Hyperostosis of the Ligament Causing Stenosis | Prevalence in East Asian Populations
- OPLL is a genetic disorder of heterotopic ossification (COL6A1, COL11A2 genes).
- Strongly associated with DISH (Diffuse Idiopathic Skeletal Hyperostosis).
- The 'Double Layer Sign' on CT suggests Dural Ossification (High risk of CSF leak).
- The 'K-Line' (Kyphosis Line) determines if Posterior Surgery (Laminoplasty) is viable.
- Major risk of surgery is C5 Palsy and Dural Tear.
- “Always look for the 'Double Layer Sign' on CT before attempting Anterior Surgery.
- “If K-Line is NEGATIVE (Ossification crosses line), Laminoplasty will FAIL (Need Fusion or Corpectomy).
- “Beware of 'Floating Island' technique for dural adherence.
- “Differential: AS (Ankylosing Spondylitis) - but AS affects discs/annulus, OPLL affects ligament.
Overview and Epidemiology
Definition OPLL is a hyperostotic condition characterized by calcification and ossification of the posterior longitudinal ligament. It results in spinal canal stenosis and myelopathy.
Etiology
- Genetic: Strong familial inheritance. Associated with collagen genes (COL11A2, COL6A1).
- Metabolic: Associated with Diabetes (NIDDM), Obesity, and DISH.
- Mechanical: Stress on the ligament may trigger osteogenesis.
Pathology
- Begins as hypertrophy of the ligament.
- Progresses to cartilaginous proliferation.
- Ends in enchondral ossification.
- Can penetrate the dura mater ("Dural Ossification"), making surgical separation impossible without dural resection.
Pathophysiology and Anatomy
The Posterior Longitudinal Ligament (PLL)
