Multimodal Approach | Evidence-Based Optimization | Reduced LOS and Complications
- ERAS is multimodal - no single intervention, combination of evidence-based elements
- Patient education is critical - informed patients are more compliant
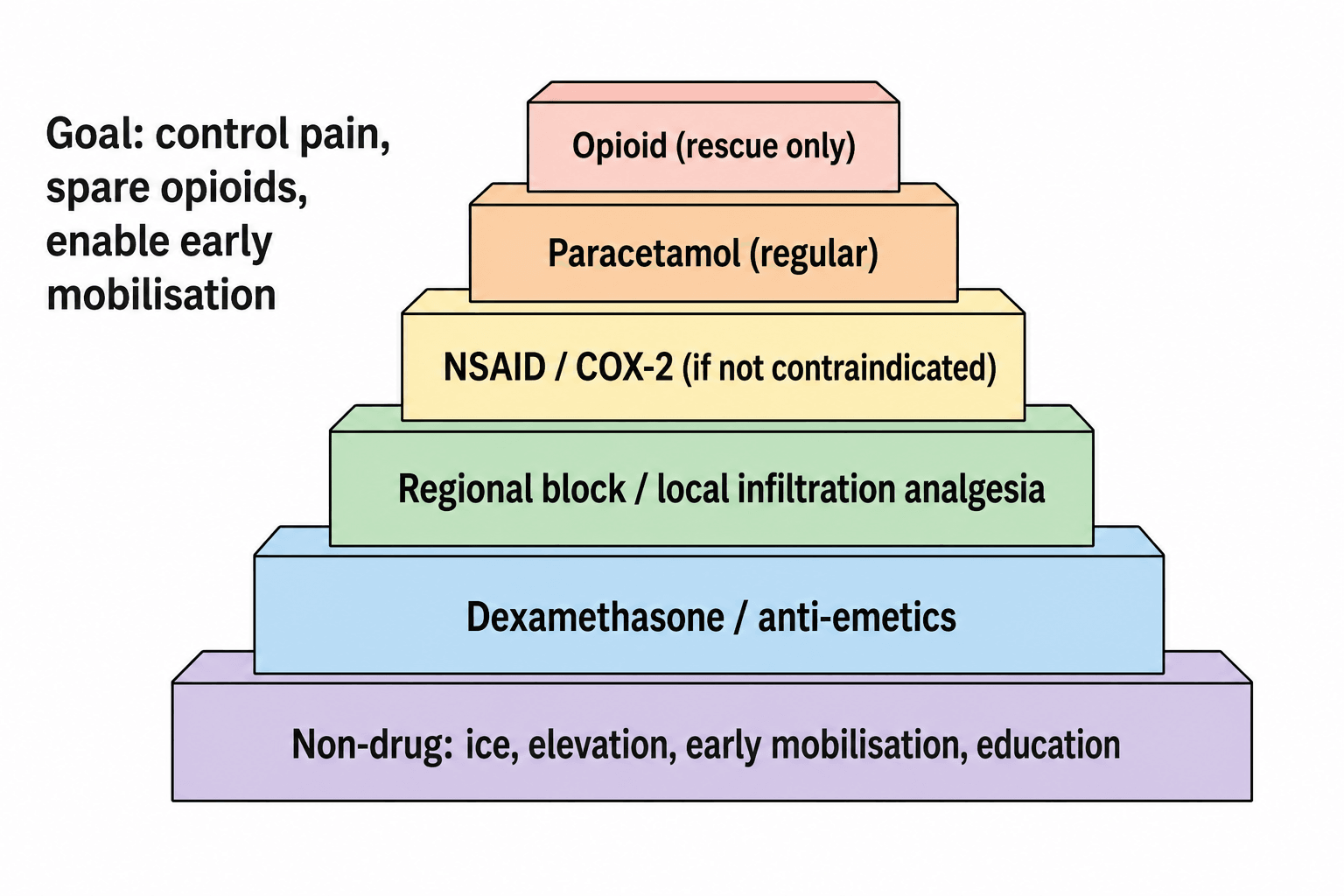
- Multimodal analgesia reduces opioid use by 40-60% (paracetamol, NSAIDs, local infiltration)
- Early mobilization (day of surgery) reduces complications and LOS
- Goal-directed fluid therapy avoids overload and hypovolemia
- Carbohydrate loading 2h preop reduces insulin resistance and catabolism
- “ERAS protocols reduce LOS by 1-3 days in TKA/THA
- “Multimodal analgesia cornerstone: paracetamol + NSAID + local infiltration + opioid-sparing
- “Tranexamic acid reduces blood loss by 30-50% in arthroplasty
- “Prehabilitation improves outcomes in frail/elderly patients
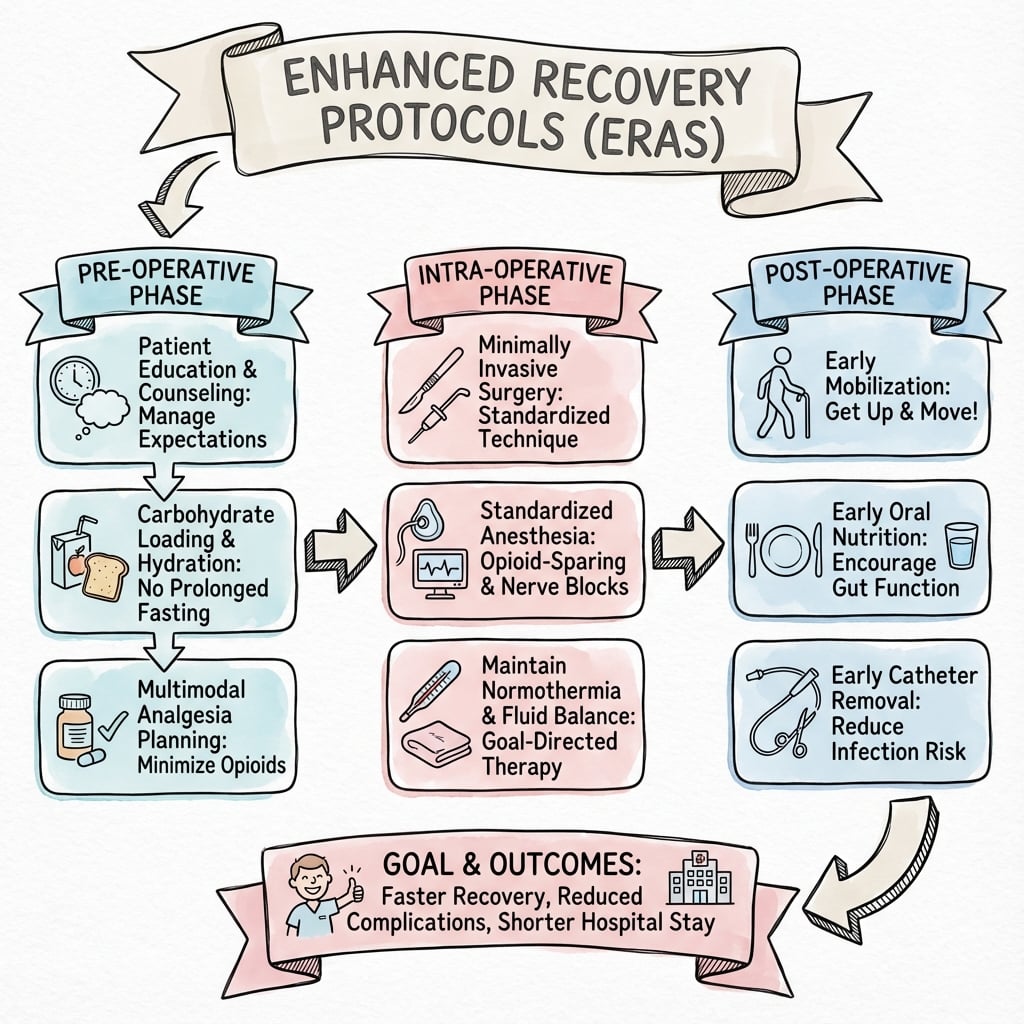
ERAS is NOT a single intervention - it is a comprehensive, evidence-based bundle of interventions spanning preoperative, intraoperative, and postoperative phases. Typical protocols include 15-24 elements. Success requires multidisciplinary team coordination.
Cornerstone of ERAS: Combination of paracetamol (1g QID), NSAIDs (celecoxib 200mg BD or parecoxib IV), local infiltration analgesia (LIA), and opioid-sparing adjuncts (gabapentin, dexamethasone). Reduces opioid use by 40-60%.
Mobilization on day of surgery is a key ERAS principle. Reduces DVT risk, improves respiratory function, and accelerates functional recovery. Target: walking 4 hours post-THA/TKA. Requires adequate analgesia and patient education.
Goal-directed fluid therapy (GDFT) avoids both hypovolemia and fluid overload. Use cardiac output monitoring or pulse pressure variation. Target: euvolemia. Avoid routine nasogastric tubes and drains that delay mobilization.
