Segmental Defects | Distraction Osteogenesis | Docking Site
- Transport rate: 1mm/day standard, same as lengthening
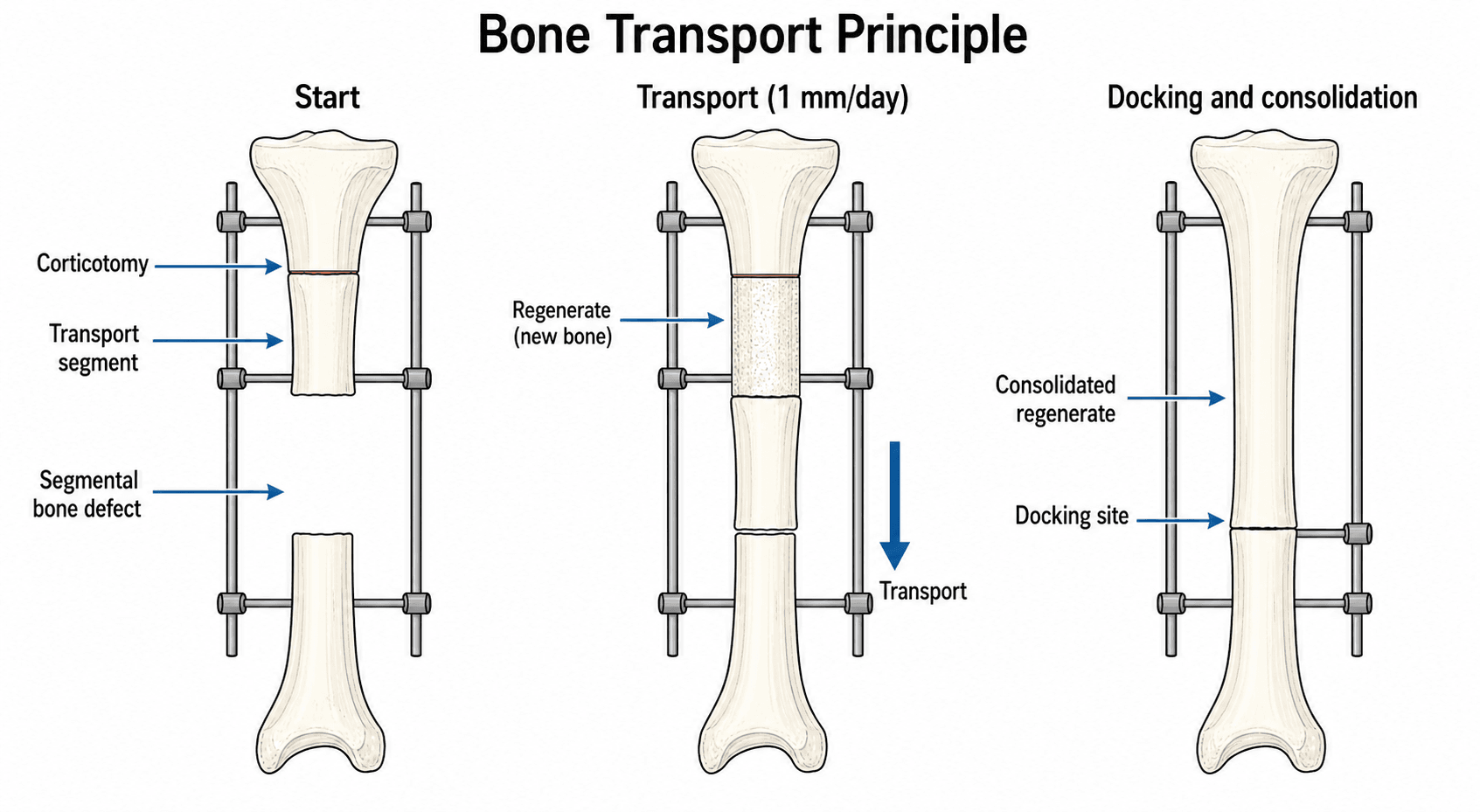
- Docking site: Where transported segment meets target - often requires bone graft
- Regenerate: New bone forming at osteotomy site during transport
- Bifocal: Two osteotomies halve the transport distance each segment travels
- Shortening-lengthening: Alternative for infected defects - acute shortening then gradual lengthening
- “Defects greater than 4cm generally require transport rather than bone graft alone
- “Docking site union is the Achilles heel - expect 25-50% need bone grafting
- “Infected nonunion: Debride, external fixation, transport through healthy bone
- “Consider prophylactic fibular osteotomy for tibial transport
The docking site is where the transported bone meets the target bone. Union here is unpredictable. Plan for bone grafting in 25-50% of cases. Options: Autograft, refresh ends, compression across site, combined approach.