- Runs along the posterior aspect of the vertebral bodies (within the canal).
- Acts to prevent hyperflexion.
- In OPLL, it becomes a space-occupying lesion anterior to the cord.
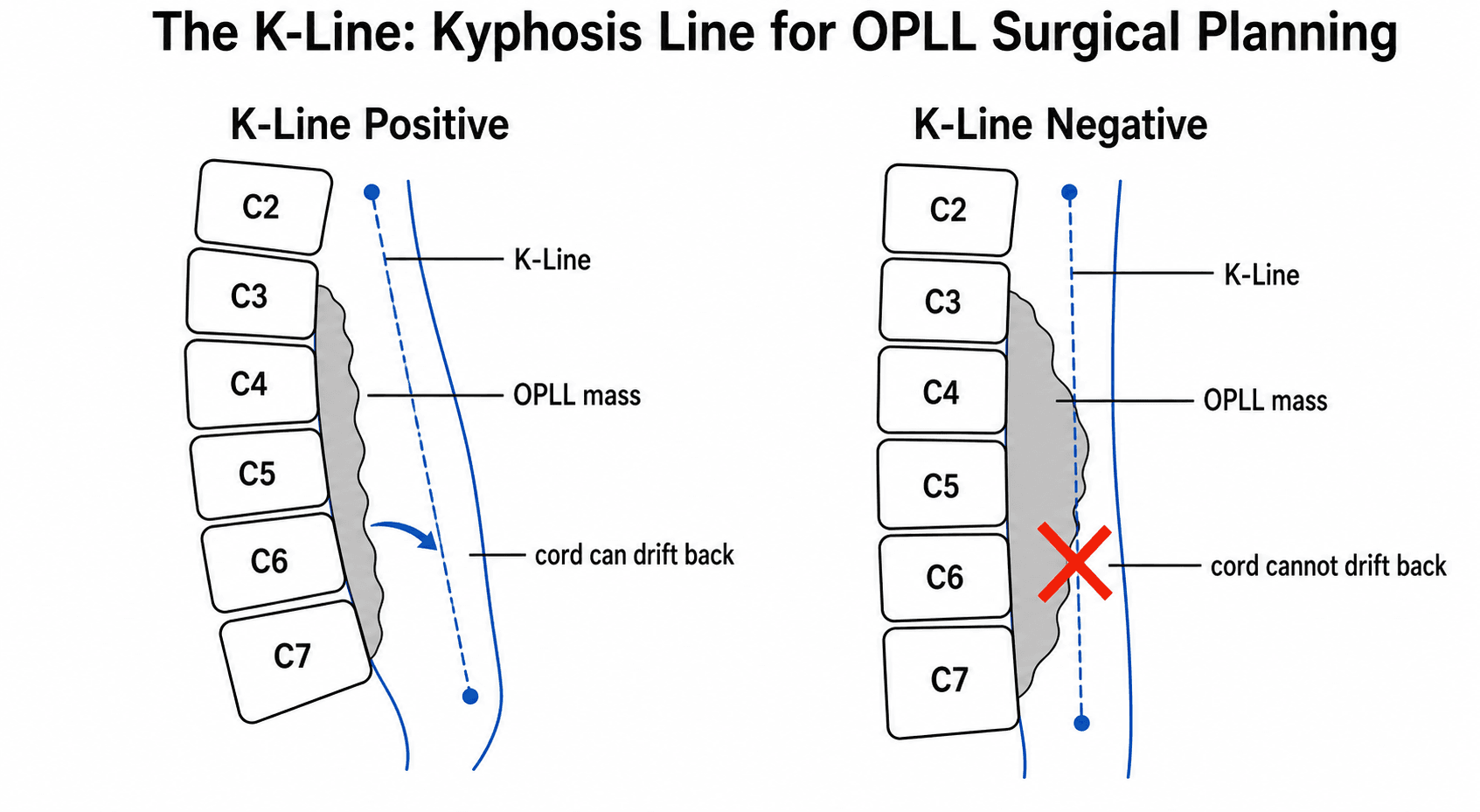
The K-Line (Kyphosis Line)
- A virtual line drawn on a lateral Neutral X-ray.
- Start: Midpoint of C2 Spinal Canal.
- End: Midpoint of C7 Spinal Canal.
- Significance: Defines the anterior limit of the spinal canal.
- K-Line Positive: The OPLL mass lies ANTERIOR to the line. (Good for posterior surgery).
- K-Line Negative: The OPLL mass CROSSES the line. (Posterior surgery will fail as cord cannot drift back past the mass).
Classification Systems
Tsuyama Classification (Based on Lateral X-ray/CT)
- Continuous Type (27%): A long lesion extending over several vertebrae. Most difficult to treat.
- Segmental Type (39%): Lesions located behind each vertebral body, not crossing the disc. (Safest for ACDF/Corpectomy as discs are clear).
- Mixed Type (29%): Combination of above. Most common.
- Localized Type (5%): Circumscribed lesion at disc level.
Clinical Assessment
Presentation
- Similar to CSM but often more severe/rapid once symptomatic.
- Myelopathy: Hands (clumsy), Gait (ataxic), Bladder (late).
- Radiculopathy: Can occur if lateral extension involves roots.
- Trauma: Acute quadriplegia after minor fall is a classic presentation (stiff spine + stenosis).
Examination
- UMN signs (Hyperreflexia, Clonus, Hoffman's).
- Limited ROM (Stiff neck - often has DISH).
50% of OPLL patients have DISH. Check the rest of the spine (Thoracic/Lumbar) for ankylosis. Rigid spines are prone to "Chalk stick fractures".
