Socket Design | Suspension Systems | Knee Units | Prosthetic Feet | Upper Limb Prosthetics
- Socket types: PTB (patellar tendon bearing) vs TSB (total surface bearing) for transtibial; quadrilateral vs ischial containment for transfemoral
- Suspension systems: Pin lock (mechanical), suction (seal-in liner), vacuum (active pump), sleeve (neoprene/gel)
- Knee units: Single-axis (simple, durable), polycentric (stability), hydraulic/pneumatic (cadence responsive), microprocessor (C-Leg, Genium)
- Prosthetic feet: SACH (solid ankle cushion heel), single/multi-axis, dynamic response (energy storing/returning)
- K-levels (K0-K4) determine component prescription - match complexity to functional capacity
- “TSB socket distributes load over entire residual limb vs PTB which concentrates on patellar tendon
- “Ischial containment socket provides better coronal femoral control than the older quadrilateral design
- “Microprocessor knees significantly reduce stumbles and uncontrolled falls vs mechanical knees (RCT and systematic-review evidence)
- “Energy-storing (dynamic response) feet improve gait efficiency, most measurably at faster walking and running speeds
Volume fluctuation is the most common socket problem - residual limb shrinks with weight loss, expands with edema. Pistoning (vertical movement) indicates poor suspension or socket looseness. Skin breakdown occurs at pressure points - check socket fit, liner condition, and hygiene. All require prosthetist review and socket adjustment.
Match knee complexity to K-level. K1-K2: Single-axis or polycentric mechanical knee. K3: Hydraulic or pneumatic (cadence responsive). K4 or high falls risk: Microprocessor knee (C-Leg, Genium). Microprocessor knees detect stumble and resist buckling - RCT and systematic-review evidence shows significantly fewer stumbles and uncontrolled falls than mechanical knees.
SACH foot: Simple, durable, low activity (K1). Single-axis: Allows plantarflexion for knee stability (K1-K2). Multi-axis foot: Terrain adaptation (K2-K3). Dynamic response (energy-storing): Carbon fiber, returns energy for efficient gait (K3-K4). Match foot to activity level and terrain requirements.
Body-powered: Cable-operated, reliable, provides proprioceptive feedback, lower cost. Myoelectric: EMG-controlled, cosmetically superior, higher grip strength. Terminal devices: Hooks (functional, durable) vs hands (cosmetic, complex). Higher rejection rates in upper limb than lower limb prosthetics.
- Mechanism
- Simple hinge with friction control
- Best For (K-Level)
- K1-K2 (limited ambulators)
- Advantages
- Durable, low maintenance, inexpensive
- Disadvantages
- No cadence response, manual lock often needed
- Mechanism
- Multiple pivot points, shortens in swing
- Best For (K-Level)
- K2-K3 (stability needed)
- Advantages
- Inherent stance stability, toe clearance in swing
- Disadvantages
- Heavier, more complex mechanism
- Mechanism
- Fluid resistance varies with speed
- Best For (K-Level)
- K3 (variable cadence)
- Advantages
- Cadence-responsive, smooth gait at all speeds
- Disadvantages
- Heavier, requires maintenance, more expensive
- Mechanism
- Air resistance varies with speed
- Best For (K-Level)
- K3 (lighter option)
- Advantages
- Lighter than hydraulic, cadence-responsive
- Disadvantages
- Less resistance range than hydraulic
- Mechanism
- Sensors detect gait phase, adjust resistance
- Best For (K-Level)
- K3-K4 or falls risk
- Advantages
- Stumble recovery, stairs descent, reduced falls
- Disadvantages
- Expensive, battery dependent, requires training
SACH-MDRProsthetic Foot Types
Hook:Start Simple with SACH, Add Motion with axes, go Dynamic for high activity
Overview and Prosthetic Fundamentals
Prosthetic limb components are the elements that make up an artificial limb system. Understanding these components is essential for orthopaedic surgeons involved in amputation surgery and post-operative rehabilitation planning.
Key Principles of Prosthetic Prescription:
- Match components to functional level - K-level classification guides selection
- Socket fit is paramount - the interface between residual limb and prosthesis
- Suspension must be reliable - prevents pistoning and skin breakdown
- Knee and foot selection affects gait efficiency - higher function = more advanced components
- Early prosthetist involvement - ideally preoperative for optimal stump planning
Components are prescribed based on the K-Level functional classification. K0: No prosthetic ambulation. K1: Basic components for limited household use. K2: Intermediate components for limited community ambulation. K3: Advanced components for unlimited community ambulation with variable cadence. K4: High-activity components for athletes. Over-prescribing wastes resources; under-prescribing limits function.
