Monosodium Urate | Negatively Birefringent | Needle-Shaped Crystals
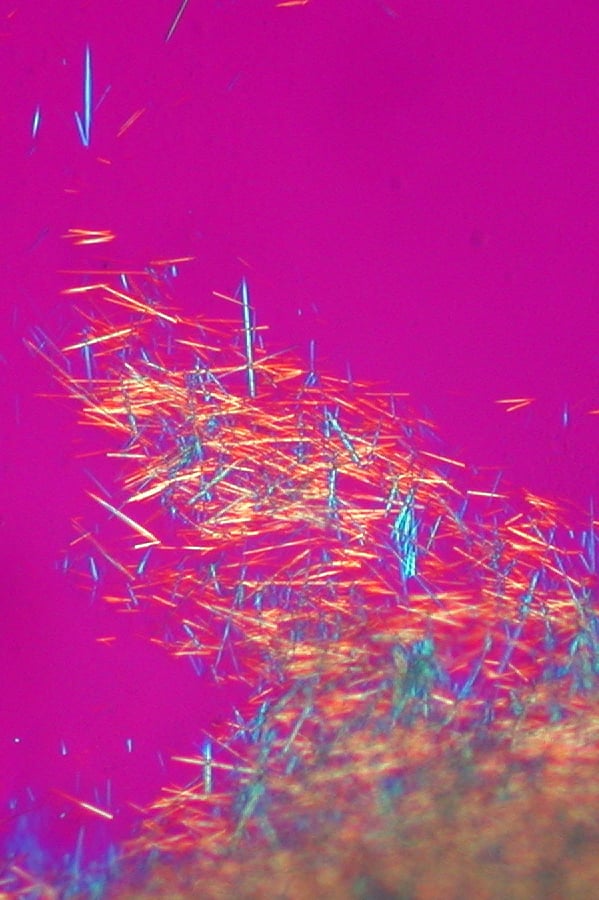
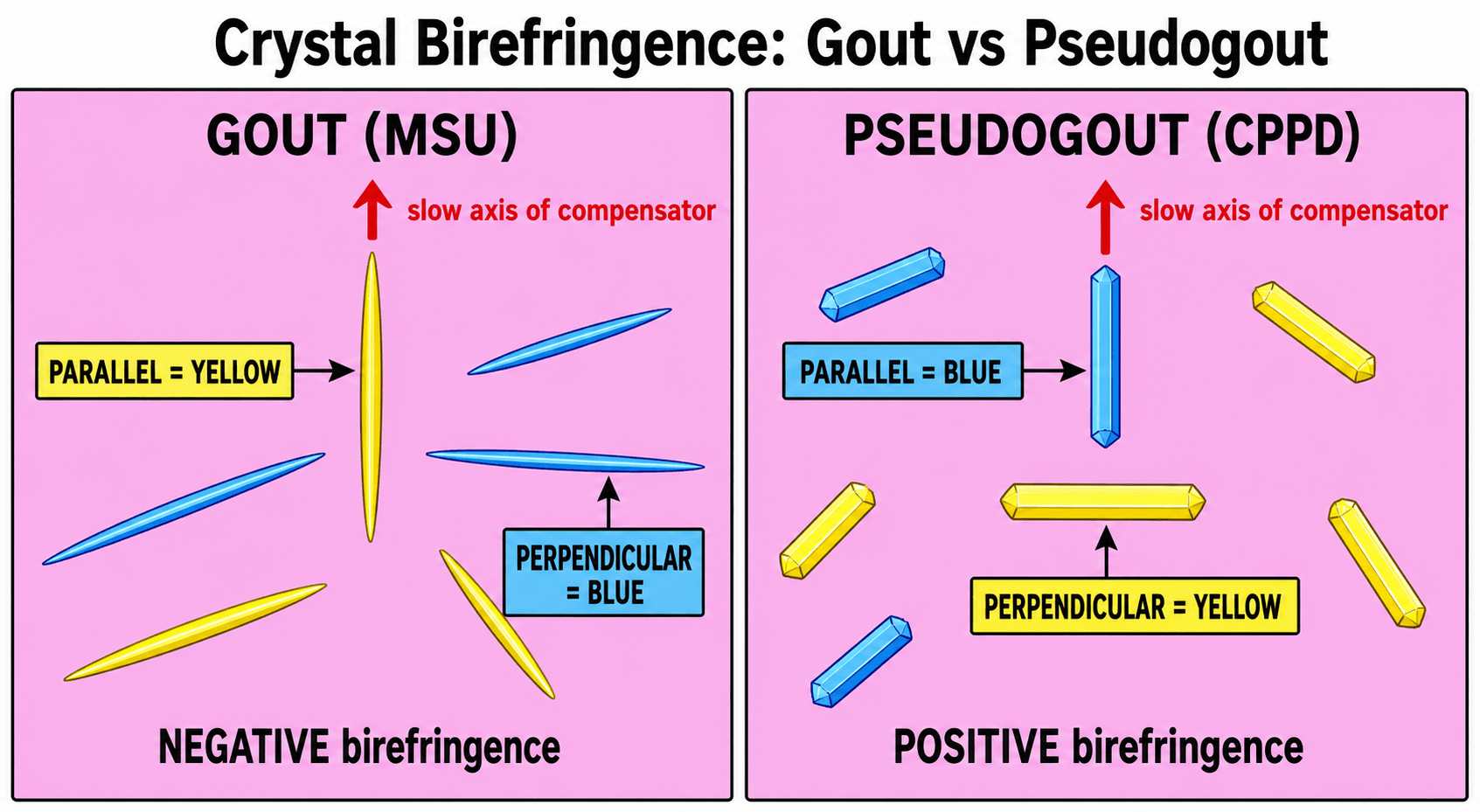
- MSU crystals are needle-shaped and negatively birefringent (yellow parallel to polarizer)
- Podagra (1st MTP involvement) is the classic presentation
- Joint aspiration is gold standard for diagnosis - even during acute attack
- Urate-lowering therapy target is serum urate less than 6 mg/dL (360 micromol/L)
- Surgical indications: mechanical symptoms, ulceration, infection, nerve compression
