Proximal Median Nerve Compression | Forearm Pain | Sensory AND Motor Loss
- Palmar Cutaneous Branch: Involved in pronator syndrome, SPARED in CTS - key differentiator
- Forearm Pain: Hallmark of pronator syndrome, absent in CTS
- Four Compression Sites: Lacertus, pronator teres (most common), FDS arch, ligament of Struthers
- Pronator Provocation: Resisted pronation reproduces symptoms
- Less Common Than CTS: Pronator syndrome is rare, often misdiagnosed as CTS
- “Thenar sensation loss = pronator syndrome not CTS
- “Forearm pain = proximal median nerve compression
- “Resisted pronation + flexion = provocative test
- “NCS often normal (unlike CTS where abnormal)
Palmar cutaneous branch involved. Loss of sensation over thenar eminence differentiates pronator syndrome from CTS (where palmar cutaneous is spared).
Pain in proximal volar forearm. This is the hallmark symptom. CTS causes hand/wrist symptoms but not forearm pain.
NCS often normal. Unlike CTS where NCS is typically abnormal. Diagnosis is primarily clinical.
Lacertus, pronator teres, FDS arch, ligament of Struthers. Must release all potential sites during surgery.
- Pronator Syndrome
- Proximal volar forearm
- Carpal Tunnel Syndrome
- Wrist and hand
- Pronator Syndrome
- LOST (palmar cutaneous involved)
- Carpal Tunnel Syndrome
- NORMAL (palmar cutaneous spared)
- Pronator Syndrome
- Less common
- Carpal Tunnel Syndrome
- Very common (hallmark)
- Pronator Syndrome
- Negative
- Carpal Tunnel Syndrome
- Positive
- Pronator Syndrome
- POSITIVE
- Carpal Tunnel Syndrome
- Negative
- Pronator Syndrome
- Often normal
- Carpal Tunnel Syndrome
- Abnormal (prolonged latency)
LPFSFour Compression Sites
Hook:LPFS = Lacertus, Pronator, FDS, Struthers - four compression sites from proximal to distal!
Overview and Epidemiology
Pronator syndrome is an uncommon but important differential for median nerve symptoms. It is frequently misdiagnosed as CTS, leading to failed carpal tunnel releases. The key is recognizing thenar sensory loss and forearm pain.
Pronator Syndrome is compression of the median nerve in the proximal forearm, most commonly between the two heads of pronator teres muscle.
- Incidence: Rare (1% frequency of CTS)
- Female predominance: 2:1 ratio
- Peak age: 30-50 years
- Bilateral: Uncommon (10-15%)
- Occupational: Repetitive pronation, gripping
Often missed or misdiagnosed as carpal tunnel syndrome.
- Repetitive pronation: Mechanics, assembly workers
- Weightlifting: Especially supination/pronation exercises
- Anomalous anatomy: Ligament of Struthers, aberrant muscles
- Direct trauma: Fractures, contusions to forearm
- Hypertrophy: Pronator teres muscle hypertrophy
Occupational and anatomical factors both contribute.
Pathophysiology and Mechanisms
The median nerve enters the forearm between the two heads of pronator teres (humeral and ulnar heads). Proximal to this, it may pass under the lacertus fibrosus. Distal to pronator, it passes under the FDS arch. Compression at any of these sites causes pronator syndrome.