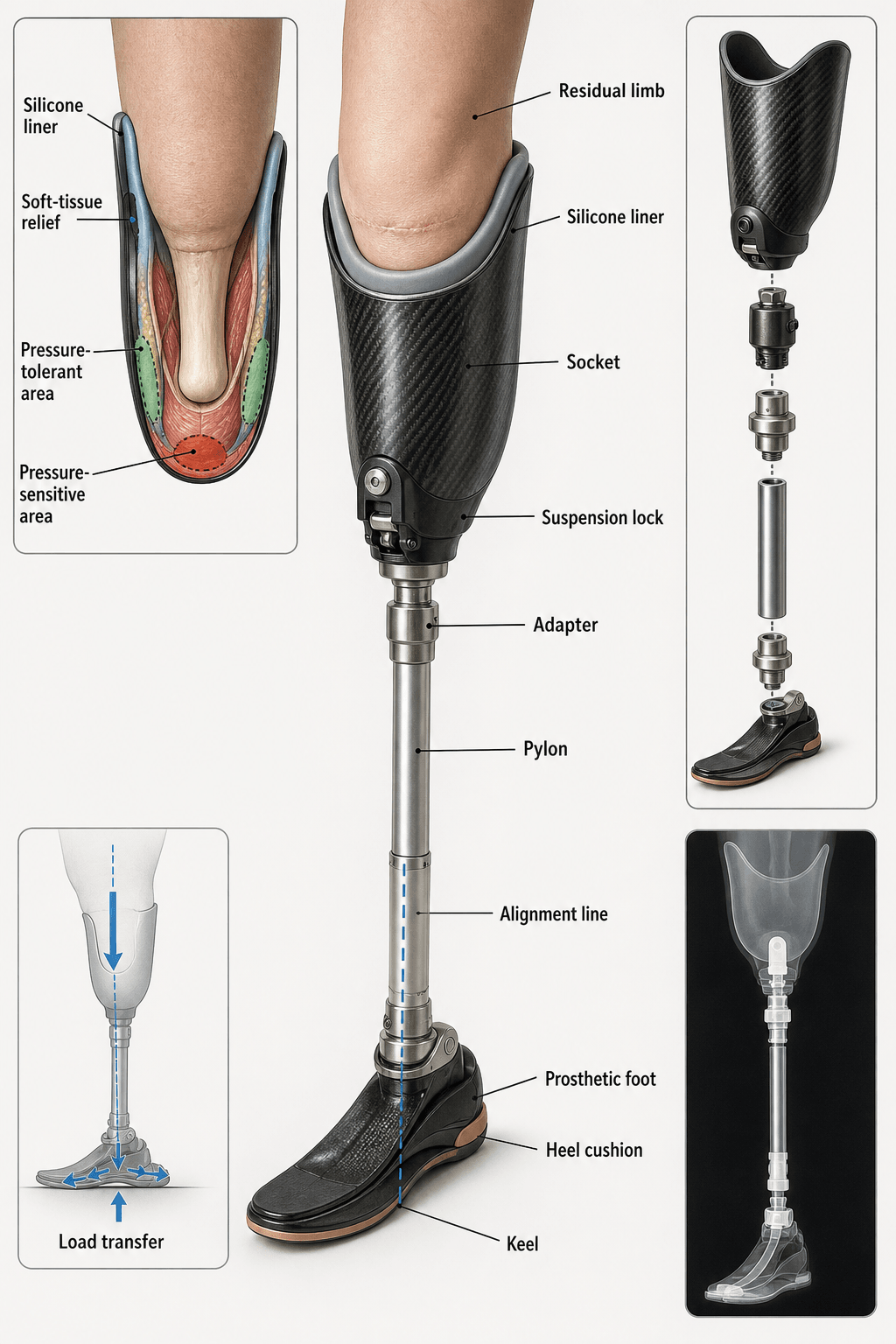
Basic Prosthetic Anatomy:
- Socket: Interface with residual limb (most critical component)
- Liner: Cushioning layer between skin and socket
- Suspension system: Keeps prosthesis attached
- Pylon/shank: Connects socket to foot (or knee to foot)
- Knee unit (transfemoral): Controls swing and stance
- Prosthetic foot: Ground contact and energy return
- Socket: Interface with residual limb
- Suspension: Harness or suction
- Elbow unit (transhumeral): Controls flexion/extension
- Wrist unit: Allows pronation/supination, quick disconnect
- Terminal device: Hook or hand for function/cosmesis
- Control system: Body-powered cables or myoelectric
Socket Design Principles
The socket is the most critical component of any prosthesis - it is the interface between the residual limb and the artificial limb. Poor socket fit leads to skin breakdown, pain, and prosthetic rejection.
