Plasma Cell Neoplasm | Lytic Bone Disease | CRAB Criteria
- CRAB criteria define symptomatic myeloma requiring treatment - must have end-organ damage
- Lytic lesions show NO blastic response - purely osteolytic, unlike metastases which may show healing
- Bisphosphonates are mandatory for all patients with bone disease to prevent skeletal events
- Pathological fractures common in vertebrae, ribs, and long bones - prophylactic fixation for impending fractures
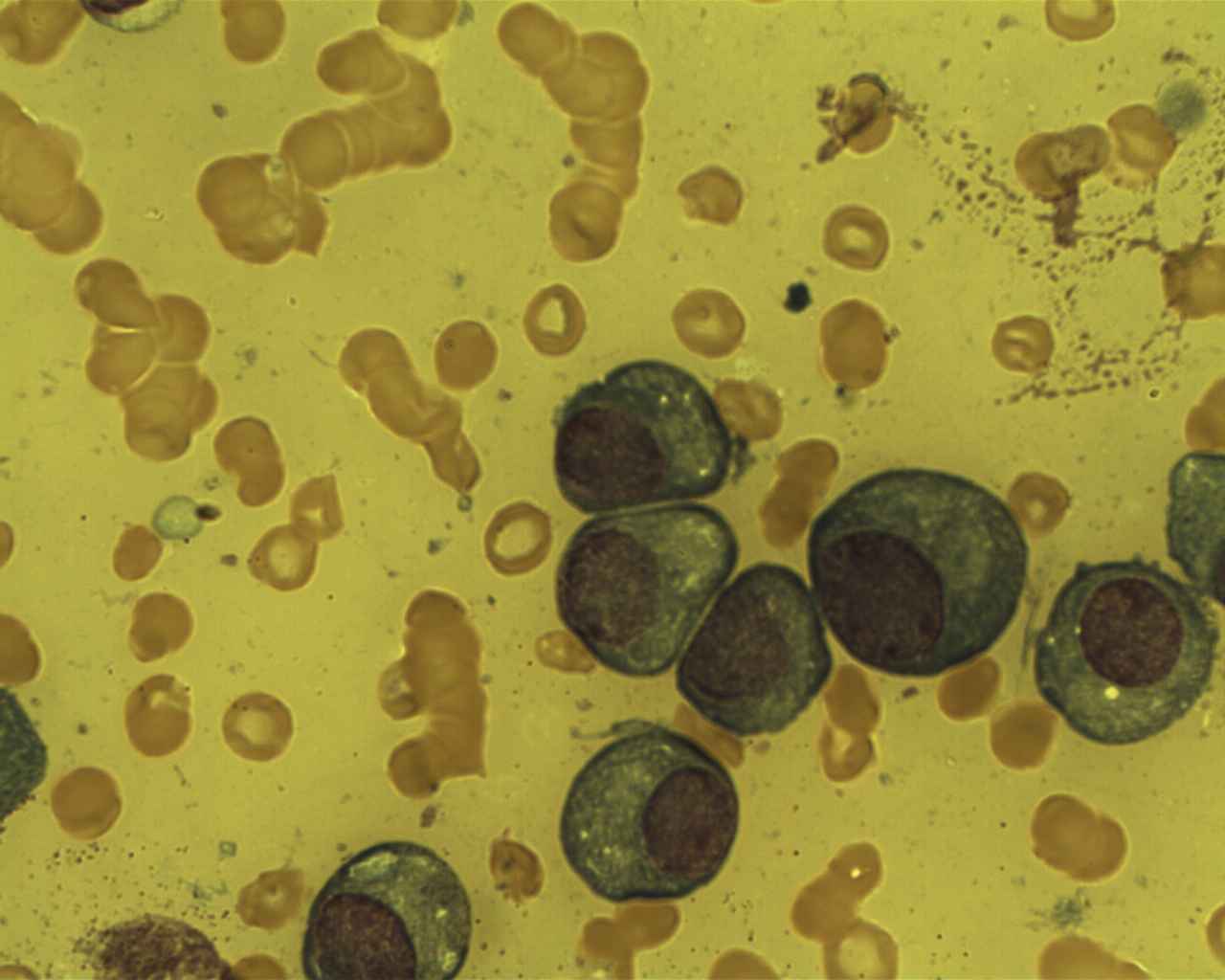
- Diagnosis requires serum protein electrophoresis (SPEP), urine protein, and bone marrow biopsy showing over 10% plasma cells
- “Purely lytic lesions with NO sclerotic response differentiates myeloma from metastatic disease
- “Whole-body MRI or PET-CT more sensitive than skeletal survey for detecting bone involvement
- “Impending pathological fracture needs prophylactic fixation - use intramedullary nails for long bones
- “Spinal cord compression is an emergency - dexamethasone, radiotherapy, and consider surgery
Must know CRAB backwards and forwards. This defines symptomatic myeloma requiring treatment. Without CRAB features, patient has smoldering myeloma and only needs observation.
Purely osteolytic lesions with NO sclerosis. This is pathognomonic - osteoblasts are inhibited by DKK1 and sclerostin from myeloma cells. Healing or sclerotic lesions suggest metastases instead.
Fix impending and actual pathological fractures. Use intramedullary devices for long bones. Mirels score over 8 indicates prophylactic fixation. Vertebroplasty for painful compression fractures.
All patients with bone disease need bisphosphonates. Reduces skeletal events by 40%. Beware osteonecrosis of jaw - dental clearance before starting. Hold before surgery.
Overview and Epidemiology
Multiple myeloma is a malignant neoplasm of plasma cells characterized by clonal proliferation in the bone marrow, production of monoclonal immunoglobulin (M-protein), and end-organ damage. It accounts for approximately 1-2% of all cancers and represents the most common primary malignancy of bone in adults over 40 years of age.
