Forestier Disease | Mechanical Dysphagia from Anterior Osteophytes
- DISH (Forestier's Disease) is a systemic condition causing 'flowing wax' calcification of the ALL.
- OALL is the cervical manifestation, which can mechanically compress the esophagus (Dysphagia) or Airway.
- The airway can be 'Difficult' to intubate due to osteophytes preventing visualization.
- Surgery (Osteophytectomy) is reserved for severe dysphagia or airway compromise.
- Unlike OPLL, OALL does NOT typically cause myelopathy directly.
- “Look for 'Candle Wax' dripping appearance on X-ray.
- “Ask about 'Aspiration Pneumonia' history in elderly patients with neck stiffness.
- “Differentiation from Ankylosing Spondylitis (AS): DISH spares the SI joints and facets.
- “Surgery should preserve the disc space (Osteophytectomy ONLY) unless instability exists.
Overview and Epidemiology
Definition
- DISH (Forestier disease) is a systemic, non-inflammatory enthesopathy causing "flowing" ossification of spinal ligaments and peripheral entheses, sparing the disc and synovial joints.
- OALL (ossification of the anterior longitudinal ligament) is the cervical expression that grows anteriorly, compressing the pharynx, oesophagus and airway rather than the cord.
Key epidemiology (global)
- Radiographic prevalence rises with age: roughly 10 percent over 50 years and up to 25-30 percent over 70 years in autopsy and CT cohorts.
- Male predominance (about 2:1); rare under 40 years.
- Cervical osteophytes are most marked at C3-C6; symptomatic dysphagia affects a minority (often quoted under 20 percent of those with cervical DISH).
- Strongly linked to metabolic syndrome (type 2 diabetes, obesity, hypertension) — DISH is increasingly viewed as a metabolic bone phenotype, not simple "wear and tear".
- The rigid, brittle "bamboo-like" spine fractures easily after low-energy trauma (chalk-stick fractures) with a high rate of neurological injury.
Pathophysiology and Anatomy
The Anterior Longitudinal Ligament (ALL)
- Broad ligament covering the anterior vertebral bodies.
- Prevents hyperextension.
- In DISH, it ossifies but spares the annulus fibrosus and nucleus pulposus (unlike Ankylosing Spondylitis).
The Swallowing Mechanism
- Phase 1 (Oral): Bolus prep.
- Phase 2 (Pharyngeal): Pharynx constricts, Hyoid elevates, Epiglottis inverts.
- Phase 3 (Esophageal): Peristalsis. OALL disrupts Phase 2 by physically blocking epiglottic inversion or narrowing the pharyngeal space.
OALL vs OPLL
The must-know list states that, "unlike OPLL," OALL does not cause myelopathy — so the contrast with OPLL is worth drawing out, because the two are mirror-image problems and a classic exam pairing.
OPLL is the posterior counterpart. Ossification of the posterior longitudinal ligament ossifies behind the vertebral bodies and grows into the spinal canal, compressing the cord and causing cervical myelopathy — the opposite clinical problem to OALL, which grows anteriorly and causes dysphagia/airway obstruction without myelopathy.
What they share. Both are ectopic-ossification disorders that sit within the DISH / metabolic ossification spectrum; OPLL is notably more common in East-Asian populations; and the two can coexist in the same patient (anterior and posterior ossification together).
The contrast in one line:
- OALL
- Anterior longitudinal ligament
- OPLL
- Posterior longitudinal ligament
- OALL
- Anteriorly (away from canal)
- OPLL
- Posteriorly (into the canal)
- OALL
- Dysphagia / airway obstruction
- OPLL
- Cervical myelopathy (cord compression)
- OALL
- Anterior osteophytectomy (no fusion usually)
- OPLL
- Posterior decompression (laminoplasty/laminectomy) for multilevel disease
OPLL is classified by morphology (continuous, segmental, mixed and localised/circumscribed), and multilevel disease is typically decompressed posteriorly (laminoplasty), with dural ossification and CSF leak as recognised hazards of anterior resection — developed in the dedicated OPLL topic.
OPLL is the posterior mirror of OALL: ossification of the posterior longitudinal ligament grows into the canal → cervical myelopathy, whereas OALL grows anteriorly → dysphagia, no myelopathy. Both belong to the DISH/ectopic-ossification spectrum, are commoner in East Asians, and can coexist. Multilevel OPLL is usually decompressed posteriorly (laminoplasty) — detail in the OPLL topic.
