Joint-Preserving Realignment | Acetabular Dysplasia | Young Adult | Four Osteotomy Cuts | Modified Smith-Petersen | LCEA and Tonnis Correction
- PAO is indicated for symptomatic acetabular dysplasia in the young adult with a congruent joint and preserved cartilage (Tonnis grade 0-1) - it is a joint-preserving realignment, not an arthritis treatment
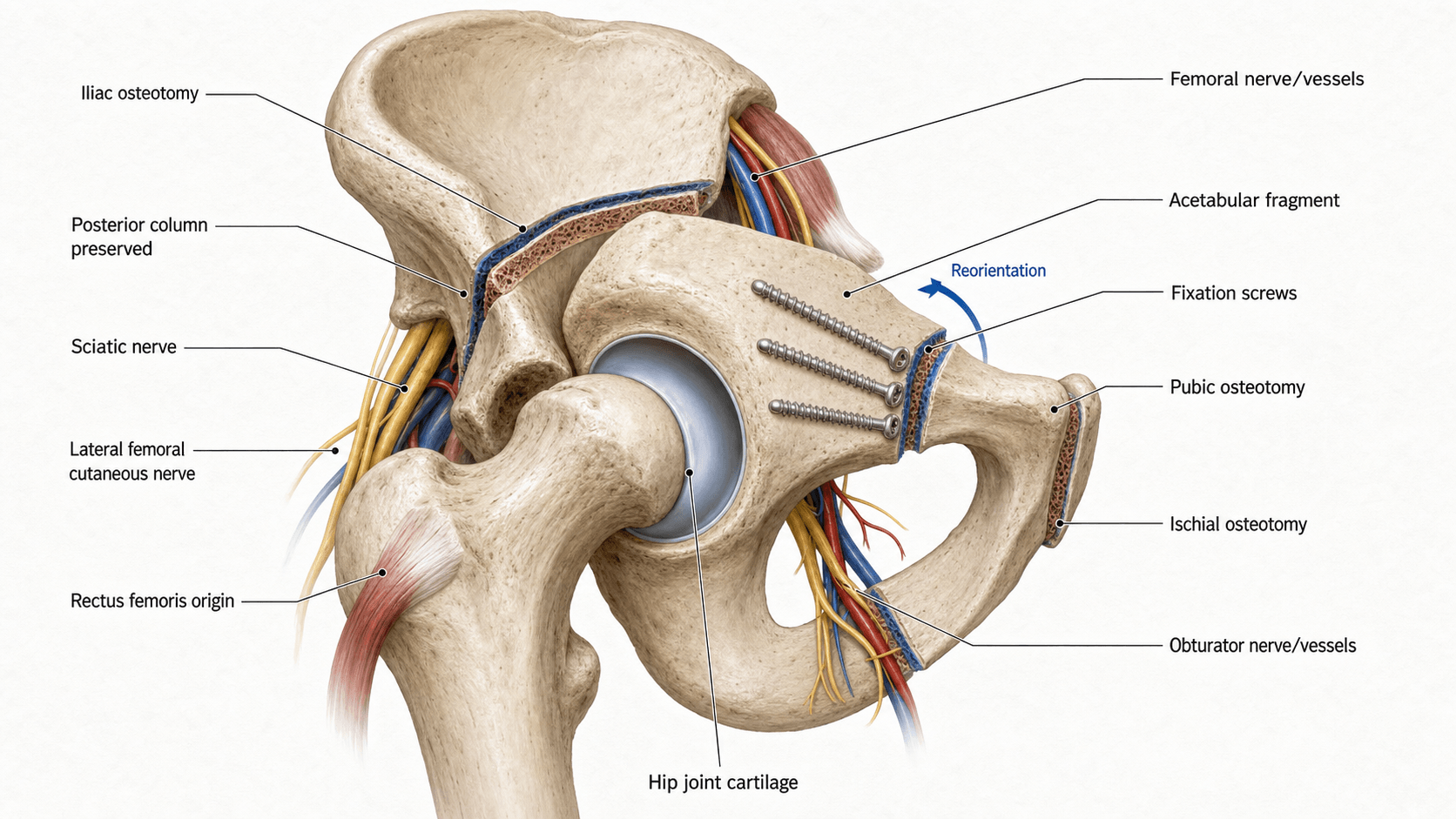
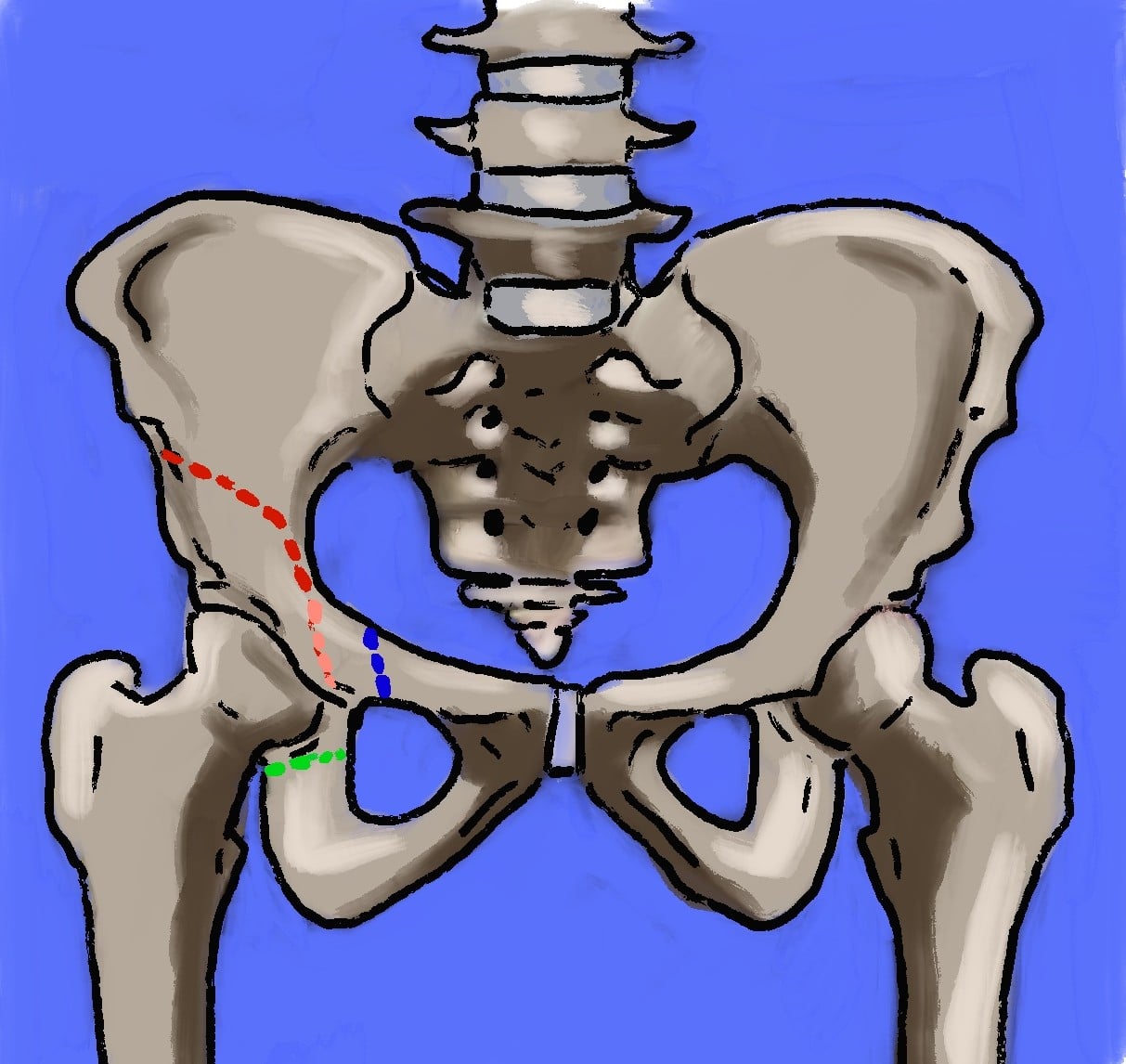
- The Bernese PAO uses four osteotomy cuts (ischial, pubic, iliac, posterior column) to free the acetabulum while maintaining its blood supply via the inferior gluteal artery - this is its key advantage over earlier triple osteotomies
- Correction targets are: LCEA 25-35 degrees, Tonnis angle 0-10 degrees, anterior centre-edge angle (ACEA) greater than 25 degrees - overcorrection risks femoroacetabular impingement (FAI)
- The modified Smith-Petersen (Hueter) approach is most common; the rectus-sparing (Roberge) approach preserves the direct head of rectus femoris and reduces post-operative abductor weakness
- The most feared complications are sciatic nerve injury, intra-articular extension of the osteotomy, and avascular necrosis of the acetabular fragment - meticulous technique and fluoroscopic guidance are essential
- “Always begin a viva answer by confirming the joint is congruent and the cartilage is preserved - PAO fails when arthritis is already established
- “The Bernese PAO differs from triple innominate osteotomy (Tonnis/Steel/Sutherland) because the posterior column remains intact, preserving pelvic stability and allowing immediate mobilisation
- “The LCEA of Wiberg is the single most important radiographic measurement: less than 20 degrees is dysplastic, less than 0 degrees is severe (subluxation), and the target after PAO is 25-35 degrees
- “Intra-operative fluoroscopy with a Judet-type view confirms the correction before definitive fixation - check LCEA, Tonnis angle, and anterior coverage on multiple projections
Periacetabular Osteotomy (Ganz/Bernese PAO)
PAO fails when the joint is incongruent (the femoral head does not sit within the dysplastic acetabulum in a reduced position) or when significant arthritis is present (Tonnis grade 2 or 3, joint space less than 2 mm). Examiners want you to exclude these patients and refer them for THA instead. A 55-year-old with Tonnis grade 3 OA and an incongruent joint needs a THA, not a PAO. PAO is for the young patient with dysplastic anatomy but a preserved, congruent joint that can be salvaged by realignment.