Imaging and Investigations
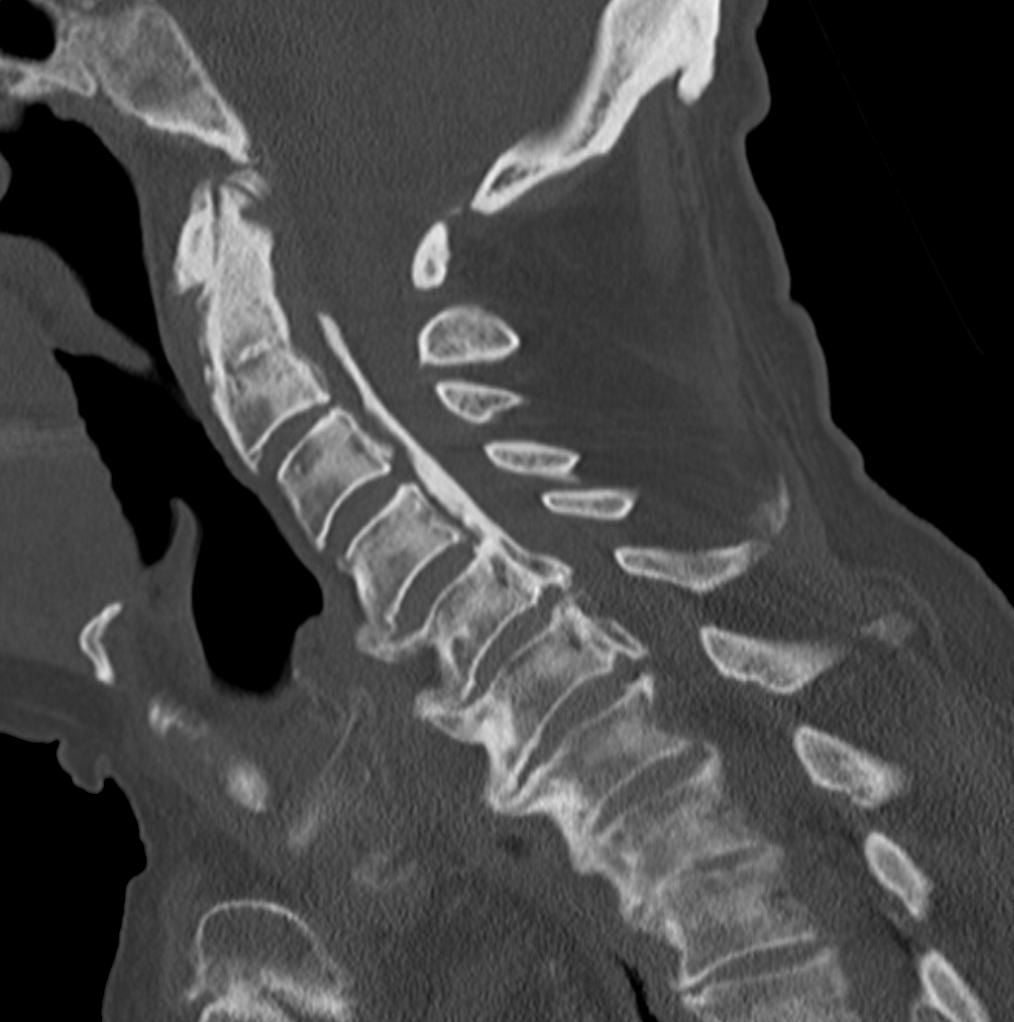
Workup Protocol
- Mandatory for OPLL. MRI allows visualization but CT defines the bony anatomy.
- Assess:
- Thickness of ossification (greater than 50% canal occupancy = bad prognosis).
- Shape (Beak/Hill/Mushroom).
- Double Layer Sign (Dural involvement).
- T2 Signal: Check for myelomalacia.
- Effacement: CSF signal loss.
- Lateral: Draw the K-Line. Measure C2-C7 angle.
- Flex/Ext: Usually stiff, but check for instability.
Quantifying the OPLL: Occupying Ratio and Mass Shape
The workup above repeatedly relies on "canal occupancy" and the ossification "shape (beak/hill/mushroom)" as prognostic levers, but neither is defined. Both are measured on the CT and both predict whether a cord will become myelopathic and how it will respond to surgery, so they deserve to be spelled out.
