Level Selection | Myodesis vs Myoplasty | Prosthetic Considerations | Multidisciplinary Approach
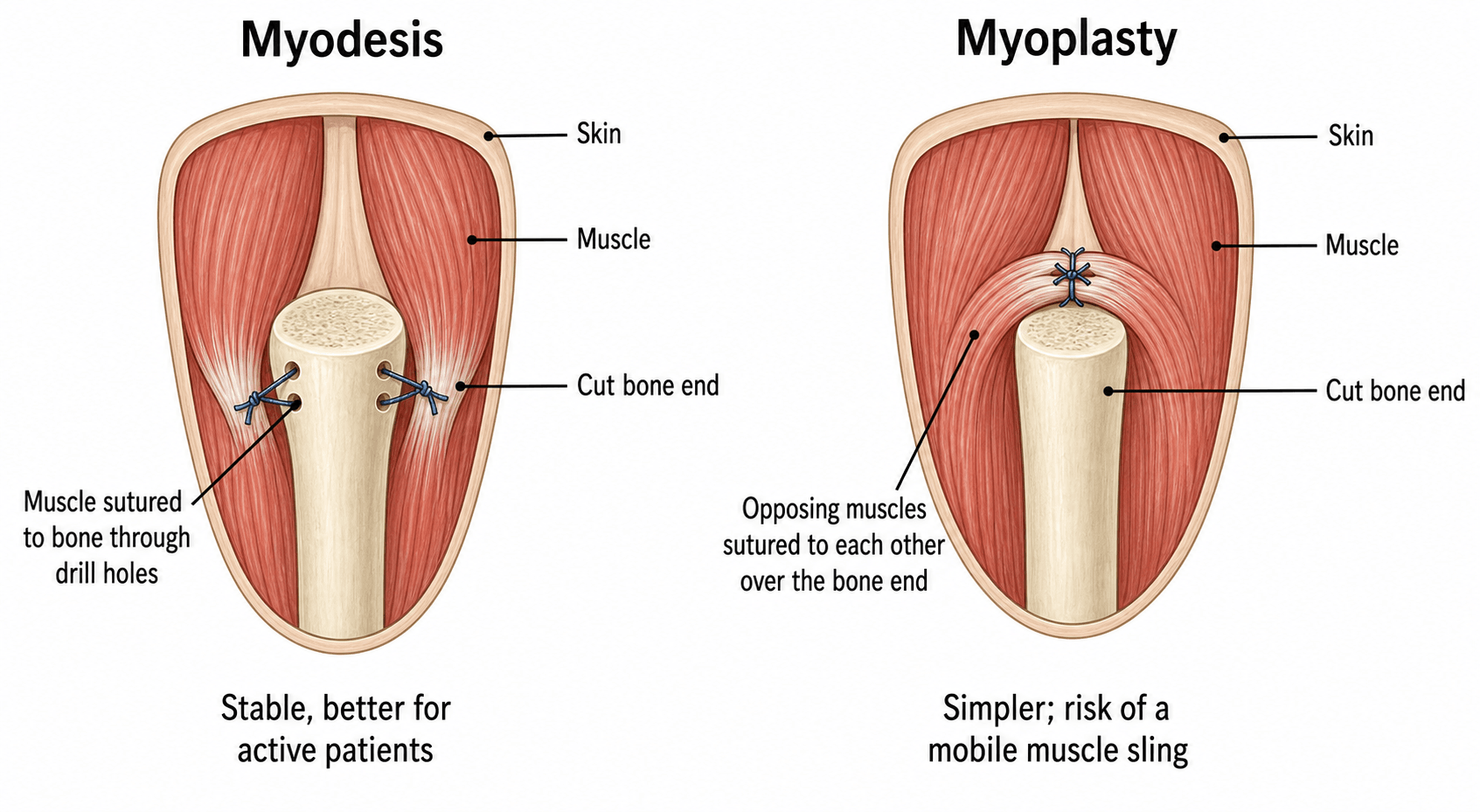
- Myodesis = muscle sutured to bone (optimal function), myoplasty = muscle to fascia/muscle
- Bone handling: Round edges, bevel tibia anteriorly, adequate bone length for lever arm
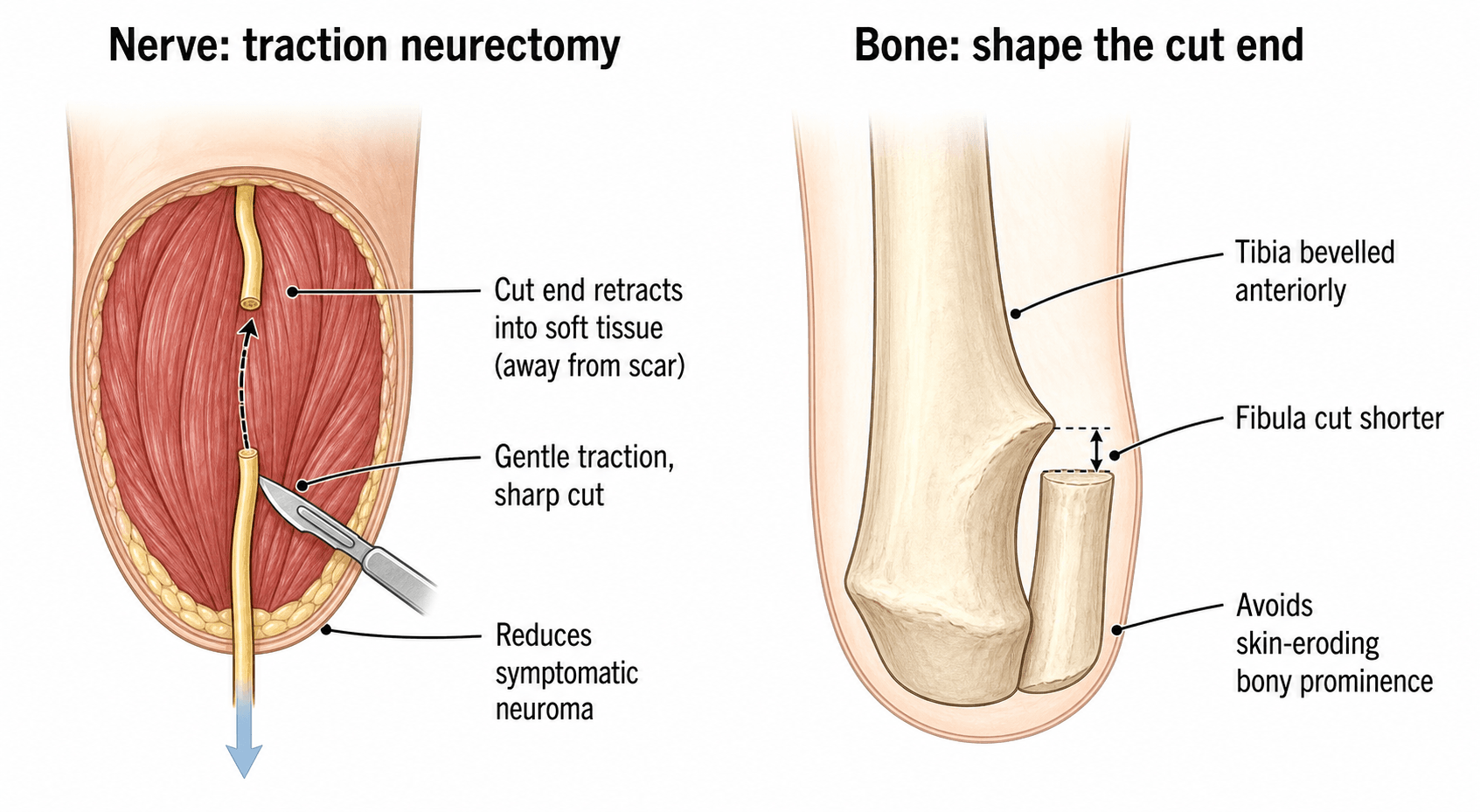
- Nerve management: Identify, transect sharply under tension, allow retraction into soft tissues
- Prosthetic consideration: Preserve joints where possible, adequate soft tissue envelope
- Phantom limb pain affects 70-80% - multifactorial, prevention with perioperative analgesia
- “Equal anterior-posterior flaps for transfemoral, longer posterior flap for transtibial
- “Maintain knee for BKA - reduces energy expenditure by 40-60% vs AKA
- “Traction neurectomy reduces neuroma pain - pull nerve, transect sharply, allow retraction
- “Staged approach for infection: guillotine then definitive closure when sepsis controlled
Preserve maximum functional length while ensuring healing. For vascular disease, balance healing potential (more proximal heals better) against function (more distal preserves joints). Knee preservation is paramount - reduces energy expenditure by 40-60% compared to transfemoral. Always consider prosthetic requirements.
Myodesis = muscle attached directly to bone through drill holes or suture anchors. Provides optimal muscle tension and proprioception. Myoplasty = muscle sutured to opposing muscle or fascia. Quicker but less stable. Myodesis is the gold standard for functional amputation - know this distinction.
Nerves: Identify major nerves, apply gentle traction, transect sharply with new blade, allow proximal retraction into soft tissues away from scar. Bone: Rasp edges smooth, bevel tibia anteriorly to prevent skin breakdown, adequate length for lever arm and prosthetic socket.
Affects 70-80% of amputees. Distinct from residual limb pain. Risk factors: preoperative pain, traumatic amputation. Prevention: perioperative epidural/nerve blocks. Treatment is multimodal - mirror therapy, gabapentinoids, antidepressants, TENS. Counsel patients preoperatively.
