Forearm Ring Concept | Bado Classification | Fracture of Necessity | Fix the Bone, Reduce the Joint
- Forearm ring concept: PRUJ + IOM + DRUJ - if one bone fractured with displacement, disruption must occur elsewhere
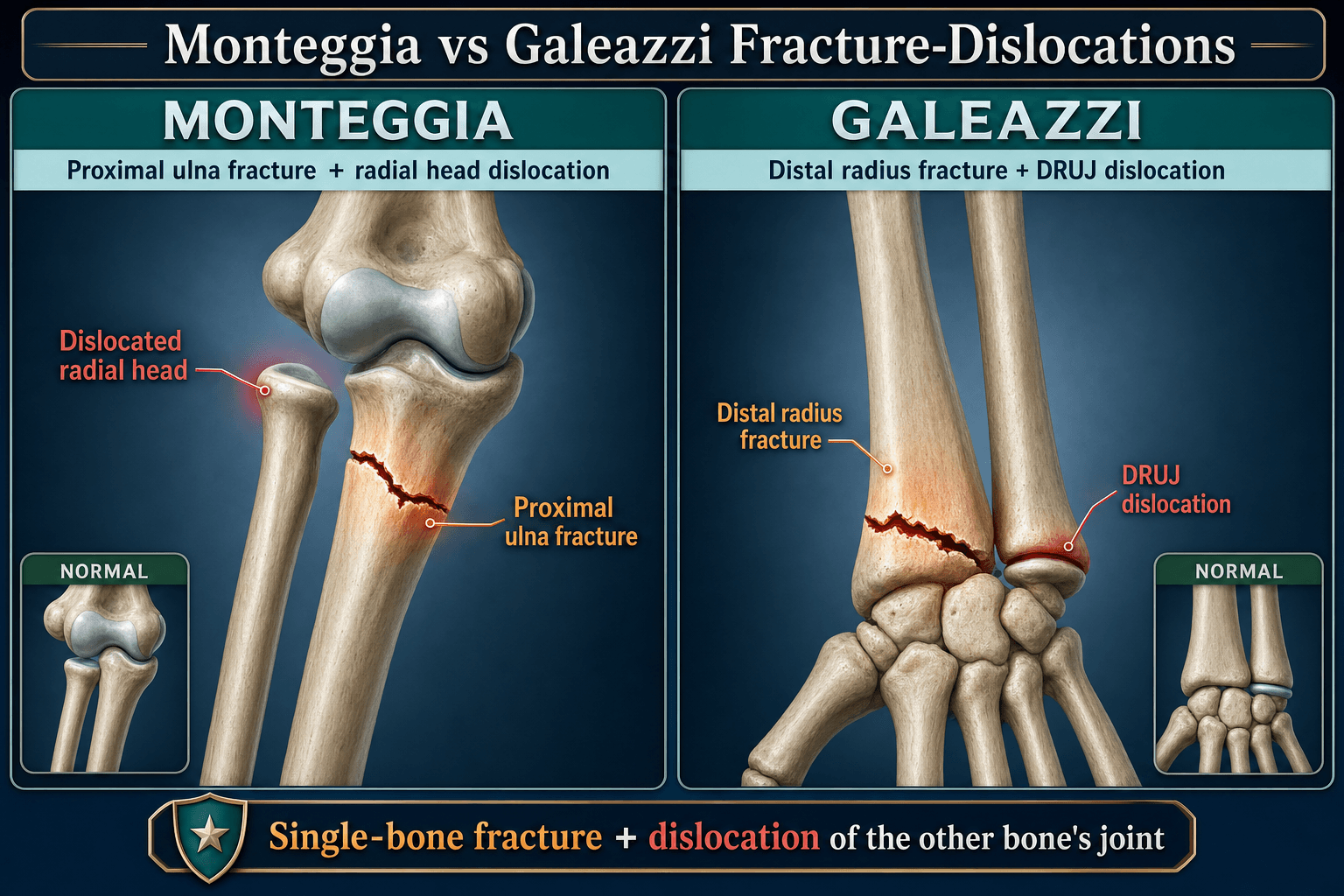
- Monteggia = proximal Ulna fracture + radial head dislocation (M = Misses radial head at elbow)
- Galeazzi = distal Radius fracture + DRUJ disruption (G = Got the wrist DRUJ) - 'fracture of necessity'
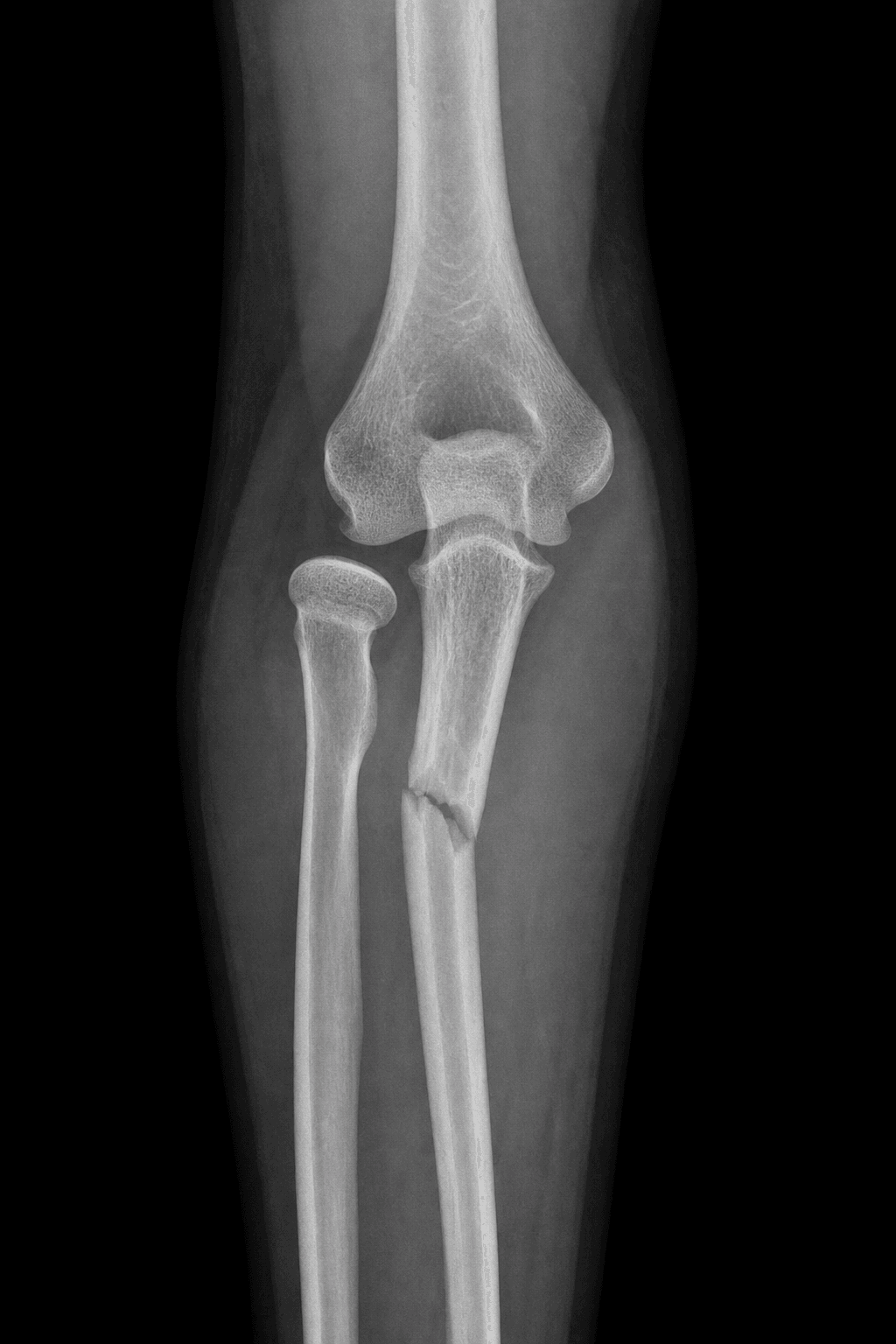
- Radiocapitellar line: Draw along radial neck/shaft axis - must pass through capitellum on ALL views
- Key principle: Fix the fractured bone anatomically and the joint usually reduces spontaneously
- “Bado classification for Monteggia: Type I anterior (most common overall), Type II posterior (PIN risk, commonest in adults), Type III lateral, Type IV both bones
- “'Any isolated ulna fracture is a Monteggia until proven otherwise' - always image the elbow
- “Galeazzi DRUJ assessment: After ORIF radius, stress test in neutral/pronation/supination - supination is most stable
- “Missed Monteggia = major medico-legal issue - chronic radial head dislocation has poor reconstruction outcomes
Monteggia and Galeazzi Fractures
Misses the radial head (proximal = elbow). Any isolated ulna fracture is a Monteggia until proven otherwise.
