Wells Score | D-dimer + Ultrasound | Anticoagulation 3-6 Months
- Wells score stratifies pretest probability - guides D-dimer use
- D-dimer has HIGH sensitivity but LOW specificity - rules OUT if negative + low Wells
- Compression ultrasound is gold standard (95% sensitive for proximal DVT)
- Proximal DVT (popliteal and above) MUST be treated - high PE risk
- Anticoagulate 3 months if provoked (surgery), 3-6 months if unprovoked
- “D-dimer useless if high Wells score - go straight to ultrasound
- “Calf vein DVT (distal) controversial - some treat, some serial ultrasound
- “Postoperative DVT is PROVOKED - lower recurrence risk than unprovoked
- “Rivaroxaban and apixaban do NOT need LMWH lead-in (unlike warfarin)
Wells score only estimates probability. You still need D-dimer or imaging to diagnose. High Wells = skip D-dimer, go to ultrasound.
Postoperative patients often have elevated D-dimer (trauma, surgery, inflammation). Only useful if LOW Wells AND negative D-dimer = excludes DVT.
Proximal DVT (popliteal vein and above) MUST be treated - 10-30% PE risk. Distal (calf) DVT - controversial, some treat, some observe with serial ultrasound.
Provoked (surgery): 3 months. Unprovoked: 3-6 months minimum, consider indefinite if high risk. Weigh recurrence risk vs bleeding risk.
- Wells Score
- 0-1 (Low)
- Next Step
- D-dimer first
- If Positive
- If D-dimer negative - stop. If positive - ultrasound
- Wells Score
- 2 (Moderate)
- Next Step
- D-dimer + ultrasound
- If Positive
- Treat if ultrasound positive
- Wells Score
- 3+ (High)
- Next Step
- Skip D-dimer, go to ultrasound
- If Positive
- Anticoagulate immediately if positive
- Wells Score
- Consider alternative diagnosis
- Next Step
- Assess for heart failure, hypoalbuminemia
- If Positive
- DVT is usually unilateral
Overview and Clinical Significance
Orthopaedic surgery is VERY HIGH RISK for VTE due to: venous stasis (immobility, tourniquet), endothelial injury (surgical trauma), hypercoagulability (inflammatory response). THA and TKA have 40-60% DVT risk WITHOUT prophylaxis.
- Incidence: 1-2 per 1000 population annually
- Ortho surgery: 2-3% WITH prophylaxis
- Peak: Days 7-14 postoperatively
- Location: 80% lower limb, 20% upper limb
- Proximal vs distal: 60% proximal, 40% calf only
- Pulmonary embolism: 10-30% risk
- Post-thrombotic syndrome: 20-50% at 2 years
- Recurrent VTE: 10-30% over 5 years
- Chronic venous insufficiency
- Death from massive PE: 1-5%
Pathophysiology and Virchow's Triad
Virchow's Triad
DVT results from the interplay of three factors (Virchow's Triad):
- Immobility from surgery, anesthesia, bed rest
- Tourniquet use during surgery
- Cast immobilization
- Long-haul flights (economy class syndrome)
- Paralysis (stroke, spinal cord injury)
- Surgical trauma to vessels
- Positioning pressure during surgery
- Central venous catheters
- Previous DVT (vessel damage)
- Inflammatory conditions
- Surgical stress response (tissue factor release)
- Cancer (procoagulant factors)
- Inherited thrombophilias (Factor V Leiden, Prothrombin mutation)
- Acquired states (pregnancy, OCP, HRT)
- Dehydration
Orthopaedic Surgery Risk
- Prolonged immobility (pre-op, intra-op, post-op)
- Direct vascular trauma (hip, knee surgery)
- Cement polymerization (heat, emboli)
- Tourniquet ischemia-reperfusion
- Inflammatory response activating coagulation
- THA: 40-60% DVT, 2-5% PE
- TKA: 40-70% DVT, 2-5% PE
- Hip fracture surgery: 40-50% DVT
- Spine surgery: 15-40% DVT
- Arthroscopy: 2-5% DVT
Orthopaedic surgery involves ALL THREE components of Virchow's triad - stasis (immobility), endothelial injury (surgery), and hypercoagulability (inflammatory response). This is why VTE prophylaxis is mandatory.