The occupying ratio (OR). This is the single most-quoted number in OPLL. It is the maximum antero-posterior thickness of the ossified mass divided by the antero-posterior diameter of the spinal canal at the same level, expressed as a percentage (measured on the mid-sagittal CT or axial bone window):
Occupying ratio = (AP thickness of OPLL ÷ AP canal diameter) × 100
A higher ratio means less reserve space for the cord. A ratio approaching or exceeding about 60% is the classic threshold associated with a high likelihood of myelopathy and a poorer natural history; combined with dynamic factors (segmental mobility on flexion-extension) it is one of the radiographic predictors of deterioration that push towards surgery rather than observation. A very high ratio also argues against posterior surgery alone, because even a fully drifted cord can remain draped over a large anterior mass.
The shape of the mass. Two masses with the same occupying ratio do not behave the same way - the cross-sectional shape matters:
- Description
- A focal, pointed, often single-level prominence projecting into the canal
- Significance
- Concentrates pressure on a small area of cord; associated with more severe focal myelopathy and a poorer response to posterior drift-back - frequently favours direct anterior decompression
- Description
- A broad-based, flatter mass spread over the vertebral body
- Significance
- Spreads load over a wider cord surface; generally more amenable to indirect posterior decompression if the K-Line is positive
- Description
- A broad base with an expanded posterior cap
- Significance
- Behaves like a large plateau but with a prominent apex; assess occupancy and lateral deviation carefully
Lateral deviation of the mass off the midline is an additional warning sign: an asymmetric beak loads one side of the cord and limits the uniform posterior drift that laminoplasty depends on, so a laterally-deviated, high-ratio beak is one of the patterns that tips the decision toward an anterior or circumferential strategy.
When asked "how compressed is this cord?", do not just say "severe" - state the occupying ratio (AP OPLL thickness ÷ canal diameter × 100), flag that roughly 60% or more predicts myelopathy and a worse natural history, then add that a sharp beak-type or laterally-deviated mass concentrates pressure and resists posterior drift-back, biasing the choice toward anterior or fusion surgery even when the K-Line is borderline.
Differential Diagnosis
- Key Distinguishing Feature
- Ossified PLL behind vertebral bodies
- Imaging Clue
- Linear ossification in canal; double-layer sign if dural involvement
- Typical Pattern
- Myelopathy more than axial pain
- Key Distinguishing Feature
- Disc-osteophyte complex and uncovertebral hypertrophy
- Imaging Clue
- Soft and bony stenosis at disc levels, no continuous posterior ossified strip
- Typical Pattern
- Multilevel degenerative change
- Key Distinguishing Feature
- Flowing anterolateral bridging osteophytes, disc/facet spared
- Imaging Clue
- Ossification anterior to bodies; coexists with OPLL in up to half of cases
- Typical Pattern
- Often asymptomatic stiffness
- Key Distinguishing Feature
- Inflammatory; affects annulus/syndesmophytes and SI joints
- Imaging Clue
- Bamboo spine, marginal syndesmophytes, fused SI joints
- Typical Pattern
- HLA-B27, young, inflammatory back pain
- Key Distinguishing Feature
- Posterior compression from ossified flavum
- Imaging Clue
- Ossification arising from lamina/facet, mainly thoracic
- Typical Pattern
- Thoracic myelopathy, can coexist with OPLL
- Key Distinguishing Feature
- Calcification rather than mature ossification
- Imaging Clue
- Amorphous calcium, often retro-odontoid (crowned dens)
- Typical Pattern
- Older patients, can mimic focal mass
Non-Operative Management
Observation
- Many patients have OPLL incidentally.
- Progression rate is slow but steady.
- Contraindications to observation: Progressive myelopathy (mJOA score dropping), acute onset.
- Advice: Avoid contact sports, fall prevention, collar for comfort only.
Management Algorithm
- 1
Diagnosis Confirmed on CT
- 2
Symptomatic Myelopathy?
