Osteoarthritis | Post-Traumatic | Silicone Arthroplasty | Arthrodesis
- PIP Anatomy: Collateral ligaments (proper and accessory), volar plate, central slip insertion.
- Bouchard Nodes: Dorsal osteophytes at PIP joint in primary OA.
- Arthrodesis Angle: 40° index, 45° middle, 50° ring, 55° small finger.
- Silicone Arthroplasty: Best for low-demand patients, preserves 60-70° arc of motion.
- Surface Replacement: For younger active patients, requires intact collaterals.
- “Index finger arthrodesis at 40° (pointing/pinch)
- “Middle finger can tolerate arthroplasty (motion needed)
- “Unstable joints: arthrodesis over arthroplasty
- “Check collateral ligaments before surface replacement
Increasing flexion from radial to ulnar. Index 40° (pinch), Middle 45°, Ring 50°, Small 55°. Functional position for power grip.
Essential for surface replacement success. Intact proper and accessory collaterals required. Incompetent ligaments = arthrodesis.
Silicone: Low-demand, elderly, multiple digits. Surface: Young, active, isolated joint. Know the indications.
Common after fracture-dislocation. Central slip injury leads to boutonniere. Volar plate injury leads to swan-neck. Address deformity first.
- Best Indication
- Low-demand, elderly, multiple digits
- Motion Preserved
- 60-70° arc
- Durability
- 10-15 years
- Key Limitation
- Fracture, subsidence, synovitis
- Best Indication
- Young, active, isolated joint
- Motion Preserved
- 70-80° arc
- Durability
- 5-10 years
- Key Limitation
- Requires intact collaterals, expensive
- Best Indication
- High-demand, unstable, index finger
- Motion Preserved
- 0° (fused)
- Durability
- Permanent
- Key Limitation
- Loss of motion, non-union risk
IMRS 40-45-50-55PIP Arthrodesis Angle
Hook:IMRS = Index-Middle-Ring-Small. Each digit increases 5° of flexion from radial to ulnar for optimal cascade and grip function.
HILUIndications for Arthrodesis over Arthroplasty
Hook:HILU = when to fuse the PIP joint. High-demand, Index, Ligament injury, Unstable joint = choose arthrodesis.
Overview and Epidemiology
PIP joint arthritis is a common viva topic. Examiners test understanding of surgical decision-making: when to fuse vs replace, optimal arthrodesis angles, assessment of collateral ligament integrity. Know the functional demands of each finger.
PIP Joint Arthritis encompasses degenerative, post-traumatic, and inflammatory conditions affecting the proximal interphalangeal joint, resulting in pain, stiffness, and functional impairment.
- Prevalence: 10-15% of adults over 60 years
- Gender: Female greater than male (3:1) for primary OA
- Age: Peak 50-70 years
- Digits: Middle and index most commonly affected
- Occupation: Higher in manual laborers
Post-traumatic arthritis affects younger patients (30-50 years) following fracture-dislocations.
- Primary osteoarthritis: Idiopathic, Bouchard nodes
- Post-traumatic: Fracture-dislocation, chronic instability
- Inflammatory: Rheumatoid arthritis, psoriatic arthritis
- Crystalline: Gout, pseudogout
- Septic sequelae: Prior infection with cartilage loss
Post-traumatic is the most common surgical etiology.
Pathophysiology
The PIP joint is a hinge joint with critical soft tissue stabilizers: proper collateral ligaments (tight in flexion), accessory collateral ligaments (tight in extension), volar plate (prevents hyperextension), and central slip insertion (maintains extension). Understanding these structures is essential for surgical planning.
- Bony Structure: Bicondylar head of proximal phalanx articulating with base of middle phalanx
- Proper Collateral Ligaments: Origin dorsal to axis of rotation, tight in flexion
- Accessory Collateral Ligaments: Insert on volar plate, tight in extension
- Volar Plate: Fibrocartilaginous structure preventing hyperextension
- Central Slip: Insertion on dorsal base of middle phalanx for extension
- Progressive cartilage loss from repetitive microtrauma
- Subchondral bone sclerosis and cyst formation
- Marginal osteophyte formation (Bouchard nodes)
- Synovial inflammation and joint capsule contracture
- Progressive pain, stiffness, and loss of motion
- Intra-articular fracture malunion causing incongruity
- Chronic instability from ligament injury
- Avascular necrosis of middle phalanx base
- Central slip injury leading to boutonniere deformity
- Volar plate injury leading to swan-neck deformity
Classification Systems
Eaton-Littler Classification (PIP Arthritis)
- Radiographic Findings
- Synovitis, minimal changes
- Clinical Features
- Pain, mild stiffness, preserved motion
- Treatment
- NSAIDs, splinting, activity modification
- Radiographic Findings
- Joint space narrowing, early osteophytes
- Clinical Features
- Moderate pain, 20-30° motion loss
- Treatment
- Conservative, intra-articular injection
- Radiographic Findings
- Significant joint space loss, bone-on-bone
- Clinical Features
- Severe pain, stiffness, functional limitation
- Treatment
- Arthroplasty or arthrodesis
- Radiographic Findings
- Severe destruction with subluxation or instability
- Clinical Features
- Severe pain, deformity, ligament incompetence
- Treatment
- Arthrodesis preferred
Clinical Application:
- Grades I-II: Trial conservative management for 3-6 months
- Grade III: Surgical decision based on patient demands and joint stability
- Grade IV: Arthrodesis preferred due to ligament incompetence
This classification system guides surgical decision-making for PIP arthritis.