-
Ligament of Struthers (1% of population)
- Anomalous ligament from supracondylar process to medial epicondyle
- Nerve passes underneath
- Rare but must be identified if present
-
Lacertus Fibrosus (Bicipital Aponeurosis)
- Fascia from biceps tendon crossing over median nerve
- Tight in full elbow extension with forearm supination
- Second most common site
-
Pronator Teres (MOST COMMON, 85%)
- Between humeral and ulnar heads of pronator teres
- Nerve compressed with forceful/repetitive pronation
- Primary surgical target
-
FDS Arch
- Fibrous arch of flexor digitorum superficialis (to middle finger)
- Nerve passes beneath arch
- Tight with resisted finger flexion
- Dynamic compression with muscle contraction
- Chronic ischemia and nerve irritation
- Progressive fibrosis and scarring
- Eventual demyelination and axonal damage
Classification Systems
Classification by Anatomical Site
- Frequency
- 1% (rare)
- Provocative Maneuver
- Elbow extension
- Release Technique
- Divide ligament, excise supracondylar process
- Frequency
- 10-15%
- Provocative Maneuver
- Elbow extension + supination
- Release Technique
- Divide bicipital aponeurosis
- Frequency
- 85% (most common)
- Provocative Maneuver
- Resisted pronation
- Release Technique
- Release between two heads
- Frequency
- 5-10%
- Provocative Maneuver
- Resisted finger flexion
- Release Technique
- Release fibrous arch
Multiple sites may coexist in same patient - comprehensive release essential.
Clinical Assessment
- Pain: Proximal volar forearm (key symptom)
- Numbness: Median nerve distribution INCLUDING thenar eminence
- Timing: Activity-related, worse with pronation/gripping
- Less nocturnal: Unlike CTS, less nocturnal waking
- Occupation: Ask about repetitive pronation activities
- Red flags: Rapid progression, severe weakness
Forearm pain is the hallmark that distinguishes from CTS.
- Sensory: Test thenar eminence (palmar cutaneous)
- Motor: APB, FPL, FDP usually normal (may be subtle weakness)
- Tinel's: Over pronator teres (less specific)
- Resisted pronation: Reproduces forearm pain (key test)
- Resisted FDS flexion: May reproduce symptoms
- Phalen's: Negative (unlike CTS)
- Palpation: Tenderness over pronator muscle
Palmar cutaneous sensory loss is pathognomonic.
- Technique
- Resist forearm pronation with elbow 90° flexed
- Positive Finding
- Forearm pain/paresthesias
- Sensitivity
- Moderate (60-70%)
- Technique
- Resist isolated PIP flexion of middle finger
- Positive Finding
- Forearm pain/paresthesias
- Sensitivity
- Low (30-40%)
- Technique
- Full elbow extension + supination held 60 seconds
- Positive Finding
- Symptoms reproduced
- Sensitivity
- Moderate (50-60%)
- Technique
- Compress pronator teres for 30 seconds
- Positive Finding
- Paresthesias in median distribution
- Sensitivity
- Moderate (40-60%)
CTS (most common misdiagnosis - no thenar sensation loss, nocturnal symptoms), AIN syndrome (pure motor, no sensory), C6/C7 radiculopathy (neck pain, dermatomal pattern), thoracic outlet syndrome, medial epicondylitis.
PAINClinical Features of Pronator Syndrome
Hook:PAIN = the key symptom that distinguishes pronator syndrome from CTS!
Lacertus Syndrome and the Scratch-Collapse Test
The evidence base for this topic is dominated by a modern reframing that the main text only glances at: much of what is labelled "pronator syndrome" is actually compression at the lacertus fibrosus, diagnosable by three clinical signs.
- Lacertus (not pronator teres) as the primary site. A growing literature argues the lacertus fibrosus (bicipital aponeurosis) is frequently the true, and often sole, compression point — some authors call it "lacertus tunnel syndrome" and treat it as a distinct subset of pronator syndrome rather than a minor secondary site.
- Hagert's three clinical signs. The diagnosis is clinical: (1) weakness of median-innervated muscles distal to the lacertus (test FPL, the FDP to the index, and APB against resistance); (2) pain on pressure over the median nerve at the lacertus; and (3) a positive scratch-collapse test.
- The scratch-collapse test. The seated patient holds both arms adducted, elbows flexed 90 degrees, and resists the examiner's external-rotation force; the examiner lightly scratches the skin over the compression site (the lacertus), and a transient loss of external-rotation resistance (a brief "collapse") on the affected side is positive and localises the level.