- Key Interventions
- Education, carbohydrate loading, no bowel prep, prehabilitation
- Expected Outcome
- Reduced anxiety, optimized physiology
- Evidence Level
- High (Level I)
- Key Interventions
- Multimodal analgesia, GDFT, normothermia, TXA, minimally invasive
- Expected Outcome
- Reduced surgical stress response
- Evidence Level
- High (Level I)
- Key Interventions
- Early mobilization, oral nutrition, multimodal analgesia, avoid drains
- Expected Outcome
- Faster recovery, reduced complications
- Evidence Level
- High (Level I)
- Key Interventions
- Continue mobilization, wean opioids, DVT prophylaxis, discharge planning
- Expected Outcome
- Achieve discharge criteria
- Evidence Level
- Moderate (Level II)
OPTIMISEERAS Core Principles
Hook:OPTIMISE your patient for faster recovery and fewer complications
PAIN-FREEMultimodal Analgesia Components
Hook:Keep patients PAIN-FREE with multimodal approach, minimize opioids
PREPAREPreoperative Optimization
Hook:PREPARE the patient thoroughly to reduce surgical stress and complications
MOBILEDischarge Criteria
Hook:Patient must be MOBILE and meet all discharge criteria for safe early discharge
Overview and Epidemiology
Enhanced Recovery After Surgery (ERAS) is a multimodal, evidence-based perioperative care pathway designed to reduce surgical stress, accelerate recovery, and minimize complications. Originally developed for colorectal surgery by Henrik Kehlet in the 1990s, ERAS has been successfully adapted to orthopaedic surgery, particularly total joint arthroplasty.
Historical Development
ERAS evolution in orthopaedics:
- 1990s: Henrik Kehlet develops "fast-track surgery" in colorectal surgery
- 2000s: Principles adapted to THA/TKA in Scandinavia (Husted, Kehlet)
- 2010s: ERAS Society publishes guidelines for various specialties
- 2016: ERAS guidelines for THA/TKA published
- 2020s: Widespread adoption, integration with value-based care
ERAS Society Guidelines
The ERAS Society (International) has published evidence-based guidelines for:
- Total hip arthroplasty (2016)
- Total knee arthroplasty (2016)
- Spine surgery (2019)
- Hip fracture surgery (2019)
Each guideline includes 15-24 evidence-based elements with recommendations graded by level of evidence.
- Evidence-based: Every element supported by research
- Multimodal: No single intervention is sufficient
- Multidisciplinary: Requires team coordination
- Patient-centered: Education and engagement critical
- Length of stay: Reduced by 1-3 days (typical 24-48h discharge)
- Complications: 30-50% reduction in medical/surgical complications
- Readmissions: No increase (some studies show reduction)
- Patient satisfaction: Improved (higher scores)
ERAS accelerates recovery because each element blunts the surgical stress response - the neuroendocrine and inflammatory reaction to tissue injury that drives catabolism and complications. This mechanism is the examiner's favourite 'why'.
- Neuroendocrine limb: afferent nociceptive and inflammatory signals activate the hypothalamic-pituitary-adrenal axis (raised ACTH and cortisol) and the sympathoadrenal system (catecholamines), with ADH and the renin-angiotensin-aldosterone system - producing hyperglycaemia and insulin resistance, protein catabolism (negative nitrogen balance, muscle loss), and sodium/water retention.
- Inflammatory limb: tissue trauma releases cytokines (IL-6 is the principal driver and correlates with the magnitude of injury, with IL-1 and TNF-alpha), producing the acute-phase response (CRP), fever and a degree of immunosuppression that raises infection risk.
- Ebb and flow: a brief early hypometabolic "ebb" phase is followed by a catabolic "flow" phase proportional to the magnitude of surgery.
How ERAS attenuates it: regional/neuraxial anaesthesia and multimodal analgesia block the afferent nociceptive limb; minimally invasive surgery reduces the tissue-injury stimulus; pre-operative carbohydrate loading and early enteral nutrition reduce insulin resistance and catabolism; and normothermia, euvolaemic goal-directed fluids and avoiding prolonged fasting/opioids limit the derangement. The synergistic blunting of this response - not any single element - is why the bundle works. Exam point: ERAS targets the cortisol/catecholamine and IL-6 stress response and its catabolism/insulin resistance, each element addressing a limb of that response.
ERAS Principles and Core Elements
The ERAS Multimodal Approach
Critical concept: ERAS protocols work because of the synergistic effect of multiple evidence-based interventions. Implementing only one or two elements (e.g., just early mobilization) will not achieve full ERAS benefits. Compliance with the complete bundle is essential.
ERAS Elements by Phase
Preoperative Phase (Days to Weeks Before Surgery)
Goal: Optimize patient condition and set expectations
- Intervention
- Written/verbal information, expectation setting
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced anxiety, improved compliance
- Intervention
- Exercise program 4-6 weeks preop
- Evidence Level
- Moderate (Level II)
- Expected Benefit
- Improved functional capacity
- Intervention
- Correct malnutrition, protein supplementation
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced wound complications
- Intervention
- IV iron if Hb under 120-130g/L
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced transfusion need
- Intervention
- Stop 4-6 weeks prior if possible
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced wound/respiratory complications
- Intervention
- Control diabetes, cardiac risk assessment
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced medical complications
- Intervention
- Avoid unless specific indication
- Evidence Level
- High (Level I)
- Expected Benefit
- Reduced dehydration/electrolyte disturbance
- Intervention
- Clear CHO drink 2h before surgery
- Evidence Level
- Moderate (Level II)
- Expected Benefit
- Reduced insulin resistance
Carbohydrate loading involves drinking a clear carbohydrate solution (e.g., 400mL of 12.5% carbohydrate drink) 2 hours before surgery. This reduces the preoperative fasting period, decreases insulin resistance, and reduces postoperative catabolism. Safe in non-diabetic patients. Evidence shows reduced hospital stay and improved patient comfort.