VTE Prophylaxis in Orthopaedic Surgery
Because the unprophylaxed risk is so high, prophylaxis - not just treatment - is the dominant orthopaedic VTE exam theme. It combines mechanical and pharmacological measures with early mobilisation, risk-stratified against bleeding.
- Examples
- Intermittent pneumatic compression (IPC), graduated compression stockings, venous foot pumps
- Duration / note
- Start peri-operatively; useful when bleeding risk is high or as an adjunct; combine with early mobilisation
- Examples
- Enoxaparin
- Duration / note
- Standard pharmacological agent; renally cleared (caution in renal impairment)
- Examples
- Rivaroxaban, apixaban, dabigatran
- Duration / note
- Oral; first-line in many guidelines after hip/knee arthroplasty
- Examples
- Aspirin 81-150 mg
- Duration / note
- Non-inferior extended prophylaxis after THA/TKA (EPCAT II); low cost
- Examples
- TKA vs THA/hip fracture
- Duration / note
- TKA: ~10-14 days; THA and hip fracture: EXTENDED to ~28-35 days
Guidelines differ in emphasis: ACCP/CHEST and NICE favour pharmacological prophylaxis (LMWH or a DOAC) for major lower-limb arthroplasty and hip fracture, with extended duration (~35 days) for hip procedures, whereas the AAOS is more permissive and accepts aspirin (and mechanical methods) as reasonable in standard-risk patients. All agree on risk-stratifying VTE against bleeding, using mechanical methods when bleeding risk is high, and early mobilisation. Hip fracture and THA warrant longer prophylaxis than TKA.
SEEVirchow's Triad for Thrombosis
Hook:SEE why DVT occurs: Stasis, Endothelial injury, Excessive clotting!
Clinical Assessment - Wells Score
Clinical features (pain, swelling, warmth) have LOW specificity - many mimics exist. Wells score improves pretest probability estimation but imaging is required for diagnosis.
- Points
- +1
- Clinical Notes
- Treatment within 6 months or palliative
- Points
- +1
- Clinical Notes
- Plaster cast or bedridden with lower limb paresis
- Points
- +1
- Clinical Notes
- Most ortho patients score this
- Points
- +1
- Clinical Notes
- Palpation of deep veins
- Points
- +1
- Clinical Notes
- Thigh and calf both swollen
- Points
- +1
- Clinical Notes
- Measure 10cm below tibial tuberosity
- Points
- +1
- Clinical Notes
- Confined to symptomatic leg
- Points
- +1
- Clinical Notes
- Non-varicose
- Points
- +1
- Clinical Notes
- Prior confirmed DVT
- Points
- -2
- Clinical Notes
- Cellulitis, Baker cyst, muscle strain
Wells Score Interpretation
- Probability
- Low (unlikely)
- DVT Prevalence
- 5%
- Next Step
- D-dimer - if negative, stop; if positive, ultrasound
- Probability
- Moderate
- DVT Prevalence
- 17%
- Next Step
- D-dimer AND ultrasound
- Probability
- High (likely)
- DVT Prevalence
- 53%
- Next Step
- Proceed directly to ultrasound (skip D-dimer)
CAPSBEDWells Score for DVT
Hook:Remember CAPSBED to calculate Wells score - Cancer, Active immobility, Prior DVT, Swelling, Bedridden, Enlarged calf, and Deduct 2 if alternative diagnosis!