- Why it matters. Because electrodiagnostics are usually normal, these clinical signs ARE the diagnosis — and recognising lacertus compression explains the roughly 10% of pooled surgical series who had already undergone a failed carpal tunnel release before the proximal lesion was found.
Q: How is lacertus (proximal median) compression diagnosed when nerve conduction studies are normal? A: Clinically, by Hagert's three signs - weakness of median muscles distal to the lacertus, tenderness over the median nerve at the lacertus, and a positive scratch-collapse test (a brief loss of resisted external rotation when the skin over the lacertus is scratched). Many "pronator syndrome" cases are really lacertus tunnel syndrome, and about 10% have had a failed carpal tunnel release first.
FOREARMPronator Syndrome vs CTS
Hook:FOREARM pain and sensory loss over FOREARM helps diagnose pronator syndrome!
Investigations
Investigation Protocol
Clinical diagnosis based on forearm pain, median nerve sensory symptoms including thenar eminence, and positive resisted pronation test.
Often normal in pronator syndrome (key difference from CTS). May show mild slowing of forearm segment conduction if severe. EMG may show minimal denervation in median-innervated muscles.
MRI forearm if mass lesion suspected, failed conservative treatment, or pre-operative planning. May show nerve compression, muscle hypertrophy, or anomalous structures.
Local anesthetic injection around pronator teres. Temporary symptom relief suggests pronator syndrome and helps confirm diagnosis in uncertain cases.
Key Investigations:
- NCS: Usually NORMAL (unlike CTS where prolonged latency expected)
- EMG: May show minimal changes in median muscles
- X-ray: Look for supracondylar process if ligament of Struthers suspected
- MRI: Assess for masses, anomalous muscles, nerve signal changes
- Diagnostic injection: Can confirm diagnosis if resolution of symptoms
Management Algorithm
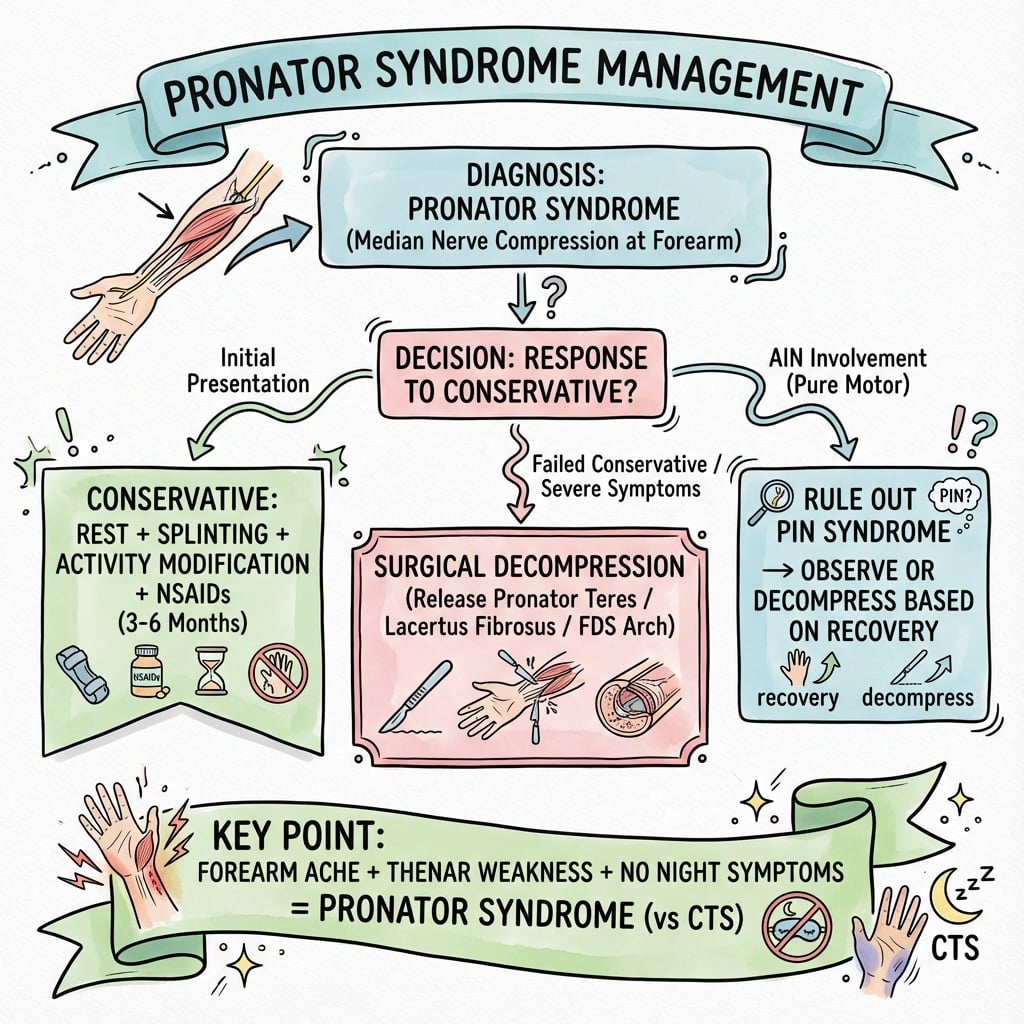
- 1Initial Presentation
Patient with forearm pain and/or median nerve paresthesias
Comprehensive clinical examination required
- 2Clinical Examination
Test thenar eminence sensation, resisted pronation test, Phalen's and Tinel's at wrist
Thenar sensation loss and positive resisted pronation suggests pronator syndrome
- 3Diagnostic Workup