- Preferred Level
- Transmetatarsal or transtibial
- Key Principle
- Preserve knee if vascular supply adequate
- Prosthetic Consideration
- Short BKA still better than AKA
- Preferred Level
- Transtibial if popliteal pulse, else transfemoral
- Key Principle
- Level determined by healing potential
- Prosthetic Consideration
- Consider vascular input for level selection
- Preferred Level
- Most distal viable level
- Key Principle
- Preserve length, consider reconstruction first
- Prosthetic Consideration
- MESS score greater than 7 indicates amputation
- Preferred Level
- Transfemoral with wide margin
- Key Principle
- Oncological margin takes priority (greater than 2cm)
- Prosthetic Consideration
- Consider skip metastases, rotationplasty alternative
- Preferred Level
- Guillotine at viable level
- Key Principle
- Life before limb - emergent debridement
- Prosthetic Consideration
- Revise to definitive level when sepsis controlled
VICTIMAmputation Indications
Hook:The limb became a VICTIM of disease requiring amputation
Overview and Epidemiology
Amputation is the surgical removal of part or all of a limb. While historically considered a failure of treatment, modern amputation surgery is a reconstructive procedure aiming to create a functional residual limb optimized for prosthetic fitting and rehabilitation.
Epidemiology:
- Lower limb amputations are 10-20 times more common than upper limb
- Vascular disease (peripheral vascular disease, diabetes) accounts for approximately 80% of major amputations
- Incidence increases with age - 65% occur in patients over 65 years
- Diabetes increases amputation risk 15-40 fold
- Male predominance (2:1 ratio)
Amputation is reconstruction, not failure. The goal is to create a residual limb that maximizes function and quality of life. This requires attention to bone length, soft tissue envelope, muscle stabilization, and prosthetic considerations. A well-performed amputation with good rehabilitation can provide excellent functional outcomes.
Indications - The VICTIM Mnemonic:
- Peripheral vascular disease: Critical limb ischaemia, gangrene
- Diabetic foot disease: Infection, osteomyelitis, Charcot collapse
- Failed revascularization
- Unsalvageable tissue loss
- Trauma: Mangled extremity, irreconstructible injury (MESS greater than 7)
- Malignancy: Where limb salvage not possible, skip metastases
- Palliative amputation for fungating tumours
- Failed limb salvage with recurrence
Contraindications (Relative):
- Inadequate healing potential (assess with vascular studies)
- Unrealistic patient expectations
- Inability to participate in rehabilitation
- Life expectancy precluding benefit from rehabilitation
Pathophysiology and Wound Healing
Factors Affecting Wound Healing
Understanding the pathophysiology of wound healing is crucial for successful amputation surgery, particularly in the vascular population.
- Effect on Healing
- Reduced tissue perfusion, impaired oxygen delivery
- Clinical Implication
- Consider vascular input, may need more proximal level
- Effect on Healing
- Microangiopathy, neuropathy, impaired immunity
- Clinical Implication
- Optimize HbA1c less than 8%, aggressive infection control
- Effect on Healing
- Vasoconstriction, impaired wound healing
- Clinical Implication
- Cessation essential - increases healing by 30%
- Effect on Healing
- Albumin less than 30 g/L impairs healing
- Clinical Implication
- Nutritional optimization preoperatively
- Effect on Healing
- Uraemia impairs healing, calciphylaxis risk
- Clinical Implication
- Dialysis optimization, higher complication rates
Vascular Assessment
- Palpable pulses: Femoral, popliteal, posterior tibial, dorsalis pedis
- Tissue perfusion: Skin temperature, capillary refill, tissue viability
- Ankle-brachial index (ABI): Less than 0.4 suggests poor healing potential
- Toe pressures: Greater than 30 mmHg associated with healing
- Doppler arterial studies
- Angiography (CT or conventional) if revascularization considered
- Transcutaneous oxygen tension (TcPO2): Greater than 30-40 mmHg predicts healing
The most distal level that will heal should be chosen. However, a failed distal amputation requiring revision is worse than a primary proximal amputation. Vascular surgery input is essential - consider revascularization to enable more distal amputation. TcPO2 greater than 30-40 mmHg at proposed level predicts healing.
Phantom Limb Phenomena
- Non-painful awareness of amputated limb
- Universal after amputation
- Usually diminishes over time
- Painful sensations perceived in the amputated limb
- Affects 70-80% of amputees
- Can be immediate or delayed onset
- Character: burning, cramping, shooting, stabbing
- Peripheral mechanisms: Neuroma formation, ectopic discharge
- Spinal cord changes: Dorsal horn sensitization
- Cortical reorganization: Somatosensory cortex remapping
- Central sensitization: Altered pain processing
Patients with significant preoperative pain have higher rates of phantom limb pain. This supports the hypothesis that central sensitization occurs before amputation. Perioperative epidural or peripheral nerve blocks may reduce phantom pain incidence.
Classification and Decision Tools
The "classification" relevant to amputation is the set of validated scores and grading systems that drive the salvage-versus-amputation decision and the choice of level. Know what each tool measures and, crucially, what it changes in management.
Limb-Injury Severity Scores
Four components - skeletal/soft-tissue injury (1-4), limb ischaemia (1-3, doubled if more than 6 hours), shock (0-2) and age (0-2). A score of 7 or more has historically been associated with amputation.