Clinical Assessment
History
- Pain at PIP joint, worse with gripping activities
- Stiffness, especially in morning or after rest
- Difficulty with fine motor tasks (buttoning, writing)
- Swelling and visible deformity (Bouchard nodes)
- Weakness of grip strength
- Catching or locking sensation (loose bodies)
- Cold intolerance in post-traumatic cases
- Multiple joint involvement (inflammatory arthritis)
Physical Examination
Inspection
- Bouchard Nodes: Dorsal osteophytes at PIP joint (primary OA)
- Deformity: Flexion or extension contracture, swan-neck, boutonniere
- Erythema: Suggests inflammatory or crystalline arthritis
- Muscle Wasting: Intrinsic atrophy in chronic cases
Palpation
- Tenderness: Localized to PIP joint line
- Crepitus: Grinding sensation with passive motion
- Osteophytes: Palpable dorsal or lateral bony prominences
- Joint Stability: Assess collateral ligaments with radial/ulnar stress
Range of Motion
- Active ROM: Compare to contralateral hand
- Passive ROM: Assess for fixed vs dynamic contracture
- Extensor Lag: Central slip insufficiency (boutonniere)
- Hyperextension: Volar plate incompetence (swan-neck)
Special Tests
- Technique
- Radial/ulnar deviation at 30° flexion
- Positive Finding
- Greater than 20° laxity or no endpoint
- Interpretation
- Ligament incompetence, arthrodesis indicated
- Technique
- Hyperextension stress test
- Positive Finding
- Greater than 30° hyperextension
- Interpretation
- Volar plate injury, swan-neck risk
- Technique
- Elson test (90° flexion, resist extension)
- Positive Finding
- Weak or absent middle phalanx extension
- Interpretation
- Central slip disruption, boutonniere
- Technique
- Passive wrist flexion/extension
- Positive Finding
- PIP motion less than 30° arc
- Interpretation
- Severe joint contracture or adhesions
Red Flags
- Acute inflammation with fever: Septic arthritis until proven otherwise
- Rapid progression: Consider inflammatory or crystalline arthropathy
- Severe instability: Risk of dislocation, urgent surgical planning
- Vascular compromise: Check for arterial injury in trauma cases
Investigations
Imaging
Radiographs (PA, Lateral, Oblique)
- Joint Space Narrowing: Loss of articular cartilage
- Subchondral Sclerosis: Increased bone density
- Osteophytes: Bouchard nodes on dorsal and lateral aspects
- Subchondral Cysts: Geodes from synovial fluid intrusion
- Subluxation: Joint incongruity or malalignment
Advanced Imaging
- CT Scan: Assess intra-articular fracture malunion, bone loss, surgical planning
- MRI: Evaluate cartilage loss, ligament integrity, synovitis, loose bodies
- Ultrasound: Dynamic assessment of collateral ligaments, synovitis
Laboratory Tests
- Rheumatoid Factor (RF): Positive in 70-80% of RA
- Anti-CCP Antibodies: Specific for RA
- ESR/CRP: Elevated in active inflammation
- Uric Acid: Elevated in gout
- ANA: Positive in systemic lupus erythematosus
- Joint Aspiration: Synovial fluid analysis for crystals
- Monosodium Urate: Needle-shaped, negative birefringence (gout)
- Calcium Pyrophosphate: Rhomboid, positive birefringence (pseudogout)
Differential Diagnosis
Not all painful, swollen PIP joints are osteoarthritis. The pattern of involvement, the presence of systemic features, and the radiographic appearance distinguish the main causes.
- Distinguishing Features
- Older, female predominance, Bouchard nodes, DIP often involved
- Radiographic / Lab Clues
- Joint space loss, osteophytes, subchondral sclerosis; normal inflammatory markers
- Key Discriminator
- Bouchard nodes plus normal CRP
- Distinguishing Features
- Symmetrical, MCP and wrist involvement, morning stiffness over 1 hour, systemic features
- Radiographic / Lab Clues
- Periarticular erosions, osteopenia; RF and anti-CCP positive, raised ESR/CRP
- Key Discriminator
- Erosive change with positive anti-CCP
- Distinguishing Features
- DIP predominance, dactylitis, nail and skin psoriasis
- Radiographic / Lab Clues
- Pencil-in-cup deformity, new bone formation; RF usually negative
- Key Discriminator
- Skin/nail psoriasis with DIP disease
- Distinguishing Features
- Acute attacks, erythema, can be monoarticular
- Radiographic / Lab Clues
- Tophi or chondrocalcinosis; urate or CPP crystals on aspiration
- Key Discriminator
- Crystals on polarised microscopy
- Distinguishing Features
- Acute hot swollen joint, fever, rapid progression
- Radiographic / Lab Clues
- Effusion, later erosion; raised WCC/CRP, organisms on aspirate
- Key Discriminator
- Pus on aspiration - surgical emergency
- Distinguishing Features
- Prior fracture-dislocation or instability, younger patient
- Radiographic / Lab Clues
- Joint incongruity, malunion, focal cartilage loss; normal inflammatory markers
- Key Discriminator
- Clear injury history with focal damage
Surgical Approaches to the PIP Joint
The technique sections repeatedly specify a "dorsal curved incision" and to "split the central slip or use a chamfer technique", and the Murray series is quoted for its finding that the volar approach failed 6.6 times more often than the dorsal - yet the topic never sets out the approach options or why the choice governs both rehabilitation and implant survival.