EMG/NCS (often normal), MRI forearm if mass suspected, X-ray if ligament of Struthers suspected
Confirm diagnosis and exclude mass lesions
- 4Conservative Treatment
3-6 months trial: Activity modification, NSAIDs, forearm splint, PT, steroid injection (1-2 maximum)
30-40% respond to conservative measures
- 5Failed Conservative or Progressive Weakness
Surgical decompression: Release all four sites (Struthers, lacertus, pronator teres, FDS arch)
70-80% good to excellent surgical outcomes
- 6Postoperative
Early mobilization, progressive strengthening, gradual return to activities
Sensory recovery 6-12 weeks, motor recovery 3-6 months
Conservative Management (First-Line)
Conservative Treatment Protocol
Activity modification: Avoid repetitive pronation and gripping. Ergonomic workplace assessment. NSAIDs for pain control.
Forearm splint in neutral pronation/supination if symptoms severe. Less effective than in CTS but can provide relief.
Stretching and strengthening of forearm muscles. Nerve gliding exercises. Manual therapy for muscle release.
Corticosteroid injection around pronator teres. May provide temporary relief. Limit to 1-2 injections. Can be diagnostic and therapeutic.
Conservative treatment for 3-6 months before considering surgery.
Surgical Technique
Median Nerve Decompression in Forearm
Surgical Steps
Supine, arm table, tourniquet. Lazy-S incision from 2cm proximal to elbow crease, crossing antecubital fossa medial to biceps tendon, extending 8-10cm down volar forearm along FCR-PL interval.
Identify and protect medial antebrachial cutaneous nerve. Identify median nerve proximal to elbow. Check for ligament of Struthers (palpate for supracondylar process). Divide lacertus fibrosus.
Identify two heads of pronator teres (humeral and ulnar heads). Trace median nerve between heads. Release or divide humeral head if tight. Ensure nerve glides freely.
Follow nerve distally to FDS arch. Release fibrous arch of FDS (to middle finger) if present. Ensure complete decompression of nerve throughout forearm.
Identify AIN branch coming off median nerve. Ensure AIN is not compressed by fibrous bands or Gantzer's muscle. Release if tight.
Layered closure. Do not repair pronator teres if divided. Bulky dressing and forearm splint in neutral position.
Complete decompression from proximal to distal is essential.