Socket Design Goals
- Comfortable weight distribution - pressure on tolerant areas, relief over sensitive areas
- Stable suspension - prevents pistoning and rotation
- Proprioceptive feedback - allows control of prosthesis
- Cosmesis - acceptable appearance
- Durability - withstands daily use
Transtibial Socket Designs
- Traditional design developed in 1950s
- Weight-bearing concentrated on patellar tendon
- Pressure-tolerant areas: patellar tendon, medial tibial flare, popliteal area
- Pressure-sensitive areas (relieved): fibular head, tibial crest, distal tibia
- Total contact maintained for edema control
- Modern design distributing pressure uniformly
- No specific weight-bearing focus
- Uses gel liner to distribute pressure
- Hydrostatic loading principle - equal pressure throughout
- Often combined with suction or vacuum suspension
- PTB-SC (Supracondylar): Extended medial-lateral walls for rotational control
- PTB-SCSP (Supracondylar Suprapatellar): Higher anterior trim for suspension
- KBM (Kondylen Bettung Munster): Intimate medial-lateral contouring
PTB: Focuses weight on patellar tendon with relief areas. Traditional, still widely used. TSB: Distributes pressure over entire surface using gel liner. More comfortable for many patients. Both maintain total contact - the entire residual limb touches the socket to prevent distal edema.
PTB vs TSBSocket Types for Transtibial
Hook:PTB focuses on patellar tendon, TSB spreads load over Total Surface - both maintain full contact
Suspension Systems
Suspension keeps the prosthesis securely attached to the residual limb. Inadequate suspension leads to pistoning, reduced control, and skin problems.
- Mechanism
- Pin on liner engages lock in socket
- Advantages
- Simple, secure, easy don/doff
- Disadvantages
- Pistoning possible, milking effect on tissues
- Best For
- K1-K2, limited dexterity
- Mechanism
- Sealing lip on liner creates vacuum
- Advantages
- Intimate fit, good suspension
- Disadvantages
- Difficult don/doff, requires intact liner
- Best For
- K2-K3, good hand function
- Mechanism
- Active pump maintains negative pressure
- Advantages
- Excellent suspension, volume management
- Disadvantages
- Expensive, battery dependent, complex
- Best For
- K3-K4, volume fluctuation issues
- Mechanism
- Neoprene or gel sleeve over socket rim
- Advantages
- Simple, inexpensive, adds stability
- Disadvantages
- Hot, may irritate skin, stretches over time
- Best For
- Additional suspension, K1-K2
- Mechanism
- Socket contour locks over bony prominences
- Advantages
- No additional hardware needed
- Disadvantages
- Requires specific residual limb anatomy
- Best For
- Knee disarticulation, Syme
Suspension Selection Principles
- Suction or vacuum suspension preferred
- Intimate fit maximizes control
- Vacuum systems help with volume management
- Worth the complexity for high-activity users
- Consider elevated vacuum for variable activity
- Pin lock often most practical
- Easy donning/doffing
- Simple mechanism to understand
- Less reliance on hand dexterity
- Sleeve suspension as adjunct
Vacuum suspension with active pump provides:
- Consistent negative pressure maintaining fit
- Reduces volume fluctuation effects
- Decreases pistoning significantly
- Improves proprioceptive feedback
- May improve residual limb health
Ideal for active amputees with volume management issues. More expensive and complex than passive systems.
PINSSuspension Systems
Hook:PINS hold the prosthesis on - choose based on activity level and residual limb
Prosthetic Knee Units
Knee units are required for transfemoral, knee disarticulation, and hip disarticulation amputees. The knee must provide stability in stance and controlled motion in swing phase.