- Dorsal approaches (violate then repair the extensor).
- Central-slip-splitting (longitudinal): the extensor is split between the central slip and a lateral band - simple, but the central-slip repair must then be protected, delaying active extension.
- Chamay approach: a distally-based triangular (V-shaped) flap of the extensor apparatus is raised off the proximal phalanx and reflected distally, giving wide joint exposure while keeping the central-slip insertion intact; the flap is repaired at the end. Excellent for accurate implant positioning.
- Because every dorsal approach disturbs the extensor mechanism, the joint is protected and active motion is advanced cautiously, with a real risk of extensor lag or a secondary boutonniere if the repair stretches.
- Volar (Schwartz-Weiland / "shotgun") approach. A volar (Bruner) incision, the flexor sheath opened between the A2 and A4 pulleys (dividing A3), the flexor tendons retracted, and the joint hyperextended ("shotgun-opened") to deliver both articular surfaces - leaving the extensor mechanism completely intact. Its advantage is immediate active motion with no extensor to protect; its drawbacks are limited proximal exposure and the higher implant-failure rate the Murray series documents.
- Choosing. Dorsal is the workhorse for arthrodesis and for most arthroplasties (best exposure, lowest failure). Volar is chosen when early active motion is the priority and the surgeon is experienced with it. A lateral approach (between the collateral ligament and the volar plate) is a third option that spares the extensor but gives narrower access.
Q: What are the approaches to the PIP joint for arthroplasty and how do they affect rehabilitation? A: Dorsal - central-slip-splitting, or the Chamay distally-based V extensor flap - gives the best exposure and the lowest implant-failure rate but violates the extensor, so active motion is protected and there is a boutonniere/extensor-lag risk. The volar Schwartz "shotgun" approach opens the flexor sheath (dividing A3) and hyperextends the joint, leaving the extensor intact for immediate active motion, but has narrower exposure and (per the Murray series) roughly a 6.6-times higher failure rate. Dorsal is the default; reserve volar for when early motion is paramount.
PCAVPIP Joint Stability Structures
Hook:PCAV = the 4 key stabilizers of PIP joint. All must be assessed before considering surface replacement arthroplasty.
The PIP as the Functional Keystone of the Digit
The whole topic pivots on "motion preservation versus pain-free stability", quoting arcs of 40-70° and fusion angles of 40-55°, but never states why PIP motion is so precious - the biomechanical reason the motion-versus-fusion debate is fiercer here than at any other finger joint.
- The PIP is the functional keystone. It contributes the largest single share of the finger's flexion arc - of the roughly 260° of composite flexion available across the MCP, PIP and DIP, the PIP provides about 100°, more than either neighbour. It does most of the work of bringing the fingertip to the palm, so grasp depends on it disproportionately.
- Why fusing a PIP costs more than fusing a DIP. A fused DIP loses only a small terminal arc and is well tolerated; a fused PIP removes the dominant flexion contribution, so the fingertip can no longer reach the palm and both fine and power grasp suffer. This is exactly why arthroplasty (motion) is weighed so heavily against arthrodesis at the PIP, whereas DIP arthritis is comfortably fused.
- "Functional arc", not maximal arc. For most grasp the mid-range of PIP motion matters most, so the realistic surgical goal is a useful arc positioned in the functional range, not a large absolute number - which is why a silicone spacer giving a stable, painless 40-60° arc is often more useful than a wider but unstable or painful one, and why the evidence that no implant reliably increases ROM still supports arthroplasty (it preserves a functional arc and relieves pain).
- Why the border digits differ. The index trades this motion for stability willingly (pinch and pointing need a stable post, so fusion is well tolerated), while the ulnar (ring and small) digits need flexion for power grip and cascade - so motion preservation is valued most there, and the arthrodesis angle is set in progressively more flexion from radial to ulnar.
Q: Why does the PIP joint dominate the motion-versus-fusion decision? A: The PIP is the functional keystone of the finger - it supplies the largest share of digital flexion (about 100° of the roughly 260° composite arc) and does most of the work of bringing the fingertip to the palm, so a stiff or fused PIP disables grasp far more than a stiff DIP. That is why motion-preserving arthroplasty is weighed so heavily here, why a stable, painless functional arc matters more than a large absolute ROM, and why the index (needing a stable pinch post) tolerates fusion while the ulnar digits (needing flexion for power grip) prize motion.