Segmental bone loss greater than 4cm - transport preferred over bone grafting alone. Also for: post-traumatic defects, tumor resection gaps, infected nonunion with bone loss. Consider patient factors and compliance.
Regenerate (at osteotomy site) - usually heals well if biology preserved. Docking site - often problematic, avascular bone ends meeting. Different management: Regenerate = distraction principles; Docking = bone graft principles.
Total time = Transport time + Consolidation time. Transport = defect size / 1mm per day. Consolidation = 1 month per cm of transport (regenerate). Docking site adds time. May be 6-18 months total.
Overview and Epidemiology
Bone transport is a technique using distraction osteogenesis to move a bone segment across a defect, generating new bone in its wake. Developed from Ilizarov's principles, it is the definitive treatment for segmental bone defects not amenable to conventional bone grafting.
- Segmental bone loss greater than 4cm
- Post-traumatic bone defects
- Post-tumor resection reconstruction
- Infected nonunion with bone loss
- Congenital pseudarthrosis
- Uses patient's own regenerative capacity
- No donor site morbidity for large grafts
- Can address defects larger than available graft
- Simultaneous soft tissue regeneration
- Can be combined with infection treatment
- Prolonged treatment time (months)
- Pin site complications
- Technical complexity
- Patient compliance required

Pathophysiology
Biology of Bone Transport
- New bone forms at the corticotomy site during transport
- Same principles as limb lengthening
- Rate 1mm/day preserves biology
- Regenerate consolidates after transport complete
- Two bone ends meeting - often avascular
- Variable healing potential
- May have fibrous interposition
- Frequently requires augmentation
Transport Methods
- Single osteotomy proximal or distal to defect
- Transport segment moves across defect
- Simple technique, longer transport distance
- Docking site at one end
- Two osteotomies, one at each end of defect
- Two segments transport toward middle
- Each segment moves half the distance
- Docking site in middle of defect
- Three osteotomies
- Central segment transported, end segments moved in
- For very large defects
- Complex but faster
An alternative to transport for infected defects: Acutely shorten the limb to achieve bony contact and compression, then gradually re-lengthen through a distant osteotomy. Avoids transport through infected zone and provides compression at nonunion site.
Classification Systems
Bone transport itself is described by the number of osteotomies (focal level), but the defect and host are classified by widely used trauma and reconstruction systems that drive decision-making.
- What it classifies
- Number of corticotomies and transported segments
- Why it matters for transport
- Determines transport distance per segment and overall frame time
- What it classifies
- Open fracture soft-tissue injury (I to IIIC)
- Why it matters for transport
- IIIB/IIIC predict bone loss and the need for orthoplastic cover before transport
- What it classifies
- Osteomyelitis anatomy (1 to 4) and host (A/B/C)
- Why it matters for transport
- Defines extent of debridement and resultant defect; B/C hosts heal poorly
Cierny-Mader Classification of Osteomyelitis
When bone transport follows an infected nonunion, the Cierny-Mader classification named above determines how much bone must be resected and whether the host can heal a reconstruction at all. It combines an anatomic type with a physiological host class.