Diagnostic Investigations
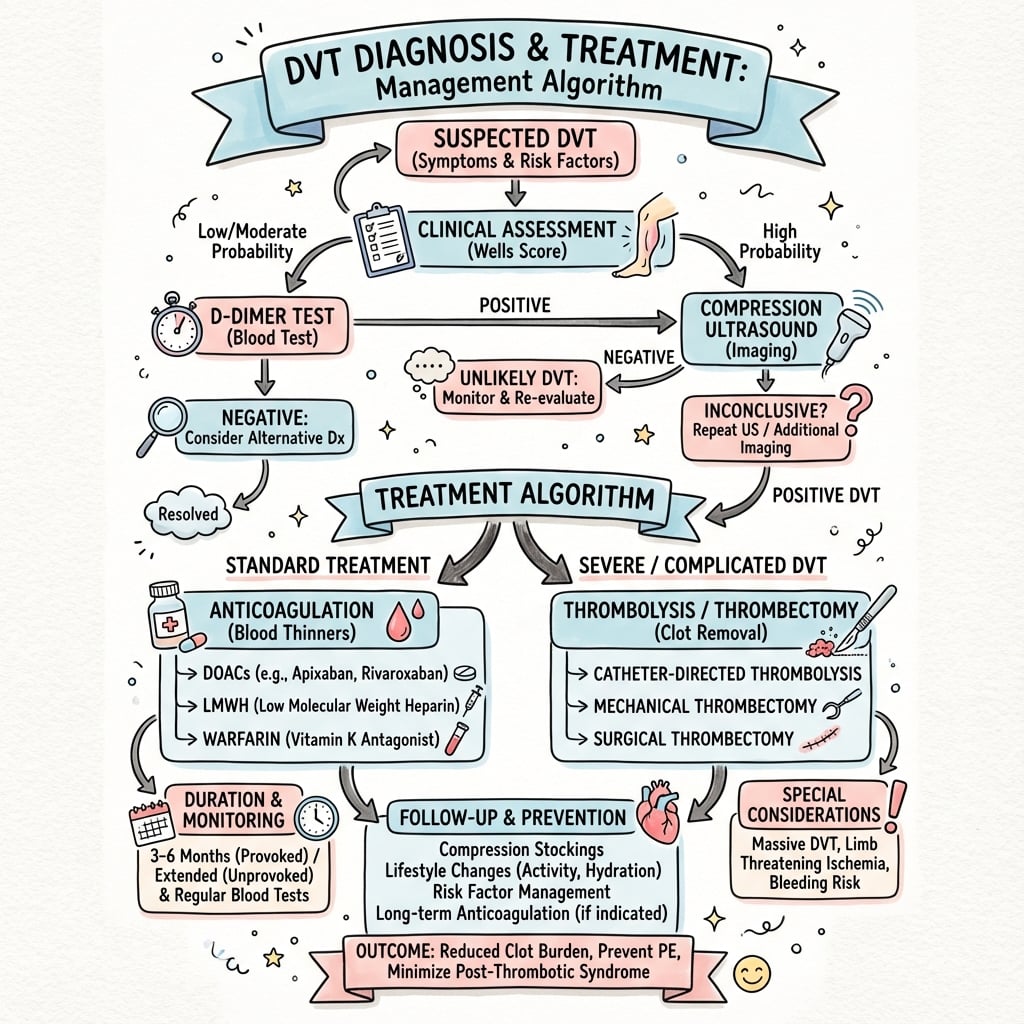
DVT Diagnostic Algorithm
Use clinical features to calculate Wells score (0-1 Low, 2 Moderate, 3+ High). This determines next step.
If Wells 0-1 (Low), check D-dimer. If NEGATIVE - DVT excluded (99% NPV). If POSITIVE - proceed to ultrasound.
If Wells 3+ (High), D-dimer has low utility - go directly to compression ultrasound. Start empiric anticoagulation if delay expected.
Proximal leg vein ultrasound (femoral and popliteal veins). If negative but high suspicion, repeat at 7 days. If positive, treat.
D-dimer Testing
Principle: D-dimer is a fibrin degradation product elevated in VTE. High sensitivity (95-98%) but low specificity (40-60%).
- Low Wells score (0-1)
- Negative D-dimer = DVT excluded
- High negative predictive value (99%)
- Avoids unnecessary imaging
- High Wells score (3+) - go to imaging
- Postoperative patients - often elevated
- Cancer, pregnancy, elderly - often elevated
- Positive D-dimer does NOT diagnose DVT
Interpretation:
- Negative D-dimer + Low Wells: DVT excluded, no further testing
- Positive D-dimer: Proceed to ultrasound (does NOT confirm DVT)
- In postop ortho patients: Often falsely elevated - limited utility
The key point is that D-dimer is a rule-out test only, not a diagnostic test.
Ultrasound Imaging




Treatment - Anticoagulation
Once DVT is diagnosed, start anticoagulation immediately (same day). Delays increase PE risk. Choice of anticoagulant depends on patient factors, renal function, and bleeding risk.
