Blood Conservation in Orthopaedic Surgery
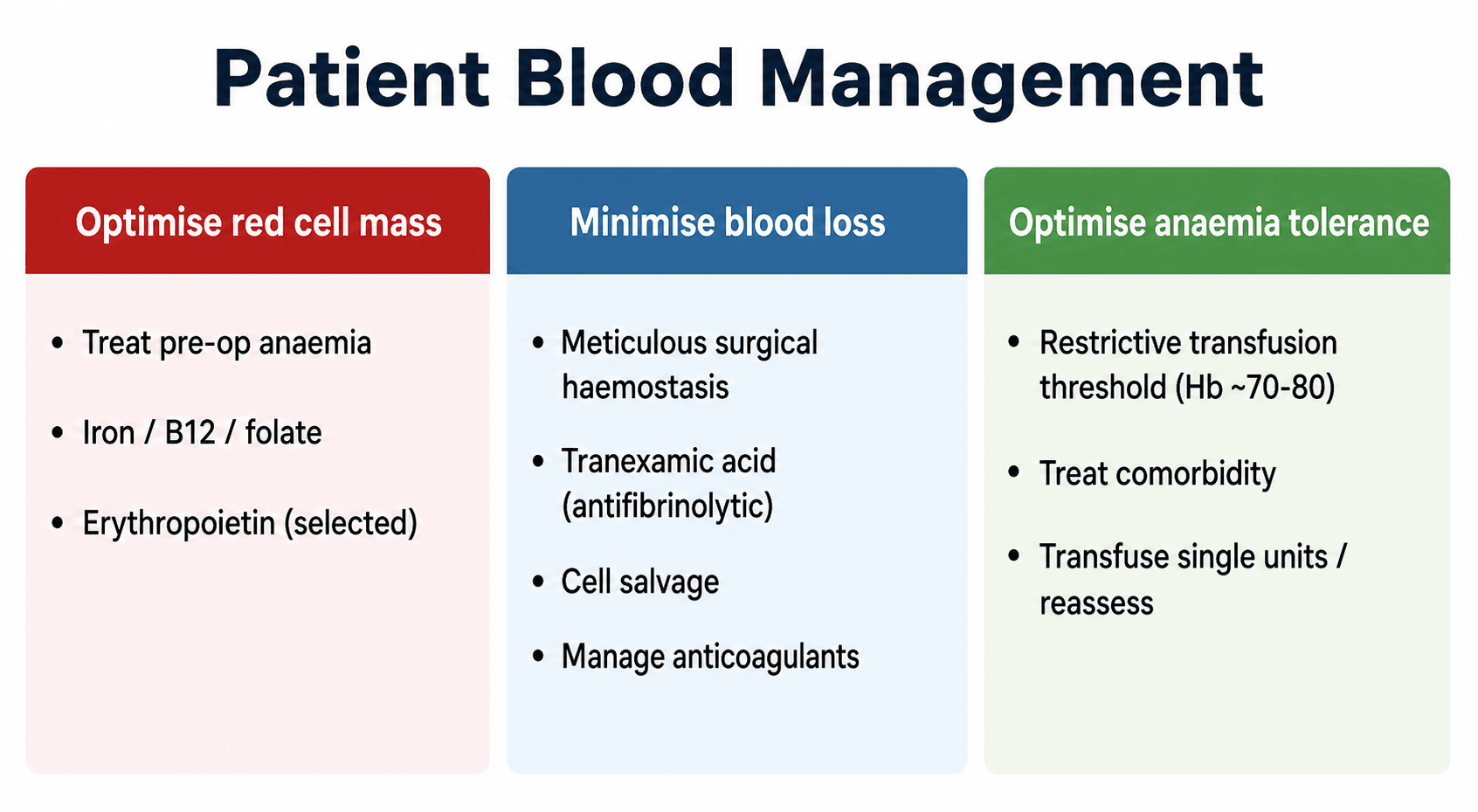
- Patient Blood Management (PBM) is an evidence-based, patient-centred strategy built on THREE PILLARS: (1) OPTIMISE the patient's RED CELL MASS (treat pre-operative anaemia), (2) MINIMISE blood LOSS and bleeding, and (3) OPTIMISE the patient's physiological TOLERANCE of anaemia (restrictive transfusion) - the aim being to avoid or reduce ALLOGENEIC (donor) blood transfusion and its risks.