- Best option
- Periacetabular osteotomy (Bernese PAO)
- Reasoning
- Joint-preserving; corrects bony deficiency in all planes; preserves native articular cartilage; allows return to high-level activity
- Best option
- Total hip arthroplasty (THA)
- Reasoning
- Reliable pain relief and function when cartilage is lost; THA in dysplasia may require specialised components (high hip centre, structural graft, cup-cage)
- Best option
- Hip arthroscopy with labral repair
- Reasoning
- Addresses the labral pathology; caution: arthroscopy alone without bony correction in true dysplasia (LCEA less than 18) has high failure rate
- Best option
- Chiari osteotomy or shelf arthroplasty
- Reasoning
- Salvage procedures when PAO is not feasible (non-congruent, neurogenic, or multiply operated hips); provides coverage but not true articular congruity
Overview and Indications
The Bernese periacetabular osteotomy (PAO) is a joint-preserving realignment procedure that reorients the acetabulum to improve femoral head coverage in patients with symptomatic acetabular dysplasia. Developed by Reinhold Ganz and colleagues in Bern, Switzerland, and first described in 1988, the PAO has become the gold standard surgical treatment for acetabular dysplasia in the young adult with a preserved, congruent joint.
dysplasia results in an acetabulum that is too shallow and/or too anteverted, providing inadequate coverage of the femoral head. This concentrates contact pressures on a small area of articular cartilage, leading to labral overload, chondral damage, and premature osteoarthritis. By reorienting the acetabulum, PAO redistributes forces over a larger articular surface area, relieves pain, and aims to delay or prevent the onset of osteoarthritis.
- Posterior column remains intact - preserving pelvic ring stability and allowing early mobilisation
- Large corrections possible in all three planes (lateral coverage, anterior coverage, version)
- Preserved vascularity of the acetabular fragment via the inferior gluteal artery
- No external immobilisation required (unlike some triple osteotomies)
- Spherical acetabulum maintained - the congruent joint remains congruent
- Symptomatic acetabular dysplasia (groin pain, activity-related pain, limp) despite conservative management (activity modification, physiotherapy, NSAIDs)
- Age typically 15-45 years (some centres extend to 50-55 in suitable candidates)
- LCEA less than 20 degrees (dysplastic range) on well-centred AP pelvis radiograph
- Congruent joint - the femoral head reduces into the acetabulum on functional abduction views
- Preserved joint space (Tonnis grade 0 or 1)
- Good range of motion (flexion greater than 90 degrees, minimal fixed deformity)
- Skeletally mature (or near-mature; combined with other procedures in the skeletally immature)
- Realistic expectations and motivation for rehabilitation
- Borderline dysplasia (LCEA 18-25 degrees) with labral pathology requiring bony correction
- Mild coxa valga amenable to combined PAO and varus derotational femoral osteotomy (VDRO)
- Residual dysplasia after prior childhood pelvic osteotomy (salvage PAO, technically demanding)
Examiners test your ability to exclude unsuitable patients. Key contraindications: Tonnis grade 2-3 OA (joint space less than 2 mm), incongruent joint (femoral head does not reduce on abduction views), severe obesity (BMI greater than 35-40), active infection, significant medical comorbidities precluding major surgery, stiff hip (less than 70 degrees flexion), and inflammatory arthritis (RA, ankylosing spondylitis). Patients over 50-55 with OA are better served by THA.