Got the DRUJ (distal = wrist). Distal radius fracture with DRUJ disruption. "Fracture of necessity" - surgery in adults.
The forearm is a ring structure. If one bone is fractured and displaced, there must be disruption elsewhere (either the other bone or a joint).
Always image the entire forearm including joints above (elbow) and below (wrist). Missing a joint injury is a major pitfall.
At a Glance
Monteggia and Galeazzi are the two classic forearm fracture-dislocations that test the ring concept: fix the fractured bone anatomically and the dislocated joint usually reduces. Monteggia = proximal ulna fracture + radial head dislocation (Bado I-IV). Galeazzi = distal-third radius fracture + DRUJ disruption, the "fracture of necessity". The dominant mistake in both is missing the associated joint injury.
MUGRMonteggia vs Galeazzi
Hook:MUGR: Monteggia = Upper/elbow, Galeazzi = wRist
Overview and Epidemiology
Monteggia and Galeazzi fractures are the two classic forearm fracture-dislocations that test the ring concept: because the radius and ulna are bound at both ends (PRUJ and DRUJ) and along the shaft (interosseous membrane), a displaced fracture of one bone mandates a corresponding joint or bony disruption elsewhere. Missing the associated joint injury is the central pitfall in both.
- Monteggia = proximal ulna fracture + radial head dislocation. Classified by Bado I-IV. Type I (anterior) is most common overall and the dominant paediatric pattern; Type II (posterior) is the commonest pattern in adults (Ring, JBJS Am 1998).
- Galeazzi = fracture of the distal third of the radius + DRUJ disruption. The "fracture of necessity" - conservative treatment fails in ~80% of adults (Mikic, JBJS Am 1975), so adults require ORIF.
Epidemiology (global):
- Monteggia lesions account for roughly 1-2% of forearm fractures; bimodal, with a paediatric peak (fall on outstretched hand) and an adult peak (higher-energy trauma, often Bado II).
- Galeazzi fracture-dislocations comprise ~3-7% of forearm fractures, predominantly adults aged 30-50, frequently work- or sport-related.
- Across all settings the governing principle is identical: fix the fractured bone anatomically and the joint usually reduces.
Anatomy and Biomechanics
The Forearm Ring Concept
The forearm functions as a closed ring whose three links must all be intact for normal rotation:
- Proximal radioulnar joint (PRUJ) - radial head in the radial notch of the ulna; stabilised by the annular ligament. Disrupted in Monteggia.
- Interosseous membrane (IOM) - the central band transmits ~70% of axial load from the radius to the ulna; the key longitudinal stabiliser.
- Distal radioulnar joint (DRUJ) - ulna head in the sigmoid notch of the radius; primary stabiliser is the TFCC. Disrupted in Galeazzi.
If one bone fractures and displaces, the ring must fail elsewhere. Hence an isolated displaced ulna fracture is a Monteggia until proven otherwise, and any distal radius fracture demands DRUJ assessment.
- TFCC (triangular fibrocartilage complex) - primary stabiliser; dorsal and palmar radioulnar ligaments
- Interosseous membrane and pronator quadratus
- ECU subsheath
- Location
- Elbow
- Clinical Relevance
- Radial head dislocation in Monteggia
- Location
- Central forearm
- Clinical Relevance
- Longitudinal stability; lost in Essex-Lopresti
- Location
- Wrist
- Clinical Relevance
- Disrupted in Galeazzi
Mechanism of Injury
- FOOSH with forced hyperpronation (classically Type I, anterior)
- Direct blow to the posterior proximal forearm
- Axial load through a supinated forearm (associated with Type II in adults)
- FOOSH with the forearm pronated
- Direct dorsoradial blow to the wrist
- Axial load with rotation
Classification Systems
Bado Classification of Monteggia Lesions
Classified by the direction of radial head dislocation and the associated ulna fracture pattern.
