Opioid-Sparing | Multiple Drug Classes | Superior Outcomes
- Synergistic effect of multiple analgesics acting at different pain pathways
- Opioid-sparing reduces side effects: PONV, ileus, respiratory depression, sedation
- Preemptive analgesia given before incision reduces central sensitization
- Regional anesthesia is cornerstone for major orthopaedic procedures
- Acetaminophen and NSAIDs are foundation - scheduled, not PRN dosing
- “Multimodal means targeting multiple pain pathways, not just multiple drugs
- “WHO ladder is outdated - modern approach uses concurrent non-opioid agents
- “Gabapentinoids effective for neuropathic pain but sedation limits use
- “IV acetaminophen no better than oral - save money, use oral when possible
Different targets equal additive effect. Acetaminophen (central COX inhibition), NSAIDs (peripheral COX), gabapentinoids (alpha-2-delta calcium channels), local anesthetics (sodium channels), opioids (mu receptors). Combining these produces superior analgesia with lower doses of each.
30-50 percent opioid reduction achievable with multimodal approach. Benefits: reduced PONV (40 percent reduction), faster return of bowel function, less sedation, lower respiratory depression risk, earlier mobilization, shorter hospital stay.
Give analgesics BEFORE surgical incision to prevent central sensitization (wind-up phenomenon). Gabapentin 600-1200mg, acetaminophen 1g, celecoxib 200-400mg given 1-2 hours preoperatively. Reduces postoperative pain scores and opioid requirements.
Gold standard for major procedures. Peripheral nerve blocks (femoral, sciatic, interscalene) or neuraxial (epidural, spinal) provide superior analgesia compared to systemic opioids. Single-shot vs continuous catheter depends on surgery and expected pain duration.
- Mechanism
- Central COX inhibition, serotonergic pathways
- Timing
- 1g every 6 hours scheduled (max 4g per day)
- Key Contraindications
- Severe hepatic impairment
- Mechanism
- Peripheral COX-2 inhibition, reduced prostaglandins
- Timing
- Celecoxib 200mg twice daily or etoricoxib 90-120mg daily
- Key Contraindications
- Active GI ulcer, severe renal impairment, CV disease
- Mechanism
- Alpha-2-delta calcium channel, reduces glutamate release
- Timing
- Gabapentin 300-1200mg preop, then 300mg three times daily
- Key Contraindications
- Severe renal impairment (dose adjustment needed)
- Mechanism
- NMDA receptor antagonist, prevents central sensitization
- Timing
- Low dose 0.1-0.5 mg/kg/hr intraop, 0.1 mg/kg bolus
- Key Contraindications
- Psychosis, uncontrolled hypertension, raised ICP
- Mechanism
- Sodium channel blockade, prevents action potentials
- Timing
- Nerve blocks, local infiltration, wound catheters
- Key Contraindications
- Allergy, local infection at injection site
MULTIMODALPrinciples of Multimodal Analgesia
Hook:MULTIMODAL reminds you that pain management needs multiple approaches, not just morphine!
Overview
Definition
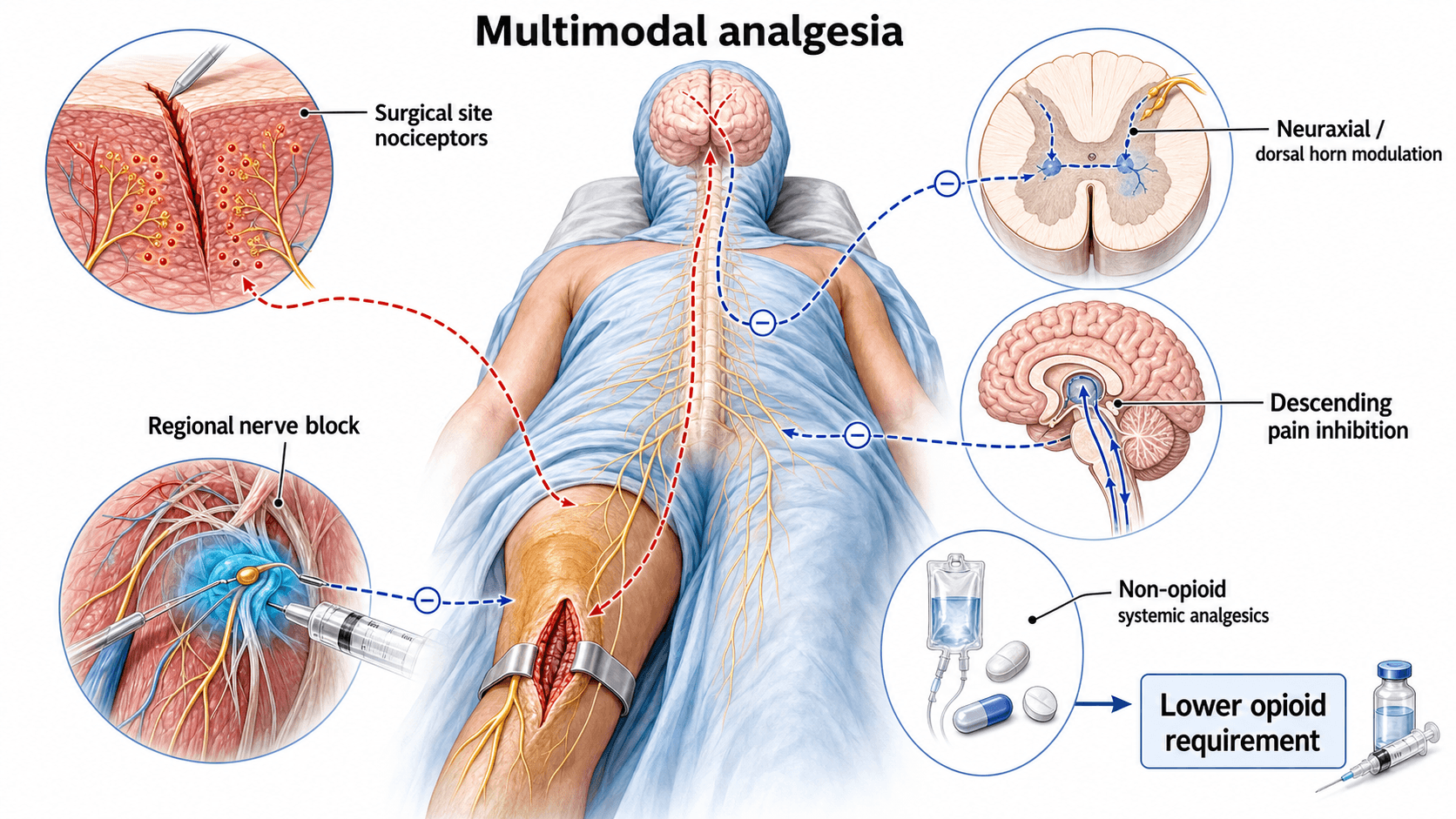
Multimodal analgesia (also called balanced analgesia) is the concurrent use of multiple analgesic agents with different mechanisms of action to target different pain pathways. The goal is to achieve superior pain relief with fewer side effects compared to single-agent therapy, particularly reducing opioid consumption and opioid-related adverse events.
Historical Context
Evolution of pain management:
- 1980s: WHO analgesic ladder (step-wise escalation from non-opioids to strong opioids)
- 1990s: Recognition of opioid side effects and development of multimodal concept
- 2000s: ERAS (Enhanced Recovery After Surgery) protocols incorporating multimodal analgesia