The hardest modern decision is the borderline dysplastic hip (LCEA 18-25 degrees) - is the pain from instability (needs bony coverage, i.e. PAO) or from impingement (a cam lesion treatable by arthroscopy)? Getting this wrong is harmful: isolated arthroscopic rim trimming in a truly unstable borderline hip removes restraint and accelerates failure. Discriminators favouring instability/PAO include a break in Shenton's line, a positive anterior apprehension sign, a hypertrophic labrum or os acetabuli, increased femoral anteversion, and a positive femoro-epiphyseal acetabular roof (FEAR) index - the angle between the acetabular sourcil and the femoral physeal scar, where a value greater than about 5 degrees predicts an unstable hip likely to benefit from PAO, while a low or negative FEAR suggests a stable hip suited to arthroscopic management. Always assess femoral version (CT/MRI) as well: excessive femoral anteversion compounds instability and may warrant a combined femoral derotation osteotomy. Treat the borderline hip on the whole stability picture, not the LCEA alone.
Relevant Anatomy and Biomechanical Principles
- The acetabulum is a hemispherical socket formed by the confluence of the ilium, ischium, and pubis at the triradiate cartilage (fused in adults). In dysplasia, the socket is shallow (under-coverage) and often excessively anteverted.
- The lateral centre-edge angle of Wiberg (LCEA) measures lateral acetabular coverage on an AP pelvis radiograph. Normal is 25-39 degrees; less than 20 degrees is dysplastic; less than 0 degrees indicates severe dysplasia with subluxation.
- The Tonnis acetabular index (acetabular roof angle) measures the slope of the weight-bearing acetabular surface. Normal is 0-10 degrees; greater than 10 degrees indicates acetabular dysplasia (the sourcil slopes upward rather than being horizontal).
- The anterior centre-edge angle (ACEA) of Lequesne and de Seze measured on the false-profile view assesses anterior coverage. Normal is approximately 25 degrees or greater; less than 20 degrees indicates anterior deficiency.
- In a dysplastic hip, the contact area between the femoral head and acetabulum is reduced, leading to elevated contact pressures per unit area of articular cartilage. Pauwels calculated that acetabular dysplasia increases resultant joint forces by reducing the weight-bearing surface.
- Labral overload occurs as the labrum becomes the primary restraint to femoral head subluxation, leading to labral tears, degeneration, and ganglion formation.
- The femoral head may be eccentrically loaded anterosuperiorly, producing a characteristic pattern of anterosuperior chondral wear seen arthroscopically and on MRI.
- Over time, this mechanical overload initiates a degenerative cascade: labral failure, chondral delamination, osteophyte formation, and progressive osteoarthritis.
- The inferior gluteal artery (branch of the internal iliac artery) is the primary blood supply to the mobilised acetabular fragment, entering via the short external rotators and the posterior soft-tissue pedicle. Preservation of this pedicle during the posterior column cut is essential to prevent AVN.
- The superior gluteal artery exits the pelvis via the greater sciatic notch above piriformis and supplies the gluteus medius/minimus; it must be protected during the iliac cut.
- The medial femoral circumflex artery (MFCA) is the primary blood supply to the femoral head; it is not typically at risk during PAO but must be considered if concurrent femoral osteotomy is performed.
- LCEA (Wiberg angle): angle between a vertical line through the centre of the femoral head and a line to the lateral edge of the acetabular sourcil on AP pelvis. Target after PAO: 25-35 degrees.
- Tonnis angle (acetabular index): angle between a horizontal line and a line from the medial to the lateral edge of the acetabular sourcil on AP pelvis. Target after PAO: 0-10 degrees.
- ACEA (Lequesne): measured on the false-profile (Lequesne) view. Target: greater than 25 degrees.
- Shenton's line: should be intact (or nearly so) in a congruent dysplastic hip; broken Shenton's line suggests subluxation.
- Extrusion index: percentage of the femoral head uncovered by the acetabulum; less than 25% is normal.
- Femoroacetabular impingement (FAI) risk: overcorrection of LCEA to greater than 40 degrees or excessive retroversion creates iatrogenic FAI, which is increasingly recognised as a cause of poor outcome after PAO.
The LCEA of Wiberg is the single most tested radiographic measurement in hip dysplasia. Less than 20 degrees = dysplasia. Less than 0 degrees = severe dysplasia with subluxation. Target after PAO: 25-35 degrees. Overcorrection to greater than 40 degrees risks iatrogenic FAI. Always measure on a well-centred AP pelvis (obturator foramina symmetrical, coccyx pointing to symphysis, tip of coccyx 1-2 cm above symphysis).
Internervous Plane and Surgical Interval
The Bernese PAO is performed through one of two main approaches:
- Interval: between the tensor fasciae latae (TFL) (superior gluteal nerve) laterally and the sartorius (femoral nerve) medially - the classic Smith-Petersen internervous plane.
- The lateral femoral cutaneous nerve (LFCN) crosses this interval variable distances below the anterior superior iliac spine (ASIS) and is at risk; it should be identified and protected or intentionally sacrificed if it obstructs the exposure.