- Type I - Anterior radial head dislocation; ulna fracture with anterior angulation. Most common type overall and the dominant paediatric pattern. Mechanism: hyperpronation.
- Type II - Posterior/posterolateral radial head dislocation; ulna fracture with posterior angulation. Commonest pattern in adults and frequently associated with radial head and coronoid fractures. Highest PIN palsy association.
- Type III - Lateral/anterolateral radial head dislocation; ulnar metaphyseal fracture. Largely a paediatric injury.
- Type IV - Anterior radial head dislocation with fractures of both radius and ulna in the proximal third.
- Radial head
- Anterior
- Ulna fracture
- Anterior angulation
- Note
- Commonest overall / paediatric
- Radial head
- Posterior
- Ulna fracture
- Posterior angulation
- Note
- Commonest in adults; PIN risk
- Radial head
- Lateral
- Ulna fracture
- Metaphyseal
- Note
- Paediatric
- Radial head
- Anterior
- Ulna fracture
- Both-bone proximal third
- Note
- Rare
APLBBado Classification (Monteggia)
Hook:APLB = Anterior-Posterior-Lateral-Both - directions the radial head goes
Clinical Assessment
- Pain, swelling and deformity of the proximal forearm/elbow
- Palpable/dislocated radial head; reduced elbow flexion-extension and forearm rotation
- Always test PIN function (especially Type II): finger and thumb extension at MCP joints, wrist extension in radial deviation. Document pre- and post-operatively.
- Wrist pain and swelling; tenderness over the DRUJ and ulnar fovea
- Prominent ulna head (dorsal or palmar depending on rotation)
- Painful, restricted forearm rotation
- Assess the median nerve / AIN given the volar surgical territory
- Monteggia
- Proximal ulna
- Galeazzi
- Distal third of radius
- Monteggia
- Radial head position
- Galeazzi
- DRUJ
- Monteggia
- Radiocapitellar line disrupted
- Galeazzi
- DRUJ widening over 2mm vs contralateral; radial shortening; ulnar styloid base fracture
On every elbow view (AP, lateral, oblique), a line drawn along the axis of the radial neck/shaft must pass through the centre of the capitellum. If it misses, the radial head is dislocated. This single check is how missed Monteggia injuries are caught.
Investigations
Radiographic Assessment
- AP and lateral of the entire forearm
- Dedicated elbow views (AP, lateral) - mandatory for any ulna fracture
- Dedicated wrist views (PA, lateral) - mandatory for any distal radius fracture
- Contralateral comparison views are invaluable for ulnar variance and DRUJ width
- Proximal ulna fracture with angulation
- Radiocapitellar line disrupted on at least one view
- Coronoid and radial head fractures in Bado II (look specifically)
- Distal radius fracture (middle/distal third junction)
- DRUJ widening over 2mm compared with the contralateral side
- Ulnar styloid (base) fracture indicating TFCC avulsion
- Radial shortening / loss of radial height
- Monteggia
- Proximal ulna
- Galeazzi
- Distal radius
- Monteggia
- Radial head position
- Galeazzi
- DRUJ widening
- Monteggia
- Radiocapitellar line
- Galeazzi
- Radial height + DRUJ width
Differential Diagnosis
The differential is about recognising the whole injury rather than the obvious fracture, and distinguishing the fracture-dislocations from their mimics.
- Fracture
- Proximal ulna
- Joint disruption
- Radial head (PRUJ)
- Distinguishing feature
- Radiocapitellar line disrupted on elbow views
- Fracture
- Distal radius
- Joint disruption
- DRUJ
- Distinguishing feature
- DRUJ widening, radial shortening, ulnar styloid base fracture
- Fracture
- Ulna shaft, minimally displaced
- Joint disruption
- None
- Distinguishing feature
- Radial head congruent on all views (must exclude Monteggia)
- Fracture
- Radial head
- Joint disruption
- DRUJ + IOM
- Distinguishing feature
- Longitudinal pain; IOM ruptured; do NOT excise radial head
- Fracture
- Radius + ulna shafts
- Joint disruption
- Usually none
- Distinguishing feature
- Two shaft fractures without a joint dislocation
- Fracture
- None
- Joint disruption
- Chronic radial head dislocation
- Distinguishing feature
- Bilateral, dome-shaped/hypoplastic capitellum, convex radial head, no trauma
Management Algorithm

- ORIF of the ulna restores length, alignment and IOM tension.
