a posterior Monteggia; 15 had loose fixation
- Realignment with a dorsal contoured plate achieved union and concentric ulnohumeral reduction in all 17
- Excellent/good result in 14 of 17 at mean 59 months