- “Negatively birefringent = yellow when parallel to polarizer axis
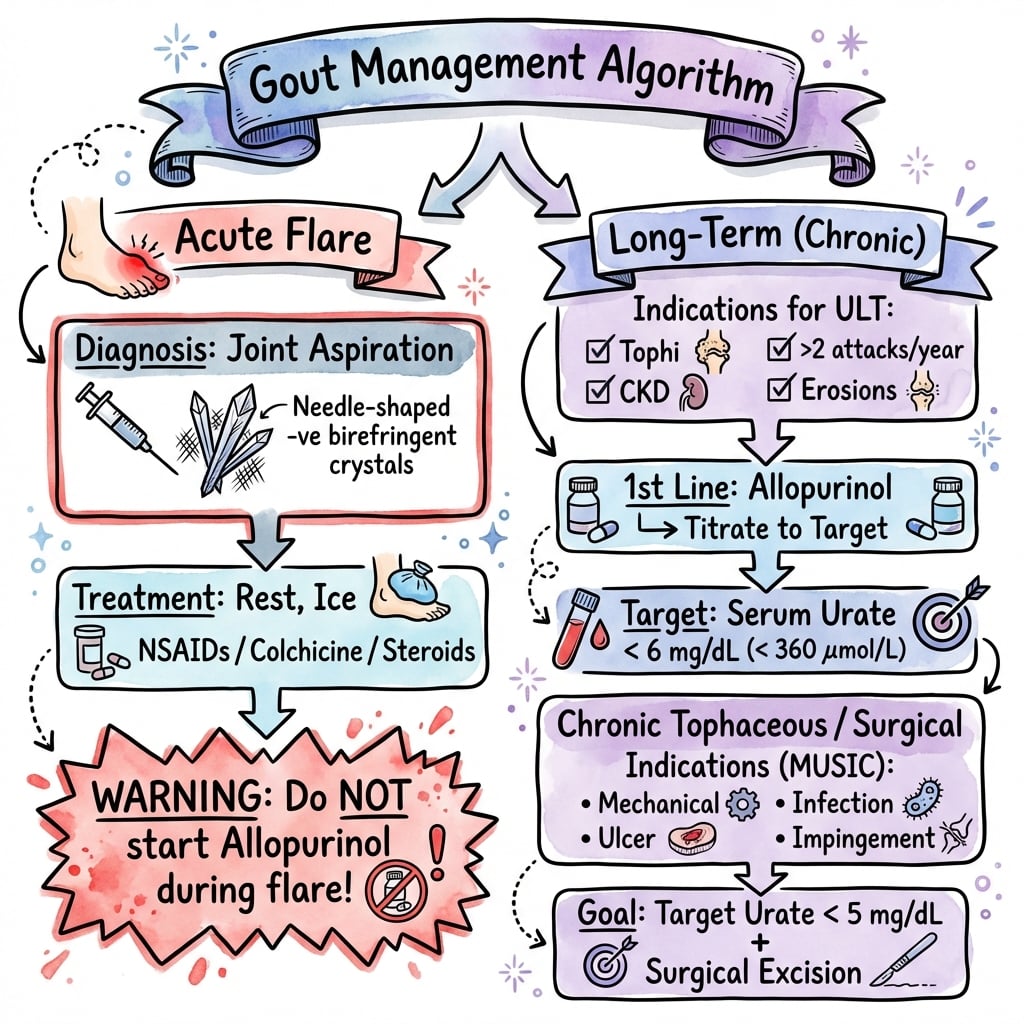
- “Acute attack: do NOT start allopurinol - may prolong attack
- “Dual-energy CT can identify urate deposits non-invasively
- “Tophi surgery: avoid primary closure over large defects
MSU crystals: Needle-shaped, negatively birefringent (yellow parallel, blue perpendicular). CPPD crystals: Rhomboid, positively birefringent (blue parallel, yellow perpendicular). This distinction is fundamental to diagnosis.