- 3
Surgical Approach: Check K-Line
Surgical Technique
Laminoplasty (Preferred)
- Indication: Multilevel OPLL (C3-C7) with K-Line (+).
- Rationale: Expanding the canal posteriorly allows the cord to "drift back" away from the anterior OPLL mass.
- Technique: "Open Door" (Hirabayashi) or "French Door" (Kurokawa).
- Plate Fixation: Use mini-plates to keep the lamina open.
- Advantages: Preserves motion (vs fusion), lower complication rate than anterior.
- Risks: C5 palsy (tethering from drift back), Axial neck pain.
Step-by-Step (Double Door / French Door):
- Positioning: Prone, Mayfield head clamp. Neck flexed slightly (military tuck).
- Exposure: Midline approach. Subperiosteal dissection to the lateral masses. Preserve the Semispinalis Cervicis attachment to C2 (reduces post-op kyphosis/pain).
- Spinous Process: Removed.
- Troughs:
- Midline Trough: Created through the junction of the lamina (roof). Full thickness cut.
- Lateral Troughs: Created at the lamina-facet junction bilaterally. Thin the outer cortex but leave the inner cortex intact (Greenstick fracture).
- Opening: The split lamina are opened like a book ("French Door") laterally.
- Fixation: Ceramic spacers or mini-plates bridge the gap and hold the door open.
- Closure: Deep closure over a drain.
ACAF: Anterior Controllable Antedisplacement and Fusion
The evidence base and the controversies section both invoke ACAF, yet the technique is never described. It is the most important recent addition to OPLL surgery and a high-yield viva topic, because it is designed specifically to solve the problem that makes anterior corpectomy so dangerous: peeling a dura-adherent ossified mass off the cord.
The core idea. In a conventional corpectomy the surgeon removes the vertebral bodies and then tries to resect the OPLL, risking a massive unrepairable dural tear. ACAF instead moves the whole vertebral-body-plus-OPLL complex forward as a single unit rather than removing the ossified mass at all:
- Anterior plate and screws are positioned first, with the screws set to the intended new (anterior) position.
- The vertebral bodies bearing the OPLL are isolated by bilateral longitudinal osteotomies/grooves at the body-pedicle junction, and the discs above and below are released, freeing a "bone-OPLL complex".
- The freed complex is then lifted (ante-displaced) anteriorly and held in its new forward position by tightening it down onto the pre-contoured plate.
Because the OPLL is never separated from the dura - the cord is decompressed by translating the whole anterior wall forward - the dreaded step of stripping ossified dura is avoided, which is the rationale for ACAF's lower CSF-leak profile in difficult, dura-adherent disease.
- ACAF
- Translate the bone-OPLL complex forward (no resection)
- Corpectomy (resection)
- Directly remove/resect the OPLL
- Laminoplasty
- Indirect cord drift-back
- ACAF
- Handled WITHOUT stripping dura
- Corpectomy (resection)
- Highest dural-tear / CSF-leak risk
- Laminoplasty
- Avoids the dura but needs K-Line (+)
- ACAF
- Restored (anterior fusion)
- Corpectomy (resection)
- Restored
- Laminoplasty
- Not corrected (relies on existing lordosis)
- ACAF
- Longer operation, more dysphagia, lateral OPLL/vertebral-artery risk during grooving
- Corpectomy (resection)
- CSF leak, graft kick-out
- Laminoplasty
- C5 palsy, continued OPLL growth
What the evidence shows. A meta-analysis of multilevel cervical OPLL (Zhang, PMID 38157983: 7 studies, 467 patients) found that, compared with laminoplasty, ACAF gave higher JOA scores and improvement rate, better restored cervical lordosis, and lower rates of C5 palsy and axial symptoms, with less blood loss - at the cost of longer operative time and more dysphagia, and with no significant difference in CSF-leak or overall complication rate. ACAF is therefore an attractive option for multilevel, high-occupancy, K-Line-negative or dura-adherent OPLL where both a corpectomy and a laminoplasty are problematic, accepting a swallowing-morbidity and learning-curve trade-off.