Wide-Awake (WALANT) Release and Intra-operative Confirmation
The operative evidence for proximal median compression has shifted toward a minimally-invasive, awake approach that the classic open technique above does not describe.
- The WALANT paradigm. Release is increasingly performed wide-awake under local anaesthesia with lidocaine-adrenaline and no tourniquet (WALANT) through a small (about 2 cm) incision at the lacertus, as a day-case/ambulatory procedure with low morbidity.
- Intra-operative confirmation. Its defining advantage: because the patient is awake and un-tourniqueted, the return of median-muscle strength can be tested on the table immediately after release — an instant confirmation that the correct structure was decompressed (seen in essentially all patients in the awake series).
- The percutaneous option. An emerging ultrasound-guided percutaneous release of the lacertus (performed superficial to pronator teres under WALANT) reproduces the immediate strength return through a millimetric skin incision with same-week return to work.
- Outcomes and the caveat. Awake lacertus release gives large early functional gains (QuickDASH falling by roughly 25-45 points across series) with few complications; the caveats are careful case selection and the reminder that a persistent case may still need a carpal tunnel or superficialis-arcade release.
Q: What is the advantage of a wide-awake (WALANT) lacertus/median release? A: Performed under local anaesthesia with no tourniquet, it lets you test the immediate return of median-muscle strength intra-operatively - confirming the right structure was released - through a small (~2 cm) day-case incision (an ultrasound-guided percutaneous version also exists). It gives large early QuickDASH gains, but a residual case may still need a carpal tunnel or superficialis-arcade release.
Complications
- Incidence
- 10-15%
- Management
- Careful dissection, neurolysis if symptomatic
- Incidence
- 15-20%
- Management
- Ensure all sites released at initial surgery
- Incidence
- 20-30%
- Management
- May indicate wrong diagnosis or incomplete release
- Incidence
- Rare (under 2%)
- Management
- Gentle handling, avoid excessive traction
- Incidence
- 5-10%
- Management
- Standard wound care, antibiotics if needed
Incomplete decompression and persistent symptoms are common because: 1) Wrong initial diagnosis (was actually CTS or other condition), 2) Incomplete surgical release of all compression sites, 3) Coexisting CTS or cervical pathology.
Postoperative Care
Postoperative Protocol
Forearm splint in neutral position. Wound care. Finger and elbow ROM immediately. Suture removal at 10-14 days.
Discontinue splint. Active ROM exercises. Gentle pronation/supination. Scar massage. No strengthening yet.
Progressive strengthening. Gradual return to gripping and pronation activities. Functional exercises.
Return to full activities. Sensory recovery usually within 6-12 weeks. Motor recovery (if weakness present) may take 3-6 months.
Return to work: Light duty at 2-4 weeks. Full duty at 6-8 weeks for most occupations. Manual labor may require 8-12 weeks.
Outcomes and Prognosis
Surgical Outcomes:
- Overall success: 70-80% good to excellent results
- Complete relief: 50-60%
- Partial improvement: 20-30%
- No improvement: 10-20% (often wrong diagnosis)
Prognostic Factors:
- Better Outcome
- Short (under 6 months)
- Worse Outcome
- Long (over 1-2 years)
- Better Outcome
- Clear clinical diagnosis, positive injection
- Worse Outcome
- Uncertain diagnosis, normal exam
- Better Outcome
- Identifiable compression (ligament, band)
- Worse Outcome
- No clear pathology at surgery
- Better Outcome
- Isolated pronator syndrome
- Worse Outcome
- Coexisting CTS or cervical issues
Reasons for Failure:
- Wrong diagnosis (was CTS or radiculopathy)
- Incomplete surgical decompression
- Coexisting compression sites (double crush)
- Progression of symptoms post-operatively
Guidelines, Registries & Global Practice
Global epidemiology. Proximal median nerve entrapment is genuinely uncommon and historically under-recognised; it is roughly an order of magnitude less frequent than carpal tunnel syndrome. There is a female predominance (around 2:1 to 3:1 across recent series) and a working-age peak (late 30s to 50s). A recurring international observation is that a meaningful minority of patients — about 10% in pooled lacertus-release data — have already undergone a failed carpal tunnel release before the proximal lesion is recognised.