Do NOT start urate-lowering therapy during acute attack - may prolong symptoms. Treat with NSAIDs, colchicine (within 12 hours), or corticosteroids. Continue existing ULT if already established.
Orthopaedic involvement for: mechanical symptoms from tophi, skin ulceration over tophi, secondary infection, nerve compression (carpal tunnel), joint destruction requiring arthroplasty.
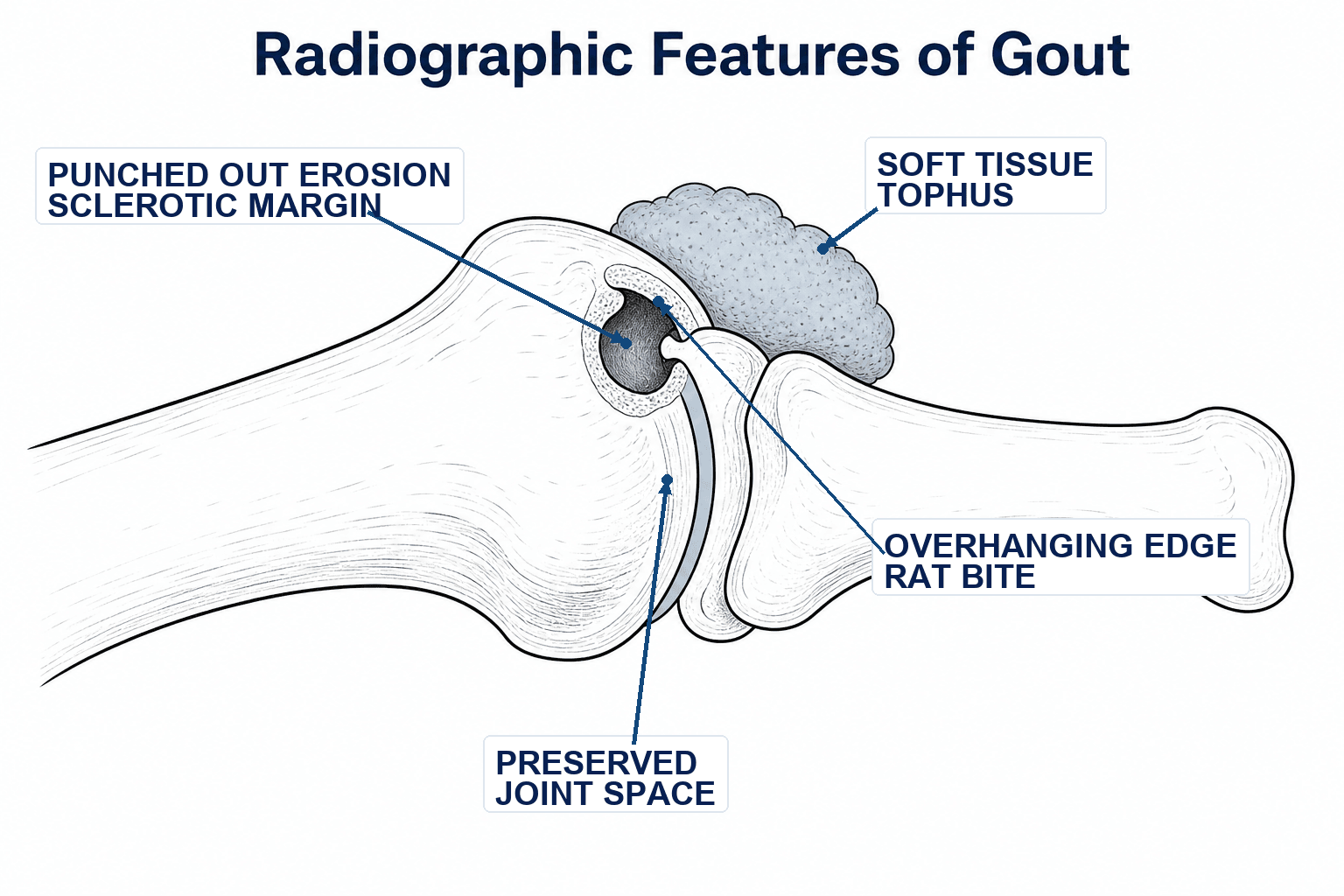
Radiographic signs: Punched-out erosions with overhanging edges ("rat bite"), preserved joint space until late, soft tissue tophi with calcification. Dual-energy CT shows urate deposits as green.