- 2010s: Opioid crisis drives emphasis on opioid-sparing techniques
- 2020s: Standardized multimodal protocols, regional anesthesia expansion, personalized pain medicine
The traditional WHO analgesic ladder suggests sequential escalation (paracetamol, then weak opioid, then strong opioid). Modern multimodal analgesia uses concurrent administration of multiple non-opioid agents, reserving opioids for breakthrough pain only. This paradigm shift has reduced opioid consumption by 30-50 percent in major surgery.
Rationale for Multimodal Approach
Synergistic mechanisms:
- Additive or synergistic effect - drugs acting at different sites produce greater pain relief than sum of individual effects
- Opioid-sparing - reduced opioid requirements decrease side effects (PONV, sedation, respiratory depression, ileus, addiction risk)
- Reduced individual drug doses - lower doses of each agent minimize dose-dependent toxicity
- Comprehensive coverage - addresses nociceptive, inflammatory, and neuropathic pain components
- Prevention of central sensitization - preemptive analgesia reduces wind-up phenomenon
Pathophysiology
Nociceptive Processing
Four-step pain pathway:
- Transduction (peripheral) - noxious stimulus converted to electrical signal at nociceptors
- Transmission (peripheral and spinal) - signal conducted via A-delta and C fibers to dorsal horn
- Modulation (spinal) - signal amplification or suppression at dorsal horn synapses
- Perception (supraspinal) - conscious awareness of pain in thalamus and cortex
Transduction and transmission:
- NSAIDs - reduce prostaglandin synthesis, decrease nociceptor sensitization
- Local anesthetics - block sodium channels, prevent action potential propagation
- Opioids - peripheral mu receptors reduce nociceptor excitability
- Corticosteroids - reduce inflammatory mediator release
Modulation and perception:
- Acetaminophen - central COX inhibition, serotonergic pathways
- Gabapentinoids - reduce excitatory neurotransmitter release in dorsal horn
- Ketamine - NMDA receptor antagonism prevents central sensitization
- Opioids - spinal and supraspinal mu receptor activation
- Alpha-2 agonists - enhance descending inhibitory pathways
Central Sensitization (Wind-Up)
- Repeated C-fiber stimulation causes progressive amplification of dorsal horn neuron responses
- NMDA receptor activation by glutamate leads to increased excitability
- Results in hyperalgesia (increased pain to noxious stimuli) and allodynia (pain from non-noxious stimuli)
- Persists beyond tissue healing - contributes to chronic pain
- Preemptive analgesia - administer analgesics before surgical incision
- NMDA antagonists - low-dose ketamine during surgery
- Gabapentinoids - reduce glutamate release
- Adequate regional anesthesia - complete afferent blockade prevents sensitization
Preemptive equals given before incision. Preventive equals given before incision AND continued postoperatively. Evidence suggests preventive (extended duration) is more effective than single preoperative dose. The key is preventing central sensitization throughout the entire nociceptive period.
The wind-up discussion above explains acute sensitisation; the examinable downstream consequence is chronic (persistent) postsurgical pain (CPSP), which the topic otherwise only alludes to:
- Definition: pain persisting beyond the expected healing period (conventionally more than 3 months) after surgery, not explained by another cause, and often carrying a neuropathic component. It is common - after total knee arthroplasty roughly 10-20 percent of patients report persistent pain.