- Advantages
- Oral from day 1, no monitoring, no LMWH lead-in
- Disadvantages
- Cost, renal impairment, limited reversal options
- Practice Note
- Globally first-line for non-cancer VTE
- Advantages
- Cheap, reversible, familiar
- Disadvantages
- LMWH injections, INR monitoring, drug interactions
- Practice Note
- Still used where DOAC cost/access is limiting
- Advantages
- No monitoring, safe in cancer
- Disadvantages
- Daily injections, expensive long-term
- Practice Note
- Cancer-associated VTE (CLOT); DOACs now an option (Caravaggio)
- Advantages
- Oral, predictable
- Disadvantages
- Need 5-10d LMWH lead-in, renal clearance
- Practice Note
- Used less than rivaroxaban/apixaban
Direct Oral Anticoagulants (First-Line)
- 15mg BD for 21 days, then 20mg daily
- No LMWH lead-in needed
- Reduce to 15mg daily if CrCl 30-50
- 10mg BD for 7 days, then 5mg BD
- No LMWH lead-in needed
- Reduce to 2.5mg BD if 2 of: age greater than 80, weight less than 60kg, creatinine greater than 133
Oral from day 1, predictable, no monitoring, easier than warfarin.
CrCl less than 30, active bleeding, mechanical valve, antiphospholipid syndrome.
3-3-IDVT Treatment Duration
Hook:3-3-I: 3 months provoked, 3-6 months unprovoked, Indefinite if recurrent or cancer!
Treatment Duration
- Duration
- 3 months
- Rationale
- Transient risk factor removed
- Recurrence Risk
- 1-3% annual recurrence
- Duration
- 3-6 months minimum
- Rationale
- Assess bleeding vs recurrence risk
- Recurrence Risk
- 10% first year, 5% annual after
- Duration
- Indefinite
- Rationale
- High recurrence risk (15% annual)
- Recurrence Risk
- 15% annual if stopped
- Duration
- Indefinite (while cancer active)
- Rationale
- Ongoing hypercoagulable state
- Recurrence Risk
- High recurrence
- Duration
- Variable, often indefinite
- Rationale
- Persistent increased risk
- Recurrence Risk
- Depends on thrombophilia type
DVT occurring after orthopaedic surgery is PROVOKED (transient risk factor). Treat for 3 months only. Lower recurrence risk (1-3% annually) vs unprovoked DVT (10% first year). Do NOT automatically anticoagulate indefinitely.
In unprovoked DVT, positive D-dimer 1 month after stopping anticoagulation predicts higher recurrence risk. May guide decision for extended anticoagulation.
Complications of DVT and Anticoagulation
DVT Complications
- Incidence
- 10-30% untreated
- Prevention/Management
- Anticoagulation prevents PE
- Incidence
- 20-50% at 2 years
- Prevention/Management
- Compression stockings (debated), early ambulation
- Incidence
- 10% first year (unprovoked)
- Prevention/Management
- Extended anticoagulation if high risk
- Incidence
- Variable
- Prevention/Management
- Compression, elevation
- Incidence
- Rare
- Prevention/Management
- Emergency surgical thrombectomy
Anticoagulation Complications
- Risk
- 1-3% annually
- Management
- Reversal agents, hold anticoagulant
- Risk
- 0.5-1% annually
- Management
- Stop anticoagulation, reversal agent, neurosurgical review
- Risk
- 2-4% annually
- Management
- Endoscopy, reversal, PPI
- Risk
- 1-5% with UFH
- Management
- Stop heparin, use alternative (argatroban, fondaparinux)
- Risk
- Rare (Protein C deficient)
- Management
- Bridge with heparin when initiating warfarin
Phlegmasia cerulea dolens is massive iliofemoral DVT causing limb-threatening ischemia. Features: severely swollen, blue, painful leg with absent pulses. Emergency treatment: anticoagulation +/- surgical thrombectomy or catheter-directed thrombolysis. Fasciotomy if compartment syndrome develops.
Reversal of Anticoagulation
When major bleeding occurs (or urgent surgery is needed), each agent has a specific reversal strategy - examiners expect you to name them.