- Gout (MSU)
- Needle-shaped
- Pseudogout (CPPD)
- Rhomboid/rod-shaped
- Gout (MSU)
- Negative (yellow parallel)
- Pseudogout (CPPD)
- Positive (blue parallel)
- Gout (MSU)
- 1st MTP (podagra)
- Pseudogout (CPPD)
- Knee, wrist
- Gout (MSU)
- Punched-out erosions
- Pseudogout (CPPD)
- Chondrocalcinosis
- Gout (MSU)
- Purine-rich diet, alcohol, obesity
- Pseudogout (CPPD)
- Age, OA, metabolic disease
- Gout (MSU)
- Yes - allopurinol, febuxostat
- Pseudogout (CPPD)
- No specific therapy
NEEDLEGout Crystal Features
Hook:NEEDLE crystals cause NEEDLE-sharp pain in gout!
Overview and Epidemiology
Gout is the most common inflammatory arthritis in adults, caused by deposition of monosodium urate (MSU) crystals in joints and soft tissues. It results from prolonged hyperuricemia leading to crystal formation when serum urate exceeds its saturation point of 6.8 mg/dL (404 micromol/L).
- Prevalence: 1-4% of adults in developed countries
- Male to female ratio: 4:1 (equalizes after menopause)
- Peak incidence: Males 40-50 years, females post-menopause
- Increasing prevalence due to obesity, metabolic syndrome, aging population
- Dietary: Purine-rich foods (red meat, seafood), alcohol (especially beer), fructose-sweetened beverages
- Medications: Thiazide diuretics, low-dose aspirin, cyclosporine
- Comorbidities: Chronic kidney disease, metabolic syndrome, hypertension, obesity
- Genetic: Variants in urate transporters (URAT1, GLUT9)
MSU crystals trigger the innate immune system via the NLRP3 inflammasome, leading to IL-1beta release. This explains why IL-1 inhibitors (anakinra, canakinumab) are effective in refractory cases.
Pathophysiology
Understanding the pathophysiology of gout is essential for both diagnosis and management. The disease results from a complex interplay of uric acid metabolism, crystal formation, and inflammatory responses.
Uric Acid Metabolism
- Uric acid is the end product of purine metabolism in humans
- Purines derived from dietary intake (exogenous) and cellular turnover (endogenous)
- Key enzyme: Xanthine oxidase converts hypoxanthine to xanthine to uric acid
- Humans lack uricase enzyme (present in most mammals) - cannot break down uric acid further
- 70% renal excretion via complex tubular handling
- 30% gastrointestinal excretion
- Key transporters: URAT1 (reabsorption), ABCG2 (secretion), GLUT9
Crystal Formation
- Monosodium urate (MSU) saturates at 6.8 mg/dL (404 micromol/L)
- Below this level, crystals gradually dissolve
- Above this level, crystals can precipitate in tissues
- Lower temperature (explains predilection for peripheral joints)
- Lower pH (trauma, exercise-induced acidosis)
- Presence of nucleating agents
- Connective tissue matrix components
Inflammatory Response
NLRP3 Inflammasome activation:
- MSU crystals are phagocytosed by macrophages
- Crystals destabilize lysosomal membranes
- Cathepsin B released into cytoplasm
- NLRP3 inflammasome assembly triggered
- Caspase-1 activation
- Pro-IL-1beta cleaved to active IL-1beta
- Massive inflammatory cascade initiated
The NLRP3 inflammasome pathway explains why IL-1 inhibitors (anakinra, canakinumab) are effective in refractory gout. This is increasingly tested in fellowship exams as it bridges basic science with clinical application.
Resolution:
- Acute attacks are self-limiting (7-14 days)
- Aggregated neutrophil extracellular traps (NETs) help resolve inflammation
- Coating of crystals by proteins reduces immunogenicity
- Anti-inflammatory macrophage phenotype emerges
Tophus Pathology and Composition
The tophus is the pathological hallmark of chronic gout and the structure the surgeon excises - understanding what it actually is explains both its radiographic appearance and the principle that optimised urate-lowering therapy can dissolve it medically. A tophus is not a simple lump of crystal but an organised, chronic foreign-body granulomatous response to deposited monosodium urate.