- Risk factors (the predictable ones): severe, poorly-controlled acute postoperative pain, pre-operative pain and pre-operative opioid use, psychological factors (catastrophising, anxiety, depression), nerve injury during surgery, and female sex/younger age in some series.
- What actually prevents it (and what does not): the strongest levers are excellent acute pain control and regional anaesthesia that blunt central sensitisation, plus addressing psychological risk; low-dose ketamine may reduce it in high-risk/high-pain surgery. Note the negative: gabapentinoids do NOT prevent CPSP (the large meta-analysis found no effect) - do not justify them on this basis.
- The transitional-pain-service concept: identify high-risk patients pre-operatively and follow them across the acute-to-chronic transition, optimising non-opioid analgesia and opioid weaning rather than escalating opioids.
Exam point: define CPSP (pain over 3 months post-surgery, often neuropathic, ~10-20 percent after TKA), name the risk factors (severe acute pain, pre-op pain/opioids, psychological factors, nerve injury), and state that good acute/regional analgesia and ketamine help prevent it while gabapentinoids do not.
Drug Classes and Mechanisms
Acetaminophen (Paracetamol)
- Central COX inhibition - reduces prostaglandin synthesis in CNS
- Serotonergic pathway activation - enhances descending pain inhibition
- Cannabinoid system - possible indirect activation of CB1 receptors
- NO-mediated pathways - may involve nitric oxide signaling
- Adult: 1g PO/IV every 6 hours (maximum 4g per day)
- Elderly or low body weight (less than 50kg): 500-750mg every 6 hours
- Hepatic impairment: reduce dose or extend interval
- NNT for 50 percent pain relief: 4-5 (single 1g dose)
- Opioid-sparing: 20-30 percent reduction in morphine consumption
- Combination with NSAIDs: additive effect, superior to either alone
- IV vs oral: no significant efficacy difference in patients able to take oral
IV acetaminophen costs 10-20 times more than oral with no proven superiority in analgesia when oral route available. Reserve IV for patients who are NBM, have GI dysfunction, or require immediate effect. Switch to oral as soon as feasible.
Contraindications and cautions:
- Severe hepatic impairment (Child-Pugh C) - contraindicated
- Chronic alcohol use - reduce maximum daily dose to 2-3g
- Glutathione depletion states - malnutrition, HIV, chronic illness
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Mechanism of action:
- COX enzyme inhibition - reduces prostaglandin synthesis
- COX-1 (constitutive) - gastric protection, platelet function, renal blood flow
- COX-2 (inducible) - inflammation, pain, fever
- Peripheral and central effects - reduce inflammatory sensitization
Classification:
- COX Selectivity
- Non-selective
- Dosing
- 400mg every 6-8 hours (max 2.4g/day)
- Key Advantage
- Short half-life, rapid onset, low cost
- COX Selectivity
- Preferential COX-2
- Dosing
- 50mg every 8 hours or 75mg every 12 hours
- Key Advantage
- Potent analgesia, good toleration
- COX Selectivity
- Selective COX-2
- Dosing
- 200mg twice daily or 400mg preop
- Key Advantage
- Reduced GI bleeding risk, no platelet effect
- COX Selectivity
- Highly selective COX-2
- Dosing
- 90-120mg daily
- Key Advantage
- Once-daily dosing, potent
- COX Selectivity
- Non-selective (IV)
- Dosing
- 10-30mg every 6 hours (max 5 days)
- Key Advantage
- IV/IM option for NBM patients
- Opioid-sparing: 30-40 percent reduction in morphine consumption
- Combination with acetaminophen: synergistic effect
- COX-2 selective vs non-selective: similar analgesia, reduced GI bleeding with COX-2 (BUT increased CV risk at high doses)
- Active peptic ulcer disease - absolute contraindication for non-selective NSAIDs
- Severe renal impairment (eGFR less than 30 mL/min) - avoid or use cautiously
- History of GI bleeding - use COX-2 selective with PPI
- Cardiovascular disease - avoid high-dose COX-2 inhibitors
- Bleeding risk - non-selective NSAIDs impair platelet function (avoid perioperatively if concern)
- Third trimester pregnancy - risk of premature ductus arteriosus closure
- Aspirin-sensitive asthma - cross-reactivity possible
Concern: NSAIDs may impair fracture healing and spinal fusion. Evidence: Animal studies show delayed healing. Human studies are conflicting - short-term use (less than 2 weeks) appears safe. Current consensus: Avoid NSAIDs in high-risk fractures (scaphoid, femoral neck stress fracture) and spinal fusions. Safe for short-term use in routine arthroplasty and stable fractures.