Classification Systems
Resnick Criteria (Gold Standard)
Used to diagnose DISH and distinguish from normal spondylosis.
- Flowing calcification along the anterolateral aspect of at least 4 contiguous vertebral bodies.
- Preservation of disc height in the involved segments, and absence of extensive radiographic changes of degenerative disc disease (vacuum sign, marginal sclerosis).
- Absence of apophyseal joint ankylosis or sacroiliac joint erosion/sclerosis/fusion.
Clinical Assessment
Presentation
- Dysphagia: Most common presenting symptom of cervical OALL (a minority of all cervical DISH). "Food sticking".
- Globus Sensation: Feeling of a lump in the throat.
- Dysphonia: Hoarseness (RLN compression or vocal cord edema).
- Stiffness: Decreased cervical ROM.
- Dyspnea: Rare, caused by laryngeal edema or massive C3 osteophyte compressing glottis.
Examination
- Palpation: Hard, bony mass palpable in the posterior pharynx (beware gag reflex).
- Neck: Stiffness, loss of extension.
- Neuro: Usually normal (OALL grows OUT, not IN to the canal).
Imaging and Investigations
Workup Protocol
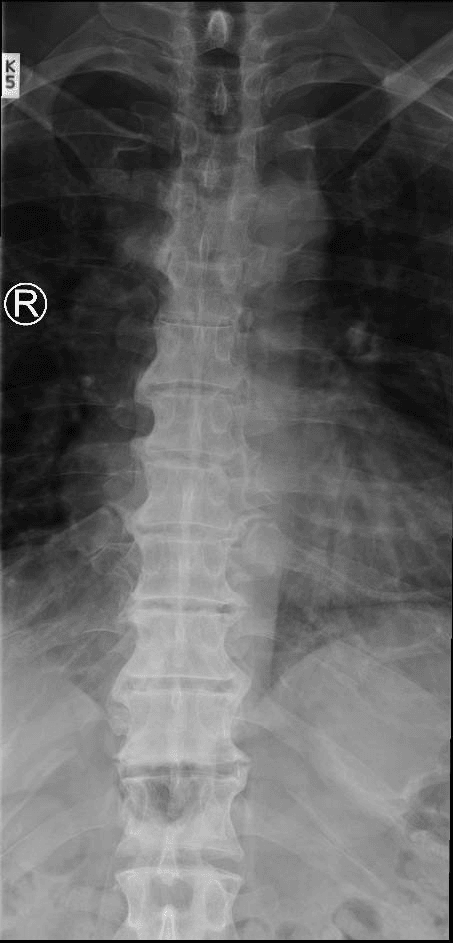
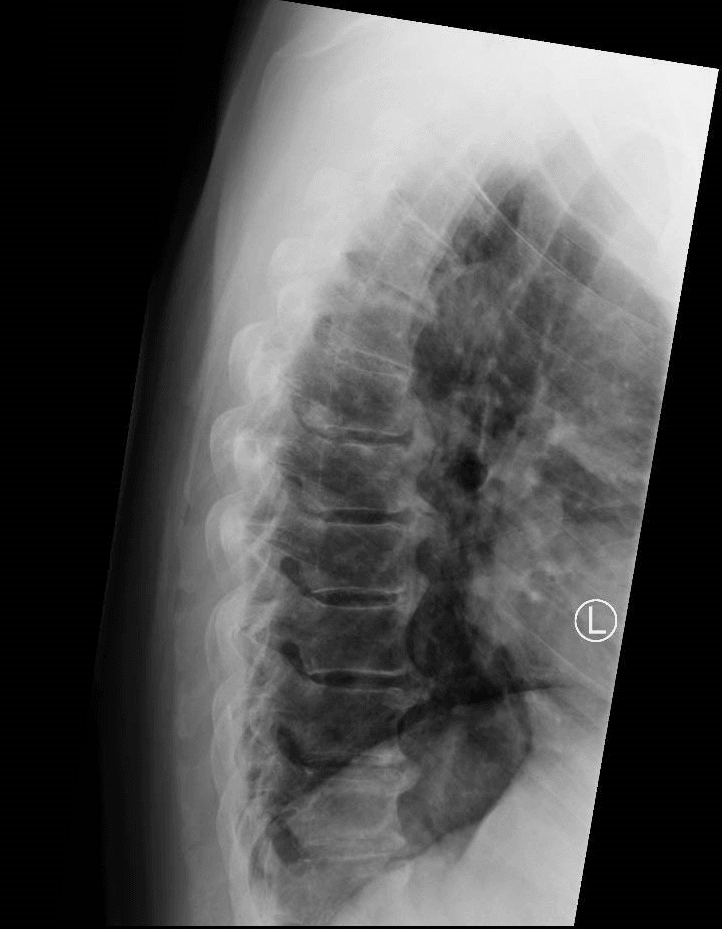
- "Flowing Candle Wax" appearance anterior to bodies.