- 3.5mm DCP or LCP; compression plating for simple patterns, bridge plating if comminuted
- Anatomic reduction is the single most important step
- Assess the radial head after ulna fixation.
- Reduces concentrically and is stable in most cases - no further action
- Irreducible/unstable: explore for interposed annular ligament/capsule; repair or reconstruct as needed
- In Bado II address associated radial head and coronoid fractures
- Post-op: brief protection then early ROM; avoid forced rotation initially.
- Closed reduction of the ulna often restores the radial head
- Fix the ulna (flexible nail or plate) if the reduction is unstable or for length-unstable patterns
FASGaleazzi Management
Hook:Be FASt to recognise and treat Galeazzi - Fix, Assess, Stabilise
Surgical Technique
Monteggia ORIF
- Supine, arm table, tourniquet
- Posterior (subcutaneous border) approach to the proximal ulna; lateral Kocher interval (anconeus / ECU) if the radial head must be explored
- 3.5mm DCP or LCP
- Compression plating for simple patterns; bridge plating if comminuted
- Restore length and correct angulation precisely - this is what reduces the radial head
- After fixing the ulna, take the elbow through full flexion-extension and pronation-supination
- Concentric, stable reduction in most cases
- If unstable/irreducible: explore via Kocher, remove interposed annular ligament/capsule, repair or reconstruct the annular ligament; address radial head/coronoid fractures (Bado II)
- Approach
- Posterior ulna (+/- lateral Kocher)
- Plate
- 3.5mm DCP/LCP
- Approach
- Volar Henry radius
- Plate
- 3.5mm or anatomic plate
Key Differences
Monteggia vs Galeazzi Comparison
Complications
- Missed diagnosis - the most important and most preventable complication; up to half are missed initially, leading to chronic radial head dislocation that is difficult to reconstruct (see Controversies).
- Radial head instability - usually from inadequate ulna reduction; occasionally interposed annular ligament. Re-examine ulna alignment first.
- PIN palsy - associated with Bado II; usually neurapraxia that recovers; document function pre- and post-op.
- Proximal radioulnar synostosis / heterotopic ossification - more frequent after high-energy Bado II and radial head fixation.
- Stiffness - mitigated by early mobilisation once fixation is stable.
Nerve Injuries in Forearm Fracture-Dislocations
Both injuries carry a characteristic - and different - neurological risk that the topic repeatedly flags but which deserves explicit examination technique and a management plan. Document nerve function before and after any manipulation or surgery.
- The PIN (the deep, motor continuation of the radial nerve) winds around the radial neck and passes between the two heads of supinator, entering beneath its proximal fibrous edge (the arcade of Frohse). A displaced radial head therefore stretches or compresses it - PIN palsy is the commonest nerve lesion in Monteggia. It is emphasised with the posterior (Bado II) pattern in adults but also occurs with anterior (Bado I) and lateral (Bado III) radial head displacement, especially in children.
- It is a pure motor deficit with no sensory loss. Test extension of the fingers and thumb at the MCP joints and wrist extension: the wrist still extends but drifts into radial deviation because ECRL (innervated proximal to the PIN) is spared while ECU is denervated.
- Natural history is favourable: most are a neurapraxia that recovers spontaneously once the radial head is reduced, typically over roughly 8 to 12 weeks. Observe after anatomic reduction; obtain nerve conduction studies if there is no recovery by about three months and consider exploration then (or earlier if the nerve is suspected to be entrapped at open reduction).
- The AIN (a motor branch of the median nerve) and the median nerve itself lie in the volar (Henry) surgical territory used for radial fixation, so a deficit is usually an iatrogenic retraction neurapraxia rather than a primary injury.
- Test the AIN with the "OK" sign (FPL and index FDP - flexion of the thumb IP and index DIP joints) and check median sensation over the volar radial three-and-a-half digits. Recovery from a retraction neurapraxia is the rule.
A patient who can extend the wrist but only into radial deviation, with preserved sensation, has a PIN palsy rather than a complete radial nerve injury: ECRL is spared (its branches leave proximal to the PIN) while ECU is denervated. After a Monteggia reduction this is almost always a recovering neurapraxia - reduce the radial head, document the deficit, and observe rather than rush to explore.