Patient Education Details
- What to expect on day of surgery
- Pain management expectations (realistic goals: VAS 3-4, not 0)
- Mobilization timeline (walking day 0)
- Expected length of stay (24-48 hours for TKA/THA)
- Discharge criteria
- Red flags for complications
- Follow-up plan
- Written information booklets
- Video education
- Group education classes
- One-on-one counseling
Prehabilitation Programs
Components:
- Exercise: Strengthen quadriceps, hip abductors, core
- Aerobic fitness: Walking, cycling to improve cardiovascular reserve
- Education: As above
- Nutrition: Protein supplementation if needed
Duration: Typically 4-6 weeks preoperatively
Evidence: Meta-analyses show modest improvements in functional outcomes, particularly in frail/elderly patients. Effect size greater in patients with poor baseline function.
This completes the preoperative phase overview.
ERAS Application to Orthopaedic Procedures
ERAS for Total Knee and Hip Arthroplasty
Most mature ERAS protocols in orthopaedics, with Level I evidence supporting multiple elements.
The ERAS Society published a multidisciplinary consensus statement for THR and TKR (Wainwright et al., Acta Orthop 2020, available online 2019) covering 17 topic areas of perioperative care. It frames best practice as an opioid-sparing multimodal analgesic approach combined with early mobilisation, optimised education, anaesthetic technique and transfusion strategy. Meta-analytic data (Zhu et al. 2017) show ERAS bundles significantly reduce length of stay and complication rates without increasing readmissions.
Specific Considerations for TKA
- TKA typically more painful than THA in first 24-48 hours
- Multimodal analgesia essential:
- LIA (ropivacaine + ketorolac)
- Adductor canal block (ACB) - preserves quadriceps strength vs femoral block
- Paracetamol + COX-2 inhibitor around-the-clock
- Opioids for breakthrough only
- Straight leg raise by 4 hours post-op
- Walk with walker by 6 hours post-op
- Stairs by day 1
- Discharge day 1-2 if criteria met
- Walking 30m+ with walker
- Stairs (if home has stairs)
- Pain controlled on oral analgesia (VAS under 4)
- No complications (wound, neurovascular)
- Home support adequate
Specific Considerations for THA
- Generally less painful than TKA
- Faster return to mobilization
- Lower DVT risk than TKA
- Traditional approach: Hip precautions (avoid flexion beyond 90�, adduction past midline, internal rotation) for 6-12 weeks
- ERAS approach: No routine precautions if stable implant and adequate soft tissue repair
- Evidence: Randomized trials show no difference in dislocation rate with vs without precautions in primary THA with modern techniques
- Stand and walk by 4 hours post-op
- Independent mobilization with aids by evening of surgery
- Discharge day 1 if criteria met
Evidence for ERAS in TKA/THA
- LOS reduction: Mean 1.5-2.5 days shorter (typical LOS 1-2 days vs 3-4 days traditional)
- Complication reduction: 30-40% reduction in medical complications, 20-30% in surgical complications
- Readmission: No increase (some studies show reduction)
- Cost savings: Significant per-patient savings (from reduced LOS and complications)
- ERAS protocols increasingly adopted by high-volume centers
- No adverse effect on revision rates or patient-reported outcomes
- Association with reduced LOS (registry does not capture LOS, but hospital data shows trend)
This completes the TKA/THA ERAS application.
The natural extension of a mature ERAS pathway is same-day-discharge (day-case/outpatient) hip and knee arthroplasty - increasingly performed and examinable.
- It is the same bundle: multimodal opioid-sparing analgesia, tranexamic acid, spinal anaesthesia with short-acting agents, no drain/no urinary catheter, and day-of-surgery mobilisation - but with discharge on the day of surgery rather than at 1-2 days.
- Patient selection is the safety-critical step: younger, motivated, ASA I-II patients without significant cardiac, pulmonary or obstructive-sleep-apnoea disease or poorly-controlled diabetes, a sensible BMI, low bleeding/VTE risk, and adequate home support with a responsible adult for the first 24 hours; validated tools such as the Outpatient Arthroplasty Risk Assessment (OARA) score aid selection.
- Safeguards: rigorous pre-operative education, a same-day discharge-criteria checklist (mobilising safely, pain controlled on oral analgesia, voiding, no concerning observations), a 24-hour telephone hotline with clear safety-netting, and audited readmission rates.