- Anatomy
- Endosteal / intramedullary infection (e.g. haematogenous, infected nail)
- Relevance to transport
- Debridement is intramedullary; usually no segmental defect
- Anatomy
- Cortical surface infection contiguous from a soft-tissue focus or ulcer
- Relevance to transport
- Needs soft-tissue cover; limited bone loss
- Anatomy
- Full-thickness cortical sequestrum, but bone stable after debridement
- Relevance to transport
- Cavity or partial defect; may need graft rather than transport
- Anatomy
- Through-and-through / segmental, unstable, needing segmental resection
- Relevance to transport
- The classic indication for bone transport - resection creates the segmental defect
- Status
- Normal immune and vascular status
- Implication
- Tolerates curative resection and reconstruction
- Status
- Compromised - local (Bl: scarring, radiation), systemic (Bs: diabetes, smoking, malnutrition), or both (Bls)
- Implication
- Optimise first; higher complication and nonunion risk
- Status
- Treatment morbidity would exceed that of the disease itself
- Implication
- Palliation / suppression rather than radical reconstruction
The clinical stage is the anatomic type plus the host (for example a 4B tibia). Stage 4 (diffuse/segmental) is the pattern whose radical debridement creates the segmental defect that bone transport reconstructs - but only a type A (or optimised B) host should be offered curative reconstruction, while a C host is managed by suppression or amputation rather than a year in a frame.
Clinical Presentation
Patient Assessment
- Mechanism of bone loss
- Infection history (critical for planning)
- Previous surgery and implants
- Comorbidities affecting healing
- Soft tissue envelope quality
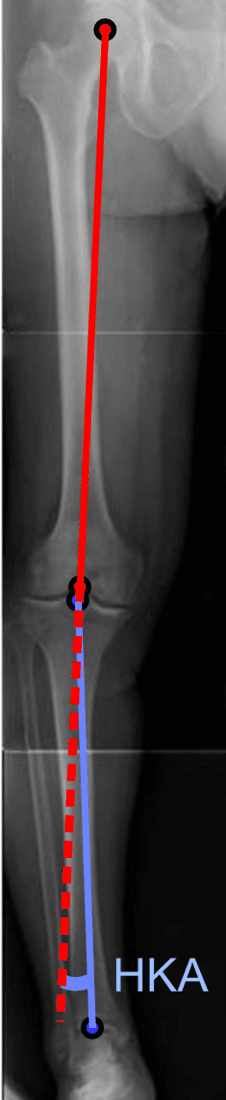
- Limb alignment
- Neurovascular status
- Signs of active infection
Preoperative Planning
- Full-length bone radiographs
- CT for defect measurement and bone quality
- MRI if infection suspected
- Size in centimeters
- Location (metaphyseal vs diaphyseal)
- Bone quality at proposed osteotomy sites
- Soft tissue condition
Investigations
Imaging
- Full-length views of affected bone
- Assess defect size and location
- Bone quality evaluation
- Accurate defect measurement
- Plan osteotomy site
- Assess sequestra in infection
- Soft tissue evaluation
- Infection extent
- Marrow involvement
Imaging Atlas
Infection Workup
For infected cases:
- ESR and CRP (baseline and monitoring)
- White cell count
- Intraoperative cultures (at least 5 samples)
- Histopathology
Management
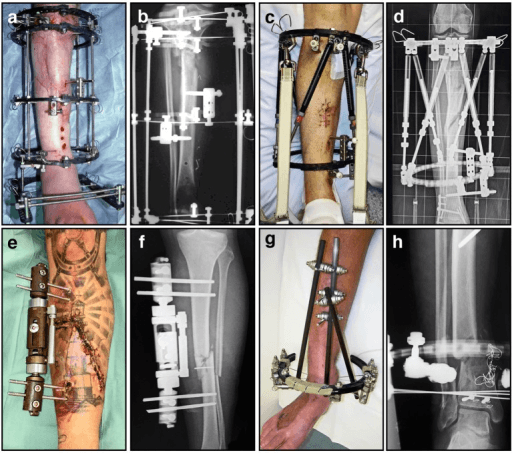
Bone Transport Technique
- Ilizarov or hexapod frame (TSF)
- Minimum 2 rings per segment
- Transport ring connected to segment to be moved
- Low-energy corticotomy
- Metaphyseal if possible
- Preserve periosteum and blood supply
- Same technique as for lengthening
- 5-7 days before beginning transport
- Allows initial callus formation
- 1mm/day in 4 divided doses
- Monitor regenerate weekly
- Adjust rate based on regenerate quality
- When transported segment reaches target
- Freshen bone ends
- Compress across site
- Bone graft if needed
- Continue frame until regenerate solid
- Approximately 1 month per cm of transport
- Frame removal when 3 cortices visible
This section covers the bone transport technique.