MESS flags a high-risk limb but must not be used in isolation - the LEAP study showed scores have limited predictive value for the final salvage decision. Plantar sensation and the patient's physiology weigh heavily.
Limb Salvage Index, NISSSA, Predictive Salvage Index and Hannover Fracture Scale exist but none is sufficiently sensitive and specific to mandate amputation alone.
Clinical Presentation and Assessment
Indications by Aetiology
Vascular Disease and Diabetes
- Critical limb ischaemia with rest pain
- Gangrene (dry or wet)
- Non-healing ulcers despite revascularization
- Failed bypass or angioplasty
- Extensive tissue loss precluding reconstruction
- Vascular surgery consultation
- Consider revascularization to enable more distal amputation
- Optimize medical comorbidities (diabetes, cardiac disease)
- Nutritional assessment
- TcPO2 greater than 30-40 mmHg predicts healing
- Palpable pulse at level above amputation favourable
- When in doubt, vascular opinion essential
Differential Diagnosis - The Threatened Limb
Before committing to amputation, distinguish the irretrievable limb from conditions that mimic it but may be salvageable with timely intervention. Misclassifying a salvageable limb leads to unnecessary amputation; missing an unsalvageable septic limb risks life.
- Key features
- Pain, pallor, pulselessness, paraesthesia, paralysis, perishing cold
- Discriminator
- Rutherford category; sensory/motor loss and muscle tenderness signal advanced ischaemia
- Salvageable?
- Often, if revascularised within the viable window
- Key features
- Rest pain, non-healing ulcer, gangrene; low ABI/toe pressure
- Discriminator
- Perfusion testing (TcPO2, angiography); revascularisation potential
- Salvageable?
- Sometimes; revascularise to enable a distal level
- Key features
- Pain out of proportion, systemic toxicity, crepitus, skin changes, raised lactate
- Discriminator
- LRINEC score, gas on imaging, finger test at surgery - this is a surgical emergency
- Salvageable?
- Limb sometimes; life takes priority - debride or guillotine
- Key features
- Combined bone, soft-tissue, vascular and nerve injury
- Discriminator
- MESS and clinical judgement; plantar sensation and warm-ischaemia time
- Salvageable?
- Often reconstructable; outcomes equivalent to amputation [see LEAP]
- Key features
- Tense compartments, pain on passive stretch, evolving sensory loss
- Discriminator
- Clinical diagnosis +/- compartment pressures - fasciotomy can save the limb
- Salvageable?
- Yes if decompressed early - do not amputate a salvageable limb
- Key features
- Deep mass, night pain, pathological fracture, abnormal radiograph
- Discriminator
- Staging MRI of whole bone and biopsy before any surgery
- Salvageable?
- Often limb-salvage; amputation only if salvage not oncologically safe
Preoperative Assessment Checklist
- Vascular assessment: ABI, toe pressures, TcPO2
- Cardiac optimization: Functional status, echo if indicated
- Diabetes control: HbA1c target less than 8%
- Nutrition: Albumin greater than 30 g/L
- Smoking cessation: Refer to Quitline
- Prosthetist: Early involvement for level planning
- Physiotherapy: Preoperative conditioning, wheelchair training
- Occupational therapy: Home assessment, equipment needs
- Psychology: Counselling for body image, grief
- Social work: Discharge planning, support services
Investigations
Investigation Protocol for Amputation Planning
Essential for vascular amputations:
- Ankle-brachial index (ABI): Less than 0.4 suggests poor healing
- Toe pressures: Greater than 30 mmHg associated with healing
- Duplex ultrasound: Assess arterial and venous patency
- CT angiography: If revascularization being considered
- TcPO2: Greater than 30-40 mmHg at proposed level predicts healing
- Plain radiographs of affected limb
- Assess bone quality, level of disease
- For trauma: Full trauma series
- MRI whole bone (skip metastases)
- CT chest (staging)
- PET scan if indicated
Preoperative baseline:
- Full blood count, coagulation studies
- Urea, electrolytes, creatinine
- HbA1c (diabetes control)
- Albumin, prealbumin (nutrition)
- CRP, ESR (infection)
- Blood cultures if sepsis suspected
Multidisciplinary team:
- Vascular surgery: Level selection, revascularization options
- Prosthetist: Early involvement for optimal stump planning
- Anaesthesia: Perioperative nerve blocks (phantom pain prevention)
- Pain service: Preoperative pain management plan
Transcutaneous oxygen tension (TcPO2) is a useful predictor of healing. TcPO2 greater than 40 mmHg has high probability of healing. TcPO2 less than 20 mmHg predicts healing failure. Between 20-40 mmHg is indeterminate - clinical judgment required.