Gabapentinoids
- Gabapentin - requires dose escalation, three times daily dosing
- Pregabalin - higher bioavailability, twice daily dosing, faster onset
- Alpha-2-delta subunit of voltage-gated calcium channels in dorsal horn
- Reduces calcium influx into presynaptic terminals
- Decreases excitatory neurotransmitter release (glutamate, substance P)
- Prevents central sensitization
- Preoperative: 600-1200mg single dose 1-2 hours before surgery
- Postoperative: 300mg three times daily, titrate to 300-600mg three times daily
- Renal adjustment: reduce dose if CrCl less than 60 mL/min
- Preoperative: 150-300mg single dose 1-2 hours before surgery
- Postoperative: 75mg twice daily, titrate to 150mg twice daily
- Renal adjustment: reduce dose if CrCl less than 60 mL/min
- Large meta-analysis (281 RCTs, 24,682 patients) found the reduction in pain intensity was below the minimally important difference at every timepoint, with no effect on chronic postsurgical pain and increased dizziness/visual disturbance
- Routine perioperative use is no longer supported by high-quality evidence; the historical "25-30 percent opioid-sparing" claim has not held up in pooled data
- Reserve for a genuine neuropathic component (nerve injury, amputation, some spine surgery) on a case-by-case basis
- Respiratory depression risk is the key safety signal, especially combined with opioids in the elderly or those with sleep-disordered breathing
- Sedation (20-30 percent) - dose-limiting, avoid in elderly
- Dizziness (15-20 percent)
- Visual disturbances (blurred vision)
- Peripheral edema
- Cognitive impairment (especially elderly or cognitively impaired)
Best for: Neuropathic pain component (spine surgery, limb amputation, nerve injury). Avoid: Elderly patients, pre-existing cognitive impairment, patients requiring high alertness postoperatively. Alternative: Use lower doses (gabapentin 300mg twice daily) or omit if sedation is concern.
Contraindications:
- Severe renal impairment - dose reduction required (renally cleared)
- Respiratory depression risk - caution when combined with opioids (synergistic respiratory depression)
- Myasthenia gravis - may worsen muscle weakness
Ketamine
- NMDA receptor antagonist - prevents glutamate-mediated excitation
- Prevents central sensitization and wind-up
- Opioid receptor interactions - may reverse opioid-induced hyperalgesia
- Anti-inflammatory effects - modulates cytokine release
- Intraoperative infusion: 0.1-0.5 mg/kg/hr (typical 0.2 mg/kg/hr)
- Bolus: 0.1-0.25 mg/kg IV at induction
- Postoperative infusion: 0.05-0.2 mg/kg/hr for 24-48 hours
- Opioid-sparing: 15-30 percent reduction in morphine consumption
- Most effective in: opioid-tolerant patients, procedures with high pain intensity
- Persistent pain reduction: possible benefit in preventing chronic postsurgical pain
- Psychomimetic effects - dysphoria, hallucinations, nightmares (dose-dependent)
- Nausea - less common than with opioids
- Hypertension and tachycardia - sympathomimetic effects
- Respiratory depression - minimal at low doses
- Psychotic disorders - may precipitate psychosis
- Uncontrolled hypertension - sympathomimetic effects
- Raised intracranial pressure - increases cerebral blood flow and ICP
- Ischemic heart disease - caution due to increased myocardial oxygen demand
Psychomimetic effects occur at doses greater than 1 mg/kg. Analgesia occurs at much lower doses (0.1-0.5 mg/kg/hr infusion). Always use low-dose protocols for postoperative analgesia. Consider benzodiazepine (midazolam 1-2mg) if emergence phenomena occur.
Local Anesthetics
Mechanism of action:
- Sodium channel blockade - prevents action potential generation and propagation
- Differential blockade - smaller fibers (pain, autonomic) blocked before motor fibers
- Reversible nerve conduction block
Agents:
- Onset
- Fast (5-10 min)
- Duration
- Short (60-120 min)
- Maximum Dose
- 4.5 mg/kg plain, 7 mg/kg with epinephrine
- Onset
- Slow (15-20 min)
- Duration
- Long (4-8 hours)
- Maximum Dose
- 2 mg/kg plain, 3 mg/kg with epinephrine
- Onset
- Moderate (10-15 min)
- Duration
- Long (4-8 hours)
- Maximum Dose
- 3 mg/kg
- Onset
- Slow (15-20 min)
- Duration
- Long (4-8 hours)
- Maximum Dose
- 2.5 mg/kg
- Peripheral nerve blocks - femoral, sciatic, interscalene, adductor canal, TAP block
- Neuraxial techniques - spinal, epidural analgesia
- Local infiltration - wound infiltration, intra-articular injection
- Continuous catheters - peripheral nerve catheters, wound catheters
- CNS toxicity - tinnitus, metallic taste, perioral numbness, seizures
- Cardiovascular toxicity - arrhythmias, cardiac arrest (bupivacaine most cardiotoxic)
- Treatment: lipid emulsion (Intralipid 20 percent) 1.5 mL/kg bolus, then infusion
Prevention: Aspiration before injection, incremental dosing, stay below maximum dose. Recognition: CNS symptoms (tinnitus, seizures) precede cardiovascular collapse. Treatment: Stop injection, call for help, manage airway/seizures, give Intralipid 20 percent 1.5 mL/kg bolus (repeat if needed), start CPR if arrest occurs.
PANGCore Drug Classes (Foundation)
Hook:PANG is the foundation - these four should be in every multimodal protocol!
Regional Anesthesia Integration
Peripheral Nerve Blocks
TKA, femoral shaft fracture, anterior thigh procedures
excellent quadriceps analgesia
quadriceps weakness (fall risk)
adductor canal block (motor-sparing)
Femoral nerve blocks provide excellent analgesia but cause motor weakness.