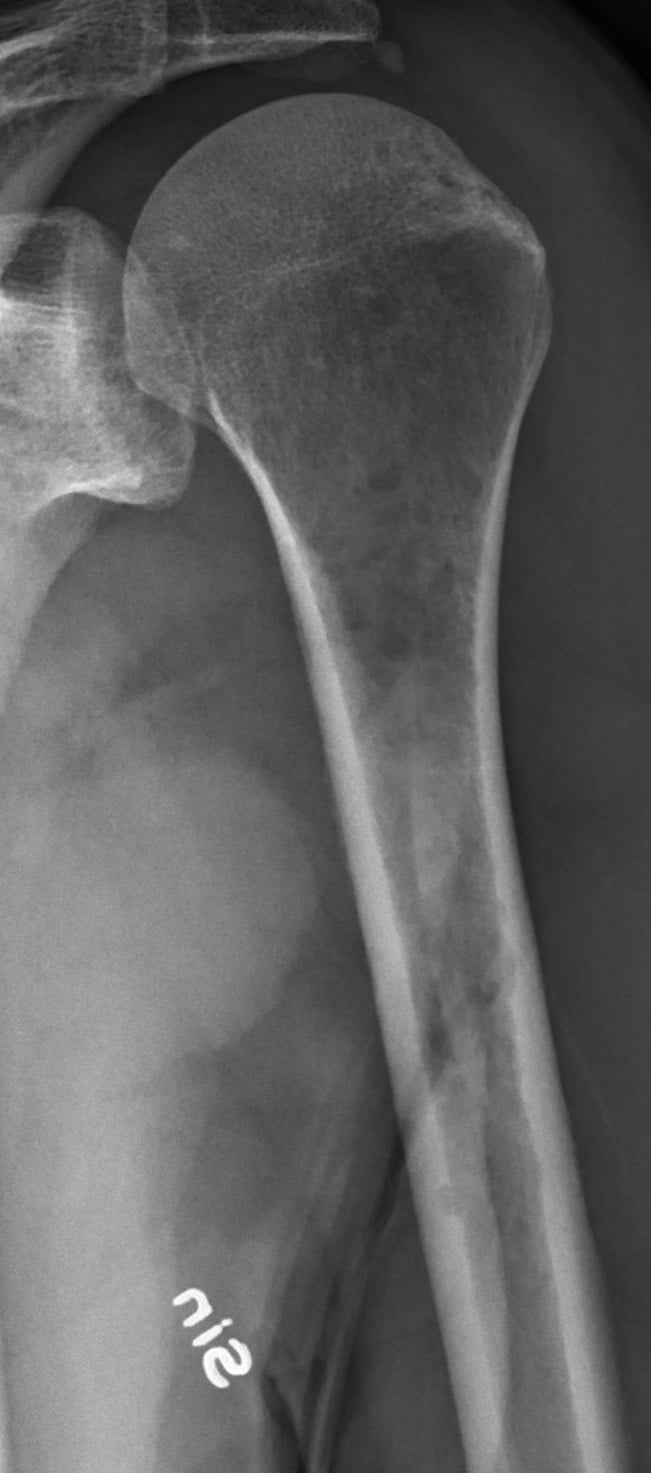
Skeletal involvement occurs in 90% of patients and is often the presenting feature. Patients present with pathological fractures, severe bone pain, or spinal cord compression. Orthopaedic surgeons must recognize the characteristic punched-out lytic lesions without sclerotic response and understand when surgical intervention is indicated. Bisphosphonate therapy is critical to prevent skeletal complications.
- Median age: 65 years at diagnosis
- Rare under 40: Only 2% of cases
- Gender: Slight male predominance (1.4:1)
- Ethnicity: 2-fold higher in African populations
- Incidence: 4-6 per 100,000 per year
- Vertebral column: 70% (most common site)
- Ribs: 50%
- Skull: 40% (classic "punched-out" lesions)
- Pelvis: 30%
- Proximal long bones: Femur and humerus 25%
- Distal skeleton: Rarely involved
Risk Factors and Precursor Conditions
- M-protein under 30 g/L
- Bone marrow plasma cells under 10%
- No CRAB features
- Progresses to myeloma at 1% per year
- Requires annual monitoring
- M-protein 30 g/L or higher OR bone marrow plasma cells 10-60%
- No CRAB features (key distinction)
- Progresses to symptomatic myeloma at 10% per year in first 5 years
- Observation only - do not treat
- One or more CRAB criteria present
- OR malignant biomarkers: Bone marrow plasma cells over 60%, serum free light chain ratio over 100, or over 1 focal lesion on MRI
- Requires chemotherapy and supportive care
Orthopaedic Management and Surgical Indications
Principles of Orthopaedic Management
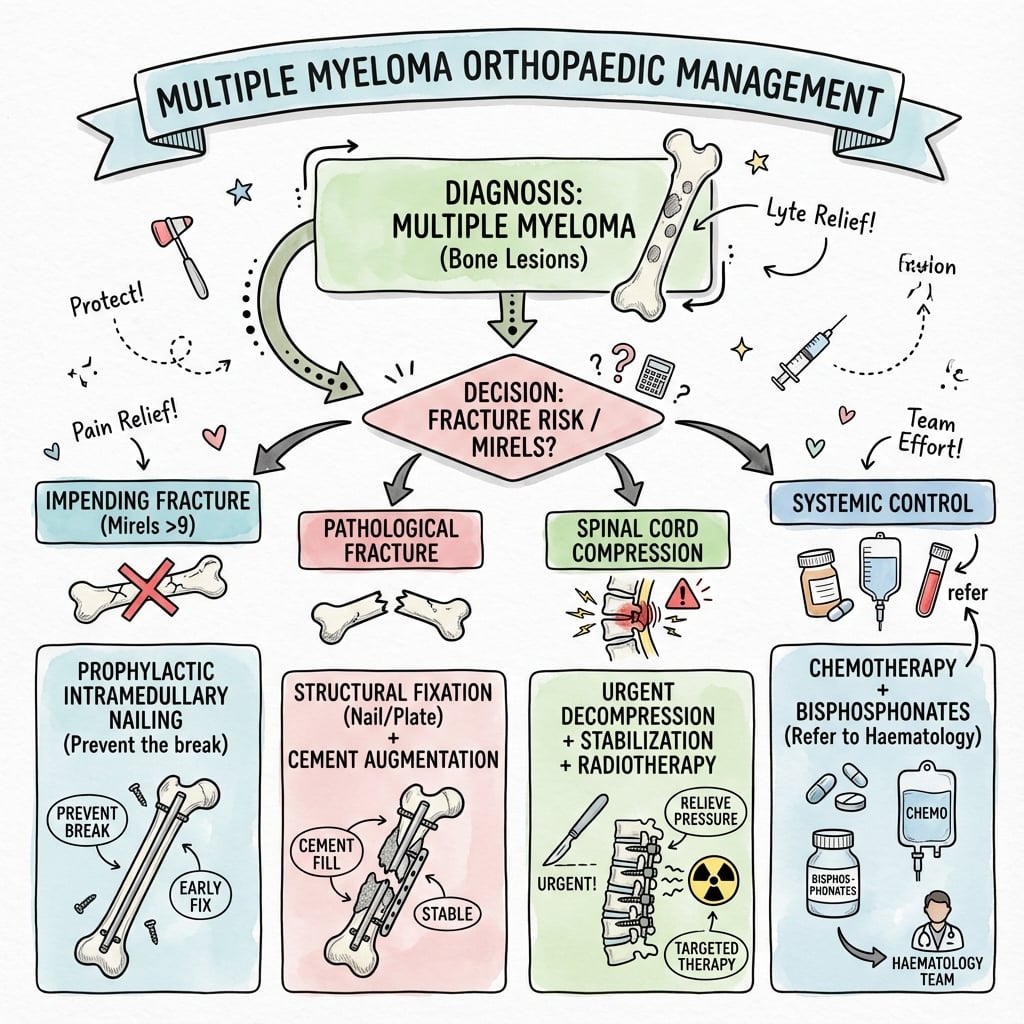
Myeloma is a systemic disease requiring systemic treatment. Surgery is palliative and aims to:
- Stabilize actual or impending pathological fractures to restore function
- Decompress neural structures in spinal cord compression
- Provide pain relief through stabilization or vertebroplasty/kyphoplasty
- Improve quality of life by restoring mobility and independence
Surgery alone NEVER cures myeloma - chemotherapy is essential for disease control.