Management Principles

Level Selection Principles
Goals:
- Most distal level that will heal
- Preserve joints where possible (especially knee)
- Adequate bone length for prosthetic lever arm
- Sufficient soft tissue for durable coverage
- Consider prosthetic requirements
- Indications
- Localized gangrene, osteomyelitis
- Advantages
- Preserves foot function, no prosthesis needed
- Disadvantages
- High revision rate in vascular disease
- Indications
- Forefoot gangrene, diabetic foot
- Advantages
- Ambulation without prosthesis possible
- Disadvantages
- Equinovarus deformity risk, healing issues
- Indications
- Ankle pathology, heel pad viable
- Advantages
- End-bearing, long lever arm
- Disadvantages
- Cosmesis issues, requires experienced surgeon
- Indications
- Most common major amputation
- Advantages
- Preserves knee - 40-60% less energy vs AKA
- Disadvantages
- Higher revision rate in PVD than AKA
- Indications
- Long femoral stump not possible
- Advantages
- End-bearing, long lever arm, no bone cut
- Disadvantages
- Bulky prosthetic knee, limited cosmesis
- Indications
- Knee preservation not possible
- Advantages
- High healing rate (90%+)
- Disadvantages
- Significant energy expenditure increase
- Indications
- Proximal thigh tumour, trauma
- Advantages
- Complete limb removal
- Disadvantages
- Very high energy expenditure, limited prosthetic use
Knee preservation is paramount. Energy expenditure for ambulation with transtibial amputation is 40-60% less than transfemoral. Even a short transtibial amputation is preferable to transfemoral if healing is achievable. Vascular input is essential for level decisions.
Level selection in the dysvascular limb is not only about how proximal to go but about which tissue is actually perfused. The angiosome concept divides the limb into three-dimensional blocks of skin and deeper tissue, each fed by a named source artery — in the foot the posterior tibial artery supplies the heel and plantar/medial angiosomes, the anterior tibial/dorsalis pedis the dorsum, and the peroneal the lateral hindfoot and lateral ankle. The practical message for amputation and flap design is that a stump or foot amputation will heal only if its skin lies in an angiosome whose source artery (or a robust collateral) is patent — so a heel wound fed by an occluded posterior tibial artery heals poorly even when other vessels are open, and direct (angiosome-targeted) revascularisation of the artery feeding the wound improves healing and may permit a more distal level. This complements rather than replaces global perfusion tests (TcPO2, toe pressures): the global test tells you whether enough blood reaches the limb, the angiosome map tells you whether it reaches this flap.
MIRRORSPhantom Limb Pain Management
Hook:Use MIRRORS to treat phantom pain - mirror therapy is evidence-based
Surgical Technique
Transtibial (Below-Knee) Amputation
- Most common major amputation
- Vascular disease with viable knee
- Trauma with adequate proximal tissue
- Infection controlled at this level
- Confirm vascularity (clinical, TcPO2)
- Mark level: Minimum 12-15 cm from tibial tuberosity
- Posterior flap length = 1.5 times AP diameter of leg
Transtibial Amputation Steps
Supine position, tourniquet if applicable (avoid in PVD).
Mark level at junction of proximal and middle third of tibia.
Mark anterior fish-mouth incision.
Posterior flap: One-third circumference of leg, extending distally.
Incise skin and deep fascia anteriorly.
Identify and ligate anterior tibial vessels.
Identify deep peroneal nerve - transect sharply under tension.
Divide anterior compartment muscles.
Tibia: Score periosteum, cut with oscillating saw.
Create 45-degree anterior bevel to prevent skin pressure.
Fibula: Cut 1-2 cm shorter than tibia.
Rasp all bone edges smooth.
Create long posterior myocutaneous flap.
Based on gastrocnemius and soleus (soleus often trimmed).
Identify and ligate posterior tibial and peroneal vessels.
Identify tibial and sural nerves - transect sharply under tension.
Drill holes in anterior tibia.
Suture posterior muscle flap to anterior tibia (myodesis).
Close deep fascia over muscle.
Skin closure: Interrupted or subcuticular, no tension.
Apply soft dressing, rigid cast, or IPOP (immediate post-op prosthesis).
Technical Pearls:
- Long posterior flap: Gastrocnemius provides durable, well-vascularized coverage
- Nerve handling: Gentle traction, sharp transection, allow retraction
- Hemostasis: Meticulous - haematoma increases infection risk
- No drain vs drain: Surgeon preference; drain if large dead space
FLAPSTranstibial Amputation Technique
Hook:Good FLAPS make a good stump - posterior flap is key for BKA
Complications
Wound-Related Complications
- Incidence
- 10-15%
- Risk Factors
- Diabetes, PVD, malnutrition
- Management
- Antibiotics, drainage, debridement if needed
- Incidence
- 5-10%
- Risk Factors
- Tension closure, poor vascularity
- Management
- VAC therapy, revision if extensive
- Incidence
- 5-20% (higher in PVD)
- Risk Factors
- Inadequate blood supply, wrong level
- Management
- Debridement, may need more proximal revision
- Incidence
- 5%
- Risk Factors
- Poor haemostasis, anticoagulation
- Management
- Aspiration or surgical evacuation
Revision Amputation:
- Required in 5-30% depending on level and indication
- Higher revision rates with more distal amputations in PVD
- Consider vascular surgery input before revision
Postoperative Care and Rehabilitation
Rehabilitation begins on day one and is as important as the operation. The residual limb must be protected, shaped and conditioned while the patient is mobilised and prepared psychologically and physically for a prosthesis.