The one sentence that wins the ACAF question: instead of removing the OPLL (and risking the dura), you osteotomise the vertebral-body-OPLL complex and shift it forward en bloc onto a pre-set plate, decompressing the cord without ever separating ossified dura. That is why it is favoured for dura-adherent, K-Line-negative multilevel disease - at the price of longer surgery and more dysphagia.
Complications
- Ant Rate
- High (20%)
- Post Rate
- Low
- Management
- Lumbar drain, bed rest, fibrin glue. Do NOT repair primarily (tissue too thin).
- Ant Rate
- 5%
- Post Rate
- 10-15%
- Management
- Observation. Usually recovers. Due to 'tethering' effect.
- Ant Rate
- Low
- Post Rate
- Medium
- Management
- OPLL can grow post-surgery. Laminoplasty allows continued growth.
- Ant Rate
- High (Corpectomy)
- Post Rate
- Low
- Management
- Use supplemental posterior fixation for multilevel corpectomy.
Postoperative Care
- CSF Leak Protocol: If leak suspected/confirmed: Flat bed rest 24-48hrs. Acetazolamide. Lumbar Drain if persistent.
- Collar: Aspen collar 6 weeks (especially if fusion).
- Neuro Rehab: Intensive gait training.
Outcomes and Prognosis
- Surgical Outcome: Generally good if K-Line respected.
- Recurrence: OPLL mass continues to grow in 20% of cases, especially with Laminoplasty (motion preserved). Fusion arrests growth.
- Poor Prognostic Factors:
- Diagnosis over 60 years.
- Myelopathy duration over 1 year.
- Massive canal occupancy (greater than 60%).
- Trauma-induced onset.
- High intramedullary signal intensity on T2 MRI.
- Diabetes Mellitus (Poor wound healing, infection risk).
Progression Rates:
- Longitudinal studies show OPLL grows 2mm/year in 10% of patients.
- Anterior fusion stops this growth in the fused segments, but adjacent segment disease is accelerated.
- Laminoplasty allows continued growth, but usually the canal expansion is sufficient to accommodate it.
Guidelines, Registries & Global Practice
Global epidemiology
- Prevalence is strongly ethnicity-dependent: 1.9-4.3% in Japanese adults over 30 (Matsunaga, Spine 2012), and broadly 0.4-3% across East Asian populations (Japan, Korea, China, Taiwan).
- Much lower in populations of European and African descent (roughly 0.1-1.7%), but rising with CT use and ageing — OPLL should be on the myelopathy differential worldwide, not only in East Asian patients.
- Male predominance (about 2:1), peak presentation in the 5th-7th decades, strong associations with type 2 diabetes, obesity, and DISH.
Side-by-side guideline / consensus positions
- Position on cervical OPLL / myelopathy
- Operative decompression recommended for moderate-to-severe myelopathy; surgery may be offered in mild myelopathy; structured non-operative trial with close monitoring acceptable for very mild/non-myelopathic disease.
- Position on cervical OPLL / myelopathy
- OPLL managed as a defined disease entity; CT mandatory; mJOA-based surveillance; approach guided by K-Line and canal occupancy.
- Position on cervical OPLL / myelopathy
- Approach individualised to alignment and compression level; anterior favoured for focal kyphotic compression, posterior for multilevel lordotic disease.
- Position on cervical OPLL / myelopathy
- Consensus that posterior is safer for multilevel K-Line (+) lordotic spines; anterior reserved for focal or kyphotic compression with experienced surgeons.
Registry / outcome evidence
- Unlike arthroplasty, there is no dedicated implant registry for OPLL; the evidence base is dominated by large Japanese multicentre cohorts and meta-analyses (e.g. ACAF vs laminoplasty, Zhang 2024).