Surgical Management
Method Selection
Monofocal Transport
- Defects less than 6cm
- Single segment adequate
- Simpler technique preferred
- Single osteotomy at one end of bone
- Transport segment across defect
- Docking at opposite end
- Simpler construct
- Single regenerate to monitor
- Longer transport distance
- More soft tissue stretch
- Longer treatment time
This section covers monofocal transport.
Complications
Transport Complications
- Poor regenerate: Slow rate, bone graft if persistent
- Premature consolidation: Speed up rate or accordion
- Axial deviation: Adjust frame during transport
- Soft tissue tethering: May limit transport
Docking Site Complications
- Nonunion: 25-50% need bone grafting
- Malalignment: Correct before union
- Infection persistence: Further debridement
General Complications
- Pin site infection: Standard external fixator issue
- Joint contracture: Aggressive physiotherapy
- Refracture: Protect after frame removal (risk rises with defects over 8cm)
Choosing the Reconstruction Method
The key exam decision is not "how to do transport" but "which technique for this defect, this host, these soft tissues". The four mainstream options are compared below.
- Best defect size
- Any size, including over 8cm; tolerates active infection
- Strengths
- Like-for-like bone, no graft-volume limit, treats infection, restores length
- Limitations / pitfalls
- Long frame time, pin-site problems, docking-site nonunion, high overall complication rate
- Best defect size
- Roughly 4 to 12cm
- Strengths
- Technically simpler, shorter fixation, two predictable stages
- Limitations / pitfalls
- Limited by autograft volume, two operations, less suited to very large or actively infected defects
- Best defect size
- Large defects with good recipient vessels
- Strengths
- Living vascularised bone, faster union, hypertrophies under load, lower complication rate in pooled data
- Limitations / pitfalls
- Microsurgical expertise, donor-site morbidity, slender graft needs protection, stress fracture risk
- Best defect size
- Smaller infected defects (acute shortening 3 to 4cm)
- Strengths
- Compression at nonunion, can close soft-tissue gap without flap, avoids transport through infected zone
- Limitations / pitfalls
- Limited safe acute shortening, neurovascular kinking, later relengthening required
The Induced-Membrane (Masquelet) Technique
The induced-membrane technique is the principal alternative to transport for a segmental defect, and the examiner expects you to know its two stages and why the membrane matters.
- What is done
- Radical debridement, skeletal stabilisation (nail/plate/fixator), fill the defect with an antibiotic-loaded PMMA cement spacer, and achieve soft-tissue cover (flap if needed)
- Key point
- The spacer both delivers antibiotic AND induces a vascular membrane around itself
- What is done
- Carefully incise and PRESERVE the membrane, remove the spacer, fill the cavity with cancellous autograft (iliac crest or reamer-irrigator-aspirator), and close the membrane over the graft
- Key point
- Graft before the membrane loses bioactivity; do not strip the membrane
Why the induced membrane works: the foreign-body reaction to the cement creates a vascularised pseudosynovial membrane that secretes growth factors (VEGF, BMP-2, TGF-beta), prevents graft resorption, and provides a contained, well-vascularised bed; its bioactivity peaks at around one month, which is why grafting is timed to roughly 6 to 8 weeks.
The Masquelet technique is technically simpler than transport with a shorter time in fixation, but is limited by autograft volume (the reamer-irrigator-aspirator helps) and needs good soft-tissue cover; bone transport better tolerates very large defects and active infection. At stage 2, preserve the induced membrane (it is the biological reactor) and graft before it loses bioactivity at about 6 to 8 weeks.