- Specific reversal
- Idarucizumab (monoclonal antibody fragment)
- Alternative / adjunct
- Haemodialysis (dabigatran is dialysable); activated PCC
- Specific reversal
- Andexanet alfa (recombinant decoy factor Xa)
- Alternative / adjunct
- 4-factor prothrombin complex concentrate (PCC) where andexanet unavailable
- Specific reversal
- 4-factor PCC + intravenous vitamin K
- Alternative / adjunct
- FFP if PCC unavailable (slower, volume load)
- Specific reversal
- Protamine sulfate (full reversal)
- Alternative / adjunct
- Stop infusion (short half-life)
- Specific reversal
- Protamine (partial, ~60% reversal)
- Alternative / adjunct
- Andexanet not standard; supportive measures
Whatever the agent: stop the anticoagulant, apply local haemostasis and resuscitation, check renal function and the timing of the last dose (DOAC effect falls with time and rises in renal impairment), and consider tranexamic acid as an adjunct. Reserve the specific reversal agents above for life-threatening or critical-site bleeding (e.g. intracranial) or emergency surgery that cannot wait for drug clearance.
Guidelines, Registries & Global Practice
Global Epidemiology
- Population incidence of VTE: approximately 1-2 per 1000 adults annually, rising sharply with age (over 5 per 1000 above age 80).
- DVT-to-PE ratio: roughly two-thirds of incident VTE presents as DVT alone, one-third as PE with or without DVT.
- Surgical attributable risk: without prophylaxis, venographic DVT after major lower-limb arthroplasty reaches 40-60%; symptomatic VTE with modern prophylaxis is approximately 1-3%.
- Ethnic variation: VTE incidence is reported lower in East Asian and South Asian populations than in European-ancestry populations, though prophylaxis is still indicated after major orthopaedic surgery.
Side-by-Side Guideline Comparison
- First-line treatment
- DOAC over VKA for non-cancer VTE (Grade 2B)
- Provoked DVT duration
- 3 months
- Compression stockings
- Not routine for preventing PTS (Grade 2B)
- First-line treatment
- Apixaban or rivaroxaban first-line
- Provoked DVT duration
- 3 months (3-6 if active cancer)
- Compression stockings
- Not offered solely to prevent PTS
- First-line treatment
- DOAC preferred unless contraindicated
- Provoked DVT duration
- 3 months for transient provoking factor
- Compression stockings
- Considered for persistent symptoms, not routine
- First-line treatment
- DOAC over VKA; DOAC acceptable in many cancers
- Provoked DVT duration
- 3 months for surgery-provoked
- Compression stockings
- Suggests against routine use
Across ACCP/CHEST, NICE, ESC and ASH the message is consistent: DOACs are first-line for most non-cancer DVT, provoked (surgery-related) DVT is treated for 3 months, and graduated compression stockings are no longer recommended purely to prevent post-thrombotic syndrome. Differences are mostly in emphasis, not direction.
Registry and Surgical-Context Notes
- Arthroplasty registries (NJR England/Wales, AOANJRR Australia, AJRR US, Swedish/Norwegian registries) track symptomatic VTE and 90-day readmission as quality metrics rather than venographic endpoints, reflecting the move to clinically relevant outcomes.
- Aspirin as extended prophylaxis after hip/knee arthroplasty (following a short DOAC lead-in) is supported by EPCAT II and is increasingly reflected in registry-era practice and AAOS/ICM consensus.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: same-day compression ultrasound, age-adjusted D-dimer, and DOAC-based outpatient treatment are standard; many proximal DVTs are managed without admission.
- Limited-resource settings: ultrasound access may be delayed, so empirical LMWH while awaiting imaging is more common; warfarin remains widely used where DOAC cost or INR-monitoring infrastructure dictates, and LMWH may be the only practical option for cancer-associated VTE.
Special Situations
Calf Vein DVT - Controversial Management

Two Approaches:
- Rationale
- Prevent propagation (20-30% propagate to proximal veins)
- Recommendation
- If symptomatic, high risk patients
- Rationale
- Treat only if propagates to proximal veins
- Recommendation
- If asymptomatic, low bleeding risk
Current trend: Serial ultrasound unless high-risk features (extensive thrombus, severe symptoms, active cancer, prior VTE).
Controversies and Areas of Uncertainty
Whether to anticoagulate or perform serial ultrasound remains debated. Trial data (e.g. the CACTUS study) found limited benefit from anticoagulation in low-risk patients, so many guidelines now favour surveillance unless severe symptoms, extensive thrombus, prior VTE, or active cancer are present.