- Evidence: in well-selected patients, same-day discharge is safe, with readmission/complication rates comparable to inpatient pathways and high satisfaction - but it is not appropriate for the frail, comorbid or poorly-supported patient.
Exam point: day-case arthroplasty is ERAS plus stringent patient selection and safety-netting - the bundle is the same; the difference is who you choose and the support you wrap around same-day discharge.
ERAS Implementation and Challenges
Implementing an ERAS Program
ERAS cannot be implemented by surgeons alone. Success requires buy-in and coordination from anesthesia, nursing, physiotherapy, pharmacy, and hospital administration. A dedicated ERAS coordinator (nurse practitioner or clinical nurse specialist) is critical.
Steps to Implementation
- ERAS champion (surgeon)
- Anesthesia lead
- Nursing manager
- Physiotherapy lead
- Pharmacy
- Hospital administration (for resource allocation)
- Current LOS, complication rates, readmission rates
- Patient satisfaction scores
- Cost per episode
- Review ERAS Society guidelines
- Adapt to local context (resources, patient population)
- Create standardized order sets and documentation
- Didactic sessions on ERAS principles and evidence
- Hands-on training (e.g., LIA technique, nerve blocks)
- Nursing education on early mobilization protocols
- Develop written information booklets
- Create video education modules
- Train staff to deliver consistent messaging
- Select one surgeon or one procedure type (e.g., elective TKA)
- Implement all ERAS elements (not piecemeal)
- Close monitoring and data collection
- Weekly team meetings to review cases
- Identify barriers and solutions
- Adjust protocol as needed
- Expand to all surgeons and procedure types
- Standardize across institution
- Monitor compliance with each ERAS element
- Track outcomes (LOS, complications, readmissions)
- Benchmark against national/international data
- Annual protocol review and updates
Common Barriers and Solutions
- Impact
- Low compliance with protocol
- Solution
- Education, data sharing, involve stakeholders early
- Impact
- Insufficient PT, nursing staff
- Solution
- Business case to administration (cost savings), prioritize resource allocation
- Impact
- Inconsistent protocols
- Solution
- Surgeon champions, peer influence, data showing improved outcomes
- Impact
- Fear of early discharge complications
- Solution
- Clear discharge criteria, 24h hotline, readmission tracking
- Impact
- Different analgesic techniques
- Solution
- Standardized anesthesia protocol, dedicated ERAS anesthesiologists
- Impact
- Early mobilization labor-intensive
- Solution
- Dedicated ERAS nursing team, PT assistants, adjust nurse-patient ratios
Measuring Success - Key Metrics
- Percentage of patients receiving each ERAS element
- Target: Over 80% compliance with all elements
- Length of stay (median and mean)
- Complication rate (medical and surgical)
- Readmission rate (30-day)
- Patient satisfaction scores
- Time to mobilization
- Cost per episode of care
- Savings from reduced LOS and complications
Studies show that compliance with the full ERAS bundle is critical. Implementing only selected elements (e.g., just early mobilization without multimodal analgesia) will not achieve full benefits. Audit and feedback mechanisms are essential to maintain compliance.
Differential Diagnosis: Failure to Progress on an ERAS Pathway
When a patient does not meet discharge criteria on schedule, the key clinical skill is to differentiate the cause - because each has a different fix. Do not simply attribute slow recovery to "the patient"; work through this differential.
- Distinguishing features
- High pain scores at rest/movement, declines physiotherapy, splinting
- Action
- Optimise multimodal analgesia; check LIA/block worked; short opioid rescue
- Distinguishing features
- Drowsy, nauseated, low respiratory rate, constipated, paradoxically still in pain
- Action
- Reduce opioids, switch to multimodal/regional, treat PONV
- Distinguishing features
- Dizziness/syncope on standing, falls hypovolaemic or over-diuresed
- Action
- Reassess fluid balance (GDFT), review antihypertensives, graded mobilisation
- Distinguishing features
- Nausea, vomiting, distension, not tolerating diet
- Action
- Prokinetics, multimodal antiemesis, minimise opioids, mobilise
- Distinguishing features
- Disproportionate pain, swelling, wound discharge, fever, neurovascular change
- Action
- Examine wound/limb, bloods/imaging - exclude haematoma, infection, VTE
- Distinguishing features
- Tachycardia/desaturation (PE, chest infection), confusion (delirium), reduced urine output (AKI)
- Action
- Targeted work-up and treatment; escalate to medical/orthogeriatric team
- Distinguishing features
- Clinically fit but no home support, stairs, or transport
- Action
- Early discharge planning, OT/social work, interim rehabilitation
Management Algorithm
Guidelines, Registries & Global Practice
ERAS is a worldwide standard of perioperative care. The defining international reference is the ERAS Society consensus for THR/TKR (Wainwright et al., Acta Orthop 2020; PMID 31663402), supplemented by ERAS Society guidance for spine and hip-fracture surgery and by national society and registry data.