Mechanical Knee Units
- Simplest design - single pivot point
- Friction or manual lock controls motion
- Weight-activated stance control (some models)
- Durable, low maintenance, inexpensive
- Suitable for K1-K2 ambulators
- No cadence response - single walking speed
- Multiple pivot points (typically 4-bar linkage)
- Instantaneous center of rotation moves during flexion
- Inherent geometric stability in stance
- Shortens in swing phase (improved toe clearance)
- Good for long residual limbs, knee disarticulation
- More stable than single-axis
- Locked in full extension during stance
- Manually unlocked for sitting
- Maximum stability for weak or nervous ambulators
- Limited to K0-K1 function
- Stiff-legged gait
Four-bar polycentric knees offer:
- Inherent stance stability (center of rotation posterior to weight line)
- Functional shortening in swing (toe clearance)
- Cosmetic sitting position (posterior displacement)
- Good for longer residual limbs
Ideal for knee disarticulation or nervous ambulators needing stability.
Prosthetic Feet
The prosthetic foot provides ground contact, shock absorption, and energy return during gait. Selection depends on activity level, terrain requirements, and patient goals.
SACH and Basic Prosthetic Feet
- Simplest prosthetic foot design
- No moving parts - solid construction
- Compressible foam heel cushion
- Simulates ankle plantarflexion at heel strike
- Rigid forefoot (keel) for push-off
- Durable, low maintenance, inexpensive
- Suitable for K1 limited ambulators
- SACH variant with flexible keel
- Allows some forefoot flexibility
- Smoother rollover than rigid SACH
- Still no moving parts
- Heel durometer (hardness) selected for body weight
- Softer heel for lighter/less active patients
- Firmer heel for heavier/more active patients
- Waterproof, minimal maintenance
The SACH foot has no ankle joint. Ankle motion is simulated:
- Heel strike: Compressible heel cushion plantarflexes to absorb impact
- Midstance: Rigid structure provides stability
- Push-off: Stiff forefoot keel provides lever for propulsion
Simple, durable, but no energy return. Appropriate for low-activity K1 patients.
Upper Limb Prosthetics
Upper limb prosthetics present unique challenges compared to lower limb. The hand's complexity (27 bones, 18 degrees of freedom) cannot be replicated. Prosthetic options provide partial function or cosmesis.
Body-Powered Prosthetics
- Cable and harness system
- Movement of opposite shoulder or trunk
- Bowden cable transmits motion to terminal device
- Scapular abduction, humeral flexion, or chest expansion
- Figure-of-8 harness: Standard for transradial
- Figure-of-9 harness: For transhumeral, adds elbow control
- Wrist unit: Quick disconnect for terminal devices
- Terminal device: Hook or voluntary-opening hand
- Proprioceptive feedback through cable tension
- Durable and reliable
- Lower cost than myoelectric
- Waterproof options available
- Works in any environment
- Requires body motion (harness effort)
- Limited grip strength (typically 20-25 lbs)
- Visible harness system
- Can be hot and uncomfortable
Proprioceptive feedback is a key advantage of body-powered prosthetics:
- Cable tension provides sensory information
- User feels how hard they are gripping
- Important for delicate tasks
- This is lost with myoelectric prosthetics
Many long-term users prefer body-powered for this feedback.
Upper Limb Prosthetic Rejection
- Transradial: 20-30% rejection
- Transhumeral: 30-50% rejection
- Higher rejection with proximal amputation
- Insufficient function compared to remaining abilities
- Discomfort with socket and harness
- Weight of prosthesis
- Appearance concerns
- Lack of sensory feedback
- Difficulty learning myoelectric control
Keys to successful upper limb prosthetic use:
- Early fitting (within 30 days if possible)
- Comprehensive training program
- Realistic expectations counseling
- Multiple device options for different activities
- Ongoing prosthetist and therapy support
Delay beyond 6 months significantly reduces acceptance rates.
K-Level Classification and Functional Outcomes
Functional (K-Level) Classification
The K-level (functional classification, K0-K4) originated in the US Medicare system but is now used internationally as a shorthand for matching prosthetic component complexity to a patient's ambulation potential. Most funding bodies worldwide (UK NHS limb-fitting services, European social-insurance schemes, and private insurers) use the same functional concept even where the K0-K4 label is not the formal billing term.