Management Algorithm
Conservative Management
Indications:
- Mild to moderate symptoms (Eaton-Littler Grade I-II)
- Patient refuses surgery or unfit for surgery
- Trial before surgical decision
Non-Pharmacological
- Buddy Taping: Tape affected digit to adjacent finger for stability
- Static Splint: Maintain joint in functional position (40-45° flexion)
- Serial Splinting: Progressive correction of contracture over 6-12 weeks
- Night Splint: Prevent flexion contracture during sleep
- Activity modification to reduce joint stress
- Adaptive devices for ADLs (buttonhooks, jar openers)
- Joint protection education
- Range of motion exercises to maintain flexibility
Pharmacological
- Topical: Diclofenac gel applied 3-4 times daily
- Oral: Ibuprofen 400mg TDS, Naproxen 500mg BD
- Duration: 4-6 weeks trial, use lowest effective dose
- Caution: GI bleeding, renal impairment in elderly
- Corticosteroid: Triamcinolone 10mg or methylprednisolone 20mg
- Technique: Dorsal approach, avoid extensor mechanism
- Frequency: Maximum 3 injections per year
- Efficacy: 50-70% experience pain relief for 3-6 months
Conservative management provides satisfactory symptom control in 40-60% of patients with mild to moderate arthritis. Failure of 3-6 months of conservative treatment warrants surgical consideration.
Conservative management is the first-line approach for most patients with PIP arthritis.
Surgical Technique
Silicone (Swanson) Arthroplasty
- Low-demand patients (elderly, sedentary)
- Desire for motion preservation
- Stable joint with competent collaterals
- Multiple digits involved (RA)
- Regional anesthesia (axillary block) or WALANT
- Supine position, hand table
- Tourniquet at 250 mmHg
- Fluoroscopy available
- Incision: Dorsal curved incision over PIP joint
- Dissection: Elevate skin flaps, identify and protect digital neurovascular bundles
- Extensor Mechanism: Split central slip longitudinally or elevate radial lateral band
- Joint Exposure: Divide collateral ligaments from middle phalanx origin
- Excise arthritic joint surfaces (proximal phalanx head and middle phalanx base)
- Resect 2-3mm of proximal phalanx distal to condyle
- Resect articular surface of middle phalanx base
- Create medullary canal in both phalanges using awls or reamers
- Trial implant to confirm appropriate sizing
- Insert silicone spacer into proximal phalanx canal
- Reduce joint with implant stem into middle phalanx canal
- Confirm full passive flexion and extension
- Ensure no stem impingement or fracture
- Repair central slip or lateral band with 4-0 non-absorbable suture
- Ensure extensor mechanism integrity
- Close skin with 4-0 nylon interrupted sutures
- Apply dorsal blocking splint in 30-40° flexion
- Preserve collateral ligaments if possible for stability
- Avoid excessive bone resection (subsidence risk)
- Ensure stems fully seated in medullary canals
- Test full ROM before closure
- Reliable pain relief is the main benefit; reported patient satisfaction is high
- Arc of motion typically 40-60°; motion gain over the pre-operative arc is often modest
- Lower revision and explantation rates than resurfacing implants (silicone explantation 11% vs titanium 27% vs pyrocarbon 39% in the Daecke RCT)
- Complications: implant fracture, subsidence, recurrent deformity, and late silicone synovitis
Silicone arthroplasty provides reliable pain relief and a functional arc for low-demand patients.
Complications
Early Complications (less than 6 weeks)
- Incidence
- 1-2%
- Presentation
- Wound erythema, drainage, fever
- Management
- Antibiotics, possible I&D
- Incidence
- 2-3%
- Presentation
- Swelling, ecchymosis, pain
- Management
- Compressive dressing, elevation
- Incidence
- 5-10%
- Presentation
- Wire prominence, skin irritation
- Management
- Wire removal and replacement
- Incidence
- Less than 1%
- Presentation
- Numbness, vascular compromise
- Management
- Immediate exploration if acute
Late Complications (greater than 6 weeks)
- Incidence
- 5-10%
- Presentation
- Persistent pain, motion at fusion site
- Management
- Revision with bone graft and rigid fixation
- Incidence
- 5-10%
- Presentation
- Sudden pain, deformity, crepitus
- Management
- Revision with new implant or arthrodesis
- Incidence
- 10-15%
- Presentation
- Progressive deformity, loss of motion
- Management
- Observation vs revision
- Incidence
- 5%
- Presentation
- Pain, swelling, bone erosion (years later)
- Management
- Implant removal, synovectomy, arthrodesis
- Incidence
- 20-30%
- Presentation
- Limited ROM despite therapy
- Management
- Intensive therapy, possible manipulation
- Incidence
- 10%
- Presentation
- Joint subluxation, pain with use
- Management
- Revision to arthrodesis
Prevention Strategies
- Pre-operative antibiotics (Cefazolin 2g IV)
- Strict sterile technique
- Meticulous hemostasis
- Early post-operative wound monitoring
- Maximize bone contact at fusion site
- Rigid internal fixation (screws or plate)
- Smoking cessation mandatory
- Consider bone graft in osteoporotic bone
- Appropriate patient selection (low-demand for silicone)
- Preserve bone stock (minimal resection)
- Ensure intact collateral ligaments for surface replacement
- Strict adherence to post-operative protocol
- Early protected ROM (days 3-5)