Impending Pathological Fracture Assessment
- 1 Point
- Upper limb
- 2 Points
- Lower limb
- 3 Points
- Peritrochanteric
- 1 Point
- Mild
- 2 Points
- Moderate
- 3 Points
- Functional (severe)
- 1 Point
- Blastic
- 2 Points
- Mixed
- 3 Points
- Lytic
- 1 Point
- Less than 1/3 diameter
- 2 Points
- 1/3 to 2/3 diameter
- 3 Points
- Over 2/3 diameter
Interpretation:
- Score ≤7: Low fracture risk - observation, bisphosphonates, radiotherapy if painful
- Score 8: Intermediate risk - consider prophylactic fixation
- Score ≥9: High fracture risk - prophylactic fixation indicated
Mirels scoring was developed for metastatic disease, but myeloma lesions have NO sclerotic response and may be at higher fracture risk than the score suggests. Cortical destruction over 50% or lesion over 3cm in long bone should prompt strong consideration of prophylactic fixation regardless of score.
Long Bone Pathological Fractures
Surgical Technique for Long Bone Fractures
Surgical Principles
Intramedullary nailing preferred over plate fixation for:
- Load sharing vs load bearing
- Protection of entire bone including skip lesions
- Lower reoperation rate with progression
- Allows early weight-bearing
Long segment fixation:
- Protect entire bone at risk
- Assume disease may progress
- Bridge all lytic lesions
- Use locked interlocking screws
PMMA cement indicated for:
- Large segmental defects
- Periarticular fractures
- Adjunct to intramedullary nails
- Immediate pain relief and stability
Consider postoperative RT:
- Local disease control
- Pain management
- Timing: 2-3 weeks post-op (allow wound healing)
- Typical dose: 20-30 Gy in 5-10 fractions
Femur Fractures - Specific Considerations
- Long cephalomedullary nail (e.g., long Gamma nail, trochanteric femoral nail)
- Protect entire femur down to supracondylar region
- Consider cemented hip arthroplasty if extensive femoral head/neck involvement
- Long antegrade intramedullary nail
- Protect from subtrochanteric to supracondylar region
- Ream if cortical destruction significant
- Static locking proximally and distally
- Retrograde intramedullary nail OR lateral locked plate
- Cement augmentation of screw holes
- Consider distal femoral replacement if extensive metaphyseal involvement
Humerus Fractures
- Antegrade humeral nail OR shoulder hemiarthroplasty/reverse shoulder arthroplasty
- Arthroplasty preferred if extensive humoral head destruction or elderly patient
- Antegrade humeral nail preferred
- Alternative: Plate fixation if radial nerve concern or very distal lesion
- Protect full length of diaphysis
This completes the long bone surgical principles section.
Spinal Involvement and Cord Compression
Spinal cord compression is an orthopaedic and oncological EMERGENCY. Prognosis depends on neurological status at treatment initiation - patients who lose ambulation rarely regain it. Immediate dexamethasone 10mg IV, MRI whole spine, and urgent oncology consultation are mandatory.
- Back pain (95%) - often first symptom
- Motor weakness (75%) - lower extremity weakness
- Sensory changes (50%) - numbness, paresthesias
- Bladder/bowel dysfunction (40%) - late finding, poor prognosis
- Cauda equina syndrome - saddle anesthesia, urinary retention
- MRI whole spine - gold standard
- Identifies level(s) of compression
- Assesses spinal stability
- Detects multiple levels (30% have multiple sites)
- STIR sequence best for edema/disease
- Spinal Stability
- Stable spine
- Treatment
- Dexamethasone + radiotherapy + bisphosphonates + chemotherapy
- Prognosis for Ambulation
- Over 90% maintain ambulation
- Spinal Stability
- Unstable spine
- Treatment
- Posterior stabilization + decompression, then radiotherapy
- Prognosis for Ambulation
- Over 90% maintain ambulation
- Spinal Stability
- Stable or unstable
- Treatment
- Dexamethasone + URGENT radiotherapy OR surgery if unstable + chemotherapy
- Prognosis for Ambulation
- 60-80% maintain/regain ambulation
- Spinal Stability
- Any stability
- Treatment
- Dexamethasone + EMERGENCY surgery (decompression + stabilization) + radiotherapy
- Prognosis for Ambulation
- 40-60% regain ambulation
- Spinal Stability
- Any stability
- Treatment
- Dexamethasone + radiotherapy (surgery unlikely to help) + chemotherapy
- Prognosis for Ambulation
- Under 20% regain ambulation
Vertebroplasty and Kyphoplasty
- Painful vertebral compression fractures
- Failed conservative management (analgesia, bracing)
- No spinal cord compression
- Fracture under 3 months old (better outcomes)
- Vertebral body height over 33% preserved
- Spinal cord compression
- Posterior vertebral wall disruption
- Infection (osteomyelitis, discitis)
- Uncorrectable coagulopathy
- Extensive vertebral collapse (under 33% height)
- Vertebroplasty
- Direct PMMA injection into vertebral body
- Kyphoplasty
- Balloon inflation to create cavity, then PMMA injection
- Vertebroplasty
- Minimal (10-20%)
- Kyphoplasty
- Moderate (30-40%)
- Vertebroplasty
- 10-15% (higher)
- Kyphoplasty
- 5-7% (lower)
- Vertebroplasty
- 75-85% achieve significant relief
- Kyphoplasty
- 80-90% achieve significant relief
- Vertebroplasty
- Lower
- Kyphoplasty
- Higher (balloon equipment)
- Vertebroplasty
- 30-45 minutes
- Kyphoplasty
- 60-90 minutes
Outcomes:
- Pain relief: 75-90% of patients achieve significant improvement within 24-48 hours
- Functional improvement: Reduced analgesic requirements, improved mobility
- Durability: Pain relief sustained in 80% at 1 year
- Cement leakage: Usually asymptomatic, rarely causes neural compression (under 1%)
Pathophysiology and Skeletal Mechanisms
Plasma Cell Biology and Bone Destruction
Multiple myeloma represents a clonal proliferation of malignant plasma cells in the bone marrow. These cells produce excessive amounts of monoclonal immunoglobulin (M-protein), which can be detected in serum and urine. The characteristic skeletal manifestations result from profound disruption of normal bone remodeling.
Myeloma cells secrete RANKL (receptor activator of nuclear factor kappa-B ligand) which dramatically increases osteoclast activity. This drives bone resorption and creates lytic lesions. Additionally, decreased OPG (osteoprotegerin) removes the natural brake on osteoclast function.
Myeloma cells produce DKK1 and sclerostin which inhibit the Wnt signaling pathway essential for osteoblast function. This explains why myeloma lesions show NO sclerotic or healing response - osteoblasts cannot form new bone.
IL-6, IL-1, and TNF-alpha are overproduced, promoting myeloma cell growth and survival while further stimulating bone resorption. These cytokines also contribute to systemic symptoms like fatigue and weight loss.
VEGF production by myeloma cells promotes new blood vessel formation in the bone marrow microenvironment, supporting tumor growth and creating the vascular network seen on MRI.