Postoperative Care
Distraction and Monitoring Phase
- Start distraction after the 5 to 7 day latency; instruct the patient/carer on 0.25mm four-times-daily adjustments.
- Pin-site care: daily cleaning regimen; pin-site infection is expected and treated early with oral antibiotics, escalating only if deep.
- Weight-bearing: encouraged within tolerance to load the regenerate, which improves bone quality.
- Radiographs: regenerate reviewed approximately every 2 weeks; slow the rate for poor regenerate, speed up or perform an accordion manoeuvre for premature consolidation.
- Range of motion: aggressive physiotherapy for adjacent joints throughout to prevent equinus (tibia) and knee/hip contractures.
Consolidation and Frame Removal
- Continue the frame through consolidation (roughly 1 month per cm transported).
- Confirm union of regenerate and docking site before removal - 3 of 4 cortices visible on orthogonal views.
- After removal, protect the limb (cast/brace) to reduce refracture risk, especially for defects over 8cm.
Outcomes and Prognosis
Pooled data come from systematic reviews and case series rather than registries. Reported figures (verified in the Evidence Base) include:
- Union: achievable in the high 80s to mid 90s percent with appropriate docking-site management; nonunion rates are comparable between transport and free fibula.
- Infection eradication: transport markedly reduces deep infection in infected lesions (risk ratio 0.14 in meta-analysis).
- Docking-site grafting: required in 25 to 50% of cases - the principal predictable hurdle.
- Refracture: about 5% overall, rising roughly 3.7-fold for tibial defects over 8cm.
- Amputation: around 2.9%, including a voluntary amputation rate of about 1.6% reflecting treatment burden.
- External fixation index: roughly 1.5 months/cm with a frame alone, falling to as low as 0.4 months/cm when transport/lengthening is performed over a nail.
Functional outcomes (ASAMI) are good to excellent in most series, but treatment is long and demanding; patient selection and counselling are decisive prognostic factors.
Guidelines, Registries & Global Practice
Global Epidemiology
Segmental long-bone defects most often follow high-energy open tibial fractures (Gustilo IIIB/IIIC), infected nonunion/osteomyelitis, and tumour resection. Worldwide the tibia is the commonest site because of its subcutaneous position and tenuous blood supply. There is no dedicated international registry for bone transport; the evidence base is dominated by single-centre case series and a small number of systematic reviews, so reported figures vary widely with defect size, infection and host status.
Side-by-Side Guidance
- Position
- Distraction osteogenesis (transport) and induced-membrane (Masquelet) both endorsed; defect size, infection and soft tissues drive choice
- Emphasis
- Radical debridement and stable fixation before reconstruction; stage according to host
- Position
- Orthoplastic care in a specialist centre; definitive skeletal and soft-tissue reconstruction together
- Emphasis
- Single combined orthoplastic procedure; early flap cover before any reconstruction
- Position
- No single mandated technique; transport, induced membrane and vascularised fibula all accepted
- Emphasis
- Patient selection, infection control and shared decision-making
- Position
- Recognises transport, induced membrane and vascularised graft as complementary; matches method to defect length and biology
- Emphasis
- Multidisciplinary limb-reconstruction teams; salvage vs amputation discussion
The common thread across all bodies: control infection and achieve healthy soft-tissue cover first, then reconstruct bone with the method best matched to defect length, host biology and local expertise. None mandates a single technique.
Registry and Outcome Notes
No arthroplasty-style registry tracks bone transport. The best pooled outcome data come from systematic reviews (e.g. Papakostidis 2013, Paul 2023) rather than national registries, so quoted union, refracture and amputation rates derive from aggregated case series and carry meaningful heterogeneity.