Rehabilitation Pathway After Major Amputation
Protect the residual limb (soft dressing, rigid dressing or immediate post-operative prosthesis per local protocol). Control pain with multimodal and regional analgesia to limit central sensitisation. Prevent contracture by avoiding prolonged knee/hip flexion and encouraging prone lying. Commence bed mobility, transfers and upper-limb strengthening. Venous thromboprophylaxis and early sitting.
Monitor wound healing and watch for infection or dehiscence. Begin residual-limb oedema control with elastic shrinker or compression once the wound is stable. Desensitisation and scar management. Wheelchair independence and standing balance. Early prosthetist review for casting timing.
Fit an interim/preparatory prosthesis once the limb is healed and oedema settled. Progressive gait re-education, energy-efficient walking and falls prevention. Address phantom and residual limb pain proactively. Occupational therapy for activities of daily living and home modification.
Definitive prosthesis once limb volume stabilises. Functional, vocational and recreational goals; return to work and driving assessment. Long-term follow-up of skin, socket fit, the contralateral limb and cardiovascular risk.
After a dysvascular amputation the remaining limb is at high risk - up to half of patients undergo contralateral amputation within a few years. Lifelong foot protection, vascular surveillance, glycaemic and smoking-risk control are essential, not optional.
Outcomes and Prognosis
Outcomes after major amputation depend on the indication, the level, the patient's physiology and the quality of rehabilitation. Survival in the dysvascular population is sobering and must inform honest preoperative counselling.
- Typical finding
- High after major (especially above-knee) amputation in vascular patients; in-hospital mortality after above-knee amputation around 10% in registry data [SerbVasc]
- Main determinants
- Age, cardiac/renal disease, emergency presentation
- Typical finding
- Markedly reduced in dysvascular amputees; many do not survive beyond a few years
- Main determinants
- Cardiovascular comorbidity, diabetes, renal failure
- Typical finding
- Rises with more proximal level; transtibial far more efficient than transfemoral [Waters]
- Main determinants
- Level, age, fitness, prosthetic technology
- Typical finding
- Better with knee preservation and good rehabilitation; many transtibial amputees regain community walking
- Main determinants
- Level, cognition, comorbidity, rehab access
- Typical finding
- Equivalent 2-year function for amputation and reconstruction in severe trauma [LEAP]
- Main determinants
- Psychosocial factors, complications, return to work
The strongest predictors of a poor patient-reported outcome after limb-threatening injury are not the surgical choice but self-efficacy, smoking, social support and socioeconomic factors - directly from the LEAP study. Set realistic expectations and mobilise psychosocial support early.
Guidelines, Registries & Global Practice
Global Epidemiology
Lower-limb amputation is overwhelmingly driven by dysvascular disease and diabetes worldwide. The Global Burden of Disease analysis estimated that 131 million people (1.8% of the world population) were living with diabetes-related lower-extremity complications in 2016, contributing 16.8 million years lived with disability, with age-standardised disability rates rising 14.6% to 31.0% since 1990. [1] Men and people aged 50 to 69 years carry a disproportionate share of the burden. [1]
- Vascular disease and diabetes are the dominant indications in high- and middle-income settings (the large majority of major amputations)
- Trauma, infection and tumour dominate in younger patients and in conflict / limited-resource settings
- Lower-limb amputations greatly outnumber upper-limb
- Incidence rises steeply with age and with diabetes duration
- Marked variation between and within countries reflects access to vascular and foot-protection services [1]
- Indigenous, socially deprived and rural populations consistently show higher amputation rates and more proximal levels
- Outcome is driven as much by psychosocial factors (self-efficacy, smoking, support) as by surgery [2]
- Multidisciplinary diabetic-foot and limb-preservation services reduce major amputation rates
- Early prosthetic and rehabilitation access improves return to walking and work [3]
- Smoking cessation improves wound healing and is universally recommended
Guidelines and Recommendations (side by side)
- Key recommendation
- Structured perfusion assessment before amputation; revascularise where feasible; multidisciplinary foot service to prevent major amputation
- Evidence emphasis
- TcPO2 / perfusion testing for level and healing [4]
- Key recommendation
- Vascular and diabetic-foot MDT input before major amputation; early rehabilitation and prosthetic referral; manage pain pre-emptively
- Evidence emphasis
- Service-level, MDT and rehabilitation pathways
- Key recommendation
- Individualise reconstruction versus amputation in trauma; MESS and scores guide but do not dictate; preserve functional length
- Evidence emphasis
- LEAP-informed shared decision making [2]
- Key recommendation
- Assess and optimise perfusion before level selection; consider revascularisation to enable a more distal level
- Evidence emphasis
- Perfusion-based level selection [4]
- Key recommendation
- No flap design proven superior to long posterior flap; stage the procedure in wet gangrene
- Evidence emphasis
- RCT-level evidence on incision type [5]
Registry and Practice Variation
National vascular and amputation registries (for example Vascunet-linked registries such as the UK National Vascular Registry, the Swedish Swedvasc, and emerging registries such as SerbVasc) consistently report that major lower-limb amputation carries high perioperative mortality (in-hospital mortality after above-knee amputation of the order of 10%) and that only a minority of patients undergoing amputation have had prior revascularisation, highlighting late presentation of peripheral arterial disease. [6] Registry data drive quality-improvement targets to reduce avoidable major amputation through earlier diagnosis and limb-preservation pathways.