- Radiolucent line: Between the ossified ALL and the vertebral body (unossified deep layer).
- Check disc heights (spared).
- Video Fluoroscopic Swallowing Study (VFSS).
- Critical to demonstrate the mechanical cause of dysphagia.
- Shows the bolus hitting the osteophyte and spiraling or causing aspiration.
- CT: Defines bony anatomy for resection.
- ENT Nasendoscopy: Mandatory to rule out intrinsic malignancy (cancer) or vocal cord palsy BEFORE surgery.
Non-Operative Management
First Line Treatment
- Dietary Modification: Soft foods, thicken fluids (Speech Pathology involvement).
- NSAIDs: Reduce soft tissue inflammation around the osteophytes.
- Steroids: Short course for acute flare of dysphagia.
- Review: Monitor weight and aspiration signs.
Management Algorithm
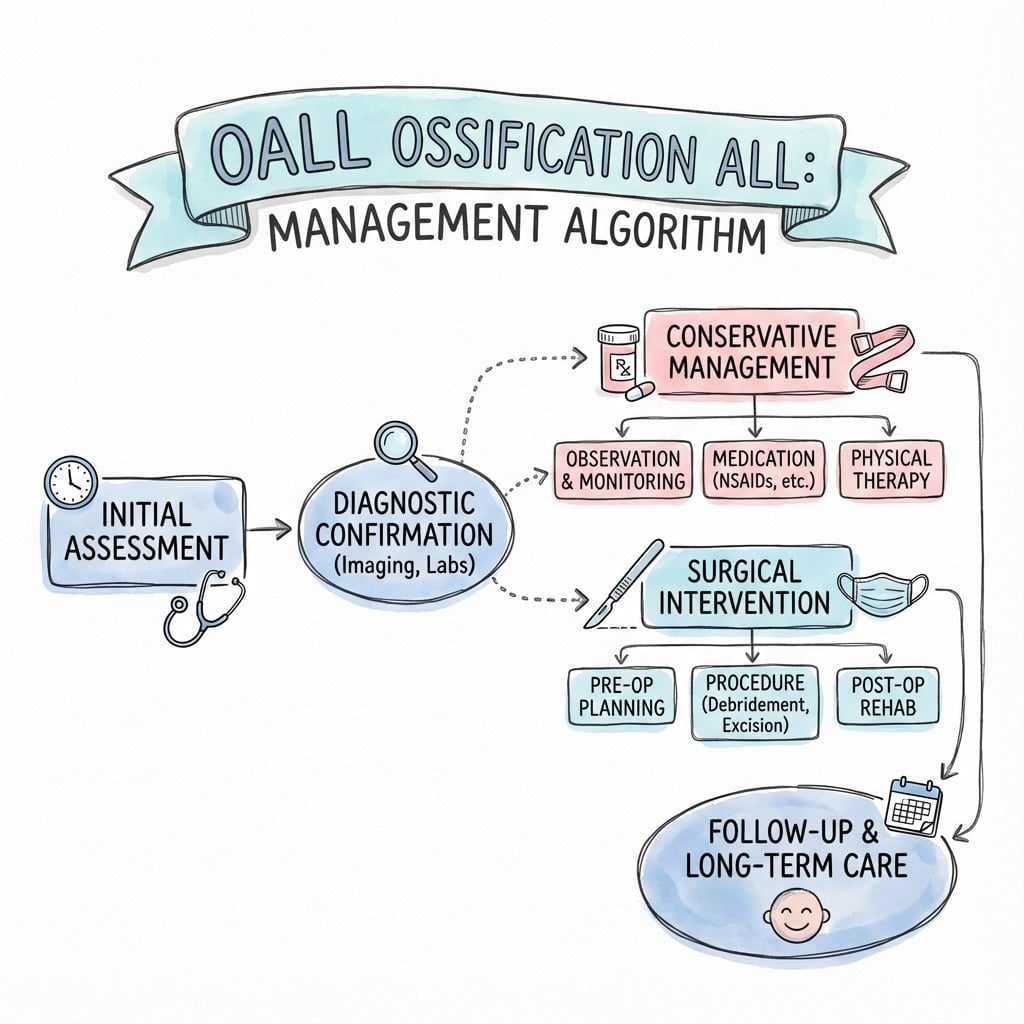
- 1
Dysphagia Symptoms Present
- 2
Rule out Malignancy/Stricture
- 3
Severity of Dysphagia
Surgical Technique
Anterior Cervical Osteophytectomy
- Goal: Resect the anterior bony mass to decompress the esophagus.