Why Lesions Are Purely Lytic
The absence of any sclerotic or blastic response in myeloma bone lesions is pathognomonic and distinguishes myeloma from metastatic carcinoma. This occurs because:
- DKK1 and sclerostin from myeloma cells completely suppress osteoblast differentiation and function
- Even with successful chemotherapy, lesions rarely show healing or sclerosis
- Any sclerotic change in a presumed myeloma lesion should prompt reconsideration of the diagnosis
Classification
Multiple myeloma is classified based on:
- Smoldering (asymptomatic) myeloma: M-protein or clonal plasma cells present without CRAB features
- Symptomatic myeloma: Presence of CRAB features or myeloma-defining biomarkers
- IgG myeloma (most common, 50-55%)
- IgA myeloma (20-25%)
- Light chain only (Bence Jones, 15-20%)
- IgD, IgE, or non-secretory (rare)
- Standard risk cytogenetics
- High-risk cytogenetics: del(17p), t(4;14), t(14;16), gain 1q
See "Classification and Staging" section below for detailed ISS and R-ISS staging systems.
Classification and Staging
International Staging System (ISS)
- Criteria
- Beta-2 microglobulin under 3.5 mg/L AND albumin 35 g/L or higher
- Median Survival
- 62 months
- Frequency
- 30% of patients
- Criteria
- Neither Stage I nor Stage III
- Median Survival
- 44 months
- Frequency
- 40% of patients
- Criteria
- Beta-2 microglobulin 5.5 mg/L or higher
- Median Survival
- 29 months
- Frequency
- 30% of patients
Revised International Staging System (R-ISS)
The R-ISS incorporates ISS stage plus LDH and high-risk cytogenetics for improved prognostication.
- Criteria
- ISS Stage I AND standard-risk cytogenetics AND normal LDH
- 5-Year Survival
- 82%
- Clinical Implication
- Excellent prognosis - may defer treatment in smoldering myeloma
- Criteria
- Not R-ISS I or III
- 5-Year Survival
- 62%
- Clinical Implication
- Intermediate prognosis - standard treatment approach
- Criteria
- ISS Stage III AND (high-risk cytogenetics OR elevated LDH)
- 5-Year Survival
- 40%
- Clinical Implication
- Poor prognosis - consider novel agents and early transplant
High-Risk Cytogenetics
Detected by FISH on bone marrow plasma cells:
- del(17p) - TP53 deletion - worst prognosis
- t(4;14) - FGFR3/MMSET translocation - high risk
- t(14;16) - MAF translocation - high risk
- Gain 1q - chromosome 1q gain/amplification - adverse
- del(13) - Chromosome 13 deletion - adverse when detected by conventional cytogenetics
Unlike other hematological malignancies, myeloma plasma cells often have low mitotic index, making conventional karyotyping difficult. FISH (fluorescence in situ hybridization) is essential to detect high-risk translocations and deletions. Presence of del(17p) or t(4;14) indicates aggressive disease requiring intensive treatment.
Clinical Presentation and CRAB Criteria
Presenting Symptoms
Most patients present with one or more symptoms related to skeletal involvement or systemic effects of plasma cell proliferation.
- Bone pain: Persistent, often in back or chest
- Pathological fractures: Minimal trauma fractures
- Height loss: From vertebral compression fractures
- Spinal cord compression: Emergency presentation
- Fatigue and weakness: From anemia
- Recurrent infections: Hypogammaglobulinemia
- Weight loss: Cachexia from tumor burden
- Bleeding tendency: Hyperviscosity syndrome (rare)
- Renal insufficiency: Light chain cast nephropathy
- Dehydration: Hypercalcemia-induced
- Amyloidosis: AL amyloid deposition (10-15%)
- Tubular dysfunction: Fanconi syndrome
CRAB Criteria in Detail
CRAB criteria define symptomatic myeloma requiring treatment. The presence of ANY ONE CRAB feature (or myeloma-defining biomarker) mandates initiation of chemotherapy. Without CRAB features, patients have smoldering myeloma and should NOT be treated.
- Definition
- Serum calcium over 2.75 mmol/L (or corrected calcium over 2.75 mmol/L or ionized calcium over 1.30 mmol/L)
- Pathophysiology
- Osteoclast-mediated bone resorption releases calcium; renal insufficiency impairs calcium excretion
- Management
- Aggressive IV hydration (3-4L per day), bisphosphonates (zoledronic acid), calcitonin if severe, treat underlying myeloma
- Definition
- Creatinine clearance under 40 mL/min or creatinine over 173 micromol/L (over 2 mg/dL)
- Pathophysiology
- Light chain cast nephropathy (myeloma kidney), hypercalcemia, dehydration, nephrotoxic drugs
- Management
- Hydration, treat hypercalcemia, avoid NSAIDs and contrast, dialysis if needed, chemotherapy to reduce light chains
- Definition
- Hemoglobin under 100 g/L (under 10 g/dL) or over 20 g/L below normal
- Pathophysiology
- Bone marrow infiltration by plasma cells suppresses normal hematopoiesis; renal insufficiency decreases EPO
- Management
- Transfusion if symptomatic, erythropoietin, treat underlying myeloma to restore marrow function
- Definition
- One or more osteolytic lesions on skeletal survey, CT, or PET-CT
- Pathophysiology
- RANKL-mediated osteoclast activation plus DKK1/sclerostin-mediated osteoblast suppression creates purely lytic lesions
- Management
- Bisphosphonates (zoledronic acid or pamidronate monthly), fixation for fractures/impending fractures, vertebroplasty for painful VCFs
Myeloma-Defining Biomarkers (SLiM Criteria)
In addition to CRAB, the following biomarkers define symptomatic myeloma even in the absence of CRAB features:
- 60 or more percent clonal plasma cells on bone marrow biopsy
- Light chain ratio 100 or higher (involved/uninvolved free light chain ratio)
- MRI with more than 1 focal lesion at least 5mm in size
These "SLiM" criteria allow earlier treatment initiation in high-risk patients before end-organ damage occurs.
Hyperviscosity Syndrome
Among the presenting features the topic lists hyperviscosity as a rare cause of bleeding. It is worth developing because, unlike most myeloma complications, it is a treatable emergency with a specific intervention.
- Detail
- A high circulating monoclonal protein raises serum viscosity and impairs the microcirculation; more likely with IgA (which polymerises) and with IgM (Waldenstrom macroglobulinaemia) than with typical IgG myeloma, but possible at very high paraprotein levels
- Detail
- Mucosal/spontaneous bleeding (epistaxis, gum bleeding), visual disturbance (blurring; engorged 'sausage-shaped' retinal veins and haemorrhages on fundoscopy) and neurological symptoms (headache, dizziness, confusion, drowsiness; rarely seizure or stroke); volume overload may cause dyspnoea
- Detail
- Measured serum viscosity (symptoms usually appear above about 4 centipoise; normal relative viscosity is roughly 1.4 to 1.8) together with fundoscopy
- Detail
- Plasmapheresis (plasma exchange) for rapid paraprotein removal and immediate symptom relief, alongside systemic anti-myeloma therapy for durable control; avoid red-cell transfusion before plasmapheresis as it can further raise viscosity
Hyperviscosity is the myeloma complication treated by plasmapheresis. Suspect it with the triad of mucosal bleeding, visual disturbance (engorged retinal veins on fundoscopy) and neurological symptoms in a patient with a very high paraprotein - it is commoner with IgA and IgM (Waldenstrom) than with IgG. Plasma exchange rapidly lowers viscosity while anti-myeloma therapy treats the cause; do not transfuse a hyperviscous patient before exchange.