- Functional Description
- Non-ambulatory, cannot use prosthesis
- Prosthetic Components
- Cosmetic prosthesis only, wheelchair
- Expected Outcomes
- No prosthetic ambulation expected
- Functional Description
- Household ambulator, transfers
- Prosthetic Components
- SACH foot, single-axis knee, pin suspension
- Expected Outcomes
- Limited indoor walking, standing
- Functional Description
- Limited community ambulator
- Prosthetic Components
- Multi-axis foot, polycentric knee
- Expected Outcomes
- Community distances, low obstacles
- Functional Description
- Unlimited community ambulator, variable cadence
- Prosthetic Components
- Dynamic response foot, hydraulic knee, vacuum suspension
- Expected Outcomes
- Variable speed, terrain adaptation
- Functional Description
- Active athlete, high-impact activities
- Prosthetic Components
- Carbon fiber foot, microprocessor knee, specialized sport components
- Expected Outcomes
- Running, sports, exceeds basic ambulation
Functional Assessment Tools
- Validated tool predicting prosthetic mobility potential
- 21-item assessment (without prosthesis version available)
- Scores correlate with K-level classification
- Used preoperatively and during rehabilitation
- Standard mobility measure
- Rise from chair, walk 3m, return, sit
- Greater than 19 seconds suggests falls risk
- Endurance assessment
- Distance correlates with community ambulation
- Greater than 200m suggests community ambulatory potential
- Modified TUG with turns
- More challenging than TUG
- Better predicts community mobility
K-level is determined by:
- Prior functional level (pre-amputation)
- Current physical examination
- Comorbidities and healing
- Cognitive ability
- Motivation and goals
K-level can change - reassess at follow-up. K2 patient may progress to K3 with training. Deteriorating health may reduce K-level.
K-LEVELSK-Level Functional Classification
Hook:K-LEVELS tell you what components to prescribe - higher level, higher technology
Endoskeletal versus Exoskeletal Construction
The basic-anatomy list names the 'pylon/shank' connecting socket to foot, but the body never explains the two ways a prosthesis is built around it.
- Exoskeletal ('crustacean'). The load is carried by a rigid outer shell shaped to the limb (laminated or wood). It is durable, robust and waterproof - good for heavy or harsh use - but heavy, its alignment is fixed once built, and its cosmesis is the shell shape itself.
- Endoskeletal ('modular') - the modern standard. The load is carried by an internal pylon/tube (metal or carbon) connecting socket to knee or foot, covered by a soft shaped foam cosmetic cover. It is lighter, modular (components and alignment couplings swap and adjust easily) and gives better cosmesis - at the cost of the cover and slightly less brute durability.
- Why it matters. Almost all modern limbs are endoskeletal because the adjustable alignment couplings are what let the prosthetist perform static and dynamic alignment; exoskeletal designs persist mainly where ruggedness and waterproofing outweigh adjustability. (The imaging atlas below shows an endoskeletal limb - an internal pylon with modular couplings, seen exploded and on radiograph.)
Q: What is the difference between an endoskeletal and an exoskeletal prosthesis?
A: Exoskeletal ('crustacean') = the load is borne by a rigid outer shell shaped to the limb (durable, robust, waterproof, but heavy and alignment fixed once built). Endoskeletal ('modular', the modern standard) = the load is borne by an internal pylon/tube with a soft shaped foam cosmetic cover (lighter, modular, adjustable alignment couplings, better cosmesis). Do not swap them: exoskeletal = outer shell bears load; endoskeletal = internal pylon bears load. Modern limbs are almost all endoskeletal because the adjustable couplings are what enable static and dynamic alignment.
Prosthetic Alignment
Viva 3 flags that 'malalignment affects stability', and the imaging atlas even labels the alignment line, but the body never explains what prosthetic alignment is or how it is set.
- Alignment is the spatial relationship - the angles and positions - of the socket to the knee and foot, and it is set in three stages.
- Bench alignment. The initial workshop setup: the prosthetist assembles the components to standard skeletal reference positions - built-in socket flexion and adduction, the foot under the load line, correct height - before the patient stands.
- Static alignment. With the patient standing and weight-bearing, the prosthetist checks the load (plumb) line, socket position, foot-flat and height, adjusting angles and translations for a stable, comfortable stance.