- TRANEXAMIC ACID (TXA) is the CORNERSTONE pharmacological measure: an antifibrinolytic (a lysine analogue that inhibits plasminogen activation) given intravenously or topically, it significantly REDUCES blood loss and the need for transfusion in arthroplasty, hip-fracture and trauma surgery WITHOUT a significant increase in thromboembolic events in trials.
- A RESTRICTIVE transfusion strategy - transfusing at a haemoglobin around 70-80 g/L (the higher end, ~80, in symptomatic or cardiovascular patients) or for symptoms of anaemia, rather than a 'liberal' trigger - is as safe as liberal transfusion and reduces unnecessary transfusion; transfuse SINGLE UNITS and REASSESS rather than giving fixed multi-unit orders.
- INTRAOPERATIVE CELL SALVAGE (collecting, washing and re-infusing the patient's own red cells) is useful in HIGH-BLOOD-LOSS surgery (revision arthroplasty, complex spine, pelvic/acetabular trauma), but in PRIMARY arthroplasty it adds LITTLE benefit OVER tranexamic acid alone and adds cost - so it is targeted to high-loss cases, not used routinely when TXA suffices; it is used cautiously in malignancy/infection.
- PRE-OPERATIVE ANAEMIA is a common, MODIFIABLE risk factor for transfusion and worse outcomes - elective patients should be screened and treated (iron deficiency with oral or IV iron, B12/folate, erythropoietin in selected cases) before surgery to build up red cell mass.
- JEHOVAH'S WITNESS patients DECLINE allogeneic blood (and usually pre-stored autologous blood) on religious grounds but, individually, often ACCEPT CELL SALVAGE and some fractionated products kept in CONTINUITY with their circulation; they require careful pre-operative PLANNING and documented consent/advance directive, maximisation of red cell mass (iron/erythropoietin), meticulous haemostasis, TXA, continuous-circuit cell salvage, a lower transfusion trigger, senior involvement and RESPECT for their autonomy.
- “PBM 3 pillars: optimise red cell mass (treat anaemia), minimise blood loss (TXA/haemostasis/cell salvage), optimise anaemia tolerance (restrictive transfusion).
- “Tranexamic acid = cornerstone (reduces transfusion, no significant VTE increase). Restrictive trigger ~70-80 g/L; single-unit transfusion + reassess.
- “Cell salvage for HIGH-loss surgery (revision/spine/pelvis), limited added benefit over TXA in primary arthroplasty. Jehovah's Witness: plan ahead, document consent, accept cell salvage in continuity, respect autonomy.
Antifibrinolytic that reduces blood loss and transfusion in arthroplasty/hip-fracture/trauma, with no significant rise in VTE - give IV and/or topical to most major orthopaedic cases.
Transfuse at ~70-80 g/L (or for symptoms), single units with reassessment - as safe as a liberal trigger and avoids unnecessary transfusion.
The Three Pillars
PBM reframes care around the patient's own blood rather than the blood bank. Pillar 1 - optimise red cell mass: screen for and treat pre-operative anaemia (iron, B12/folate, erythropoietin in selected cases) before elective surgery. Pillar 2 - minimise blood loss: meticulous surgical haemostasis, tranexamic acid, regional/hypotensive anaesthesia, a tourniquet where appropriate, cell salvage in high-loss cases, and careful management of anticoagulants/antiplatelets. Pillar 3 - optimise tolerance of anaemia: a restrictive transfusion threshold, single-unit transfusion with reassessment, and managing cardiorespiratory comorbidity. Together these reduce exposure to allogeneic blood and its risks (infection, TRALI, TACO, immunomodulation, cost).
Key Measures
- Tranexamic acid: the most effective single pharmacological measure - reduces blood loss and the need for transfusion across arthroplasty, hip-fracture and trauma surgery, given IV and/or topically, without a significant increase in venous thromboembolism in trials.
- Restrictive transfusion: transfuse at a haemoglobin of about 70-80 g/L (using ~80 in symptomatic or cardiovascular patients) or for symptoms; give single units and reassess.