Myeloma Kidney: Cast Nephropathy and Acute Kidney Injury
Renal impairment is the "R" of CRAB, and the topic names light-chain cast nephropathy as its cause. The management deserves development because the renal injury is potentially reversible if treated early, and it directly shapes perioperative care.
- Detail
- Filtered monoclonal free light chains precipitate with Tamm-Horsfall protein (uromodulin) in the distal tubules, forming obstructing casts - the commonest cause of renal failure in myeloma
- Detail
- Light-chain deposition disease, AL amyloidosis, hypercalcaemic nephropathy and dehydration also contribute
- Detail
- Hypercalcaemia, dehydration and nephrotoxins - especially NSAIDs and iodinated contrast (also aminoglycosides) - must be stopped or avoided
- Detail
- Aggressive hydration, correct hypercalcaemia, stop nephrotoxins, and - the key step - rapidly reduce the toxic light chains with bortezomib-based anti-myeloma therapy; dialysis if required. Extracorporeal light-chain removal (plasma exchange or high-cut-off haemodialysis) has not shown a clear renal-recovery benefit and is not standard
Cast nephropathy from precipitated free light chains is the usual cause of renal failure in myeloma, and it is potentially reversible if the light chains are reduced quickly (bortezomib-based therapy) and precipitants are removed. For the orthopaedic surgeon this means avoiding iodinated contrast and NSAIDs, maintaining hydration, correcting hypercalcaemia, and adjusting drug and anaesthetic dosing; in renal impairment, denosumab is preferred over a bisphosphonate for bone protection.
Investigations

Laboratory Investigations
- Purpose
- Detect and quantify M-protein
- Typical Finding in Myeloma
- Monoclonal spike in gamma region (70% IgG, 20% IgA)
- Clinical Significance
- Diagnostic - quantifies disease burden; M-protein level correlates with tumor mass
- Purpose
- Detect Bence Jones protein
- Typical Finding in Myeloma
- Monoclonal light chains (kappa or lambda)
- Clinical Significance
- Present in 75% - indicates light chain production; nephrotoxic
- Purpose
- Quantify free light chains
- Typical Finding in Myeloma
- Elevated involved FLC; abnormal kappa/lambda ratio
- Clinical Significance
- More sensitive than UPEP; useful for monitoring non-secretory myeloma
- Purpose
- Confirm clonal plasma cells
- Typical Finding in Myeloma
- Over 10% clonal plasma cells; often 30-90%
- Clinical Significance
- Diagnostic gold standard - required for diagnosis
- Purpose
- Assess cytopenias
- Typical Finding in Myeloma
- Anemia common (Hb under 100 g/L); leukopenia and thrombocytopenia in advanced disease
- Clinical Significance
- Monitors CRAB criteria (anemia); assesses bone marrow reserve
- Purpose
- Assess renal impairment
- Typical Finding in Myeloma
- Elevated creatinine over 173 micromol/L in 25%
- Clinical Significance
- Monitors CRAB criteria (renal); impacts chemotherapy dosing
- Purpose
- Detect hypercalcemia
- Typical Finding in Myeloma
- Elevated over 2.75 mmol/L in 20-30%
- Clinical Significance
- Monitors CRAB criteria (calcium); emergency if severe
- Purpose
- Prognostic marker
- Typical Finding in Myeloma
- Elevated in advanced disease
- Clinical Significance
- Part of ISS staging - higher levels = worse prognosis
- Purpose
- Prognostic marker
- Typical Finding in Myeloma
- Low in advanced disease
- Clinical Significance
- Part of ISS staging - lower levels = worse prognosis
- Purpose
- Tumor burden marker
- Typical Finding in Myeloma
- Elevated in high tumor burden
- Clinical Significance
- Part of revised ISS (R-ISS); indicates aggressive disease
Imaging Investigations
- Sensitivity
- 40-50% (low)
- Advantages
- Widely available; low cost; traditional standard
- Disadvantages
- Misses early lesions; requires 30-50% bone loss to visualize; radiation exposure
- Clinical Use
- Initial screening; shows classic punched-out lesions; useful for fracture assessment
- Sensitivity
- 90% (very high)
- Advantages
- Most sensitive for bone marrow involvement; no radiation; detects early focal lesions
- Disadvantages
- Expensive; time-consuming; not widely available; claustrophobia
- Clinical Use
- Preferred first-line imaging; detects disease before skeletal survey positive
- Sensitivity
- 85-90% (high)
- Advantages
- Detects metabolically active disease; whole-body assessment; useful for monitoring response
- Disadvantages
- Radiation exposure; expensive; false negatives in low-grade disease
- Clinical Use
- Alternative to MRI; excellent for assessing treatment response and detecting extramedullary disease
- Sensitivity
- 70-80% (moderate-high)
- Advantages
- Better than X-ray; detects smaller lesions; fast acquisition
- Disadvantages
- Radiation exposure; less sensitive than MRI/PET-CT for marrow disease
- Clinical Use
- Alternative when MRI unavailable; good for cortical bone assessment and surgical planning
Technetium-99m bone scans are NOT useful in myeloma because they rely on osteoblastic activity to show uptake. Since myeloma lesions are purely osteolytic with suppressed osteoblast function, bone scans are typically negative or show decreased uptake ("cold spots"). This is the opposite of metastatic disease, which usually shows "hot spots" of increased uptake.
Radiographic Features
"Punched-out" lesions: Multiple well-defined, round lytic lesions with sharp margins and no sclerotic rim. Classic "moth-eaten" or "Swiss cheese" appearance. Most visible in lateral skull X-ray.
Vertebral compression fractures: Often multiple levels. Diffuse osteopenia. Vertebral body collapse creating "coin-on-edge" appearance. Posterior elements usually spared (unlike metastases).
Multiple lytic lesions: Involvement of ilium, pubis, and ischium. May cause pathological fractures. Pelvic insufficiency fractures in osteopenic bone.
Proximal involvement: Preferentially affects proximal femur and humerus (red marrow sites). Endosteal scalloping. Risk of pathological fracture with cortical destruction over 50%.