The Irreducible Joint: Blocks to Reduction
The governing rule - fix the fractured bone and the joint reduces - fails in a minority, and the reason differs at each end of the forearm. Distinguish a joint that is reducible but unstable (immobilise or transfix) from one that is irreducible because a structure is mechanically blocking it (mandating open reduction). Never transfix or cast a joint that is not concentrically reduced.
- First re-check the ulna. The commonest reason a radial head stays dislocated after fixation is inadequate ulnar reduction - residual loss of length or angulation - so revise the osteosynthesis before blaming soft tissue.
- A true mechanical block is usually the torn or inverted annular ligament, interposed capsule, or an osteochondral/radial head fragment lying in the joint. This requires open reduction through a lateral (Kocher) interval to extract the interposed tissue and repair or reconstruct the annular ligament.
- After anatomic radial fixation most DRUJs reduce; if one remains frankly dislocated rather than merely lax, suspect an interposed structure. The classic culprit is the extensor carpi ulnaris (ECU) tendon and its subsheath displaced into the joint, sometimes with the extensor digiti minimi/EDC tendons or an entrapped ulnar styloid fragment, or the volar capsule buttonholed by the ulnar head.
- An irreducible DRUJ needs open reduction, usually through a dorsal approach, to lift the interposed tendon out of the joint and repair the TFCC/subsheath - it cannot be solved by forcing supination or by transfixing an unreduced joint.
The DRUJ K-wire and supination cast only work on a joint that is already concentrically reduced. Confirm reduction on a true lateral wrist radiograph; if the ulnar head remains dorsally or volarly displaced despite radial fixation, that is an irreducible DRUJ (think interposed ECU tendon) requiring open reduction - not more immobilisation.
Postoperative Care
Rehabilitation Protocol
- Brief backslab (~2 weeks) for wound/soft-tissue rest, then early elbow and rotation ROM
- Avoid extremes of pronation/supination for 4-6 weeks
- Aim for full ROM by 8-12 weeks
- Removable splint for comfort ~2 weeks, then early active ROM
- Progressive strengthening from ~6 weeks
- Supination cast or K-wires for ~6 weeks, then ROM
- Delayed start but still aim for full ROM
Outcomes and Prognosis
Expected Results
- Good/excellent results in the majority with anatomic ulna fixation; in Ring's adult series 40 of 48 were excellent/good
- Unsatisfactory outcomes cluster in Bado II with associated radial head/coronoid injury
- Minor loss of terminal extension is common; forearm rotation usually preserved
- Good results with anatomic radial fixation and a stable (or stabilised) DRUJ
- Worse outcomes with residual radial shortening or persistent DRUJ instability
- Significantly poorer; chronic Monteggia reconstruction in children gives meaningful but incomplete gains, and results are best when surgery is within one year (Chen 2018)
- Chronic DRUJ instability: variable results with reconstruction
- Acute Treatment
- Good/excellent in most (40/48 in Ring)
- Chronic
- Better if within 1 year; incomplete
- Acute Treatment
- Good with stable DRUJ
- Chronic
- Variable with DRUJ reconstruction
Guidelines, Registries & Global Practice
OrthoVellum is a global resource - the principles below hold across exam systems (FRCS, FRACS, EBOT/FEBOT, ABOS, DNB/MS, MRCS, SICOT).
Global epidemiology:
- Monteggia lesions: ~1-2% of forearm fractures; paediatric peak (Type I/III) and adult peak (Type II, higher-energy).
- Galeazzi: ~3-7% of forearm fractures; adults 30-50, often occupational/sport.
Side-by-side guidance and consensus (recommendations are broadly concordant):
- Position on these injuries
- Anatomic ORIF of the fractured bone with plate fixation; restore length/alignment so the joint reduces; assess and address the associated joint
- Position on these injuries
- Adult diaphyseal forearm and forearm fracture-dislocations managed operatively with timely imaging of the whole forearm including both joints
- Position on these injuries
- No injury-specific clinical practice guideline; teaching follows the ring-concept and anatomic fixation principles above
- Position on these injuries
- Endorses anatomic radial/ulnar fixation and intraoperative joint (radial head / DRUJ) assessment
Acute forearm fracture-dislocation fixation is not captured in arthroplasty registries (NJR, AJRR, AOANJRR), as these injuries are managed with osteosynthesis rather than implants; the evidence base is case series and classification studies rather than registry or RCT data.