- Dynamic alignment. With the patient walking, the prosthetist fine-tunes to eliminate gait deviations and optimise stability, energy cost and cosmesis. Malalignment causes gait deviations, socket pressure and instability - and is only correctable on an endoskeletal limb with adjustable couplings.
Q: What are the three stages of prosthetic alignment?
A: Bench alignment (workshop assembly of the components to standard skeletal reference - socket flexion/adduction, foot under the load line, correct height - before the patient stands), static alignment (patient standing/weight-bearing: check the load/plumb line, socket position, foot-flat and height, adjust for a stable comfortable stance), and dynamic alignment (patient walking: fine-tune to remove gait deviations and optimise stability, energy cost and cosmesis). Malalignment causes gait deviations, socket pressure and instability, and is only correctable on an adjustable endoskeletal limb.
Differential Diagnosis: The Painful or Failing Prosthesis
A common viva and clinic scenario is the amputee who "cannot use the leg". Distinguish socket/component problems from residual-limb pathology and central pain.
- Typical Features
- Diffuse pain, pistoning, sock-ply changes through day
- Key Discriminator
- Symptoms vary with limb volume and time of day
- Management
- Sock ply adjustment, reline/recast socket, vacuum suspension
- Typical Features
- Sharp/electric focal pain, positive Tinel over a nodule
- Key Discriminator
- Reproducible point tenderness; pain on socket pressure
- Management
- Offload, desensitisation; targeted muscle reinnervation or excision if refractory
- Typical Features
- Localised distal pain, palpable hard prominence
- Key Discriminator
- Confirmed on plain radiograph
- Management
- Socket relief; surgical revision if persistent
- Typical Features
- Pain perceived in the missing limb
- Key Discriminator
- Pain in absent body part, not the residuum
- Management
- Graded motor imagery, mirror therapy, neuropathic agents
- Typical Features
- Erythema, ulcer, discharge at pressure points
- Key Discriminator
- Visible skin lesion; folliculitis with poor hygiene
- Management
- Wound care, hygiene, socket modification, treat infection
- Typical Features
- Rest pain, poor healing, cool dysvascular stump
- Key Discriminator
- Vascular history; reduced perfusion
- Management
- Vascular review; may need proximal revision
Guidelines, Registries & Global Practice
Global Epidemiology
- Dysvascular disease (with diabetes) is the dominant cause of major limb amputation worldwide; trauma predominates in younger cohorts and in many low- and middle-income countries.
- Prevalence is rising and ageing - US modelling projects a doubling of people living with limb loss by 2050 (Ziegler-Graham). Diabetes-related amputation rates vary several-fold between and within countries, reflecting screening, foot-care and revascularisation access.
- Knee preservation (transtibial over transfemoral) is the single biggest determinant of prosthetic walking energy cost and long-term function (Waters).
Guidelines & Component-Selection Frameworks (Side by Side)
- Framework
- K0-K4 functional levels tie components to ambulation potential
- Microprocessor Knee Stance
- Funded for K3-K4; emerging evidence supports selected K2
- Framework
- Functional assessment + multidisciplinary limb-fitting centres
- Microprocessor Knee Stance
- Available via specialist centres; business-case/clinical justification
- Framework
- Evidence-based CPGs (e.g. knee selection CPG, Stevens 2018)
- Microprocessor Knee Stance
- Recommended to reduce falls and cognitive load in active users
- Framework
- Standards for prosthetics services incl. limited-resource settings
- Microprocessor Knee Stance
- Prioritises durable, maintainable components where service support is scarce
Registry & Outcome Data
- Amputation/prosthetic care is less registry-driven than arthroplasty; outcomes come from limb-loss cohorts, rehabilitation databases and device-specific trials rather than national implant registries.
- Osseointegration outcomes are tracked in specialist-centre prospective series (Brånemark): high 2-year implant survival with a substantial but mostly minor stoma-infection rate.
- Validated mobility tools (AMP/AMPnoPRO, TUG, 6-minute walk, L-test) provide standardised, internationally comparable functional outcomes.
High- vs Limited-Resource Practice
- Typical practice
- Microprocessor knees, vacuum suspension, carbon-fibre dynamic feet, osseointegration in selected centres
- Drivers
- Funding, prosthetist availability, device servicing
- Typical practice
- Durable mechanical knees, SACH feet, simple pin-lock/suspension, locally manufactured sockets
- Drivers
- Cost, maintenance capacity, supply chain, ISPO appropriate-technology principles
The same functional (K-level) logic applies everywhere - match component complexity to the patient's realistic ambulation potential and to the local capacity to fit, train and maintain the device.