High- vs Limited-Resource Practice Variation
- Typical practice
- Hexapod frames (TSF), motorised lengthening/transport nails, plate- or nail-assisted transport, free-flap orthoplastic cover, induced membrane with bone-graft substitutes/BMP
- Typical practice
- Ilizarov ring fixator remains the workhorse; documented use of locally fabricated/low-cost components; reliance on autograft; transport over a standard nail to cut frame time and clinic visits
The induced-membrane (Masquelet) technique is the principal global alternative to transport: a two-stage approach with a PMMA cement spacer to induce a vascular membrane, followed by autologous cancellous grafting (usually at 4 to 8 weeks). Transport better tolerates very large defects and active infection; induced membrane is technically simpler and avoids prolonged external fixation but is graft-volume limited. Vascularised free fibula is favoured for large defects with a good recipient vessel bed.
Controversies and Areas of Uncertainty
- Transport vs induced membrane vs free fibula: No high-quality randomised data establishes superiority. Systematic review evidence shows equivalent bony and functional outcomes between transport and free fibula, with free fibula achieving faster union and fewer complications but requiring microsurgery (Paul 2023). Choice remains expertise- and biology-driven.
- Prophylactic docking-site grafting: Whether to graft the docking site at the time of contact versus waiting to see if it unites spontaneously is unresolved. Acute grafting (as in nail-assisted series) may pre-empt the 25 to 50% nonunion rate but commits every patient to an extra procedure.
- Optimal distraction rate and rhythm: 1mm/day in 4 increments is conventional, but slower rates may be needed for poor regenerate and faster increments tolerated in children; the ideal rhythm for transport (as opposed to lengthening) is extrapolated rather than proven.
- Role of biologics (BMP, PRP, bone-graft substitutes): Used adjunctively at problem docking sites and to augment regenerate, but evidence is largely off-label and low-level; routine use is not established.
- Salvage vs amputation: For very large defects with severe soft-tissue and neurovascular injury, prolonged reconstruction may not outperform early amputation and prosthetic rehabilitation in function or cost - a shared decision, not a technical default.
MCQ Practice Points
A: 1mm/day delivered as 0.25mm four times daily, after a 5 to 7 day latency - identical to limb lengthening. Slowing the rate is the first response to poor regenerate.
A: The docking site (not the regenerate). Two often-sclerotic, avascular ends meet; expect to graft 25 to 50% of docking sites and plan for it.
A: An intact fibula tethers the tibia and blocks transport/compression; a fibular osteotomy allows the tibial segment to move and the docking site to compress.
A: It chiefly reduces the external fixation index/time (as low as 0.4 months/cm) and protects the regenerate during consolidation; it does not change regenerate biology.
A: Roughly 3 to 4cm. Beyond this, vascular and nerve kinking risk rises; debride to healthy bone first, then relengthen at a distant corticotomy.
A: Tibial defects over 8cm (about 3.7-fold higher). Protect the limb in a cast or brace after frame removal.
At a Glance Table
- Value / Principle
- 1mm/day
- Value / Principle
- 0.25mm four times daily
- Value / Principle
- 5 to 7 days
- Value / Principle
- Segmental defect over 4cm not amenable to grafting alone
- Value / Principle
- Roughly 1 month per cm transported
- Value / Principle
- Approximately 1.5 months/cm
- Value / Principle
- As low as 0.4 months/cm
- Value / Principle
- 25 to 50%
- Value / Principle
- 3 of 4 cortices of regenerate visible
DRIFTTransport Principles
Hook:Let the bone DRIFT across the defect!
DOCKDocking Site Management
Hook:DOCK the transported bone properly for union!
HALFBifocal vs Monofocal
Hook:Bifocal cuts the time in HALF!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man has a 6cm segmental tibial bone defect following debridement of infected nonunion. The soft tissues are healthy after flap coverage. How do you plan management?”
“A patient has completed tibial bone transport for a 5cm defect. The regenerate looks excellent, but at 4 months there is no union at the docking site. What is your management?”
“Describe the shortening-lengthening technique as an alternative to bone transport for infected tibial nonunion.”