Global epidemiology and burden
- Hip and knee osteoarthritis is a leading global cause of disability, and arthroplasty volumes are rising worldwide with population ageing - making perioperative efficiency a global priority.
- ERAS bundles consistently reduce length of stay and complications across health systems without increasing readmissions (Zhu et al., Postgrad Med J 2017; PMID 28751437).
Major guidelines, side by side
- Key recommendation
- 17-topic perioperative bundle for THR/TKR: opioid-sparing multimodal analgesia + early mobilisation; no single surgical technique privileged
- Evidence basis
- Consensus of meta-analyses/RCTs (Wainwright 2020)
- Key recommendation
- Routine TXA (topical, IV or oral) in primary TJA to reduce blood loss and transfusion
- Evidence basis
- Strong - network meta-analysis (Fillingham 2018)
- Key recommendation
- Hip-fracture surgery on day of or day after admission (within 36h); orthogeriatric co-management; mobilise day 1
- Evidence basis
- National guideline (observational + RCT data)
- Key recommendation
- Multidisciplinary hip-fracture pathway, prompt surgery, early mobilisation, bone health and falls assessment
- Evidence basis
- National standards (registry-informed)
- Key recommendation
- Endorse multimodal ERAS pathways for elective arthroplasty; regional/LIA analgesia to enable early mobilisation
- Evidence basis
- Consensus / systematic reviews
Registry and audit evidence
- What it captures
- Implant survival and revision rates
- Relevance to ERAS
- ERAS pathways have not been shown to harm revision/survivorship; registries track implant - not LOS - so LOS/complication benefit comes from trials and audits, not registries
- What it captures
- Time to surgery, orthogeriatric input, mobilisation, mortality
- Relevance to ERAS
- Associates timely surgery and orthogeriatric co-management with lower mortality and stay (observational)
- What it captures
- Hip-fracture care standards and outcomes
- Relevance to ERAS
- Drives early surgery, multidisciplinary care and day-1 mobilisation
Joint registries (NJR, AJRR, AOANJRR) measure revision/survival, not length of stay or perioperative complications - so they cannot, on their own, prove ERAS reduces stay. The LOS and complication benefits come from RCTs and meta-analyses (Zhu 2017; Fillingham 2018). For hip fracture, registry data are observational; the HIP ATTACK RCT (Lancet 2020) showed ultra-early surgery does not reduce mortality, so the message is "avoid delay", not "operate fastest".
Global practice variation
- High-resource settings: full multidisciplinary ERAS bundles, day-case/short-stay arthroplasty, regional/LIA analgesia, DOAC or LMWH thromboprophylaxis.
- Limited-resource settings: core, low-cost, high-impact elements remain feasible - patient education, reduced fasting with carbohydrate loading, TXA (cheap and effective), spinal anaesthesia for hip fracture, and early mobilisation - even where cardiac-output monitoring or dedicated ERAS coordinators are unavailable.
- Thromboprophylaxis: choice (aspirin vs LMWH vs DOAC) and duration vary by regional guidance and risk profile; the principle (chemical plus mechanical prophylaxis with early mobilisation) is universal.
MCQ Practice Points
Q: What is the recommended fasting protocol for clear fluids before elective orthopaedic surgery under ERAS guidelines?
A: Clear fluids permitted until 2 hours before anaesthesia (carbohydrate loading drink encouraged 2-3 hours pre-op). Traditional overnight fasting (NPO from midnight) is no longer recommended. Light meal can be taken 6 hours before surgery. Carbohydrate loading reduces insulin resistance, postoperative nausea, and protein catabolism. Does not increase aspiration risk in ASA 1-2 patients.
Q: What are the key elements of an ERAS multimodal analgesia protocol for total knee arthroplasty?
A: Preoperative: paracetamol 1g + gabapentin 300mg + celecoxib 200mg (if no contraindication). Intraoperative: local infiltration analgesia (LIA) or adductor canal block. Postoperative: regular paracetamol + NSAID (short course) + low-dose opioid PRN. Goals: opioid-sparing (reduce by 50%), enable early mobilization, reduce nausea/constipation. Avoid femoral nerve block (delays mobilization due to quadriceps weakness).
Q: What is the evidence for early mobilization in ERAS protocols for hip fracture surgery?
A: Day 1 mobilization (within 24 hours of surgery) reduces: mortality, pneumonia, pressure injuries, VTE, delirium, and length of stay. The UK Blue Book and the ANZHFR (Australian and New Zealand Hip Fracture Registry) recommend mobilization on day 1 post-operatively. Key enablers: adequate analgesia, avoidance of indwelling urinary catheters, physiotherapy assessment, and appropriate weight-bearing instructions.