Regional example (Australia and New Zealand): State amputee-rehabilitation units provide early prosthetist assessment, physiotherapy gait training, occupational therapy, psychology and social-work support. Prosthetics and rehabilitation are publicly subsidised (including via the NDIS), and peer-support organisations such as Limbs 4 Life assist adjustment. Indigenous Australians experience substantially higher amputation rates linked to higher diabetes prevalence, later presentation and reduced access to preventive care, mirroring the global disparity pattern. [1]
Smoking cessation should be offered to all patients before amputation. Continued smoking impairs wound healing and is associated with worse outcomes after limb-threatening injury. [2] Nicotine-replacement therapy and structured cessation support (for example national quit services such as Quitline) should be provided wherever available.
References
- Zhang Y, Lazzarini PA, McPhail SM, et al. Global Disability Burdens of Diabetes-Related Lower-Extremity Complications in 1990 and 2016. Diabetes Care. 2020;43(5):964-974. doi:10.2337/dc19-1614
- Bosse MJ, MacKenzie EJ, Kellam JF, et al. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002;347(24):1924-31. doi:10.1056/NEJMoa012604
- Waters RL, Perry J, Antonelli D, Hislop H. Energy cost of walking of amputees: the influence of level of amputation. J Bone Joint Surg Am. 1976;58(1):42-6. PMID 1249111
- Wang Z, Hasan R, Firwana B, et al. A systematic review and meta-analysis of tests to predict wound healing in diabetic foot. J Vasc Surg. 2016;63(2 Suppl):29S-36S. doi:10.1016/j.jvs.2015.10.004
- Tisi PV, Than MM. Type of incision for below knee amputation. Cochrane Database Syst Rev. 2014;(4):CD003749. doi:10.1002/14651858.CD003749.pub3
- Tanaskovic S, Ilijevski N, Koncar I, et al. Analysis of Lower Extremity Amputations from the SerbVasc Registry. J Endovasc Ther. 2023;32(4):1018-1026. doi:10.1177/15266028231199919
MCQ Practice Points and Exam Traps
High-yield, examinable facts and the errors examiners most often probe.
- Vascular disease and diabetes cause the large majority of major amputations worldwide
- Transtibial walking energy cost is far lower than transfemoral - preserve the knee
- Myodesis (muscle to bone) is superior to myoplasty for function and limb shape
- Long posterior flap (Burgess) is the established transtibial technique; no flap proven superior (Cochrane)
- Phantom limb pain affects most amputees; pre-emptive analgesia and mirror therapy have evidence
- LEAP: reconstruction and amputation give equivalent 2-year function in severe trauma
- Quoting MESS as an absolute amputation threshold - it guides, it does not dictate
- Confusing phantom limb pain (central) with residual limb pain (local cause)
- Recommending opioids first-line for phantom limb pain
- Forgetting adductor myodesis in transfemoral amputation (prevents abduction drift)
- Closing under tension or omitting the anterior tibial bevel
- Ignoring the contralateral limb and cardiovascular mortality risk
Expect to be pushed from "what" to "why": why preserve the knee (energy cost - Waters), why myodesis over myoplasty (tension, proprioception, shape), why stage a wet-gangrene amputation (better stump healing - Cochrane), and why pre-emptive analgesia (limits central sensitisation - Karanikolas). Always end with the multidisciplinary team and honest prognostic counselling.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old diabetic male presents with wet gangrene of his left foot extending to the mid-foot. He has had a failed femoral-popliteal bypass 6 months ago. His ankle-brachial index is 0.3 and toe pressures are unrecordable. How would you manage this patient?”
“Describe the surgical technique for transtibial amputation, focusing on the key principles that optimize prosthetic function.”
“A patient 6 months post-transfemoral amputation complains of severe burning pain in their absent leg. How would you assess and manage this patient?”