Diagnostic Criteria (IMWG 2014)
Multiple myeloma diagnosis requires:
-
Clonal bone marrow plasma cells ≥10% OR biopsy-proven plasmacytoma
PLUS
-
One or more of the following:
- CRAB features (any one of: Calcium elevated, Renal insufficiency, Anemia, Bone lesions)
- OR Myeloma-defining biomarkers (any one of: 60% or more clonal plasma cells, serum FLC ratio 100 or higher, over 1 focal MRI lesion)
Management Algorithm
Treatment Approach by Disease Status
- No CRAB criteria and no myeloma-defining biomarkers
- Close monitoring every 3-6 months
- Repeat SPEP, free light chains, imaging
- Do NOT treat - observation superior to early treatment in trials
- Treat only when progression to symptomatic myeloma
- Induction chemotherapy: Bortezomib + lenalidomide + dexamethasone (VRd) for 4-6 cycles
- Autologous stem cell transplant: High-dose melphalan followed by stem cell rescue
- Maintenance therapy: Lenalidomide continued until progression
- Bisphosphonates: Zoledronic acid or pamidronate monthly
- Median progression-free survival: 50+ months
- Induction chemotherapy: VRd or daratumumab + lenalidomide + dexamethasone (DRd)
- Continue until disease progression or intolerance
- Bisphosphonates: Zoledronic acid or pamidronate monthly
- Median overall survival: 4-5 years
- Second-line agents: Carfilzomib, ixazomib, daratumumab, elotuzumab, pomalidomide
- CAR T-cell therapy (ide-cel, cilta-cel) for heavily pretreated patients
- Clinical trials
- Palliation and supportive care
Key Drug Classes
Bortezomib, carfilzomib, ixazomib
- Inhibit protein degradation causing myeloma cell apoptosis
- Backbone of most regimens
- Side effects: Peripheral neuropathy, thrombocytopenia
Lenalidomide, pomalidomide, thalidomide
- Immune modulation and anti-angiogenic effects
- Highly effective in combination regimens
- Side effects: Thrombosis (require anticoagulation), neuropathy, teratogenicity
Daratumumab, isatuximab, elotuzumab
- Target CD38 or SLAMF7 on myeloma cells
- Dramatic responses in combination therapy
- Side effects: Infusion reactions, infections, cytopenias
Dexamethasone, prednisone
- Direct anti-myeloma effect and anti-inflammatory
- Used in all regimens
- Side effects: Hyperglycemia, insomnia, AVN, infections
Bisphosphonate Therapy - Essential for Skeletal Protection
ALL patients with myeloma bone disease should receive bisphosphonates. This is a class I recommendation based on randomized trials showing 40% reduction in skeletal-related events (pathological fractures, spinal cord compression, need for radiotherapy or surgery).
- Dosing
- 4mg IV over 15 minutes every 4 weeks
- Advantages
- Most potent bisphosphonate; convenient monthly dosing
- Precautions
- Requires renal dose adjustment if CrCl under 60; risk of ONJ; hold before dental procedures
- Dosing
- 90mg IV over 2-4 hours every 4 weeks
- Advantages
- Alternative if renal impairment
- Precautions
- Longer infusion time; less potent than zoledronic acid; risk of ONJ
- Dosing
- 120mg SubQ every 4 weeks
- Advantages
- Can use in renal failure; no dose adjustment needed
- Precautions
- Higher risk of hypocalcemia; ensure calcium/vitamin D supplementation; risk of ONJ
Duration: Continue monthly for first 2 years, then consider reducing to every 3 months if complete response achieved.
Osteonecrosis of Jaw (ONJ) Prevention:
- Dental examination and clearance before starting bisphosphonates
- Maintain excellent oral hygiene
- Avoid invasive dental procedures while on therapy
- If dental surgery required, hold bisphosphonates for 2-3 months before and after
- Risk increases with duration of therapy (cumulative effect)
Prognosis and Survival
Overall Survival by Era
Survival in myeloma has improved dramatically over the past two decades with the introduction of novel agents (proteasome inhibitors, immunomodulatory drugs, monoclonal antibodies) and autologous stem cell transplantation.
Prognostic Factors
- Favorable Prognosis
- Under 65 years
- Adverse Prognosis
- Over 75 years
- Favorable Prognosis
- Stage I (beta-2M under 3.5, albumin 35 or higher)
- Adverse Prognosis
- Stage III (beta-2M over 5.5)
- Favorable Prognosis
- Standard-risk: t(11;14), hyperdiploidy
- Adverse Prognosis
- High-risk: del(17p), t(4;14), t(14;16), gain 1q
- Favorable Prognosis
- Normal
- Adverse Prognosis
- Elevated
- Favorable Prognosis
- Complete response or better
- Adverse Prognosis
- Stable disease or progressive disease
- Favorable Prognosis
- Creatinine under 173 micromol/L
- Adverse Prognosis
- Creatinine over 173 micromol/L or dialysis-dependent
- Favorable Prognosis
- ECOG 0-1 (fully active)
- Adverse Prognosis
- ECOG 3-4 (limited self-care)
- Favorable Prognosis
- No fractures, limited lytic lesions
- Adverse Prognosis
- Multiple pathological fractures, extensive lytic disease
Survival by R-ISS Stage (Contemporary Data)
- 5-Year OS
- 82%
- Median PFS
- 66 months
- Median OS
- Not reached (over 10 years)
- 5-Year OS
- 62%
- Median PFS
- 42 months
- Median OS
- 83 months
- 5-Year OS
- 40%
- Median PFS
- 29 months
- Median OS
- 43 months
OS = Overall Survival; PFS = Progression-Free Survival
MRC Myeloma IX: Zoledronic Acid vs Clodronic Acid
VISTA Trial: Bortezomib in Newly Diagnosed Myeloma
Bisphosphonates in Multiple Myeloma: Cochrane Network Meta-Analysis
IMWG Updated Diagnostic Criteria for Multiple Myeloma
Revised International Staging System (R-ISS)
Guidelines, Registries & Global Practice
Global Epidemiology
According to the Global Burden of Disease Study 2016 (Cowan et al., JAMA Oncology 2018), there were approximately 138,500 incident cases of multiple myeloma worldwide in 2016, with an age-standardised incidence rate of 2.1 per 100,000 persons. Incident cases rose by 126% between 1990 and 2016, driven by population growth and ageing. Incidence is highly variable geographically, being highest in Australasia, North America and Western Europe, and substantially higher (approximately two-fold) in populations of African ancestry. Access to autologous stem-cell transplantation and to novel agents (lenalidomide, bortezomib) is concentrated in high-income regions and remains very limited in sub-Saharan Africa and parts of the Middle East.