No dedicated registry. Unlike arthroplasty, peripheral nerve decompressions are not captured by national joint or implant registries (NJR, AJRR, AOANJRR, Swedish/Norwegian/NZJR). Evidence is therefore driven by case series, prospective cohorts and the 2025 PRISMA systematic review rather than registry data — a point worth stating explicitly in a viva.
Side-by-side guidance (no society has a stand-alone pronator-syndrome guideline):
- Position relevant to proximal median compression
- CTS guidelines emphasise excluding proximal/cervical causes before CTR; no specific pronator guidance
- Position relevant to proximal median compression
- Treat as a clinical diagnosis; reserve surgery for failed conservative care; document differentiation from CTS
- Position relevant to proximal median compression
- Anatomy-based teaching of the four compression sites; complete decompression at operation
- Position relevant to proximal median compression
- Growing recognition of lacertus-level compression and wide-awake (WALANT) release
High- vs limited-resource practice. Where ultrasound and WALANT theatres are available, image-guided or minimal-incision awake release is increasingly favoured, allowing intra-operative confirmation of returned strength and same-day discharge. In limited-resource settings the diagnosis remains primarily clinical (history, thenar sensory testing, resisted pronation and scratch-collapse test), open decompression under regional/general anaesthesia is standard, and a diagnostic local-anaesthetic block is a cheap, useful confirmatory step. Electrodiagnostics are helpful chiefly to exclude CTS and cervical radiculopathy rather than to confirm pronator syndrome, since they are frequently normal.
Documentation / consent points (exam-relevant, billing-agnostic): record palmar cutaneous sensory testing, an adequate conservative trial (3-6 months), the differential considered (CTS, AIN syndrome, C6/C7 radiculopathy, TOS), and consent covering persistent symptoms (20-30%), cutaneous nerve injury and incomplete relief.
MCQ Practice Points
Q: What is the key sensory finding that differentiates pronator syndrome from CTS? A: Loss of sensation over the thenar eminence. The palmar cutaneous branch of the median nerve exits 5cm proximal to the wrist and supplies the thenar eminence. It is compressed in pronator syndrome but spared in CTS.
Q: What is the most common site of median nerve compression in pronator syndrome? A: Between the two heads of pronator teres muscle (85%). Other sites include lacertus fibrosus, FDS arch, and ligament of Struthers.
Q: How do NCS findings differ between pronator syndrome and CTS? A: NCS often NORMAL in pronator syndrome. CTS typically shows prolonged distal motor latency and sensory latency. Pronator syndrome is primarily a clinical diagnosis.
Q: What is the ligament of Struthers? A: Anomalous ligament from supracondylar process to medial epicondyle. Present in only 1% of population. When present, median nerve passes underneath and can be compressed. Palpable bony prominence on distal humerus suggests diagnosis.
Q: What is the most specific provocative test for pronator syndrome? A: Resisted forearm pronation with elbow at 90 degrees flexion. Reproduction of forearm pain and paresthesias in median nerve distribution is positive test.
Q: Can a patient have both pronator syndrome and carpal tunnel syndrome? A: Yes - double crush syndrome. The median nerve can be compressed at multiple levels. Both conditions can coexist in 10-20% of cases. May need decompression at both levels.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old office worker presents with 4 months of volar forearm pain and numbness in the thumb and index finger. Symptoms are worse with typing. She has normal Phalen's and Tinel's at the wrist. She has sensory loss over the thenar eminence. Resisted pronation reproduces her forearm pain. What is your diagnosis and management?”
“A 45-year-old woman had carpal tunnel release 6 months ago but still has persistent forearm pain and median nerve paresthesias including over the thenar eminence. What is your approach?”