- Occupational therapy for hand therapy
- Avoid prolonged immobilization
- Dynamic splinting if contracture develops
Postoperative Care
Post-Operative Protocol: Silicone Arthroplasty
Week 0-2: Protection Phase
- Immobilization: Dorsal blocking splint in 30-40° flexion
- Wound Care: Keep dry until suture removal at 10-14 days
- Edema Control: Elevation above heart level, ice packs
- Pain Management: Oral analgesics (paracetamol, NSAIDs)
Week 2-6: Early Motion Phase
- Splint: Remove for exercises, wear between sessions
- Therapy: Gentle active ROM exercises 5-10 minutes every 2 hours
- Goals: Achieve 0-60° arc by week 6
- Avoid: Forceful gripping, resistance exercises
Week 6-12: Strengthening Phase
- Splint: Discontinue daytime splint, night splint if flexion contracture
- Therapy: Progressive resistance exercises with therapy putty
- Goals: Achieve 60-70° arc, functional grip strength
- Return: Light ADLs at week 8, unrestricted light activities week 12
Month 3-6: Functional Phase
- Activities: Gradual return to pre-injury activities
- Restrictions: Avoid heavy gripping or impact activities (permanent)
- Goals: Pain-free functional range for ADLs
- Follow-Up: Clinical and radiographic at 3, 6, 12 months
Early mobilization is critical to prevent stiffness while protecting implant during healing.
Guidelines, Registries & Global Practice
PIP joint arthritis is managed similarly worldwide, guided by the same evidence base. Practice differs mainly in implant availability and resource setting rather than in core principles.
Global Epidemiology: Symptomatic interphalangeal hand OA affects roughly 10-15% of adults over 60, with a marked female predominance for primary nodal disease. Post-traumatic PIP arthritis affects younger adults and clusters in manual occupations (construction, agriculture, mining). Inflammatory arthropathy (RA, psoriatic) remains an important cause where access to disease-modifying therapy is limited.
Side-by-Side Guidance:
- Stance on PIP Arthritis Management
- Conservative-first: topical/oral NSAIDs, hand therapy, splinting; surgery for refractory disease
- Practical Emphasis
- Strong recommendation for topical NSAIDs and exercise before surgery
- Stance on PIP Arthritis Management
- Core treatments are exercise and education; pharmacotherapy with topical NSAIDs preferred over oral; surgery reserved for severe refractory cases
- Practical Emphasis
- Limit intra-articular steroid to short-term symptom control
- Stance on PIP Arthritis Management
- Match procedure to stability and demand: arthroplasty for stable low/moderate-demand joints, arthrodesis for unstable joints and the index finger
- Practical Emphasis
- Confirm collateral competence before any resurfacing
- Stance on PIP Arthritis Management
- Acknowledges no implant reliably improves motion; silicone remains benchmark, resurfacing for selected stable joints
- Practical Emphasis
- Counsel that pain relief, not large ROM gain, is the realistic goal
National arthroplasty registries (NJR UK, AJRR US, AOANJRR Australia, Swedish/Norwegian/NZ registries) focus on hip, knee and shoulder and do not systematically capture small-joint hand arthroplasty. Consequently, implant-survival counselling relies on institutional cohorts and the randomized data above rather than registry datasets — a recognised gap in the evidence.
In well-resourced settings, silicone and resurfacing implants, hand therapy and image guidance are readily available, and implant choice is driven by demand and stability. In limited-resource settings, arthrodesis (K-wire, tension band or screw) and silicone spacers predominate because they are durable, low-cost and need less specialised follow-up; resurfacing implants are often unavailable. Across all settings, arthrodesis remains the default for the unstable joint, the high-demand manual worker, and the index finger.
Manual workers typically return after PIP arthrodesis around 8-12 weeks once union is confirmed, and somewhat later after arthroplasty owing to protected rehabilitation; exact timelines vary with occupation and local rehabilitation pathways.
Controversies and Areas of Uncertainty
Stating where the evidence is weak or conflicting demonstrates consultant-level judgement. PIP arthroplasty is an area with limited high-level data, so confident nuance scores well.
-
Does any implant actually improve motion? The best randomized evidence (Daecke 2012) found no significant ROM gain for silicone or resurfacing implants, with resurfacing showing only a transient, non-significant advantage. The realistic goal of arthroplasty is pain relief and maintenance of a functional arc, not increased motion.
-
Silicone vs resurfacing. Resurfacing implants (titanium-polyethylene, pyrocarbon) were introduced to improve durability and motion, yet randomized and long-term cohort data show higher explantation and complication rates without a durable motion benefit over the silicone spacer. Their role remains contested and limited to carefully selected, stable joints.
-
Pyrocarbon-specific issues. Squeaking, subsidence (often subclinical and stabilising per Wolff's law) and a relatively high reoperation rate cloud interpretation; many "complications" do not require revision, so reported rates vary widely with definition.