- The direct head of rectus femoris arises from the anterior inferior iliac spine (AIIS); in the classic approach it is released or detached to access the anterior column and superior pubic ramus. In the rectus-sparing modification, the rectus is left attached and the exposure proceeds medial to it.
- The hip joint capsule is exposed anteriorly and medially; a limited capsulotomy may be performed for intra-operative arthrotomy to inspect the joint, though many surgeons perform this arthroscopically before the open procedure.
- The iliopsoas tendon is retracted medially; the femoral nerve and vessels lie further medial within the femoral triangle and must be protected.
- This approach accesses the inner table of the ilium and the true pelvis through a medial subperiosteal dissection, preserving the direct head of rectus femoris and minimising abductor disruption.
- The interval is developed between the iliacus (femoral nerve) medially and the gluteal muscles (superior gluteal nerve) on the outer table.
- All four osteotomy cuts are performed from within the pelvis (intra-pelvic), which reduces the risk of intra-articular extension but limits direct visualisation of the lateral ilium.
- The LFCN is still at risk during the superficial dissection.
The lateral femoral cutaneous nerve (LFCN) is injured in approximately 10-30% of PAO cases (neuropraxia or neuroma), causing numbness or dysaesthesia over the anterolateral thigh. It crosses the interval between TFL and sartorius at a variable distance below the ASIS. Patients must be counselled about this risk pre-operatively - it is the commonest nerve complication and is often permanent if the nerve is transected.
Patient Positioning and Setup
- Position: supine on a radiolucent table. The affected leg is draped free to allow full hip range of motion. Some surgeons prefer the lateral decubitus position, but supine is more common for the modified Smith-Petersen approach and facilitates fluoroscopic imaging.
- Anaesthesia: general anaesthesia with or without regional supplementation (lumbar plexus block). Epidural or spinal anaesthesia may be used. Nerve monitoring (sciatic nerve) is employed by some surgeons but is not universal.
- Fluoroscopy: essential. The image intensifier is positioned to obtain AP pelvis, obturator oblique (Judet), and iliac oblique views. Intra-operative assessment of correction requires a true AP pelvis view (symmetrical obturator foramina, coccyx aligned with symphysis) and a false-profile equivalent.
- Pre-operative planning: a well-centred AP pelvis radiograph, false-profile (Lequesne) view, and Dunn/lateral views are mandatory. CT with 3D reconstruction is increasingly used for precise planning of correction in all three planes. The planned correction is templated to achieve LCEA 25-35 degrees, Tonnis angle 0-10 degrees, and ACEA greater than 25 degrees.
- Blood conservation: PAO involves significant blood loss (average 500-1500 mL). Cell saver autotransfusion, tranexamic acid, and controlled hypotensive anaesthesia are commonly employed. Type and crossmatch is mandatory (2-4 units).
- Prophylaxis: pre-operative antibiotics (cefazolin or alternative), thromboprophylaxis (LMWH or mechanical), and heterotopic ossification prophylaxis (indomethacin 75 mg daily for 2-6 weeks) per surgeon preference.
Surgical Technique
The classic PAO approach. A longitudinal incision is made along the iliac crest, curving distally over the ASIS and extending 10-15 cm along the interval between TFL and sartorius (modified Smith-Petersen / Hueter approach). The interval is developed, identifying and protecting the LFCN. The direct head of rectus femoris is released from the AIIS (or preserved in rectus-sparing variants).
The abductor muscles (gluteus medius and minimus) are elevated subperiosteally from the outer table of the ilium, preserving the gluteal tendon attachments. The iliacus is elevated from the inner table. The hip joint capsule is exposed anteriorly and medially. The iliopectineal fascia is divided to access the true pelvis and the superior pubic ramus.
Osteotomy sequence (four cuts):
- Ischial cut: a Ganz osteotome is introduced through the inferior medial aspect of the acetabulum (infra-cotyloid groove) and directed posteriorly toward the infracotyloid notch, partially dividing the ischium under fluoroscopic guidance
- Superior pubic ramus: the ramus is exposed subperiosteally medial to the iliopectineal eminence and osteotomised with a Ganz osteotome or oscillating saw, protecting the obturator nerve and vessels
- Iliac/supra-acetabular cut: a transverse osteotomy from the lateral ilium, directed posteriorly toward the sciatic notch, staying at least 15 mm above the acetabular dome
- Posterior column cut: connects the iliac cut to the ischial cut through the posterior column, completing the mobilisation of the acetabular fragment
The acetabular fragment is then repositioned (typically rotated anterolaterally and medially) to achieve the planned correction. Schanz pins or a T-handle chuck on a threaded pin into the fragment provide control for manipulation. Correction is confirmed fluoroscopically before definitive fixation with 3.5 mm or 4.5 mm cortical screws. Bone graft from the ilium may fill residual gaps.