- Position: Supine, neck slightly extended (careful! hyperextension can fracture the fused spine). Mayfield head clamp or horseshoe.
- Approach: Standard Smith-Robinson (Anterior Cervical).
Step-by-Step:
- Incision: Transverse skin incision at the level of the osteophyte (fluoroscopy to confirm).
- Dissection: Deep dissection medial to the Carotid sheath and lateral to the Trachea/Esophagus.
- Exposure:
- The prevertebral fascia will be tight over the mass.
- Identification of the "valley" between the osteophyte and the disc space is crucial.
- Adhesions: The esophagus is often adherent to the tip of the osteophytes due to chronic inflammation. Use a peanut dissector or wet Raytec to gently peel.
- Resection:
- Use a high speed Diamond Burr or Leksell Rongeur.
- Resect the "Peaks" (Over the vertebral bodies).
- Be careful at the "Valleys" (Over the discs) not to violate the annulus.
- Limits: Resect flush with the anterior margin of the vertebral body. Do not chase lateral osteophytes near the Foramen Transversarium (Vertebral Artery risk).
- Disc Sparing: Do not enter the disc space.
- Bone Wax: Apply bone wax to the bleeding cancellous surface.
- Closure: Deep drain is essential. Close Platysma and Skin.
Fusion?
- Generally NOT indicated unless there is pre-existing instability.
- Fusion increases adjacent segment disease.
Complications
- Risk Level
- High
- Management
- Retraction injury. Observe. Vocal cord medialization if permanent.
- Risk Level
- High (Adhesions)
- Management
- Direct repair + muscle flap. NGT feeding. Antibiotics.
- Risk Level
- Moderate (years)
- Management
- Use bone wax. Ensure complete resection.
- Risk Level
- Moderate
- Management
- Place drain. Watch airway.
Radiographic osteophyte regrowth is well recognised because the underlying metabolic driver persists, but symptomatic recurrence requiring re-operation is uncommon — about 4 percent in the largest pooled surgical series at a mean follow-up of nearly 4 years. Counsel patients that regrowth is slow and most stay symptom-free.
Postoperative Care
- Airway: Monitor for retropharyngeal hematoma / edema (Stridor).
- Feeding: Nasogastric feeding may be needed if esophageal repair done or severe edema.
- Swallow Study: Repeat contrast swallow before oral intake if dura/esophagus concerns.
Outcomes and Prognosis
- Success Rate: High for dysphagia resolution — improvement in about 95 percent of operated patients in the largest pooled series.
- Aspiration: May not resolve if the cause was neurological or permanent muscle damage.
- QoL: Significant improvement in eating ability.
The Chalk-Stick (Ankylosed-Spine) Fracture
The epidemiology section warns that the "bamboo-like" spine "fractures easily after low-energy trauma (chalk-stick fractures)," the symptom mnemonic flags hyperextension trauma, and a viva asks how a chalk-stick fracture differs from a normal fracture — so this distinct, life-threatening entity deserves developing in its own right.
What it is. In the rigid, fused, often osteoporotic DISH (or AS) spine, a fracture runs transversely across the entire ossified column — like snapping a stick of chalk — usually a hyperextension injury through a disc space or vertebral body. Because the long, stiff lever arms on either side behave like long-bone segments, it is an inherently unstable three-column injury, even after trivial / low-energy trauma (a fall from standing, a minor knock).
Why it is dangerous.
- It is frequently missed or diagnosed late — obscured by the ossified mass and the pre-existing deformity on plain films.
- High rates of spinal epidural haematoma, cord injury and mortality; neurological deterioration can be delayed.
- DISH fractures cluster at the thoracolumbar junction (the topic's cited meta-analysis), whereas AS fractures favour the mid-thoracic spine.
Management principles.
- Treat new spinal pain after ANY trauma in an ankylosed-spine patient as a fracture until excluded.