Neuraxial Analgesia
- Major spine surgery (multi-level fusion)
- Lower limb surgery with expected severe pain (revision arthroplasty)
- Bilateral lower limb procedures
- Catheter placement: thoracic (T8-L1) or lumbar (L2-L4) depending on surgical level
- Infusion: bupivacaine 0.125-0.25 percent plus fentanyl 2-4 mcg/mL at 4-10 mL/hr
- Duration: 48-72 hours postoperatively
- Superior analgesia compared to systemic opioids
- Bilateral coverage
- Opioid-sparing (60-80 percent reduction)
- Facilitates mobilization and physiotherapy
- Hypotension - sympathetic blockade (manage with fluids, vasopressors)
- Motor blockade - delays mobilization if concentration too high
- Urinary retention - catheter required
- Rare complications: epidural hematoma (1 in 10,000), abscess, permanent neurological injury
High-risk scenarios: traumatic placement, anticoagulation (therapeutic or prophylactic), coagulopathy, spinal abnormalities. Timing: Stop LMWH 12 hours before neuraxial procedure, restart 6-8 hours after catheter removal. Monitoring: check motor/sensory function every 2-4 hours, remove catheter before restarting therapeutic anticoagulation.
The topic flags "rebound pain when the single-shot block wears off" but never gives the solution; the answer is catheters or adjuvants, and the alpha-2 agonist class (listed once under central targets) deserves development:
- Alpha-2 agonists (clonidine, dexmedetomidine): act on descending inhibitory (alpha-2) pathways. Given systemically (dexmedetomidine infusion) they are opioid-sparing and antiemetic but cause bradycardia, hypotension and sedation.
- As perineural block adjuvants they prolong single-shot blocks: perineural dexamethasone and perineural dexmedetomidine each meaningfully extend block and analgesia duration (often by several hours), directly reducing the rebound-pain gap. (IV dexamethasone also prolongs blocks and is the safer route where perineural use is off-label.)
- Other recognised additives: buprenorphine and epinephrine (the latter both prolongs and serves as an intravascular marker).
- The strategic point: the two ways to defeat single-shot rebound are a continuous catheter (gold standard for prolonged severe pain) or a prolonging adjuvant plus pre-emptively starting scheduled oral analgesia before the block regresses - never wait for the patient to wake in agony.
Exam point: to extend a single-shot block and prevent rebound pain, add a prolonging adjuvant (dexamethasone or dexmedetomidine, IV dexamethasone if perineural use is avoided) or place a continuous catheter, and load scheduled non-opioids/opioid before the block wears off; alpha-2 agonists are also a systemic opioid-sparing adjunct limited by bradycardia/hypotension/sedation.
SPINERegional Anesthesia Options
Hook:Think SPINE for regional techniques - they're the backbone of multimodal analgesia!
Procedure-Specific Protocols
Total Knee Arthroplasty (TKA)
- Gabapentin 600mg
- Acetaminophen 1g
- Celecoxib 400mg
- All given 1-2 hours before surgery
- Spinal anesthesia with intrathecal morphine 100-200 mcg OR
- Adductor canal block (motor-sparing, preferred over femoral block)
- Local infiltration analgesia (LIA) - 100 mL ropivacaine 0.2 percent periarticular injection
- Dexamethasone 8mg IV
- Acetaminophen 1g every 6 hours
- Celecoxib 200mg twice daily (or ibuprofen 400mg three times daily)
- Gabapentin 300mg three times daily
- Oxycodone 5-10mg PO every 4 hours PRN (goal less than 30mg per 24 hours)
- Early mobilization (day 0-1)
- Pain scores 3-4 out of 10 at rest, 5-6 with physiotherapy
- Opioid consumption 20-40 mg oral morphine equivalents in first 24 hours
- Mobilization day 0-1
- Discharge day 1-2
Total Hip Arthroplasty (THA)
- Gabapentin 600mg
- Acetaminophen 1g
- Celecoxib 200mg
- Spinal anesthesia with intrathecal morphine 100 mcg OR
- Lumbar plexus block or fascia iliaca block
- Local infiltration around acetabulum and femoral canal
- Dexamethasone 4-8mg IV
- Acetaminophen 1g every 6 hours
- Ibuprofen 400mg every 8 hours
- Oxycodone 5mg PO every 6 hours PRN (goal less than 20mg per 24 hours)
- Mobilization day 0
- Pain scores 2-3 out of 10 (THA generally less painful than TKA)
- Minimal opioid requirement (10-20 mg oral morphine equivalents)
- Mobilization day 0
- Discharge day 1
Differential of the Patient With Uncontrolled Postoperative Pain
Severe pain despite a multimodal regimen is itself a clinical problem with a differential. Do not simply escalate opioids - work through the causes, because several require a specific intervention rather than more analgesia.