Microscopic Zones
A mature tophus has three concentric zones:
- Composition
- Densely packed needle-shaped MSU crystals in a protein and lipid matrix
- Significance
- The chalky white material seen at surgery; dissolves when serum urate is held below saturation
- Composition
- Macrophages and multinucleated foreign-body giant cells directly surrounding the crystals, with other inflammatory cells
- Significance
- The active inflammatory interface that drives adjacent bone and cartilage destruction
- Composition
- Fibroblasts, connective tissue and new vessels encapsulating the deposit
- Significance
- Walls the tophus off; the poorly vascularised overlying skin partly explains delayed wound healing after excision
Because the crystals are in equilibrium with the serum urate, tophi are reversible: sustained urate-lowering therapy below the saturation point (and below 5 mg/dL when tophi are present) lets them slowly dissolve. This is why many surgeons now favour debulking plus optimised medical therapy over aggressive wide excision, which risks an unclosable defect.
The punched-out erosions with overhanging edges arise at the tophus-bone interface: the cellular corona contains osteoclast-like cells and an inflammatory milieu that drive focal bone resorption, while the encapsulated crystal mass displaces the cortex - producing the characteristic "overhanging edge" of bone draped over the deposit, with the joint space preserved until late.
Clinical Presentation
Acute Gouty Arthritis
- Rapid onset over 6-12 hours, often waking patient from sleep
- Exquisitely painful - unable to tolerate bedsheet contact
- Monoarticular in 85-90% of initial attacks
- Podagra (1st MTP) is the classic location - 50% of first attacks
- Signs of inflammation: Erythema, warmth, swelling mimicking cellulitis
- First metatarsophalangeal joint (podagra) - 50%
- Ankle and midfoot - 25%
- Knee - 15%
- Wrist, fingers, elbow - 10%
Chronic Tophaceous Gout
Features:
- Tophi: Chalky deposits of MSU crystals in soft tissues
- Common locations: Fingers, olecranon bursa, Achilles tendon, ears
- Joint destruction: Erosive arthropathy with preserved joint space initially
- Tendon involvement: Can cause rupture (Achilles, patellar, extensor tendons)
Physical Examination
- Swelling and erythema over affected joint
- Tophi visible as subcutaneous nodules (white-yellow through skin)
- Skin ulceration over tophi in advanced cases
- Extreme tenderness - even light touch is painful
- Warmth over affected joint
- Tophi are firm, irregular nodules
Investigations
Laboratory Studies
Synovial fluid analysis (Gold Standard):
- MSU crystal identification under polarized microscopy
- Needle-shaped, negatively birefringent crystals
- WBC count: 10,000-70,000/microL (predominantly neutrophils)
- May be normal during acute attack (paradoxical decrease)
- Elevated greater than 6.8 mg/dL (360 micromol/L) supports diagnosis
- Target for ULT: less than 6 mg/dL (360 micromol/L)
- Renal function (CKD common comorbidity)
- Lipid profile and glucose (metabolic syndrome)
- CBC (elevated WBC during acute attack)
Imaging
Plain Radiographs:
- Early: Soft tissue swelling, normal bone
- Established: Punched-out erosions with overhanging edges ("rat bite" or "mouse ear")
- Preserved joint space (unlike OA)
- Soft tissue tophi may calcify
- Double contour sign: Hyperechoic line on hyaline cartilage surface
- Aggregates and tophi visible
- Useful for guided aspiration
- Color-codes urate deposits (typically green)
- Pooled sensitivity approximately 0.87 and specificity 0.84 (Ogdie meta-analysis)
- Lower sensitivity in early/acute gout and small deposits (false negatives in disease under 6 weeks)
- Useful when aspiration not possible; can detect occult tophi
- Beware artefacts (nail-bed, skin, beam hardening) mimicking urate
Differential Diagnosis
The single most important mimic of acute gout is septic arthritis - the two can coexist, and a hot, swollen joint must be aspirated to exclude infection before attributing it to crystals.