- Imaging: full-length CT of the whole spine (look for non-contiguous fractures); add MRI when there is a neurological deficit or a suspected disco-ligamentous hyperextension injury (the topic's cited CT-vs-MRI data), balancing the risk of moving the patient.
- Handling: immobilise and transfer in the patient's own fixed posture — never force the neck or spine straight, as this can displace the fracture and injure the cord (the same hyperextension caution that applies to operative positioning).
- Definitive treatment is usually long-segment instrumented stabilisation (long lever arms and poor bone make short constructs fail); many of these fractures need surgery even when they look "minimally displaced." (General fracture classification and fixation are developed in the cervical-spine-fracture, subaxial-cervical-fractures, thoracolumbar-fractures and ankylosing-spondylitis topics.)
A chalk-stick fracture is a transverse three-column break through the rigid fused DISH/AS spine (usually hyperextension), often from trivial trauma — highly unstable, easily missed, with a high rate of epidural haematoma and cord injury. Treat any new pain after trauma as a fracture: full-length CT (± MRI for neurology/disco-ligamentous injury), immobilise in the patient's own deformity (never straighten the neck), and stabilise with long-segment instrumentation. DISH fractures cluster at the thoracolumbar junction.
Guidelines, Registries & Global Practice
Global epidemiology
- Radiographic DISH is common worldwide in older adults: roughly 10 percent over 50 and 25-30 percent over 70, with consistent male predominance across European, North American and Asian CT/autopsy cohorts.
- Population studies repeatedly tie DISH to metabolic syndrome, so prevalence tracks with regional obesity and type 2 diabetes burden.
- Symptomatic cervical OALL (dysphagia or airway obstruction) remains uncommon, and the published surgical literature is dominated by case reports and small series — no randomised data exist.
- Relevant stance
- Treats the ankylosed (DISH/AS) spine as a high-risk fracture pattern; low-energy trauma needs full-length CT and a high index of suspicion for unstable three-column injury.
- Relevant stance
- No DISH-specific guidance; managed under general dysphagia (2-week-wait cancer pathway to exclude malignancy first) and spinal trauma standards.
- Relevant stance
- No dedicated guideline; surgical decompression reserved for refractory mechanical dysphagia or airway compromise after ENT/swallow workup.
- Relevant stance
- Cervical OALL is a recognised predictor of difficult intubation — plan awake fiberoptic technique and avoid forced hyperextension.
Registry & practice variation
- There is no implant registry relevant to OALL because osteophytectomy is usually fusion-free; registry data (NJR, AOANJRR, AJRR) only apply if an instrumented fusion is added for instability or a chalk-stick fracture.
- Well-resourced settings: video fluoroscopic swallow study, CT planning, ENT nasendoscopy and awake fiberoptic intubation are standard before surgery.
- Limited-resource settings: diagnosis often rests on plain lateral radiographs and barium swallow; dietary modification and speech-pathology input carry most of the load, with surgery reserved for severe weight loss or aspiration.
Controversies & Areas of Uncertainty
- No high-level evidence: the entire surgical literature is case reports and small series; there are no randomised trials or formal guidelines, so recommendations are consensus-based (Harlianto/Verlaan systematic review).
- Fusion vs osteophytectomy alone: most authors avoid routine fusion to spare adjacent-segment disease and operative time, reserving it for instability or iatrogenic disc violation — but the threshold is not standardised.
- Defining "mechanical" dysphagia: dysphagia in elderly DISH patients is often multifactorial (neurological, presbyphagia, reflux). A positive swallow study does not guarantee the osteophyte is the sole cause, and a subset have persistent symptoms after technically successful surgery.
- Predicting recurrence: radiographic regrowth is common yet symptomatic recurrence is rare (~4 percent); no reliable predictor or proven preventive (bisphosphonates, metabolic control) exists.
- Imaging in trauma: whether every ankylosed-spine trauma patient needs MRI in addition to CT remains debated — current data suggest selective use for neurological deficit or suspected disco-ligamentous injury.
Mnemonics
DISHResnick Criteria for DISH
Hook:Diagnostic criteria.
DATESymptoms of OALL
Hook:Clinical presentation.
HORSESurgical Risks
Hook:Complications of osteophytectomy.
MCQ Practice Points
Q: Which feature distinguishes DISH from Ankylosing Spondylitis? A: Preservation of SI joints and Facet joints (No ankylosis).
Q: What structure ossifies in DISH? A: Anterior Longitudinal Ligament (ALL).