- Pre-operative anaemia optimisation: screen elective patients; treat iron deficiency (oral or IV iron), B12/folate, and use erythropoietin in selected cases.
- Cell salvage: reserve for high-blood-loss surgery (revision arthroplasty, complex spine, pelvic/ acetabular trauma); in primary arthroplasty it adds little over TXA alone and adds cost; use with caution in malignancy/infection.
- Anaesthetic/surgical adjuncts: regional or hypotensive anaesthesia, tourniquet, warming (hypothermia worsens coagulopathy), and managing anticoagulants/antiplatelets around surgery.
Jehovah's Witness patients decline allogeneic blood and usually pre-stored autologous blood, but individually many ACCEPT intraoperative cell salvage and some fractionated products provided these are kept in CONTINUITY with their circulation - so each patient's specific wishes must be clarified and documented. Plan ahead: an explicit advance directive/consent discussion, maximise red cell mass (iron and erythropoietin pre-operatively), meticulous haemostasis, tranexamic acid, continuous-circuit cell salvage, a lower transfusion trigger, senior anaesthetic and surgical involvement, and clear documentation. Above all, respect the patient's autonomy - their informed refusal must be honoured even if it risks life.
Evidence & Key Studies
Interventions for reducing red blood cell transfusion in hip fracture surgery: an overview of systematic reviews
- Tranexamic acid probably reduces the need for allogeneic transfusion in hip-fracture surgery (risk ratio 0.56; about 194 fewer people per 1000 requiring transfusion) and reduces the volume transfused.
- There was probably little or no difference in adverse events (DVT, PE, MI, stroke, death) with tranexamic acid.
- Intravenous iron showed little or no overall difference, and evidence for other interventions was lacking - highlighting tranexamic acid as the best-supported measure.
Combined intraoperative cell salvage and tranexamic acid for primary total hip arthroplasty: added benefit?
- In 1171 primary THAs, adding intraoperative cell salvage to tranexamic acid did NOT improve blood loss or transfusion outcomes compared with tranexamic acid alone.
- Cell salvage added about $146 per case (over $123,000 across the study period) with no observed clinical benefit.
- Routine cell salvage may not be justifiable in primary THA when tranexamic acid is used - reserve it for high-loss cases.
According to PubMed, the efficacy of tranexamic acid in reducing transfusion (with little/no increase in adverse events) and the limited evidence for iron/other measures come from the cited Lewis Cochrane overview, and the lack of added benefit (and added cost) of cell salvage over tranexamic acid alone in primary THA from the cited Miller study. The three-pillar PBM framework, restrictive transfusion thresholds and Jehovah's Witness planning are standard, well-established perioperative teaching. (See also our Preoperative Optimisation, Venous Thromboembolism Prophylaxis and Anaemia topics.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How would you minimise blood transfusion in a patient undergoing major joint arthroplasty?”
“How would you plan surgery for a Jehovah's Witness patient who needs a high-blood-loss operation and declines allogeneic blood?”
Mnemonics & Memory Aids
3 PILLARS
Hook:PBM = optimise red cell mass, minimise loss, tolerate anaemia.
SAVE BLOOD
Hook:SAVE BLOOD captures the blood-conservation toolkit.
Three pillars
- Optimise red cell mass: treat pre-op anaemia (iron/B12/folate, EPO selected)
- Minimise blood loss: haemostasis, TXA, cell salvage, manage anticoagulants
- Optimise anaemia tolerance: restrictive transfusion, single-unit + reassess
Tranexamic acid
- Antifibrinolytic (lysine analogue); IV and/or topical
- Reduces blood loss + transfusion (arthroplasty/hip fracture/trauma)
- No significant increase in VTE in trials - cornerstone measure
Transfusion & cell salvage
- Restrictive trigger ~70-80 g/L (or symptoms); single units + reassess
- Cell salvage for high-loss cases (revision/spine/pelvis)
- Cell salvage adds little over TXA in PRIMARY arthroplasty (cost)
Jehovah's Witness
- Decline allogeneic + stored autologous blood; respect autonomy
- Often accept cell salvage/fractions in CONTINUITY with circulation (individualise + document)
- Maximise red cell mass (iron/EPO), TXA, haemostasis, lower trigger, senior MDT