- Well-resourced settings: routine CT for complex Bado II, locking plates, intraoperative fluoroscopic DRUJ stress testing, radial head arthroplasty available for Essex-Lopresti.
- Limited-resource settings: greater reliance on plain radiographs and contralateral comparison, conventional DCP fixation, K-wire DRUJ transfixation and supination casting; the same anatomic-reduction principles still govern outcome.
- Universal priority everywhere: image the whole forearm and both joints and check the radiocapitellar line - the diagnostic miss, not the implant, is the main cause of poor outcomes.
Controversies and Areas of Uncertainty
- Reconstruct vs accept the chronically dislocated radial head (paediatric Monteggia): Reconstruction (ulnar osteotomy +/- open reduction +/- annular ligament reconstruction) improves stability and pain but carries notable complication rates and unpredictable rotation, and outcomes deteriorate beyond one year. Some advocate observation in late/minimally symptomatic presentations. There is genuine debate over whether annular ligament reconstruction is necessary at all - Chen et al achieved maintained reduction in 18 of 20 children without it, relying on ulnar lengthening/angulation osteotomy.
- Need for trans-capitellar K-wires: Useful when radial head reduction is unstable, but they risk breakage and are avoided by some surgeons in favour of robust osteotomy correction.
- Bado II radial head and coronoid management: The decision to fix, replace or excise the radial head, and whether to fix small coronoid fragments, drives outcome in adult Monteggia and remains individualised.
- Galeazzi DRUJ: how to stabilise: Choice between K-wire transfixation, supination immobilisation, TFCC repair and ulnar styloid fixation is not standardised; the unifying principle is anatomic radial length restoration first, then test and treat residual instability.
- Ulnar styloid fixation: Whether to fix a styloid base fragment in an otherwise stable DRUJ is contested; isolated tip fractures generally do not need fixation.
MCQ Practice Points
Q: What is the Bado classification of Monteggia fractures?
A: Type I: anterior radial head dislocation, anterior ulna angulation (commonest overall). Type II: posterior dislocation, posterior angulation (commonest in adults, PIN risk). Type III: lateral dislocation, metaphyseal ulna fracture (paediatric). Type IV: anterior dislocation with both-bone proximal-third fractures. All require radiocapitellar line assessment.
Q: What radiographic line must be checked to diagnose a Monteggia lesion?
A: The radiocapitellar line - drawn along the radial neck/shaft axis it should pass through the capitellum on all views (AP, lateral, oblique). Disruption indicates radial head dislocation. "Any isolated ulna fracture is a Monteggia until proven otherwise" - always obtain elbow views. Missed in up to 50% initially.
Q: What defines a Galeazzi fracture-dislocation?
A: Distal radius fracture with DRUJ disruption. Called the "fracture of necessity" - requires surgery in adults. DRUJ instability arises from a disrupted TFCC and loss of radial length. Signs: ulnar fovea tenderness, DRUJ widening on PA view, ulnar styloid base fracture, and instability on stress testing.
Q: What is the Essex-Lopresti injury?
A: Radial head fracture + interosseous membrane disruption + DRUJ instability (longitudinal radioulnar dissociation). If the radial head is excised, the radius migrates proximally causing wrist pain and weakness. Treat with radial head replacement (not excision) and protect/reconstruct the IOM.
Q: Why is anatomic ulna reduction critical in Monteggia treatment?
A: Anatomic ulna reduction restores length and IOM tension so the radial head usually reduces spontaneously. Persistent dislocation after ulna fixation suggests interposed tissue (annular ligament/capsule) requiring open reduction. In children, anatomic closed reduction is often sufficient; adults typically need ORIF of the ulna.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents to the emergency department after falling from a ladder onto his outstretched dominant right arm. He has pain and deformity of the proximal forearm. X-rays show a fracture of the proximal ulna with anterior angulation. On the AP view, the radial head appears congruent with the capitellum, but on the lateral view, the radial head appears to be slightly anterior to the capitellum. What is your diagnosis and how do you manage this injury?”