The osteotomy cuts must remain extra-articular. The supra-acetabular cut should be at least 15 mm above the acetabular dome. If the osteotomy enters the joint, articular cartilage is damaged and the risk of post-traumatic arthritis increases significantly. Fluoroscopic guidance in multiple planes (AP and obturator oblique) is essential during each cut. If joint penetration is recognised, redirect the osteotome or abort that cut and replan.
Structures at Risk and Complications
PAO is a major reconstructive procedure with a significant complication profile. Understanding structures at risk is essential for safe execution and for exam answers.
- Lateral femoral cutaneous nerve (LFCN): the most commonly injured nerve (10-30%); traverses the TFL-sartorius interval. Most result in anterolateral thigh numbness or dysaesthesia; some resolve, others are permanent.
- Sciatic nerve: the most feared nerve injury (1-3%); at risk during the ischial and posterior column cuts, which are performed close to the nerve as it exits the greater sciatic notch. Meticulous subperiosteal dissection and use of Ganz osteotomes (which deflect away from soft tissues) reduce risk. Post-operative sciatic nerve palsy may also result from haematoma compression or excessive limb lengthening.
- Femoral nerve: at risk during medial retraction of the iliopsoas and exposure of the anterior column; neuropraxia is rare but reported.
- Obturator nerve: at risk during the superior pubic ramus cut as it traverses the obturator foramen; protected by subperiosteal dissection.
- Intra-articular extension: the osteotomy enters the hip joint if cuts are placed too close to the acetabulum; reported in approximately 2-5% of cases. Risks chondral damage and post-traumatic arthritis. Requires intra-operative recognition and management.
- Avascular necrosis (AVN) of the acetabular fragment: rare (less than 2%) but catastrophic; caused by disruption of the inferior gluteal artery pedicle during the posterior column cut. The entire acetabular fragment becomes avascular, leading to collapse and necessitating THA.
- Nonunion or delayed union: reported in approximately 2-5% of cases, most commonly at the ischial or pubic osteotomy sites. Smoking is a significant risk factor. Symptomatic nonunion may require bone grafting or revision fixation.
- Heterotopic ossification (HO): reported in 5-20% of cases (most Brooker grade 1-2 and asymptomatic). Prophylaxis with indomethacin or single-dose radiation is used in many centres. Significant HO (grade 3-4) may restrict motion and require excision.
- Loss of correction: migration of the acetabular fragment post-operatively if fixation is inadequate; more common with screw-only fixation than plate-and-screw constructs.
- Overcorrection and iatrogenic FAI: excessive lateral coverage (LCEA greater than 40 degrees) or excessive retroversion creates pincer-type FAI, causing impingement pain and progressive labral damage. This is increasingly recognised as a cause of persistent post-operative pain.
- Wound complications: infection (approximately 1-3%), haematoma, wound dehiscence, and prominent hardware are reported. The anterior approach places hardware in a subcutaneous position.
- Thromboembolic events: DVT/PE risk is approximately 1-3%; routine thromboprophylaxis is recommended.
- Blood loss: average 500-1500 mL; transfusion rates vary from 15-50% depending on technique and blood conservation strategies.
For exams, focus on sciatic nerve injury (the most feared nerve complication, associated with the ischial/posterior column cuts) and AVN of the acetabular fragment (catastrophic if the inferior gluteal pedicle is disrupted). The LFCN is the most common nerve injury but is rarely debilitating. Intra-articular extension is a preventable technical error. Examiners want to see you understand which complications are common versus catastrophic.
Postoperative Care and Rehabilitation
PAO needs no postoperative external immobilisation (a key advantage of the intact posterior column), but protected weight-bearing is essential while the four osteotomies unite.
- Weeks 0-6 (protection): toe-touch or partial weight-bearing (typically around 15-20 kg) with two crutches to protect the ischial and pubic cuts; isometric and gentle active-assisted hip range-of-motion exercises, avoiding active hip flexion against resistance (protecting the rectus/iliopsoas and the anterior fixation). Continue thromboprophylaxis and heterotopic-ossification prophylaxis per unit protocol.
- Weeks 6-12 (progression): confirm early osseous union radiographically, then progress to full weight-bearing over 2-4 weeks and wean the crutches. Begin abductor strengthening (gluteus medius is the key weak link after the approach) with core and gait re-education.
- Months 3-6: restore symmetric strength and a normal gait; low-impact conditioning (cycling, swimming, hydrotherapy) before any impact loading.