- Gout (MSU)
- 1st MTP, midfoot, knee
- Pseudogout (CPPD)
- Knee, wrist, MCP
- Septic Arthritis
- Knee, hip; any joint
- Reactive/Psoriatic
- Knee, ankle, sacroiliac
- Gout (MSU)
- Hours, often nocturnal
- Pseudogout (CPPD)
- Subacute over days
- Septic Arthritis
- Hours to days, systemically unwell
- Reactive/Psoriatic
- Days to weeks
- Gout (MSU)
- 10,000-70,000/microL
- Pseudogout (CPPD)
- 10,000-50,000/microL
- Septic Arthritis
- Often greater than 50,000, up to 100,000+
- Reactive/Psoriatic
- 5,000-50,000/microL
- Gout (MSU)
- Needle, negatively birefringent
- Pseudogout (CPPD)
- Rhomboid, positively birefringent
- Septic Arthritis
- None
- Reactive/Psoriatic
- None
- Gout (MSU)
- Negative
- Pseudogout (CPPD)
- Negative
- Septic Arthritis
- May be positive (definitive)
- Reactive/Psoriatic
- Negative
- Gout (MSU)
- Crystals + podagra
- Pseudogout (CPPD)
- Chondrocalcinosis on X-ray
- Septic Arthritis
- Fever, raised CRP, positive culture
- Reactive/Psoriatic
- Enthesitis, skin/eye/GU features
Crystals and sepsis can occur in the same joint. If synovial WBC is very high, the patient is febrile, or CRP is markedly raised, treat as septic arthritis until cultures return - send fluid for urgent Gram stain and culture, not just crystal analysis.
Management
Acute Attack Management
Starting allopurinol or febuxostat during an acute gout flare can prolong the attack by mobilizing urate crystals. Treat the acute attack first, then initiate ULT 2-4 weeks after resolution. However, continue ULT if already established.
- NSAIDs: Indomethacin 50mg TDS, naproxen 500mg BD - continue until attack resolves
- Colchicine: Most effective within 12 hours of onset. Loading dose 1mg, then 0.5mg 1 hour later. Low-dose regimen preferred.
- Corticosteroids: Prednisolone 30-40mg daily for 5-7 days, or intra-articular injection
- IL-1 inhibitors (anakinra) for patients with contraindications to all above
- Joint aspiration alone provides significant relief
Urate-Lowering Therapy (ULT)
- Recurrent acute attacks (2 or more per year)
- Presence of tophi
- Radiographic changes
- Chronic kidney disease stage 2 or greater
- Urolithiasis
- Allopurinol: First-line xanthine oxidase inhibitor. Start low (50-100mg, lower in CKD), titrate to target. Consider HLA-B*58:01 testing before starting in high-risk ethnicities (Han Chinese, Thai, Korean with CKD) to reduce severe cutaneous adverse reactions (SCAR/SJS-TEN).
- Febuxostat: Alternative if allopurinol intolerant or target not reached. More potent urate lowering; cardiovascular safety debated (see Controversies).
- Probenecid / benzbromarone (uricosurics): Require adequate renal function and urine output; avoid with urolithiasis. Useful for under-excretors when xanthine oxidase inhibitors fail.
- Pegloticase (recombinant uricase): For severe refractory tophaceous gout; rapidly dissolves tophi but immunogenic.
- Serum urate less than 6 mg/dL (360 micromol/L)
- Less than 5 mg/dL if tophi present for faster dissolution
COINSAcute Gout Treatment
Hook:Spend your COINS wisely on acute gout treatment!
Colchicine: Mechanism, Toxicity and Drug Interactions
Colchicine appears throughout gout management - acute flares, prophylaxis when starting urate-lowering therapy, and perioperative cover - yet how it works and why it is dangerous in overdose are commonly examined.
Mechanism of Action
Colchicine is an anti-mitotic alkaloid that binds tubulin and prevents microtubule polymerisation. In gout this disrupts neutrophil function - chemotaxis, adhesion and motility - and impairs assembly and activation of the NLRP3 inflammasome, reducing IL-1beta-driven inflammation. It is anti-inflammatory only: it is not an analgesic and not urate-lowering, so it treats the crystal-induced inflammatory response but does nothing to the serum urate.
Toxicity
- Effect
- Diarrhoea, nausea, vomiting, abdominal pain
- Note
- Dose-related and the earliest sign of toxicity - the reason low-dose regimens are now standard
- Effect
- Bone-marrow suppression (neutropenia, thrombocytopenia, pancytopenia)
- Note
- A feature of overdose or accumulation in renal or hepatic impairment
- Effect
- Myopathy and axonal neuropathy
- Note
- Especially with chronic use in renal impairment or combined with statins or fibrates
- Effect
- Multi-organ failure; narrow therapeutic index with no effective antidote
- Note
- Acute overdose can be fatal - colchicine must never be aggressively re-dosed to chase pain
Drug Interactions
Colchicine is metabolised by CYP3A4 and is a substrate of the P-glycoprotein efflux transporter. Co-administration with strong CYP3A4 or P-glycoprotein inhibitors - clarithromycin and other macrolides, azole antifungals, ciclosporin, verapamil and diltiazem - raises colchicine levels and can precipitate life-threatening toxicity. The dose must be reduced, or colchicine avoided, in significant renal or hepatic impairment and when these interacting drugs are unavoidable.