“You are performing pronator syndrome decompression. After releasing the lacertus fibrosus and pronator teres, you notice the median nerve is still compressed by a thick fibrous arch under the FDS. You also notice the AIN branch seems compressed by an anomalous muscle. What do you do?”
“A 52-year-old patient presents with nocturnal hand numbness and daytime forearm pain. Examination reveals sensory loss over the thenar eminence and in the median nerve distribution of the hand. Both Phalen's test and resisted pronation test are positive. NCS shows prolonged distal motor latency at the wrist. What is your diagnosis and management approach?”
Key Differentiators from CTS
- Forearm pain (hallmark) - CTS causes hand/wrist pain
- Thenar sensory loss (palmar cutaneous involved)
- NCS often normal (CTS has abnormal NCS)
- Resisted pronation positive (negative in CTS)
Four Compression Sites (LPFS)
- Lacertus fibrosus (bicipital aponeurosis)
- Pronator teres (most common - 85%)
- FDS arch (fibrous arch to middle finger)
- Struthers ligament (anomalous, 1%)
Clinical Diagnosis
- Volar forearm pain + median nerve symptoms
- Sensory loss over thenar eminence (key finding)
- Positive resisted pronation test
- Less nocturnal symptoms than CTS
Investigations
- NCS usually normal (unlike CTS)
- EMG may show minimal median muscle changes
- MRI if mass or anomaly suspected
- Diagnostic injection can confirm diagnosis
Surgical Technique
- Lazy-S incision, antecubital fossa to forearm
- Release all four compression sites systematically
- Protect medial antebrachial cutaneous nerve
- Ensure AIN branch not compressed (Gantzer's muscle)
Outcomes and Pearls
- Conservative success low (30-40%)
- Surgical success 70-80%
- Incomplete release = main cause of failure
- Can coexist with CTS (double crush)
Evidence Base
- 39 patients over 7 years; aching forearm discomfort, hand weakness, thumb/index numbness
- Distinctive sign: tenderness over proximal pronator teres aggravated by resisted pronation
- Electrophysiology abnormal in only a few; localisation rarely possible
- 36 operations: 28 good/excellent, 5 fair, 3 unchanged; failure from inadequate release or misdiagnosis
- Comprehensive review of proximal median neuropathies mimicking CTS
- Pronator and AIN syndromes are rare relative to CTS; suspect when CTS fails to respond
- Differentiation rests on paraesthesia pattern and muscle weakness pattern, not electrodiagnostics
- Conservative strategy: rest/immobilisation, modalities, nerve gliding, then surgery
- 44 patients with proximal median nerve entrapment released prospectively (WALANT, no tourniquet)
- Diagnosis on 3 signs: weakness in median muscles distal to lacertus, tenderness at lacertus, positive scratch-collapse test
- Immediate intra-operative return of median muscle strength in all subjects
- QuickDASH fell from 35.4 to 12.7 at 6 months (p less than 0.0001)
- 93 patients with lacertus syndrome (subset of pronator syndrome); 77% women, mean age 38.7
- Isolated lacertus release under WALANT after 3 months of failed hand therapy
- Mean QuickDASH fell from 53 to 7.8 immediately and 10.6 at 6 months (p less than 0.001)
- Grip strength rose 16 to 24 kg; pinch 9 to 13 kg
- 7 studies, 446 patients undergoing isolated lacertus fibrosus release; mean follow-up 16.1 months
- 10.5% had prior failed carpal tunnel release before correct diagnosis
- Immediate pain relief and return of strength in 99.6%; only 2 complications (haematoma, infection)
- 7 residual cases needed later CTR (3) or superficialis arcade release (4)
- 15 consecutive patients: percutaneous ultrasound-guided lacertus release under WALANT
- Immediate return of muscle strength sustained at follow-up
- VAS pain fell from 6.2 to 0.6 by week 4; all working patients back to work by week 1
- No anaesthetic/surgical complications; one self-resolving haematoma