Controversies & Areas of Uncertainty
Long held to be reserved for K3-K4, but a systematic review (Kannenberg) found large fall reductions and speed gains in selected K2 limited community ambulators. Funders increasingly accept trial fitting to identify responders, blurring the rigid K-level cutoff.
IRC sockets give reliable coronal control but are often uncomfortable. RCT crossover data (Kahle and Highsmith) show brimless / sub-ischial designs can match skeletal control with lower medial pressure and better comfort - the "high wall is essential" dogma is being questioned.
Marketing claims of large "70-80% energy return" overstate clinical effect. Controlled data (Hsu) show single-digit to low-double-digit efficiency gains, mainly at higher speeds, and no consistent advantage of every carbon foot over SACH at slow walking.
Osseointegration removes socket problems and improves mobility/QoL but carries a high (mostly superficial) stoma-infection rate and lifelong skin-penetration risk. Patient selection, long-term implant survival and infection management remain unsettled.
Imaging Atlas
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old active male has undergone transtibial amputation for trauma 3 months ago. He is a construction worker who wants to return to work. What prosthetic components would you recommend for him?”
“A 72-year-old woman with diabetes and peripheral vascular disease has had a transfemoral amputation. She was previously mobile with a walking frame indoors only. What knee unit and foot would you recommend?”
“A 35-year-old transfemoral amputee reports multiple falls over the past 6 months, including one resulting in a hip fracture. He is currently using a mechanical hydraulic knee. What would you recommend?”
K-Level Classification
- K0: Non-ambulatory - cosmetic prosthesis only
- K1: Household ambulator - SACH foot, single-axis or manual lock knee
- K2: Limited community - multi-axis foot, polycentric knee
- K3: Unlimited community - dynamic response foot, hydraulic/microprocessor knee
- K4: Active athlete - specialized high-activity components
Socket Types
- Transtibial: PTB (patellar tendon bearing) vs TSB (total surface bearing)
- PTB focuses weight on patellar tendon, TSB distributes evenly
- Transfemoral: Quadrilateral (old) vs Ischial Containment (modern standard)
- Ischial containment provides better femoral control and gait
- All sockets should have total contact to prevent distal edema
Suspension Systems
- Pin lock: Simple, reliable, easy don/doff (K1-K2)
- Suction: Intimate fit, good for active (K2-K3)
- Vacuum (elevated): Best volume management, complex (K3-K4)
- Sleeve: Simple adjunct, can cause sweating
- Poor suspension causes pistoning and skin breakdown
Knee Units
- Single-axis: Simple, durable, no cadence response (K1-K2)
- Polycentric (4-bar): Inherent stability, shortens in swing (K2-K3)
- Hydraulic: Cadence-responsive, smooth gait (K3)
- Microprocessor (C-Leg/Genium): significant fall reduction, stumble recovery (K3-K4)
- Match knee to K-level - dont overprescribe or underprescribe
Prosthetic Feet
- SACH: Simple, no moving parts, compressible heel (K1)
- Single-axis: Plantarflexion for knee stability (K1-K2)
- Multi-axis: Terrain adaptation, inversion/eversion (K2-K3)
- Dynamic response: Carbon fiber, 70-80% energy return (K3-K4)
- Microprocessor feet: Active ankle control, stair/slope adaptation (K4)
Upper Limb Prosthetics
- Body-powered: Cable control, proprioceptive feedback, durable
- Myoelectric: EMG control, higher grip, no feedback, expensive
- Terminal devices: Hooks (functional) vs Hands (cosmetic)
- Rejection rates 20-30% for transradial, higher proximal
- Early fitting (less than 30 days) improves acceptance
Socket Problems
- Volume fluctuation: Most common - sock ply adjustment needed
- Pistoning: Socket loose or suspension inadequate
- Skin breakdown: Check fit, bony prominences, hygiene
- All problems require prosthetist review
- Socket is the most critical component - fit determines success
Evidence Base and Key Studies
Microprocessor (C-Leg) vs Mechanical Knee: Function, Performance and Preference
- A-B-A-B reversal crossover of 21 unilateral transfemoral amputees, mechanical vs Otto Bock C-Leg microprocessor knee
- Significant improvement in stair-descent score and hill-descent time with the C-Leg (P less than .01)