- Clues / How to Recognise
- Sudden severe pain as a single-shot block regresses (often 12-24h); dermatomal return of sensation
- Specific Action
- Anticipate with scheduled non-opioids and oral opioid before regression; consider catheter or repeat block
- Clues / How to Recognise
- Pain out of proportion, pain on passive stretch, increasing analgesic demand, tense compartment
- Specific Action
- Surgical emergency - remove dressings, do NOT mask with dense block, urgent compartment pressures and fasciotomy
- Clues / How to Recognise
- New, escalating or localised pain different in character; systemic signs; abnormal wound or imaging
- Specific Action
- Clinical review and imaging; treat the cause rather than uptitrating analgesia
- Clues / How to Recognise
- Known chronic opioid use; diffuse worsening pain despite rising opioid doses
- Specific Action
- Add ketamine, optimise non-opioid and regional components, involve acute pain service
- Clues / How to Recognise
- Burning, shooting, allodynia in a nerve distribution; nerve handled or stretched intra-operatively
- Specific Action
- Trial a gabapentinoid in selected cases, consider lidocaine, escalate to chronic pain team if persistent
- Clues / How to Recognise
- PRN-only prescribing, missed scheduled paracetamol/NSAID, no regional plan
- Specific Action
- Convert to scheduled non-opioids, add regional/LIA, reassess with a validated pain score
- Clues / How to Recognise
- High distress, disproportionate behavioural response, unrealistic pain expectation
- Specific Action
- Reassurance, education, realistic goal-setting; psychological input if persistent
Guidelines, Registries & Global Practice
Global Burden and Why It Matters
Inadequately controlled acute postoperative pain remains common worldwide and is consistently associated with delayed mobilisation, higher complication rates, prolonged stay and an increased risk of persistent postsurgical pain. Major joint arthroplasty volumes are rising globally with ageing populations, so the perioperative analgesic strategy is a high-frequency, high-impact clinical decision in every health system. The shared global driver of the last decade has been opioid stewardship: reducing both inpatient and post-discharge opioid exposure while maintaining function-enabling analgesia. Multimodal, opioid-sparing analgesia embedded within enhanced-recovery pathways is the converged international answer.
Major Guidance, Side by Side
Recommendations from the leading bodies are broadly concordant - paracetamol plus an NSAID/COX-2 backbone, regional or local-infiltration techniques, and opioids reserved as rescue. The main areas of genuine divergence are the role of gabapentinoids and the choice between intrathecal morphine and peripheral techniques.
- Core Recommendation
- For TKA: scheduled paracetamol + NSAID/COX-2, single-shot adductor canal block + periarticular LIA, single IV dexamethasone; opioids as rescue
- Notable Position / Evidence Level
- Procedure-specific systematic-review methodology (Level I synthesis); intrathecal morphine only when block and LIA impossible
- Core Recommendation
- Opioid-sparing multimodal analgesia as one integral element of a wider enhanced-recovery pathway with education and early mobilisation
- Notable Position / Evidence Level
- Multidisciplinary consensus across 17 topics; no single surgical technique independently expedites discharge
- Core Recommendation
- Multimodal regimens to minimise opioid use; preoperative counselling and limits on post-discharge opioid quantity
- Notable Position / Evidence Level
- Strong emphasis on reducing the opioid prescription that seeds long-term use
- Core Recommendation
- Perioperative multimodal analgesia and joint-replacement enhanced recovery; cautions on routine gabapentinoid use and on opioid initiation
- Notable Position / Evidence Level
- UK gabapentinoids reclassified as controlled drugs, reflecting misuse and respiratory-depression concern
- Core Recommendation
- Multimodal analgesia first-line; validated pain assessment (NRS/VAS); realistic expectation-setting and opioid minimisation
- Notable Position / Evidence Level
- Comprehensive graded evidence document used internationally as an acute-pain reference
Convergent Points of International Consensus
- Paracetamol + NSAID/COX-2 is the non-opioid backbone - scheduled, not PRN, unless contraindicated (Ong meta-analysis supports the combination).
- Regional and local-infiltration techniques are central for major joint and limb surgery (adductor canal block + LIA for TKA per PROSPECT).
- Opioids are rescue analgesics, with deliberate limits on post-discharge quantity to reduce persistent use.
- A single intra-operative dose of dexamethasone improves analgesia and reduces PONV and is now widely recommended for arthroplasty.
Genuine Areas of Practice Variation
- Gabapentinoids: historically routine, now discouraged for unselected patients after large meta-analytic data (Verret) showed sub-threshold benefit and real harms; several systems have reclassified them as controlled drugs. Reserve for a clear neuropathic component.
- Intrathecal morphine vs peripheral block/LIA: some centres still use low-dose intrathecal morphine for arthroplasty; PROSPECT positions it as a fall-back when block and LIA are not feasible, partly because of pruritus, urinary retention and delayed respiratory depression.
- Resource setting: in limited-resource environments where ultrasound and catheter services are scarce, reliance shifts toward scheduled oral non-opioids, surgeon-delivered LIA and judicious opioids; ultrasound-guided regional services and acute pain teams are concentrated in higher-resource centres.
Registry and System-Level Evidence
Although multimodal analgesia is not itself tracked by joint registries, the major arthroplasty registries (NJR for England and Wales, AJRR in the USA, AOANJRR in Australia, the Swedish and Norwegian registries, and the New Zealand Joint Registry) document the rise of same-day and short-stay arthroplasty that opioid-sparing multimodal pathways have enabled. Real-time prescription-monitoring systems in several jurisdictions now track perioperative and post-discharge opioid prescribing, reflecting the global shift toward measurable opioid stewardship.
Relevance Across Examinations
Multimodal analgesia is high-yield for every major orthopaedic board (FRCS Tr & Orth, FRACS, EBOT/FEBOT, ABOS, DNB/MS/MCh, SICOT). Examiners reliably probe: the rationale for opioid-sparing, the non-opioid backbone, procedure-specific regional choices (adductor canal block vs femoral block, interscalene for shoulder), the NSAID-and-bone-healing controversy, the modern retreat from routine gabapentinoids, and recognition of the patient whose pain signals a complication rather than under-dosing.
MCQ Practice Points
Q: What is the primary mechanism of analgesia achieved by preoperative paracetamol administration?