-
Index finger: fuse or replace? Arthrodesis is traditionally preferred for pinch stability, but comparative data (Vitale 2015) show similar pain and satisfaction with arthroplasty at the cost of more complications. The decision is increasingly shared and goal-driven rather than dogmatic.
-
Optimal arthrodesis angle. The classic radial-to-ulnar progression (around 40-55°) is widely taught but not validated by high-level evidence; surgeons individualise the angle to occupation and patient preference.
-
Registry blind spot. Small-joint hand arthroplasty is not tracked by the major national joint registries, so long-term implant survival counselling rests on single-centre series with selection bias.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old carpenter presents with chronic pain in the index finger PIP joint following a fracture-dislocation 2 years ago. He has failed 6 months of conservative management. Examination shows 30° fixed flexion contracture, bone-on-bone crepitus, and palpable osteophytes. Radiographs demonstrate severe joint space loss with subchondral sclerosis. He requests treatment to return to carpentry work.”
“A 72-year-old retired woman presents with bilateral PIP joint arthritis affecting middle, ring, and small fingers. She has prominent Bouchard nodes, moderate pain, and 40° arc of motion. She struggles with buttoning clothes and opening jars. Radiographs show Grade III arthritis (Eaton-Littler) with significant joint space loss. She has tried NSAIDs and splinting for 4 months with minimal relief. She desires motion preservation and pain relief.”
“A 52-year-old active male presents with isolated middle finger PIP arthritis. He plays recreational tennis and golfs regularly. Examination shows stable joint with intact collateral ligaments, 45° arc of motion, and significant pain. Radiographs show Grade III arthritis with preserved bone stock. He strongly desires motion preservation and asks about 'the most advanced implant options.' What would you recommend and why?”
Anatomy (Must Know)
- Proper collaterals: tight in flexion, origin dorsal to axis
- Accessory collaterals: volar plate attachment, tight in extension
- Volar plate: prevents hyperextension, critical for swan-neck
- Central slip: dorsal base of middle phalanx, extension power
- A2 and A4 pulleys: critical, never release with PIP surgery
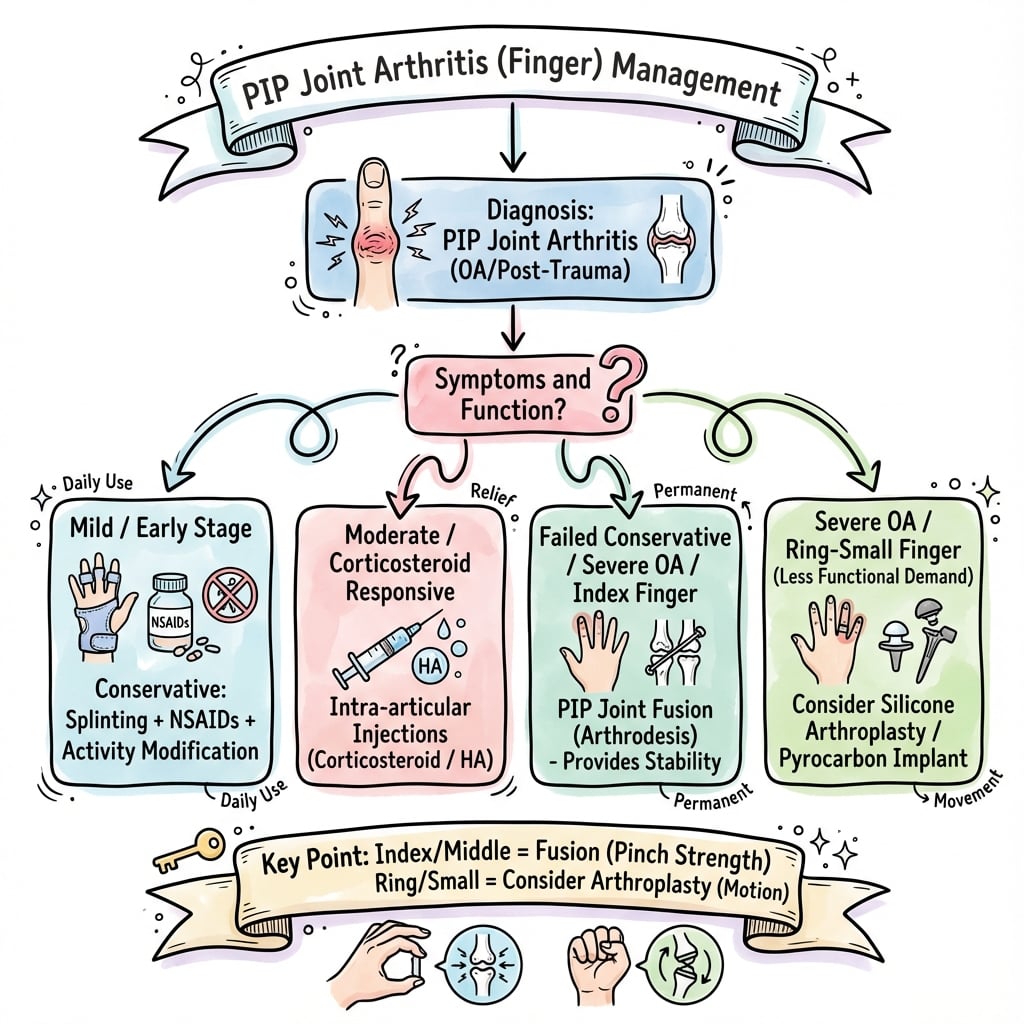
Surgical Decision Algorithm
- STABLE joint + LOW-demand = Silicone arthroplasty
- STABLE joint + MODERATE-demand = Surface replacement arthroplasty
- UNSTABLE joint or HIGH-demand = Arthrodesis
- INDEX finger = Strong preference for arthrodesis
- MULTIPLE digits = Avoid arthrodesis (cumulative stiffness)
Arthrodesis Angles (Critical)
- Index: 40° flexion (pointing, pinch precision)
- Middle: 45° flexion (balanced grip)
- Ring: 50° flexion (power grip cascade)
- Small: 55° flexion (maximum grip strength)
- Rationale: increasing flexion radial to ulnar for optimal cascade
Silicone Arthroplasty
- Best for: Low-demand, elderly, multiple digits
- Motion: typically 40-60° arc; modest gain over pre-op
- Lowest explantation rate of the implants (11% vs TI 27% vs PY 39%, Daecke RCT)
- Complications: Fracture, subsidence, late silicone synovitis
- Activity restrictions: Permanent avoidance heavy gripping
Surface Replacement
- Best for: Young, active, isolated joint, intact ligaments
- Motion: usually maintained (~40° median), not reliably increased
- Metal-PE failure ~11% at 5y, ~16% at 15-25y; dorsal approach safer
- Requires: Competent collaterals (mandatory stress test)
- Complications: Loosening, instability, squeaking, higher than silicone
Arthrodesis Pearls