LMWH was the historic standard (CLOT), but Caravaggio and Hokusai-VTE Cancer have shifted practice toward oral apixaban or edoxaban. Residual uncertainty centres on GI/GU tumours, where mucosal bleeding risk may favour LMWH or apixaban over edoxaban/rivaroxaban.
Three months is standard for surgery-provoked DVT, but optimal duration when a transient risk factor coexists with a persisting one (e.g. obesity, prior VTE) is not firmly defined and is increasingly individualised using D-dimer and risk scores.
Routine graduated compression stockings to prevent post-thrombotic syndrome are no longer recommended after the SOX trial. The role of catheter-directed thrombolysis for extensive iliofemoral DVT (ATTRACT trial) is limited to selected younger patients with severe symptoms.
MCQ Practice Points
Q: A patient has Wells score of 1. What is the next appropriate step? A: D-dimer. Low Wells (0-1) = check D-dimer. If negative, DVT excluded. If positive, proceed to ultrasound.
Q: What is the main difference in management between proximal and distal DVT? A: Proximal DVT (popliteal and above) MUST be treated due to 10-30% PE risk. Distal (calf) DVT can be managed with serial ultrasound OR anticoagulation depending on symptoms and risk factors.
Q: What is the main advantage of rivaroxaban and apixaban over warfarin for DVT treatment? A: No LMWH lead-in needed. Rivaroxaban and apixaban can be started orally from day 1, whereas warfarin requires 5-10 days of LMWH bridging.
Q: How long should a post-surgical (provoked) DVT be anticoagulated? A: 3 months. Provoked VTE has low recurrence risk (1-3% annually) after transient risk factor removed.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old woman presents 10 days after total knee arthroplasty with new onset left calf pain and swelling. Her right leg (operated) is also swollen but that is unchanged. Wells score is 2 (surgery less than 12 weeks, calf swelling). How would you investigate and manage?”
“A 72-year-old man with known metastatic prostate cancer presents with entire left leg swelling and pain. He had a previous DVT 2 years ago. Wells score is 5. What is your diagnostic and management approach?”
“A fit 40-year-old man returns 8 days after day-case knee arthroscopy with mild calf discomfort. Ultrasound shows an isolated, non-occlusive thrombus confined to the peroneal (calf) veins, with patent popliteal and femoral veins. He has no prior VTE, no cancer, and no bleeding risk factors. How do you manage him?”
Wells Score (CAPSBED)
- Cancer active +1, Paralysis +1, Prior DVT +1
- Swelling entire leg +1, Bedridden greater than 3d/surgery less than 12wks +1
- Enlarged calf greater than 3cm +1, Differential diagnosis unlikely -2
- Score 0-1 Low, 2 Moderate, 3+ High
Diagnostic Algorithm
- Low Wells (0-1): D-dimer - if negative stop, if positive ultrasound
- High Wells (3+): Skip D-dimer, go to ultrasound
- Ultrasound: Non-compressible vein = DVT
- D-dimer: High sensitivity, low specificity (useless if postop)
Treatment - Anticoagulation
- First-line: DOACs (rivaroxaban 15mg BD x21d then 20mg, OR apixaban 10mg BD x7d then 5mg BD)
- No LMWH lead-in with rivaroxaban/apixaban
- Alternative: LMWH + warfarin (5-10d overlap until INR 2-3)
- Cancer VTE: LMWH preferred (CLOT trial)
Duration of Treatment
- Provoked (surgery): 3 months
- Unprovoked first: 3-6 months minimum
- Recurrent unprovoked: Indefinite
- Active cancer: Indefinite while cancer active
Special Situations
- Distal (calf) DVT: Serial ultrasound OR treat (controversial)
- CrCl less than 30: Cannot use DOACs - use LMWH + warfarin
- Proximal DVT MUST be treated (10-30% PE risk)
- IVC filter: Only if anticoagulation contraindicated
Evidence Base
Wells Clinical Prediction Rule - Pretest Probability for DVT
- Prospective cohort of 593 outpatients with suspected DVT
- DVT prevalence rose with clinical score: 3% (low), 17% (moderate), 75% (high)
- Structured pretest probability plus proximal ultrasound was safe and feasible
- Only 0.6% of those classified as DVT-negative had VTE events over 3 months