A: Central COX-2 inhibition in the spinal cord and descending serotonergic pathways. Paracetamol is NOT peripherally anti-inflammatory but provides central analgesia by inhibiting prostaglandin synthesis in the CNS. Maximum dose 4g/day (reduce to 3g/day if liver disease or weight under 50kg). Can be given IV or oral with equal efficacy.
Q: Which injectable COX-2 selective NSAID is used perioperatively and what are its key contraindications?
A: Parecoxib 40mg IV (the prodrug of valdecoxib) is a parenteral COX-2 selective inhibitor useful when the oral route is unavailable. Key contraindications: sulfonamide allergy, established cardiovascular disease (raised MI and stroke risk - the reason rofecoxib was withdrawn), renal impairment (GFR under 60), active GI ulceration, and aspirin-sensitive asthma. Use caution with anticoagulation. The bone-healing concern remains low-quality and largely animal-derived; short-term use (under 14 days) appears acceptable in most cases.
Q: What is the opioid-sparing effect of a well-designed multimodal analgesia protocol?
A: 30-50% reduction in opioid consumption. A typical ERAS multimodal protocol includes: preoperative paracetamol 1g + gabapentin 300mg, intraoperative local infiltration analgesia (LIA), postoperative regular paracetamol + NSAID + low-dose opioid PRN. The synergistic effect of targeting multiple pain pathways reduces opioid requirements and associated complications (nausea, constipation, respiratory depression).
Q: What is the mechanism of gabapentin in multimodal analgesia and what is the optimal dosing strategy?
A: Gabapentin inhibits alpha-2-delta voltage-gated calcium channels, reducing central sensitization and hyperalgesia. For perioperative use: single preoperative dose of 300-600mg given 1-2 hours before surgery. Reduces acute postoperative pain scores and opioid requirements by approximately 30%. Avoid high doses (over 600mg) due to sedation, especially in elderly. Contraindicated in renal impairment.
Q: What are the key components of local infiltration analgesia (LIA) used in total knee arthroplasty?
A: Typical LIA cocktail contains ropivacaine 200mg (or bupivacaine 100mg) + ketorolac 30mg + adrenaline 0.3mg in saline 100-150mL. Injected into the posterior capsule, collateral ligaments, quadriceps, and subcutaneous tissues before closure. Provides 12-24 hours analgesia. Adductor canal block provides additional analgesia while preserving quadriceps strength for early mobilization (preferred over femoral nerve block).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are planning anesthesia for a 68-year-old woman undergoing primary total knee arthroplasty. She has well-controlled hypertension and takes aspirin for cardiovascular prophylaxis. Describe your multimodal analgesia plan.”
“A 45-year-old man with chronic low back pain on long-term opioids (oxycodone 40mg twice daily) requires lumbar spinal fusion L4-S1. How would you manage his perioperative analgesia?”
“The orthopaedic surgeon asks you not to use NSAIDs in a patient undergoing open reduction and internal fixation of a scaphoid nonunion as he is concerned about fracture healing. What is your response?”
Definition and Principles
- Multimodal equals concurrent use of multiple analgesics with different mechanisms targeting different pain pathways
- Goal: superior analgesia with reduced opioid consumption and fewer side effects
- Synergy - additive or synergistic effect greater than sum of individual agents
- Opioid-sparing achieves 30-50 percent reduction in opioid use with improved outcomes
Core Drug Classes (Foundation)
- Acetaminophen 1g every 6 hours - central COX inhibition, foundation of all protocols
- NSAIDs - celecoxib 200mg twice daily or ibuprofen 400mg three times daily
- Gabapentinoids - gabapentin 300-600mg three times daily or pregabalin 75-150mg twice daily
- Regional anesthesia - peripheral nerve blocks or neuraxial (gold standard)
- Opioids - rescue therapy only, NOT primary analgesic
Preemptive Analgesia
- Give BEFORE surgical incision to prevent central sensitization (wind-up)
- Gabapentin 600-1200mg given 1-2 hours preoperatively
- Acetaminophen 1g and celecoxib 200-400mg preoperatively
- Mechanism - prevents NMDA receptor activation and dorsal horn sensitization
Regional Anesthesia Options
- TKA - adductor canal block (motor-sparing) or spinal plus intrathecal morphine
- THA - spinal plus intrathecal morphine or fascia iliaca block
- Shoulder - interscalene block (gold standard, but 100 percent phrenic palsy)
- Spine fusion - ketamine infusion plus local infiltration
- Single-shot vs catheter - single shot lasts 12-24h, catheter for 48-72h
Adjuvant Agents
- Ketamine 0.1-0.5 mg/kg/hr intraoperatively - NMDA antagonist
- Dexamethasone 4-8mg IV - anti-inflammatory, antiemetic
- Local infiltration - surgeon performs periarticular injection
- Lidocaine infusion - emerging evidence for 1 mg/kg/hr for 24h
Opioid-Sparing Benefits
- PONV reduced by 40 percent
- Ileus - faster return of bowel function (6-12 hours earlier)
- Sedation reduced by 30 percent
- Respiratory depression reduced by 50 percent
- Length of stay reduced by 0.5-1 day
NSAID Controversy
- Animal studies - NSAIDs delay fracture healing (high doses, prolonged use)
- Human studies - conflicting, short-term use (less than 2 weeks) appears safe
- Avoid in - scaphoid fractures, femoral neck stress fractures, spinal fusions
- Safe in - arthroplasty, routine stable fractures (5-7 days duration)