- Finding
- Approximately 138,500 new cases; age-standardised rate 2.1 per 100,000
- Source / Evidence
- GBD 2016 (Cowan, JAMA Oncol 2018, PMID 29800065)
- Finding
- 126% rise in incident cases (largest increase in low and middle SDI countries)
- Source / Evidence
- GBD 2016 (PMID 29800065)
- Finding
- Australasia, North America, Western Europe; two-fold higher in African-ancestry populations
- Source / Evidence
- GBD 2016 (PMID 29800065)
- Finding
- Routine in high-income regions; under 5% utilisation in Africa/East Mediterranean
- Source / Evidence
- WBMT/GBD analysis (Cowan, Biol Blood Marrow Transplant 2020, PMID 32846200)
Guideline Comparison Across Jurisdictions
- Diagnostic Framework
- CRAB plus SLiM biomarkers (clonal plasma cells 60% or more, FLC ratio 100 or higher, more than 1 focal MRI lesion)
- First-line Imaging
- Whole-body low-dose CT, whole-body MRI or PET-CT preferred over skeletal survey
- Bone-Directed Therapy
- Zoledronic acid or pamidronate for all with bone disease; denosumab if renal impairment
- Evidence Level
- Level I (Rajkumar, Lancet Oncol 2014, PMID 25439696)
- Diagnostic Framework
- Adopts IMWG criteria
- First-line Imaging
- Whole-body MRI first-line; whole-body low-dose CT if MRI unsuitable; avoid isolated skeletal survey
- Bone-Directed Therapy
- Zoledronic acid offered to all (survival and SRE benefit); bisphosphonate continued
- Evidence Level
- Level I (informed by MRC Myeloma IX, PMID 21131037)
- Diagnostic Framework
- IMWG criteria; R-ISS for staging
- First-line Imaging
- Whole-body low-dose CT or PET-CT; MRI for suspected cord compression or smouldering disease
- Bone-Directed Therapy
- Zoledronic acid preferred; denosumab non-inferior alternative, useful in renal impairment
- Evidence Level
- Level I (Dimopoulos, Ann Oncol 2021)
- Diagnostic Framework
- IMWG criteria; R-ISS staging
- First-line Imaging
- Whole-body low-dose CT, PET-CT or MRI; skeletal survey only if advanced imaging unavailable
- Bone-Directed Therapy
- Bisphosphonate (zoledronic acid/pamidronate) or denosumab for all with bone disease
- Evidence Level
- Level I
There is strong international consensus across IMWG, NICE, EHA-ESMO and NCCN: diagnosis follows the CRAB-plus-SLiM framework, cross-sectional imaging (whole-body low-dose CT, whole-body MRI or PET-CT) has replaced the plain skeletal survey, and a bisphosphonate (preferably zoledronic acid) is offered to every patient with bone disease. The principal practice variation is access-driven, not evidence-driven: transplant and novel-agent availability diverge sharply between high-income and low/middle-income countries.
Registry Evidence
Large national and international registries (the US SEER programme, the European EBMT/WBMT transplant registries and the Australian Myeloma and Related Diseases Registry) document a substantial improvement in survival over the past two decades, coinciding with the introduction of proteasome inhibitors, immunomodulatory drugs, monoclonal antibodies and routine autologous transplantation. Registry data also confirm marked global disparities in access to autologous transplantation, with utilisation below 5% of incident cases in Africa and the East Mediterranean compared with over 20% in North America and Europe (Cowan et al., Biol Blood Marrow Transplant 2020).
Supportive Care and Prophylaxis
International consensus (IMWG, NCCN, EHA-ESMO) supports the following supportive-care measures for patients on multi-agent myeloma therapy:
- Pneumocystis jirovecii prophylaxis: trimethoprim-sulfamethoxazole for patients on high-dose corticosteroids or bortezomib-based regimens
- Herpes-zoster prophylaxis: aciclovir or valaciclovir during and after bortezomib-based therapy (reactivation risk)
- Venous thromboembolism prophylaxis during immunomodulatory therapy (lenalidomide, pomalidomide, thalidomide): aspirin for standard-risk patients; low-molecular-weight heparin or a direct oral anticoagulant (e.g. apixaban, rivaroxaban) for high-risk patients
MCQ Practice Points
Q: What is the characteristic radiographic appearance of multiple myeloma bone lesions?
A: Punched-out lytic lesions without surrounding sclerosis or periosteal reaction. Most common in axial skeleton: spine, skull, pelvis, ribs, proximal femur/humerus. No bone scan uptake (purely osteolytic with suppressed osteoblasts) - use skeletal survey or whole-body MRI instead. Lesions represent replaced marrow.
Q: What laboratory findings are diagnostic for multiple myeloma?
A: CRAB criteria: Calcium elevation, Renal insufficiency, Anemia, Bone lesions. M-spike (monoclonal protein) on serum protein electrophoresis. Bence Jones proteinuria (light chains). Bone marrow with greater than 10% plasma cells. Rouleaux formation on blood smear. ESR markedly elevated. Normal ALP (osteoblasts suppressed).
Q: Why is the alkaline phosphatase (ALP) typically normal in multiple myeloma?
A: Myeloma cells produce osteoclast-activating factors (RANKL, IL-6, MIP-1α) causing bone resorption WITHOUT compensatory bone formation. Osteoblast activity suppressed by Dickkopf-1 (DKK1). Hence ALP (marker of osteoblastic activity) remains normal despite extensive bone destruction. Distinguishes from metastatic bone disease.
Q: What is the surgical approach to pathological fractures in multiple myeloma?
A: Prophylactic fixation for impending fractures (Mirels score ≥8). Internal fixation + cement augmentation for actual fractures. Avoid intramedullary devices alone in spine - tumor extends into canal. Spine: Vertebroplasty/kyphoplasty for compression fractures, decompression + stabilization for cord compression. Radiation post-operatively.
Q: What is the difference between multiple myeloma and solitary plasmacytoma?
A: Solitary plasmacytoma: Single bone or soft tissue lesion, normal bone marrow (less than 10% plasma cells), absent/minimal M-protein, no other CRAB features. Better prognosis - treat with radiation ± surgery. ~50% progress to multiple myeloma within 10 years. Multiple myeloma requires systemic chemotherapy and may require autologous stem cell transplant.
At a Glance
Multiple myeloma is a plasma cell malignancy causing purely lytic skeletal lesions (no blastic component). It presents with the "CRAB" criteria: Calcium elevation, Renal insufficiency, Anemia, Bone lesions. The spine and pelvis are most commonly affected. Unlike metastatic disease, bone scans are cold (no bone formation). Pathological fractures are common and require internal fixation (avoid arthroplasty at spine). All patients need bisphosphonates to reduce skeletal events. Key orthopaedic decision: stabilize prophylactically using Mirels' criteria, and cementation is preferred for rapid stability.
- Multiple Myeloma
- Purely lytic, punched-out, NO sclerosis
- Metastatic Disease
- Mixed lytic-blastic or purely blastic
- Osteoporosis
- Diffuse osteopenia, no focal lesions
- Multiple Myeloma
- M-protein spike on SPEP
- Metastatic Disease
- Normal protein electrophoresis
- Osteoporosis
- Normal protein electrophoresis
- Multiple Myeloma
- Over 10% clonal plasma cells
- Metastatic Disease
- Metastatic carcinoma cells
- Osteoporosis
- Normal marrow
- Multiple Myeloma
- Vertebrae, ribs, proximal femur/humerus
- Metastatic Disease
- Vertebrae, femur, pelvis
- Osteoporosis
- Vertebrae, distal radius, hip
- Multiple Myeloma
- Chemotherapy plus bisphosphonates
- Metastatic Disease
- Treat primary cancer plus targeted therapy
- Osteoporosis
- Bisphosphonates, calcium, vitamin D
CRABCRAB Criteria for Myeloma End-Organ Damage
Hook:When myeloma gets CRABBY, it needs treatment! Any one CRAB feature = symptomatic myeloma requiring chemotherapy.