- Compression screw gives lowest nonunion; K-wire highest (Leibovic)
- Reliable pain relief and grip; satisfaction high despite motion loss
- Fixation: Compression screw preferred, tension band or plate alternatives
- Nonunion higher in psoriatic/RA and smokers; absent in OA in some series
- Return to work generally 8-12 weeks for manual labor
Viva Red Flags (Don't Miss)
- Assess collateral stability before any arthroplasty (stress test)
- Never recommend surface replacement with incompetent ligaments
- Index finger arthritis: default to arthrodesis unless strong reason
- Arthrodesis angle MUST match digit: 40-45-50-55°
- Silicone synovitis is LATE complication (years), requires removal
Evidence Base
Three Implant Types Compared: Silicone vs Titanium vs Pyrocarbon
- Prospective randomized multicentre trial: 43 patients (62 PIP joints) allocated to silicone (SI), titanium-polyethylene (TI) or pyrocarbon (PY); mean follow-up 35 months
- All 3 implants gave significant pain reduction at rest and load; tip-pinch slightly improved across groups
- No significant ROM gain for any device; resurfacing implants showed only a transient, non-significant ROM advantage over silicone
- Explantation rates: silicone 2 of 18 (11%), titanium 7 of 26 (27%), pyrocarbon 7 of 18 (39%)
Posttraumatic Finger Joint Reconstruction: Arc of Motion and Complications
- Systematic review of world literature (520 articles screened) comparing vascularized toe joint transfer, silicone, and pyrocarbon arthroplasty
- Mean PIP active arc of motion: vascularized toe joint 37°, silicone 44°, pyrocarbon 43°
- Major complication (revision) rates: vascularized toe joint 29%, silicone 18%, pyrocarbon 33%
- No meaningful improvement in posttraumatic finger joint outcomes over 40 years
Pyrocarbon PIP Arthroplasty: Minimum 2-Year Outcomes
- Retrospective series of 50 pyrocarbon PIP replacements in 35 patients (minimum 27-month follow-up)
- Mean arc of motion improved only modestly from 40° to 47°; pain scores fell from 6 to 1 (0-10 scale)
- Overall patient satisfaction nearly 80%; index finger results comparable to other digits
- 28% of patients required a second procedure; revision arthroplasty rate 8%; radiographic subsidence in 40% of joints
Arthroplasty vs Arthrodesis for Index Finger PIP Arthritis
- Comparative cohort of 79 index-finger PIP joints (65 arthroplasty, 14 arthrodesis) for OA or posttraumatic arthritis
- No significant difference in pain relief, satisfaction, or Michigan Hand Questionnaire scores between groups
- Arthroplasty preserved motion and improved opposition pinch; arthrodesis improved both opposition and apposition pinch
- Arthroplasty carried a 4.3-fold higher complication risk and a shorter time to first complication
PIP Arthrodesis: Fixation Method and Nonunion
- Retrospective review of 224 PIP arthrodeses fixed with Herbert screw (37), K-wire (100), tension band (69), plate (11) or other (7)
- Mean clinical union at 7 weeks, radiographic union at 10 weeks; nonunion in 31 cases
- Primary nonunion rate highest with K-wires, intermediate with tension band, lowest with Herbert screw
- Nonunion highest in psoriatic arthritis, intermediate in RA, lowest in trauma, and absent in osteoarthritis
Surface Replacement Arthroplasty: 30-Year Single-Centre Experience
- 67 CoCr/UHMWPE surface replacements in 47 patients over 30 years; mean follow-up 8.8 years
- Median total active PIP motion 40° at follow-up; median VAS pain 3 of 100
- Cumulative implant failure 8% at 3 years, 11% at 5 years, 16% at 15-25 years
- Volar approach failed 6.6 times more often than dorsal; failure rate similar for OA and RA
References
-