Q: How does ERAS protocol implementation affect length of stay following primary TKA?
A: Reduces average length of stay by 1.5-2 days (from 3-4 days to 1-2 days) without increasing complications or readmissions. Key ERAS components for TKA: preoperative education, carbohydrate loading, multimodal analgesia, no drains, no urinary catheter, early mobilization (day 0 if afternoon surgery), standardized discharge criteria. Same-day discharge TKA is feasible in selected patients.
Q: What are the standardized discharge criteria in an ERAS protocol for total joint arthroplasty?
A: Functional criteria (not time-based): (1) Pain controlled on oral medications (VAS under 4), (2) Independent mobilization with appropriate aid, (3) Manage stairs if required at home, (4) Independent toileting, (5) Wound satisfactory (no excessive drainage), (6) VTE prophylaxis organized, (7) Patient/family comfortable with discharge, (8) Follow-up arranged. Do NOT base discharge on arbitrary number of nights.
Summary
Enhanced Recovery After Surgery (ERAS) represents a paradigm shift in perioperative care, moving from traditional practices to evidence-based, multimodal protocols that optimize patient outcomes. The success of ERAS lies not in any single intervention, but in the synergistic effect of multiple evidence-based elements implemented as a comprehensive bundle.
- ERAS is multimodal - 15-24 elements across preoperative, intraoperative, and postoperative phases
- Multimodal analgesia is the cornerstone - enables early mobilization and reduces opioid-related complications
- Early mobilization (day of surgery) is critical - reduces DVT, pneumonia, delirium, accelerates recovery
- Multidisciplinary team is essential - cannot be implemented by surgeons alone
- Evidence is strong - Level I evidence for most elements in TKA/THA, growing evidence for spine and hip fracture
- Implementation requires planning - baseline data, education, pilot testing, audit and feedback
- Compliance is key - must implement full bundle, not piecemeal
- TKA/THA: Mature protocols, LOS 24-48h, 30-50% complication reduction
- Spine surgery: Adapted protocols, LOS reduction 1-2d, strongest evidence for elective 1-2 level procedures
- Hip fracture: Emphasis on medical optimization, early surgery (under 36h), delirium prevention
- National and international guidelines inform DVT prophylaxis, antibiotic timing, hip fracture management
- Increasing adoption by major centers worldwide, supported by national specialty societies
ERAS represents the future of perioperative care in orthopaedic surgery, with robust evidence supporting improved outcomes, reduced costs, and enhanced patient satisfaction.
ERAS Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are a consultant orthopaedic surgeon planning to implement an ERAS protocol for total knee arthroplasty in your hospital. What are the key elements you would include, and how would you approach implementation?”
“A 68-year-old woman is undergoing total knee arthroplasty. Describe your multimodal analgesia protocol and the evidence supporting each component.”
“An 82-year-old woman with multiple comorbidities (AF on warfarin, COPD, hypertension) presents with an intracapsular hip fracture. Discuss your perioperative management incorporating ERAS principles.”
Definition and Principles
- ERAS = Enhanced Recovery After Surgery - multimodal, evidence-based perioperative pathway
- Goal: Reduce surgical stress, accelerate recovery, minimize complications
- Core principle: Synergistic effect of multiple interventions (not single intervention)
- Requires multidisciplinary team (surgery, anesthesia, nursing, PT, pharmacy)
- Originally developed for colorectal surgery (Henrik Kehlet 1990s), adapted to orthopaedics 2000s
Key Outcomes
- LOS: Reduced by 1-3 days in TKA/THA (typical 24-48h vs 3-5 days traditional)
- Complications: 30-50% reduction in medical/surgical complications
- Opioid use: 40-60% reduction with multimodal analgesia
- Readmissions: No increase (some studies show reduction)
- Patient satisfaction: Improved
Preoperative Elements
- Patient education (written/verbal, expectation management) - HIGH
- Prehabilitation (4-6 weeks exercise, nutrition) - MODERATE
- Carbohydrate loading (400mL CHO drink 2h preop) - MODERATE
- Anemia correction (IV iron if Hb under 120-130g/L) - HIGH
- Smoking cessation (4-6 weeks prior) - HIGH
- No bowel prep (avoid unless specific indication) - HIGH
Intraoperative Elements
- Multimodal analgesia (paracetamol + NSAID + LIA + nerve block) - HIGH (CRITICAL)
- Tranexamic acid (1-2g IV, reduces blood loss 30-50%) - HIGH
- Goal-directed fluid therapy (euvolemia, avoid overload) - MODERATE