- Significant reduction in self-reported frequency of stumbles and falls and frustration with falling (P less than .05)
- Reduced reported difficulty multitasking while walking
- Subject satisfaction significantly greater with the C-Leg than the mechanical knee (P less than .001)
Energy Cost of Walking by Level of Amputation (Landmark Study)
- Compared gait and energy cost in 70 unilateral traumatic and vascular amputees vs 40 normal controls
- Performance was significantly better the more distal the amputation (Syme greater than below-knee greater than above-knee)
- Energy cost rises sharply moving from transtibial to transfemoral level
- Amputees self-select a slower comfortable walking speed to limit metabolic cost
- Conclusion: when preserving function, amputate at the lowest feasible level
Physiological Cost of Walking/Running with Different Prosthetic Feet
- Repeated-measures trial in 5 active unilateral transtibial amputees across treadmill walking and running speeds
- Compared SACH foot, Flex-Foot, and Re-Flex Vertical Shock Pylon (VSP)
- Re-Flex VSP improved energy cost vs SACH/Flex-Foot: ~5% walking, ~11% running
- Gait efficiency improved ~6% walking and ~9% running with the VSP
- No significant difference between Flex-Foot and SACH in this cohort
Transfemoral Socket Interface: Ischial Containment vs Brimless (RCT)
- Randomized crossover in 9 unilateral transfemoral amputees, ischial ramus containment (IRC) vs brimless socket, both with vacuum suspension
- Coronal hip angle and vertical/lateral socket movement were statistically equivalent between designs
- Medial-proximal peak socket pressure markedly lower with brimless (190 vs 322 mmHg)
- All subjects rated the brimless design more comfortable in short-term preference
- Challenges the assumption that high ischial-containment walls are essential for skeletal control
Upper Limb Prosthesis Use and Abandonment: 25-Year Survey
- Analytical survey of ~200 articles (40 reporting rejection rates), 1980-2006
- Adult rejection: ~26% body-powered and ~23% electric devices
- Paediatric rejection markedly higher: ~45% body-powered and ~35% electric
- Non-wear incidence similar in paediatric (~16%) and adult (~20%) populations
- Wide variance across studies due to heterogeneous samples and inconsistent definitions
Prosthetic Knee Selection Clinical Practice Guideline
- Evidence-based CPG synthesising systematic reviews and meta-analyses for unilateral transfemoral / knee-disarticulation knee selection
- Fluid (hydraulic/pneumatic) knees indicated for active walkers - improve comfort, speed and symmetry
- Microprocessor knees reduce stumbles, falls and cognitive demand, and increase confidence, mobility, satisfaction and metabolic efficiency
- Daily step counts and total rehabilitation cost are broadly comparable, so should not be primary selection criteria
- Even limited community ambulators may gain safety and walking-speed benefits from microprocessor knees
Microprocessor Knees for Limited Community Ambulators (Systematic Review)
- Systematic review of 6 trials, 57 K2 (MFCL-2) transfemoral amputees using microprocessor knees
- Microprocessor knees may reduce uncontrolled falls by up to 80% in this group
- Level-ground walking speed improved ~14-25% and uneven-surface speed ~20%
- Slope descent ~30% faster with a microprocessor knee
- Supports trial fitting to identify which K2 patients benefit, extending indications beyond K3-K4
Osseointegrated Percutaneous Prosthesis for Transfemoral Amputation
- Prospective single-centre study of 51 patients (55 transfemoral amputations), 2-year follow-up
- Cumulative implant survival 92% at 2 years
- Significant improvement in prosthetic use, mobility, global situation and SF-36 physical function (all P less than 0.001)
- Superficial infection was the commonest complication (54.9% of patients), mostly treated with oral antibiotics
- Implant removed in 4 patients (3 aseptic loosening, 1 infection)
Prevalence and Projected Burden of Limb Loss
- Modelled US prevalence of limb loss using national incidence and mortality data
- ~1.6 million people living with limb loss in 2005 (about 1 in 190)
- 38% of cases were dysvascular with comorbid diabetes - the dominant aetiology
- Prevalence projected to more than double to ~3.6 million by 2050
- A 10% fall in dysvascular amputation incidence would prevent ~225,000 cases