Indications (VICTIM)
- Vascular: PVD, diabetes - 80% of amputations
- Infection: Uncontrolled sepsis, necrotizing fasciitis
- Congenital: PFFD, fibular hemimelia
- Trauma: Mangled extremity, MESS greater than 7
- Ischaemia: Irreversible, failed revascularization
- Malignancy: Limb salvage not possible
Level Selection
- Most distal level that will heal
- Preserve knee - 40-60% less energy vs AKA
- TcPO2 greater than 30-40 mmHg predicts healing
- Vascular surgery input essential for PVD
- Minimum 12-15 cm from tibial tuberosity (BKA)
Technique Principles
- Myodesis: Muscle to bone (gold standard)
- Myoplasty: Muscle to muscle/fascia (quicker)
- Long posterior flap for BKA (Burgess)
- 45-degree anterior tibial bevel
- Traction neurectomy: Pull, sharp transect, retract
Nerve Management
- Identify nerve proximally
- Apply gentle longitudinal traction
- Transect sharply with fresh blade
- Allow retraction into soft tissues
- Position away from scar and pressure
Phantom Limb Pain
- Affects 70-80% of amputees
- Risk factor: Preoperative pain
- First-line: Gabapentinoids
- Mirror therapy: Strong evidence (NEJM 2007)
- Prevention: Perioperative regional analgesia
Complications
- Wound failure: 5-20% (higher in PVD)
- Revision rate: 5-30% depending on level
- Contractures: Prevent with early PT
- Neuroma: Tinel sign, desensitization/injection
- Depression: 30-50%, early psych support
Evidence Base and Key Studies
LEAP Study - Reconstruction vs Amputation in Leg-Threatening Trauma
- Multicentre prospective observational study of 569 patients with severe leg injuries treated by reconstruction or amputation
- No significant difference in Sickness Impact Profile at 2 years (12.6 amputation vs 11.8 reconstruction, P=0.53)
- Reconstruction patients were more often rehospitalised for a major complication (47.6% vs 33.9%, P=0.002)
- Return-to-work rates were similar at 2 years (53.0% amputation vs 49.4% reconstruction)
- Poorer outcomes were predicted by low self-efficacy, smoking, poverty and lack of social support rather than treatment chosen
Cochrane Review - Type of Incision for Below-Knee Amputation
- Systematic review of 3 RCTs (309 participants) comparing skin-incision techniques for below-knee amputation in ischaemia or diabetic foot sepsis
- Skew flaps and sagittal flaps conferred no advantage over the established long posterior flap (Burgess) technique (primary stump healing 60% for both skew and posterior flaps, RR 1.00)
- In wet gangrene, a two-stage procedure (guillotine then definitive long posterior flap) gave better primary stump healing than a single-stage operation (Peto OR 0.08)
- Reamputation, wound infection and prosthetic mobility were similar across flap designs
- Overall evidence quality moderate; incision choice can be guided by surgeon experience and tissue viability
Mirror Therapy for Phantom Limb Pain
- Randomised trial in 22 lower-limb amputees comparing mirror therapy, a covered (opaque) mirror and mental visualisation over 4 weeks
- The mirror-therapy group had a significant reduction in phantom limb pain
- Pain worsened or did not improve in the covered-mirror and mental-visualisation groups
- On crossover, patients who switched to mirror therapy also improved
- Proposed mechanism: visual feedback resolves the sensorimotor cortical conflict; the intervention is simple and low-cost
Optimised Perioperative Analgesia and Phantom Limb Pain
- Randomised controlled trial in 65 lower-limb amputees comparing five analgesic regimens, with epidural or intravenous PCA started 48 hours before surgery and continued 48 hours afterwards
- At 6 months, phantom limb pain was present in 1 of 13 patients receiving perioperative epidural analgesia versus 9 of 12 controls (P=0.001)
- Optimised epidural and intravenous-PCA regimens reduced phantom limb pain intensity, prevalence and frequency
- Severe pre-amputation pain was associated with phantom limb pain development
- Proposed mechanism: pre-emptive blockade limits central sensitisation
Targeted Muscle Reinnervation for Postamputation Pain (RCT)
- First surgical RCT (28 major-limb amputees) comparing targeted muscle reinnervation (TMR) with standard neuroma excision and muscle burial
- In mixed-model analysis the reduction in phantom limb pain was significantly greater with TMR (mean difference 3.5 on a 0-10 scale, P=0.03)
- Residual limb pain also trended in favour of TMR
- TMR redirects transected nerves into motor nerve branches, giving them a target and reducing symptomatic neuroma
- Supports a shift toward active nerve management at the time of amputation
Energy Cost of Walking by Amputation Level
- Classic gait-laboratory study of 70 unilateral traumatic and vascular amputees plus 40 normal controls
- Energy cost of prosthetic walking rose progressively with more proximal amputation level (lowest for Syme, then transtibial, highest for transfemoral)
- Performance was significantly better the lower the level of amputation in both traumatic and vascular groups
- Vascular amputees walked more slowly and at higher relative energy cost than traumatic amputees
- Provides the physiological basis for preserving the knee whenever healing allows
TcPO2 and Tests to Predict Healing (Meta-analysis)
- Systematic review and meta-analysis of 37 studies of non-invasive tests predicting wound healing and amputation risk in diabetic foot
- Transcutaneous oxygen measurement (TcPO2) had a pooled diagnostic odds ratio of 15.81 for wound healing and 4.14 for amputation risk
- Ankle-brachial index predicted amputation risk (DOR 2.89) but not wound healing
- TcPO2 and ABI were the most studied and most useful tests for level selection
- Overall evidence quality was low, limited by bias and small samples