- Normothermia (forced-air warming, warmed fluids) - HIGH
- No routine drains (delays mobilization) - MODERATE
- Antibiotic prophylaxis (within 60min of incision) - HIGH
Postoperative Elements
- Early mobilization (day 0, walking 4h post-op) - HIGH (CRITICAL)
- Early oral nutrition (resume diet day 0) - HIGH
- Multimodal analgesia (continue paracetamol + NSAID, minimize opioids) - HIGH
- DVT prophylaxis (LMWH or DOACs, 10-14d TKA, 28-35d THA) - HIGH
- Avoid urinary catheter (remove day 0-1) - MODERATE
- Multimodal PONV prevention (dexamethasone + ondansetron) - HIGH
Multimodal Analgesia Protocol (TKA/THA)
- Baseline: Paracetamol 1g QID + Celecoxib 200mg BD (or parecoxib IV)
- LIA: Ropivacaine 200mg + ketorolac 30mg + epinephrine infiltrated by surgeon
- Nerve block: Adductor canal block for TKA (preserves quadriceps vs femoral block)
- Adjuncts: Gabapentin 300-600mg single dose preop, dexamethasone 8mg IV
- Opioids: Rescue only (oxycodone IR PRN for breakthrough)
- Result: 40-60% reduction in opioid use, enables early mobilization
Discharge Criteria (MOBILE)
- M - Mobilizing independently (walking 30m+ with aids)
- O - Oral analgesia adequate (VAS under 4, on tablets)
- B - Bowel function normal (passed flatus/BM)
- I - Independent ADLs (or support arranged)
- L - Labs acceptable (no concerning drops in Hb, normal electrolytes)
- E - Education complete (understands red flags, follow-up plan)
Hip Fracture ERAS Specifics
- Early surgery: Target within 36-48h to avoid harmful delay (HIP ATTACK RCT: ultra-early 6h surgery no better than standard timing)
- Orthogeriatrician involvement: From admission (reduces mortality, LOS)
- Fascia iliaca block: Preop analgesia, facilitates assessment
- Spinal anesthesia: Preferred over GA (reduces delirium, respiratory complications)
- Delirium prevention: Minimal opioids, early mobilization, reorientation
- Bone protection: Vitamin D, calcium, fracture liaison service referral
Implementation Essentials
- Multidisciplinary team required (surgery, anesthesia, nursing, PT, pharmacy, admin)
- ERAS coordinator (NP or CNS) critical for success
- Baseline data collection (LOS, complications, costs) before implementation
- Pilot testing (start with one surgeon/procedure, rapid cycle improvement)
- Audit and feedback (monitor compliance with all elements, target 80%+)
- Compliance with full bundle is key - piecemeal implementation ineffective
Evidence Base
- ERAS Society consensus (Wainwright, Acta Orthop 2020): 17 topic areas for THR/TKR
- Zhu meta-analysis (Postgrad Med J 2017): 10 studies/9,936 cases - reduced LOS and complications, no change in readmission
- TXA network meta-analysis (Fillingham, J Arthroplasty 2018): topical/IV/oral TXA all superior to placebo for blood loss and transfusion
- Spine ERAS (Dietz, World Neurosurg 2019): 19 studies - reduced LOS, improved pain, reduced opioids
- Hip fracture timing: NICE within 36h to avoid delay; HIP ATTACK RCT (Lancet 2020) - ultra-early surgery no mortality benefit vs standard
Evidence Base and Key Studies
ERAS Society Consensus for THR/TKR (defining guideline)
- Seventeen topic areas of perioperative care synthesised
- Opioid-sparing multimodal analgesia and early mobilisation are core
- No single surgical technique independently expedites discharge
- Defines the multidisciplinary ERAS bundle for THR/TKR
Multimodal / Fast-Track Surgery (origin of ERAS)
- Coined the multimodal 'fast-track' surgery concept
- Stress-response attenuation underpins accelerated recovery
- Reorganisation of the perioperative team is essential
- Predicted routine 1-2 day stays for major elective surgery
ERAS for Hip and Knee Arthroplasty: Systematic Review and Meta-analysis
- 10 studies, 9,936 arthroplasty cases pooled
- Length of stay significantly reduced (p less than 0.01)
- Total complication incidence reduced (p=0.03)
- No significant change in 30-day readmission (p=0.18)
Tranexamic Acid in Total Knee Arthroplasty: Network Meta-analysis
- 67 studies synthesised for the combined CPG
- Topical, IV and oral TXA all beat placebo for blood loss and transfusion
- No single formulation clearly superior
- Moderate evidence favours pre-incision IV TXA
ERAS for Spine Surgery: Systematic Review
- 19 spine ERAS studies reviewed
- Reduced length of stay in 7 of the studies
- Improved pain scores and reduced opioid use
- No clear reduction in complications or readmissions
Accelerated Surgery vs Standard Care in Hip Fracture (HIP ATTACK)
- 2,970 patients, 17 countries, randomised
- Surgery at 6 h vs 24 h (median)
- No significant mortality reduction (HR 0.91)
- No significant reduction in major complications (HR 0.97)