Diarrhoea is the warning sign and usually precedes serious toxicity. Reduce the dose in renal or hepatic impairment, halve or avoid it with CYP3A4/P-glycoprotein inhibitors (for example clarithromycin, ciclosporin, verapamil), and never escalate the dose to chase pain - there is no effective antidote for colchicine overdose.
Surgical Management
Indications for Surgery
- Mechanical symptoms: Large tophi limiting joint motion or tendon function
- Skin ulceration: Over tophi with risk of secondary infection
- Secondary infection: Debridement of infected tophi
- Nerve compression: Carpal tunnel, ulnar neuropathy from tophi
- Joint destruction: Arthroplasty for end-stage arthropathy
- Tendon rupture: Repair or reconstruction
Surgical Principles
Tophus Excision
- Optimize medical management (ULT established)
- Assess skin viability and plan closure
- Consider staged procedures for large tophi
- Incision planned to allow adequate exposure and closure
- Identify and protect neurovascular structures
- Debulk tophaceous material - chalky white deposits
- Curette affected bone if involved
- Assess tendon integrity
- Irrigate thoroughly
- Primary closure if possible
- Negative pressure wound therapy for large defects
- Skin grafting or flap coverage may be required
- Avoid tension on skin closure
- Continue ULT to prevent recurrence
- Wound care and monitoring for healing
- Physiotherapy for ROM
This completes the tophus excision approach.
MUSICSurgical Indications for Tophi
Hook:When tophi cause problems, it's time to make MUSIC with surgery!
Complications
Disease Complications
- Chronic erosive arthropathy: Joint destruction, subluxation
- Tendon rupture: Achilles, patellar, extensor tendons
- Carpal tunnel syndrome: From tophaceous deposits
- Renal complications: Uric acid stones, urate nephropathy
- Cardiovascular disease: Independent risk factor
Surgical Complications
- Wound healing problems: Skin necrosis, delayed healing over tophi
- Infection: Risk increased with ulcerated tophi
- Recurrence: If ULT not optimized
- Tendon injury: During tophus excision
Guidelines, Registries & Global Practice
Global Epidemiology
- Prevalence: ranges from under 1% to 6.8% of adults depending on population (Dehlin et al., Nat Rev Rheumatol 2020). Highest in Taiwanese aboriginal, Maori and Pacific Island populations (often greater than 6-10%), where reduced renal urate excretion and genetic urate-transporter variants combine with diet.
- Incidence: 0.58-2.89 per 1000 person-years; rising worldwide with obesity, ageing and metabolic syndrome.
- Sex/age: male predominance roughly 3-4:1, narrowing after menopause; peaks in men aged 40-60.
- Care gap: only one-third to one-half of patients ever receive urate-lowering therapy, and fewer than half adhere - the dominant problem in gout is implementation, not drug efficacy.
Side-by-side Guideline Comparison
- ACR 2020 (US)
- Allopurinol (incl. CKD)
- EULAR 2016 (Europe)
- Allopurinol; adjust dose to renal function
- BSR 2017 (UK)
- Allopurinol first-line
- ACR 2020 (US)
- Below 6 mg/dL (360 micromol/L), treat-to-target
- EULAR 2016 (Europe)
- Below 6 mg/dL; below 5 mg/dL (300) in severe/tophaceous
- BSR 2017 (UK)
- Below 5 mg/dL initially, then below 6 long-term
- ACR 2020 (US)
- May start during a flare (with prophylaxis)
- EULAR 2016 (Europe)
- Start after flare settles, plus prophylaxis
- BSR 2017 (UK)
- Once flare settled
- ACR 2020 (US)
- At least 3-6 months
- EULAR 2016 (Europe)
- At least 6 months
- BSR 2017 (UK)
- Up to 6 months
- ACR 2020 (US)
- Reserve for allopurinol failure (CV caution)
- EULAR 2016 (Europe)
- Second-line; caution if CV disease
- BSR 2017 (UK)
- Second-line if allopurinol intolerant
- ACR 2020 (US)
- Conditional in high-risk groups (e.g. Han Chinese, Thai, Korean CKD)
- EULAR 2016 (Europe)
- Consider in at-risk ethnicities
- BSR 2017 (UK)
- Consider in Han Chinese/Thai/Korean
Registry & Surgical Outcome Notes
- There is no dedicated international gout registry equivalent to arthroplasty joint registries, but national arthroplasty registries (NJR UK, AJRR US, AOANJRR Australia, SHAR Sweden) capture gout as a comorbidity. Crystal arthropathy is associated with modestly higher periprosthetic joint infection and wound-complication rates in some series, reinforcing the value of preoperative urate control.