- Months 6-12: graded return to running and sport once radiographic union, full pain-free range and near-symmetric abductor strength are achieved.
Unlike some triple osteotomies, PAO needs no cast because the posterior column is intact - but the ischial and pubic osteotomies still take weeks to unite, so the patient is partial/toe-touch weight-bearing for about 6 weeks with restricted active hip flexion, then progressed to full weight-bearing once early union is confirmed. Abductor weakness (from elevating gluteus medius/minimus - less marked with the rectus-sparing approach) is the main rehabilitation focus, and full sporting return typically takes 9-12 months.
Guidelines, Registries and Global Practice
There is no single universal guideline for the management of acetabular dysplasia; practice follows the evidence-based principles of patient selection and correction targets described above. Several international societies have published consensus statements and clinical practice guidelines:
- AAOS (US): the AAOS clinical practice guideline on the treatment of osteoarthritis of the hip (non-arthroplasty) gives a moderate-strength recommendation for periacetabular osteotomy in symptomatic acetabular dysplasia with preserved joint space. The AAOS emphasises shared decision-making and referral to high-volume centres.
- BOA/BSR (UK): national guidance supports referral to specialist young adult hip services for consideration of PAO in symptomatic dysplasia. The Getting It Right First Time (GIRFT) programme in the NHS recommends centralisation of PAO to high-volume units.
- EFORT/European consensus: European practice has strongly favoured PAO since its development in Bern. The European Hip Society has published position statements supporting PAO as the gold standard joint-preserving procedure for acetabular dysplasia, with an emphasis on early intervention before arthritis develops.
- Large national and multicentre registries are increasingly capturing PAO data. The Danish Hip Arthroplasty Register and the Scandinavian PAO collaboration have provided real-world survivorship data, confirming approximately 75-85% 10-year survivorship free of THA in well-selected cohorts.
- Registry data consistently demonstrate that surgeon volume matters: outcomes are better and complication rates lower in centres performing more than 20-30 PAOs per year.
- European centres (particularly Bern, Boston/Copenhagen collaboration, and several German and French centres) have the largest PAO experience globally. The technique was developed in Europe and has been refined over three decades.
- North American adoption has increased significantly since the 2000s, with dedicated young adult hip fellowship training programmes producing surgeons skilled in PAO. However, access remains limited in many regions, with long waiting lists at high-volume centres.
- Asian centres (particularly Japan and Korea) have extensive experience with PAO for developmental dysplasia, which has higher prevalence in many Asian populations.
- In low- and middle-income settings, PAO may be the only joint-preserving option available to young patients with dysplasia, but the technical demands of the procedure limit its availability to major teaching hospitals.
- Approximately 10-25% of PAO patients require THA by 10-20 years, depending on pre-operative arthritis grade.
- THA after PAO is technically more demanding than primary THA due to altered acetabular anatomy (medialised socket, acetabular bone graft, altered version), retained hardware, and possible HO.
- Despite the added complexity, implant survivorship after THA conversion from PAO is generally comparable to primary THA when performed by experienced surgeons.
- Patients should be counselled that PAO aims to delay THA (often by 10-20 years), not necessarily prevent it entirely.
Memory Aids
PACEPatient Selection - PACE
Hook:Only offer PAO when the joint PACEs the criteria: Preserved space, Age appropriate, Congruent, Excellent ROM - the wrong patient is the commonest cause of PAO failure
ISIPThe Four Osteotomy Cuts - ISIP (In Sequence)
Hook:The four ISIP cuts free the acetabulum in sequence: Ischial, Superior pubic, Iliac, Posterior column - the fragment remains vascularised via the inferior gluteal artery pedicle
PAOComplications After PAO - DANGER
Hook:PAO complications cluster around DANGER: Delayed union, AVN, Nerve injury, Graft/hardware, Extra-articular extension (into joint), Reoperation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old recreational runner presents with a 2-year history of progressive right groin pain, worse with prolonged standing and running. She has no history of childhood hip problems. AP pelvis radiograph shows an LCEA of 8 degrees and a Tonnis angle of 18 degrees. The joint space is preserved. The hip is congruent. Discuss your management.”
“A 34-year-old woman had a Bernese PAO performed 18 months ago at an outside hospital for acetabular dysplasia. She reports persistent anterior hip pain with sitting and flexion activities. Post-operative radiographs show an LCEA of 44 degrees and a positive crossover sign. The joint space is preserved. How would you assess and manage her?”