Transport Parameters
- Rate: 1mm/day (same as lengthening)
- Latency: 5-7 days before transport
- Rhythm: 0.25mm QID
- Frame time: 1.5 months per cm typical
Method Selection
- Monofocal: Defects less than 6cm, simpler
- Bifocal: Defects greater than 6cm, faster
- Trifocal: Very large defects
- Over nail: Reduces external fixation time
Docking Site Management
- 25-50% require bone grafting
- Refresh sclerotic bone ends
- Autograft from iliac crest
- Compress and stabilize
Special Considerations - Tibia
- Fibular osteotomy allows transport
- Anteromedial surface accessible
- Soft tissue often compromised
- Consider induced membrane as alternative
Infected Nonunion Principles
- Debride all infected/necrotic bone first
- Transport through healthy bone only
- Alternative: Shortening-lengthening
- Monitor infection markers throughout
Complications
- Docking site nonunion: Most problematic
- Poor regenerate: Adjust rate
- Pin site infection: Standard management
- Joint contracture: Physiotherapy essential
Evidence Base
All primary clinical studies below have been verified against PubMed. Society guidance and core textbook principles are flagged as Guideline-level and do not carry a PMID.
Distraction Osteogenesis for Long Bone Defects: Systematic Review and Meta-analysis
- Ilizarov method significantly reduced deep infection in infected lesions (risk ratio 0.14, 95% CI 0.10 to 0.20)
- Overall refracture rate 5%, neurovascular complications 2.2%, amputation 2.9%
- Tibial defects over 8cm carried 3.7-fold higher refracture risk (odds ratio 3.7, 95% CI 1.1 to 12.5)
- Voluntary amputation rate 1.6% underlines the demand on patients and need for careful selection
Bone Transport in the Management of Fractures of the Tibia
- Mean resection 5.2cm in infected nonunions; mean bone and soft-tissue loss 8cm in IIIB fractures
- Union achieved in all cases except one; infection eradicated in all
- 10 of 21 limbs required bone grafting (predominantly at the docking site)
- Mean treatment duration 12 months
Ilizarov Fixator Combined with Intramedullary Nail for Tibial Nonunions with Bone Loss
- External fixation index averaged 0.4 months per cm (vs roughly 1.5 with frame alone)
- Mean time to union 4.6 months; mean external fixation time 4 months
- Primary docking-site iliac-crest grafting at the time of acute compression
- No refracture or malalignment; Paley bone score excellent in all 5 patients
Bone Transport vs Free Vascularised Fibula Grafting: Systematic Review and Meta-analysis
- Bony union and functional outcomes did not differ between the two techniques
- Free fibula reached union about 9.3 months sooner and reduced external-fixator time by 5.3 months
- Total complications were 68% higher in the bone transport group
- Nonunion rates did not differ between groups
Acute Shortening and Deformation with the Ilizarov/Taylor Spatial Frame for Infected Nonunion
- Acute shortening brings healthy bone ends into contact and compression at the nonunion
- Temporary deformation can close moderate soft-tissue defects without free tissue transfer
- Length and alignment restored later by distraction at a healthy corticotomy
- Best suited where soft-tissue loss exceeds bone loss
Double-level Fixator-assisted Nailing to Reduce Time in Frame
- Mean time in fixator 8.6 weeks vs 30.2 weeks for frame-only controls (p less than 0.001)
- External fixation index 17.7 days/cm vs 73.4 days/cm for controls (p less than 0.001)
- Equivalent length gain (3.9 vs 4.2cm) with no infections
- ASAMI bone and functional scores excellent or good in all segments
Masquelet Induced-Membrane Technique for Large Bone Defects
- Stage 1 PMMA (or calcium sulfate/polypropylene) spacer induces a bioactive foreign-body membrane
- Stage 2 grafting usually at 4 to 8 weeks; membrane retains bioactivity even beyond 8 weeks
- Avoids prolonged external fixation but depends on adequate graft volume and soft-tissue cover
- 3D-printed scaffolds emerging but lack large clinical series
Principles of the Ilizarov Method and Distraction Osteogenesis
- Tension-stress effect drives neo-osteogenesis when living tissue is distracted gradually
- Standard rate 1mm/day in 4 increments balances regenerate quality against premature consolidation
- Low-energy metaphyseal corticotomy preserves osteogenic blood supply
- Consolidation indexed at roughly 1 month per cm transported (3 cortices before frame removal)