- Cohort data consistently show anterior reconstruction yields higher neurological recovery but greater approach-related morbidity, while posterior decompression is safer and faster.
High- vs limited-resource practice variation
- High-resource settings: routine pre-operative CT and MRI, intra-operative neuromonitoring, ultrasonic bone scalpels and microscopes for floating-method anterior surgery.
- Limited-resource settings: reliance on plain films and MRI (CT may be limited); laminectomy or laminoplasty is often preferred as a lower-risk, lower-cost option even when anterior surgery might give marginally better recovery, because dural-tear and CSF-leak management is resource-intensive.
- Trauma context: in any setting, a rigid OPLL/DISH spine is at high risk of central cord syndrome after minor hyperextension — fall prevention and early imaging of new deficits are universal priorities.
Controversies & Areas of Uncertainty
- Asymptomatic / prophylactic surgery: How aggressively to treat high canal-occupancy OPLL before myelopathy develops remains debated. High occupancy and dynamic instability predict deterioration, but prophylactic surgery carries real risk and is not universally endorsed.
- Anterior versus posterior for multilevel disease: Anterior reconstruction (corpectomy, ACAF) tends to give better neurological recovery but more approach-related morbidity (dysphagia, CSF leak, graft issues); posterior surgery is safer and faster. There is no single correct answer — alignment (K-Line), occupancy and surgeon experience drive the choice.
- Laminoplasty versus laminectomy-and-fusion: Both decompress posteriorly. Fusion arrests OPLL progression and corrects alignment but sacrifices motion and raises C5 palsy risk; laminoplasty preserves motion but allows continued ossification growth.
- Resect versus float ossified dura: The floating (or anterior controllable antedisplacement, ACAF) philosophy of not resecting dura-adherent OPLL is increasingly favoured to avoid unrepairable dural defects, but adequacy of decompression versus leak risk is still weighed case by case.
- Steroids for C5 palsy / prophylaxis: There is no high-level evidence supporting routine steroids to prevent or treat post-decompression C5 palsy; management remains largely supportive.
- Medical modulation of progression: Identification of Wnt-pathway genes such as RSPO2 raises the prospect of pharmacological control of ossification, but no disease-modifying drug therapy currently exists.
Mnemonics
JAPANOPLL Associations
Hook:Key demographic factors.
SCMLTypes of OPLL
Hook:Classification system.
DOUBLECT Signs of Risk
Hook:Surgical danger signs.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are performing an Anterior Corpectomy for OPLL. You reach the posterior cortex and drill it down. You see a white, hard layer that looks like dura but is bone. What is this and what do you do?”
“60M with C3-C7 OPLL. Myelopathic. Lateral X-ray shows the OPLL mass crosses the K-Line. Lordosis is lost. Plan?”
“Reviewing a post-op Laminoplasty patient on Day 1. He says he cannot lift his arms (Shoulders). Legs are fine.”
MCQ Practice Points
Q: What does the genetics of OPLL tell us? A: OPLL is polygenic. Early linkage work implicated collagen genes (COL6A1, COL11A2); the large Japanese GWAS (Nakajima, Nat Genet 2014) identified six susceptibility loci, with RSPO2 (a Wnt/beta-catenin agonist) later confirmed as a functional gene. Key message: it is a true genetic disease of ectopic ossification.
Q: What is the most common concomitant spinal disorder in OPLL patients? A: DISH (Diffuse Idiopathic Skeletal Hyperostosis). Look for flowing osteophytes.
Q: Converting continuous OPLL to segmental type surgery has what sign on CT? A: Double Layer Sign. It indicates dural ossification.
Q: What is the most common neurological complication after posterior decompression for OPLL? A: C5 Palsy.
Q: A 'Negative K-Line' implies what deformity? A: Kyphosis. The OPLL mass sits posterior to the line connecting C2 and C7 canal midpoints.