One-liner
- Joint-preserving realignment of the acetabulum for symptomatic dysplasia in the young adult with a congruent, preserved joint
- Developed by Ganz in Bern (1988); four osteotomy cuts mobilise the acetabulum while preserving posterior column continuity and inferior gluteal artery blood supply
Patient selection (PACE)
- Preserved joint space: Tonnis grade 0-1
- Age appropriate: typically 15-45 years
- Congruent joint: femoral head reduces on abduction views
- Excellent ROM: flexion greater than 90 degrees
- Failed conservative management (physio, activity modification, NSAIDs)
Contraindications
- Tonnis grade 2-3 OA (joint space less than 2 mm)
- Incongruent joint (non-reducible femoral head)
- Inflammatory arthritis (RA, ankylosing spondylitis)
- Severe obesity (BMI greater than 35-40)
- Age greater than 50-55 with established arthritis
- Significant medical comorbidities
Radiographic targets
- LCEA: 25-35 degrees (less than 20 = dysplasia; greater than 40 = overcorrection/FAI risk)
- Tonnis angle: 0-10 degrees
- ACEA: greater than 25 degrees (on false-profile view)
- No crossover sign (avoid retroversion)
- Medialisation of hip centre toward normal position
Four osteotomy cuts (ISIP)
- Ischial (infra-cotyloid) - first, from within pelvis
- Superior pubic ramus - second, medial to iliopectineal eminence
- Iliac/supra-acetabular - third, at least 15 mm above acetabular dome
- Posterior column - fourth, connects iliac to ischial cut
- Fragment remains vascularised via inferior gluteal artery pedicle
Approach
- Modified Smith-Petersen (Hueter): TFL-sartorius interval, rectus released from AIIS
- Rectus-sparing (Roberge): preserves rectus, all cuts from within pelvis
- LFCN crosses the interval and is injured in 10-30% of cases
Complications (DANGER)
- Delayed/nonunion (2-5%; ischial and pubic cuts)
- AVN of acetabular fragment (less than 2%; catastrophic if inferior gluteal pedicle disrupted)
- Nerve injuries: LFCN (10-30%), sciatic (1-3%, feared), femoral (rare)
- Intra-articular extension (2-5%; cut too close to acetabulum)
- Heterotopic ossification (5-20%; prophylaxis with indomethacin)
- Overcorrection/iatrogenic FAI (LCEA greater than 40)
Outcomes and THA conversion
- 10-year THA-free survivorship approximately 75-90% in well-selected patients
- 20-year survivorship approximately 60% from Bern cohort
- Predictors of failure: older age, higher Tonnis grade, undercorrection (LCEA less than 25)
- THA after PAO is more complex but implant survivorship is comparable to primary THA
- PAO delays THA by approximately 10-20 years in the majority of patients
Evidence Base
- The original description of the Bernese PAO in 75 hips (71 patients) with developmental dysplasia. The authors described the four-osteotomy technique performed through a modified Smith-Petersen approach, preserving posterior column continuity and fragment vascularity via the inferior gluteal artery. Early results showed significant improvement in pain and function with correction of LCEA from a mean of approximately 2 degrees pre-operatively to approximately 28 degrees post-operatively. Complications included one sciatic nerve palsy and one case of intra-articular extension.
- In the longest reported follow-up of PAO (mean 20 years, range 15-27 years) from the originating centre in Bern, Switzerland, approximately 60% of hips survived without conversion to THA at 20 years. Pre-operative Tonnis grade was the strongest predictor of outcome: patients with Tonnis grade 0 had significantly better survivorship than those with grade 1 or 2. Hips that survived 20 years maintained good functional scores and patient satisfaction.
- In 116 hips followed prospectively for a mean of approximately 9 years after PAO, significant improvements were found in pain, function, and validated outcome scores (Harris Hip Score, WOMAC). Survivorship free of THA was approximately 85% at 10 years. Predictors of failure included older age at surgery (greater than 35), higher pre-operative Tonnis grade, and poor post-operative LCEA correction (undercorrection). Arthroscopic findings of full-thickness chondral damage at the time of PAO also predicted poorer outcome.
- Analysis of risk factors for PAO failure (conversion to THA) in a large Danish cohort identified that older age at surgery, higher pre-operative Tonnis grade, and post-operative LCEA less than 25 degrees (undercorrection) were independent predictors of failure. Patients with a post-operative LCEA of 25-35 degrees had the best survivorship, while those with LCEA less than 20 or greater than 40 degrees had significantly higher failure rates.
- A multicentre review of complications after PAO across several high-volume centres reported an overall complication rate of approximately 6-37% depending on definition (minor complications included). Major complications (requiring reoperation or causing permanent deficit) occurred in approximately 3-8% of cases. The most common complications were LFCN neuropraxia, heterotopic ossification, and wound problems. Sciatic nerve palsy, AVN, and intra-articular extension were rare but serious. There was a learning curve: complication rates decreased with increasing surgeon experience.