Squitieri L, Chung KC. A systematic review of outcomes and complications of vascularized joint transfer, silicone arthroplasty, and PyroCarbon arthroplasty for posttraumatic joint reconstruction of the finger. Plast Reconstr Surg. 2008;121(5):1697-1707. doi:10.1097/PRS.0b013e31816aa0b3
-
Bravo CJ, Rizzo M, Hormel KB, Beckenbaugh RD. Pyrolytic carbon proximal interphalangeal joint arthroplasty: results with minimum two-year follow-up evaluation. J Hand Surg Am. 2007;32(1):1-11. doi:10.1016/j.jhsa.2006.10.017
-
Vitale MA, Fruth KM, Rizzo M, Moran SL, Kakar S. Prosthetic arthroplasty versus arthrodesis for osteoarthritis and posttraumatic arthritis of the index finger proximal interphalangeal joint. J Hand Surg Am. 2015;40(10):1937-1948. doi:10.1016/j.jhsa.2015.05.021
-
Leibovic SJ, Strickland JW. Arthrodesis of the proximal interphalangeal joint of the finger: comparison of the use of the Herbert screw with other fixation methods. J Hand Surg Am. 1994;19(2):181-188. doi:10.1016/0363-5023(94)90002-7
-
Jennings CD, Livingstone DP. Surface replacement arthroplasty of the proximal interphalangeal joint using the PIP-SRA implant: results, complications, and revisions. J Hand Surg Am. 2015;40(3):469-473. doi:10.1016/j.jhsa.2014.11.023
-
Swanson AB. Flexible implant arthroplasty for arthritic finger joints: rationale, technique, and results of treatment. J Bone Joint Surg Am. 1972;54(3):435-455.
-
Bouchard C. Osteoarthritis of the hand: clinical manifestations and pathogenesis. In: Moskowitz RW, Howell DS, Altman RD, et al., eds. Osteoarthritis: Diagnosis and Medical/Surgical Management. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2007:191-210.
-
Eaton RG, Littler JW. Joint injuries and their sequelae. Clin Plast Surg. 1976;3(1):85-98.
-
Herren DB, Simmen BR. Palmar approach in flexible implant arthroplasty of the proximal interphalangeal joint. Clin Orthop Relat Res. 2000;371:131-135. doi:10.1097/00003086-200002000-00016
-
Chung KC, Ram AN, Shauver MJ. Outcomes of pyrolytic carbon arthroplasty for the proximal interphalangeal joint. Plast Reconstr Surg. 2009;123(5):1521-1532. doi:10.1097/PRS.0b013e3181a2059b
-
Daecke W, Kaszap B, Martini AK, Hagena FW, Rieck B, Jung M. A prospective, randomized comparison of 3 types of proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2012;37(9):1770-1779. doi:10.1016/j.jhsa.2012.06.006
-
Watts AC, Hearnden AJ, Trail IA, Hayton MJ, Nuttall D, Stanley JK. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum five-year follow-up. J Hand Surg Am. 2012;37(5):882-888. doi:10.1016/j.jhsa.2012.01.039
-
Bellemère P, Maes-Clavier C, Loubersac T, Gaisne E, Kerjean Y, Krimmer H. Proximal interphalangeal joint arthrodesis with an intramedullary screw: a review of 49 cases. J Hand Surg Eur Vol. 2011;36(5):381-387. doi:10.1177/1753193410397895
-
Teoh LC, Yeo SJ. Proximal interphalangeal joint fusion with Herbert screws. J Hand Surg Br. 1996;21(4):508-510. doi:10.1016/s0266-7681(96)80056-9
-
Stern PJ, Fulton DB. Distal interphalangeal joint arthrodesis: an analysis of complications. J Hand Surg Am. 1992;17(6):1139-1145. doi:10.1016/s0363-5023(09)91079-9
-
Murray PM, Linscheid RL, Cooney WP 3rd, Baker V, Heckman MG. Long-term outcomes of proximal interphalangeal joint surface replacement arthroplasty. J Bone Joint Surg Am. 2012;94(12):1120-1128. doi:10.2106/JBJS.J.01375
-
Zimmerman NB, Zimmerman SI, Clark GL, Wilgis EF. Silicone interpositional arthroplasty of the distal interphalangeal joint. J Hand Surg Am. 1989;14(5):882-887. doi:10.1016/s0363-5023(89)80096-8
-
Ashworth CR, Blatt G, Chuinard RG, Stark HH. Silicone-rubber interposition arthroplasty of the carpometacarpal joint of the thumb. J Hand Surg Am. 1977;2(5):345-357. doi:10.1016/s0363-5023(77)80046-8