Special Populations
- Elderly - reduce doses by 25-50 percent, avoid gabapentinoids
- Opioid-tolerant - continue baseline opioid, add ketamine, expect 50-100 percent higher needs
- Renal impairment - avoid NSAIDs if eGFR less than 30, reduce gabapentin dose
- Chronic pain - high-dose gabapentinoids, ketamine, early pain team involvement
TKA Protocol (Example)
- Preop - gabapentin 600mg, acetaminophen 1g, celecoxib 400mg
- Intraop - adductor canal block plus LIA plus dexamethasone 8mg IV
- Postop - acetaminophen 1g every 6 hours plus celecoxib 200mg twice daily
- Breakthrough - oxycodone 5-10mg every 4 hours PRN (goal less than 30mg in 24 hours)
High-Yield Numbers
- Opioid reduction - 30-50 percent achievable with multimodal approach
- PONV reduction - 40 percent compared to opioid-based analgesia
- Acetaminophen max dose - 4g per day (reduce to 2-3g in liver disease)
- Gabapentin preoperative - 600-1200mg
- Ketamine low dose - 0.1-0.5 mg/kg/hr
- Intrathecal morphine - 100-200 mcg for lower limb surgery
Evidence Base
Kehlet & Dahl: The Concept of Balanced (Multimodal) Analgesia
- Defining paper that introduced the concept of balanced (multimodal) analgesia into clinical practice
- Proposed combining analgesics with different mechanisms (local anaesthetics, NSAIDs, opioids, alpha-2 agonists) to obtain additive or synergistic relief
- Argued that combination therapy allows lower doses of each agent and therefore fewer dose-dependent side effects
- Set the rationale for opioid-sparing perioperative regimens that underpins modern ERAS pathways
PROSPECT Recommendations for Pain Management After TKA
- Analysed 151 systematic reviews and 106 RCTs that met PROSPECT inclusion criteria
- Recommends basal paracetamol plus an NSAID or COX-2-specific inhibitor as the foundation
- Recommends a single-shot adductor canal block plus periarticular local infiltration analgesia together with a single intra-operative dose of IV dexamethasone
- Intrathecal morphine 100 mcg considered only when both adductor canal block and LIA are impossible; opioids reserved as rescue analgesics
Paracetamol Combined With an NSAID Improves Analgesia
- Systematic review of 21 RCTs enrolling 1909 patients across acute pain models
- The paracetamol plus NSAID combination was superior to paracetamol alone in 85 percent of relevant studies and superior to NSAID alone in 64 percent
- Pain intensity and rescue analgesic use were reduced by roughly 35 percent versus paracetamol alone
- Supports paracetamol plus NSAID as the routine non-opioid backbone of multimodal regimens
Perioperative Gabapentinoids: Limited Clinical Benefit
- Very large meta-analysis of 281 RCTs with 24,682 participants
- Reduction in pain intensity was below the minimally important difference at every timepoint (for example 7 of 100 points lower at 24 hours)
- No effect on subacute or chronic postsurgical pain prevention
- Gabapentinoids increased dizziness and visual disturbance, with only a small reduction in PONV
Perioperative IV Ketamine for Acute Postoperative Pain (Cochrane)
- Cochrane review of 130 RCTs with 8341 participants
- Reduced 24-hour opioid consumption by about 8 mg morphine equivalents (roughly 19 percent) and 48-hour consumption by about 13 mg
- Reduced pain at rest and on movement and prolonged time to first analgesic request by around 54 minutes
- Reduced PONV and reduced the area of postoperative hyperalgesia, with no clinically important excess of CNS adverse events at sub-anaesthetic doses
Local Infiltration Analgesia (LIA): The Originating Series
- Described the LIA technique (ropivacaine, ketorolac and adrenaline infiltrated systematically around the surgical field) in 325 hip and knee arthroplasty patients
- Two-thirds of patients required no morphine for postoperative pain control
- Most patients mobilised with assistance 5-6 hours after surgery and achieved independent mobility within 13-22 hours
- 71 percent were discharged directly home after a single overnight stay
Adductor Canal vs Femoral Nerve Block for TKA
- Meta-analysis comparing adductor canal block with femoral nerve block for TKA
- Adductor canal block provides comparable (non-inferior) analgesia
- Quadriceps strength is better preserved with the adductor canal block, supporting safer early mobilisation
- No clinically important difference in pain scores or opioid consumption between the two blocks
NSAIDs and Bone Healing: The Evidence Is Weak
- Clinical studies reporting that NSAIDs impair bone healing had significantly lower methodological (Coleman) scores than studies finding them safe
- Reviews recommending NSAID avoidance cited far fewer clinical studies than reviews concluding NSAIDs were safe
- No consensus exists on NSAID safety after orthopaedic procedures; the strongest concern derives from animal data
- Withholding NSAIDs has no proven benefit and may increase opioid requirements
ERAS Society Consensus for Hip and Knee Replacement
- Multidisciplinary consensus across 17 perioperative topic areas for hip and knee replacement
- Best practice combines preoperative education, optimised anaesthetic and transfusion strategy, an opioid-sparing multimodal analgesic approach and early mobilisation
- Insufficient evidence that any single surgical technique independently expedites discharge
- Frames multimodal opioid-sparing analgesia as an integral component of enhanced recovery, not a stand-alone intervention