At a Glance
- Anterior (Corpectomy/ACDF)
- Can treat K-Line (-)
- Posterior (Laminoplasty)
- Requires K-Line (+)
- Posterior (Laminectomy + Fusion)
- Can treat K-Line (-) if corrected
- Anterior (Corpectomy/ACDF)
- High (10-30%)
- Posterior (Laminoplasty)
- Low (less than 1%)
- Posterior (Laminectomy + Fusion)
- Low (less than 1%)
- Anterior (Corpectomy/ACDF)
- Direct (Removes mass)
- Posterior (Laminoplasty)
- Indirect (Drift back)
- Posterior (Laminectomy + Fusion)
- Indirect + Realignment
- Anterior (Corpectomy/ACDF)
- Low
- Posterior (Laminoplasty)
- Moderate
- Posterior (Laminectomy + Fusion)
- High
Exam Day Cheat Sheet
Key Concepts
- Ectopic Ossification (PLL)
- Japanese/Asian (greater than 2%)
- DISH Association
- Myelopathy over Radiculopathy
Classification
- Continuous vs Segmental
- K-Line (+) = Laminoplasty OK
- K-Line (-) = Anterior or Fusion
- Double Layer Sign = Dural Tear Risk
Surgery
- Posterior preferred (Safety)
- Anterior (Corpectomy) for K-Line (-)
- Floating Island Technique
- Instrumented Fusion for Correction
Risks
- C5 Palsy (Tethering)
- CSF Leak (Anterior)
- Progression (Recurrence)
- Pseudoarthrosis
Evidence Base
The K-Line: a new concept for surgical approach selection
- Defined the K-Line as a line joining the midpoints of the canal at C2 and C7; OPLL not exceeding it = K-Line (+), exceeding it = K-Line (-).
- Mean JOA recovery rate after posterior decompression was 66.0% in K-Line (+) versus only 13.9% in K-Line (-) (p less than 0.01).
- Intra-operative ultrasonography confirmed insufficient posterior cord drift in K-Line (-) patients.
ACAF versus laminoplasty for multisegment cervical OPLL: a meta-analysis
- Anterior controllable antedisplacement and fusion (ACAF) gave higher JOA scores, better cervical lordosis and lower C5 palsy and axial symptom rates than laminoplasty.
- Laminoplasty had shorter operative time and less blood loss; ACAF carried more dysphagia.
- No significant difference in CSF leak rate or overall total complication rate between approaches.
Implications of different patterns of the double-layer sign
- Dural ossification was found in 92 of 268 patients, all showing a double-layer sign on axial CT bone windows.
- Sign was sub-typed A (crescent), B (short-straight) and C (long-straight); CSF leak rose sharply with the more linear patterns.
- All type C cases developed post-operative CSF leak, whereas only 2 of 51 type A and 6 of 35 type B did.
GWAS identifies susceptibility loci for OPLL
- Identified six susceptibility loci for OPLL (20p12.3, 8q23.1, 12p11.22, 12p12.2, 8q23.3, 6p21.1).
- Implicated genes acting through membranous and/or endochondral ossification pathways.
- Established OPLL as a polygenic disorder with a strong, reproducible genetic basis.
RSPO2 as a functional susceptibility gene for OPLL
- Identified RSPO2 (R-spondin 2), a Wnt/beta-catenin agonist, as the susceptibility gene at 8q23.1.
- The risk allele of rs374810 reduced C/EBP-beta binding and lowered RSPO2 transcription.
- Linked dysregulated Wnt signalling and chondrocyte differentiation to ectopic ossification.
OPLL of the cervical spine: etiology and natural history
- Reported OPLL prevalence of 1.9-4.3% in Japanese adults over 30 years.
- Confirmed strong genetic contribution with candidate genes and slow but steady ossification growth.
- Defined radiographic predictors (canal occupancy, dynamic factors) for development of myelopathy.