Q: Post-operative hoarseness after osteophytectomy is most likely due to? A: Recurrent Laryngeal Nerve (RLN) neurapraxia (from retraction).
Q: DISH is strongly associated with which metabolic disorder? A: Type 2 Diabetes Mellitus / Obesity.
Q: When is fusion indicated in OALL surgery? A: Only if instability is present. (E.g. fracture or iatrogenic disc violation). Routine fusion is unnecessary.
At a Glance
- DISH (Forestier)
- Old (over 50)
- Ankylosing Spondylitis (AS)
- Young (under 40)
- DISH (Forestier)
- Normal (Spared)
- Ankylosing Spondylitis (AS)
- Fused (Sacroiliitis)
- DISH (Forestier)
- Preserved
- Ankylosing Spondylitis (AS)
- Calcified/Narrowed
- DISH (Forestier)
- Normal Prevalence
- Ankylosing Spondylitis (AS)
- Highly Associated (+)
Exam Day Cheat Sheet
Key Concepts
- Flowing Anterolateral Ossification
- Disc Height Preserved
- SI Joints Normal
- Dysphagia over Dyspnea
Criteria (Resnick)
- 4+ Contiguous bodies
- Discs spared
- No Facet/SI fusion
- Flowing Candles
Surgery
- Indication: Severe Dysphagia/Wt Loss
- Procedure: Anterior Osteophytectomy
- Protect Esophagus!
- No Fusion usually
Risks
- Esophageal Perforation
- RLN Palsy
- Recurrence
- Hematoma (Airway)
Image Manifest
- [3-preoperative-computed-tomography-ct-a-ct-of-the-ce.png]: Sagittal CT showing OALL and disc preservation
- [5-preoperative-esophagram-revealed-extrinsic-compres.png]: Barium swallow showing esophageal compression
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“75M presents with 6 months of progressive difficulty swallowing solids. He has lost 5kg. He has a history of 'stiff neck'. Lateral X-ray shows massive anterior bone formation C3-C6. What is the diagnosis and workup?”
“You are called to ED for a DISH patient who has fallen and hit his head. GCS 8. The ED registrar cannot intubate. Why?”
“During osteophytectomy, you notice a Bubble in the wound field. What has happened and what do you do?”
Evidence Base
Radiographic & pathological criteria for DISH
- Evaluated 215 cadaveric spines and 100 patients with the disease.
- Defined the radiographic hallmark: flowing anterolateral ossification with a subjacent radiolucent line and preserved disc height.
- Established the three-part criteria distinguishing DISH from ankylosing spondylitis and degenerative spondylosis.
Surgical outcomes for cervical DISH dysphagia/airway obstruction
- 138 articles describing 419 patients (mean age 67 years, 85% male).
- Surgery (most often anterolateral approach) in 66 percent; dysphagia improved in 95.5 percent of operated patients.
- Total post-operative complication rate 22.1 percent (12.7 percent within 1 month).
- Dysphagia recurred in only 4 percent (12 patients) at mean 3.7-year follow-up.
Airway management in OALL of the cervical spine
- Two OALL patients with unexpectedly difficult tracheal intubation from anterior bridging osteophytes.
- Osteophytes displace the posterior hypopharyngeal wall, defeating both direct and fiberoptic-assisted awake intubation.
- OALL found in roughly 12 percent of autopsies and progresses with age.
DISH, metabolic disease and bone quality (Camargo cohort)
- 1545 postmenopausal women; DISH prevalence 8.2 percent.
- DISH associated with significantly higher obesity, metabolic syndrome, hypertension and type 2 diabetes.
- Despite higher lumbar BMD, DISH carried lower trabecular bone score and more vertebral fractures (28.6 vs 15.1 percent).
Vertebral fracture prevalence in DISH vs AS
- 7 DISH studies (n=1193): pooled vertebral fracture prevalence 22.6 percent (95% CI 13.4-33.4).
- 26 AS studies (n=2875): pooled prevalence 15.2 percent.
- DISH fractures cluster at the thoracolumbar junction; AS at the mid-thoracic spine.
CT vs MRI in ankylosing spine trauma
- 124 DISH/AS trauma patients imaged with both CT and MRI.
- MRI revealed additional injuries in 4.8 percent and changed management in 3.2 percent — mostly disco-ligamentous hyperextension injuries.
- Authors advise selective MRI for non-ankylosed levels or neurological deficit.