“A 28-year-old professional gymnast falls on her outstretched hand during training. She has pain at the wrist and distal forearm. X-rays show a fracture of the distal radius at the junction of the middle and distal thirds with dorsal angulation. You also notice the DRUJ appears widened compared to the contralateral side (3mm vs 1mm), and there is a small ulnar styloid fracture. The emergency department doctor asks if this can be treated in a cast. What is your diagnosis and management plan?”
“You are asked to see a 12-year-old boy referred by his GP for a 'funny elbow'. He fell from monkey bars 8 months ago and was treated in a cast for an 'ulna fracture' at another hospital. Since the cast came off he has progressive elbow pain and cannot fully extend or supinate. Examination shows a prominent radial head laterally. X-rays show a healed ulna fracture with residual anterior angulation, and the radial head is dislocated anteriorly/laterally with a flattened, dome-shaped capitellum. What has happened and how do you manage this?”
Monteggia
- Proximal ulna fracture + radial head dislocation
- Bado I anterior (commonest overall); Type II posterior commonest in adults (PIN risk)
- Fix ulna anatomically and the radial head reduces
- Check radiocapitellar line on all views
Galeazzi
- Distal radius fracture + DRUJ disruption
- Fracture of necessity - operate in adults (~80% conservative failure)
- ORIF radius, restore length, then assess DRUJ stability
- Supination is the stable position for the DRUJ
Ring Concept
- Forearm = ring (PRUJ + IOM + DRUJ)
- If one bone fractured + displaced...
- ...there must be disruption elsewhere
- Always X-ray entire forearm + both joints
Key Complications
- Missed diagnosis (especially Monteggia)
- Persistent joint instability
- Malunion affecting rotation
- PIN palsy (Monteggia Type II)
Evidence Base and References
Monteggia Fractures in Adults (Bado II Predominance)
- 48 adult Monteggia fractures, mean follow-up 6.5 years
- Bado type II (posterior) was the commonest adult pattern (38 of 48)
- 26 of 38 type II had associated radial head fractures; coronoid fractures common
- Stable anatomic plate fixation of the ulna gave excellent/good results in 40 of 48; unsatisfactory outcomes clustered in type II with radial head/coronoid involvement
Galeazzi 'Fracture of Necessity'
- 125 patients with Galeazzi-type fracture-dislocations (86 adults with the classic lesion)
- Conservative (cast) treatment failed in ~80% of adults; succeeded only in children
- Operative fixation of both the radius and the DRUJ gave excellent results in over half
- Established the 'fracture of necessity' concept - radial shortening perpetuates DRUJ instability
Galeazzi: Treatment-Oriented Classification (7.5cm Rule)
- 40 Galeazzi fractures treated with ORIF of the radial shaft
- Type I (fracture within 7.5cm of the distal radius articular surface): 12 of 22 had intraoperative DRUJ instability
- Type II (fracture over 7.5cm from the joint, middle third): only 1 of 18 unstable
- Distance of the radial fracture from the DRUJ predicts the need for DRUJ stabilisation
Chronic (Missed) Monteggia in Children
- 20 children with neglected radial head dislocation after missed Monteggia
- Open reduction plus ulnar lengthening/angulation osteotomy without annular ligament reconstruction
- Significant gains in elbow flexion, pain and stability (MEPI); radial head reduction maintained in 18 of 20
- Surgery within one year of injury gave better functional outcomes than later presentation
Bado Classification of the Monteggia Lesion
- Original description of the Monteggia lesion and its four types
- Types I-IV defined by direction of radial head dislocation and ulna fracture pattern
- Type I anterior is the most common type overall
- Remains the universal classification for describing Monteggia injuries
Full reference list:
- Bado JL. The Monteggia lesion. Clin Orthop Relat Res. 1967;50:71-86.
- Ring D, Jupiter JB, Simpson NS. Monteggia fractures in adults. J Bone Joint Surg Am. 1998;80(12):1733-44. PMID 9875931.
- Mikic ZD. Galeazzi fracture-dislocations. J Bone Joint Surg Am. 1975;57(8):1071-80. PMID 1201989.
- Rettig ME, Raskin KB. Galeazzi fracture-dislocation: a new treatment-oriented classification. J Hand Surg Am. 2001;26(2):228-35. PMID 11279568.
- Chen HY, Wu KW, Dong ZR, et al. The treatment of chronic radial head dislocation in Monteggia fracture without annular ligament reconstruction. Int Orthop. 2018;42(9):2165-72. PMID 29713746.