BUMPSDiagnostic Workup for Suspected Myeloma
Hook:When you suspect myeloma, look for BUMPS - the diagnostic workup essentials!
SPINAL FRACTURESOrthopaedic Complications of Myeloma
Hook:Myeloma causes SPINAL FRACTURES - remember the skeletal complications requiring orthopaedic intervention!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man presents with 3 months of progressive back pain. Plain radiographs show multiple lytic lesions in the thoracolumbar spine with compression fractures at T8 and L2. How would you approach this patient?”
“A 72-year-old woman with known multiple myeloma on chemotherapy presents with acute onset right thigh pain after a fall at home. X-ray shows a complete subtrochanteric femur fracture through a 5cm lytic lesion. Her oncologist asks your advice on management. What would you recommend?”
“You are called to the emergency department at 2 AM. A 65-year-old man with newly diagnosed multiple myeloma (started chemotherapy 2 weeks ago) presents with 24 hours of progressive lower limb weakness and urinary retention. On examination, he has grade 3/5 power in both lower limbs, a sensory level at T10, and absent ankle reflexes. Walk me through your emergency management.”
Key Definition
- Plasma cell neoplasm with clonal bone marrow plasma cells over 10% PLUS CRAB criteria or myeloma-defining biomarkers
- Most common primary bone malignancy in adults over 40 years
- Median age 65 years; 90% have skeletal involvement
CRAB Criteria (Must Know)
- C - Calcium elevated over 2.75 mmol/L
- R - Renal insufficiency (creatinine over 173 micromol/L)
- A - Anemia (Hb under 100 g/L)
- B - Bone lesions (one or more lytic lesions)
- ANY ONE = symptomatic myeloma requiring treatment
Pathognomonic Radiology
- Purely LYTIC lesions with NO sclerotic response (vs metastases)
- Punched-out lesions in skull - classic appearance
- Vertebral compression fractures (70% involve spine)
- Whole-body MRI or PET-CT more sensitive than skeletal survey
- Bone scan NOT useful (no osteoblastic activity)
Diagnostic Triad
- 1. SPEP - monoclonal protein spike (70% IgG, 20% IgA)
- 2. Urine protein electrophoresis - Bence Jones protein (75%)
- 3. Bone marrow biopsy - over 10% clonal plasma cells
- PLUS: Serum free light chains, calcium, renal function, imaging
Staging (R-ISS Preferred)
- R-ISS I: ISS I + standard cytogenetics + normal LDH (82% 5yr survival)
- R-ISS II: Not I or III (62% 5yr survival)
- R-ISS III: ISS III + high-risk cytogenetics OR elevated LDH (40% 5yr survival)
- High-risk cytogenetics: del(17p), t(4;14), t(14;16), gain 1q
Medical Treatment
- Transplant eligible: VRd induction → ASCT → lenalidomide maintenance
- Transplant ineligible: VRd or DRd until progression
- ALL with bone disease: Bisphosphonates (zoledronic acid 4mg IV monthly)
- Bisphosphonates reduce SREs by 40%
- Beware ONJ - dental clearance before starting bisphosphonates
Surgical Indications
- Pathological fractures: Intramedullary nailing preferred (long nail, protect full bone)
- Impending fractures: Mirels over 8 or cortical destruction over 50%
- Spinal cord compression: Emergency decompression + stabilization if unstable spine
- Vertebroplasty/kyphoplasty: Painful VCFs, 75-90% pain relief
- Cement augmentation: Immediate stability for large defects
Surgical Principles
- Surgery is PALLIATIVE - chemotherapy is definitive treatment
- Intramedullary nail over plate (load-sharing, protects full bone, early weight-bearing)
- LONG fixation - protect entire bone (skip lesions and progression risk)
- Adjuvant radiotherapy: 20-30 Gy starting 2-3 weeks post-op
- Weight-bearing as tolerated - goal is quality of life
Spinal Cord Compression (Emergency)
- Dexamethasone 10mg IV IMMEDIATELY (within 30 min)
- MRI whole spine urgently (within 1 hour)
- Ambulatory at presentation = 60-80% preserve function
- Paraplegic over 48hrs = under 20% recover ambulation
- Surgery if unstable spine or bony compression; RT if soft tissue mass
Complications to Know
- SREs (skeletal-related events): fracture, RT, surgery, cord compression - 60-70% experience
- Hypercalcemia: IV hydration + bisphosphonates (response 48-72hrs)
- Renal failure: Light chain cast nephropathy - hydration, avoid NSAIDs, treat myeloma
- Infections: Hypogammaglobulinemia - leading cause of death early
- ONJ from bisphosphonates: 1-10% incidence, increases with duration
Prognosis
- Median survival: 8-10 years for standard-risk with modern therapy (was 3 years in 2000)
- R-ISS I: Median OS over 10 years (82% at 5 years)
- R-ISS III: Median OS 43 months (40% at 5 years)
- Causes of death: Progressive myeloma (40-50%), infection (25-30%), renal failure (10-15%)
Exam Day Pearls
- No blastic response = pathognomonic for myeloma (vs metastases which heal)
- CRAB backwards and forwards - defines symptomatic disease
- Smoldering myeloma (no CRAB) = DO NOT TREAT, only observe
- Bisphosphonates mandatory for ALL with bone disease
- Spinal cord compression = dexamethasone within 30 min, MRI within 1 hour, treatment within 24 hours
- Intramedullary nail over plate, long fixation over short, cement augmentation for large defects
References
-
Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
-
Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-e548.
-
Terpos E, Ntanasis-Stathopoulos I, Gavriatopoulou M, Dimopoulos MA. Pathogenesis of bone disease in multiple myeloma: from bench to bedside. Blood Cancer J. 2018;8(1):7.
-
Roodman GD. Pathogenesis of myeloma bone disease. Leukemia. 2009;23(3):435-441.
-
Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-2869.
-
Hillengass J, Usmani S, Rajkumar SV, et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019;20(6):e302-e312.
-
Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(3):309-322.
-
Moreau P, Kumar SK, San Miguel J, et al. Treatment of relapsed and refractory multiple myeloma: recommendations from the International Myeloma Working Group. Lancet Oncol. 2021;22(3):e105-e118.
-
Mhaskar R, Kumar A, Miladinovic B, Djulbegovic B. Bisphosphonates in multiple myeloma: an updated network meta-analysis. Cochrane Database Syst Rev. 2017;12(12):CD003188.
-
Terpos E, Kleber M, Engelhardt M, et al. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica. 2015;100(10):1254-1266.
-
Mirels H. Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res. 1989;(249):256-264.
-
Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366(9486):643-648.
-
Berenson JR, Lichtenstein A, Porter L, et al. Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. J Clin Oncol. 1998;16(2):593-602.
-
Morgan GJ, Davies FE, Gregory WM, et al. First-line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma (MRC Myeloma IX): a randomised controlled trial. Lancet. 2010;376(9757):1989-1999.
-
Kumar SK, Dispenzieri A, Lacy MQ, et al. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia. 2014;28(5):1122-1128.
-
Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol. 2020;95(5):548-567.