- Hand-surgery series of tophaceous excision report good functional gain but real risks of delayed wound healing and recurrence if ULT is not optimised.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: ready access to polarised microscopy, ultrasound and DECT; HLA-B*58:01 genotyping where indicated; biologic IL-1 inhibitors (anakinra, canakinumab) for refractory disease.
- Limited-resource settings: diagnosis often clinical or via serum urate; polarised microscopy and DECT may be unavailable. Allopurinol and colchicine are inexpensive and on the WHO model essential-medicines landscape, so treat-to-target ULT remains achievable even where advanced imaging is not. Counterfeit colchicine and lack of monitoring are practical hazards.
- Across all settings, cardiovascular and renal risk screening is integral given the strong, consistent association of gout with CKD and cardiovascular disease.
Controversies & Areas of Uncertainty
- Febuxostat cardiovascular safety: CARES (29527974) showed higher all-cause and CV mortality with febuxostat versus allopurinol in patients with established CV disease, prompting an FDA boxed warning. The later EMA-mandated FAST trial (33181081) found febuxostat non-inferior with no excess mortality. The discrepancy (high CARES drop-out and on-treatment vs intention-to-treat handling) leaves the true CV risk unresolved; allopurinol remains the pragmatic first-line.
- Asymptomatic hyperuricaemia: routine urate-lowering for asymptomatic hyperuricaemia is not recommended by ACR or EULAR; whether high-risk subgroups (CKD, CV disease) benefit remains debated.
- Start ULT during a flare? ACR 2020 permits initiating allopurinol during an acute flare (with prophylaxis) on the basis it does not prolong the attack; traditional teaching and many other guidelines still defer ULT until the flare settles. Either way, never stop established ULT during a flare.
- Surgery for tophi: timing and technique are not standardised. Wide excision risks unclosable defects; many now favour debulking with optimised ULT to let residual deposits dissolve medically rather than aggressive resection.
- Diet vs drugs: dietary modification lowers urate only modestly (roughly 1 mg/dL); it supports but does not replace ULT, and over-emphasis can stigmatise patients and delay effective treatment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old obese man presents with sudden onset severe pain and swelling of his right first MTP joint. He woke at 3am unable to tolerate the bedsheet touching his foot. He drinks beer regularly. Examination shows an exquisitely tender, erythematous, swollen 1st MTP joint.”
“A 65-year-old man with a 15-year history of gout presents with a large tophus over his left olecranon causing skin breakdown. He has limited elbow flexion. Serum urate is 9.2 mg/dL despite allopurinol 300mg daily.”
“You are shown a polarized microscopy image of synovial fluid showing needle-shaped crystals that appear yellow when aligned parallel to the polarizer. What is your diagnosis?”
Crystal Identification
- MSU: Needle-shaped, negatively birefringent (YELLOW parallel)
- CPPD: Rhomboid, positively birefringent (BLUE parallel)
- Mnemonic: 'Yellow Parallel Gout' vs 'Blue Parallel Pseudogout'
Classic Presentation
- Podagra: 1st MTP involvement (50% of first attacks)
- Sudden onset, often nocturnal (3-4am)
- Exquisitely tender - cannot tolerate bedsheet
Imaging Signs
- Punched-out erosions with overhanging edges
- Preserved joint space until late
- Soft tissue tophi may calcify
- DECT shows urate as green
Acute Treatment
- NSAIDs: Indomethacin 50mg TDS or Naproxen 500mg BD
- Colchicine: Low-dose regimen (1mg then 0.5mg)
- Steroids: If NSAIDs/colchicine contraindicated
- DO NOT start allopurinol during acute attack
ULT Targets
- Serum urate less than 6 mg/dL (360 micromol/L)
- Less than 5 mg/dL if tophi present
- Start 2-4 weeks after acute attack resolution
Surgical Indications (MUSIC)
- Mechanical symptoms from tophi
- Ulceration of overlying skin
- Secondary infection
- Impingement on nerves
- Cosmetic concerns
Evidence Base
AGREE Trial - Low-dose vs High-dose Colchicine
- 50% or greater pain reduction at 24h: 37.8% low-dose vs 32.7% high-dose vs 15.5% placebo
- Diarrhoea in 77% of high-dose vs 23% of low-dose patients
- Most effective when started early (within roughly 12-24 hours of flare onset)
CARES Trial - Febuxostat vs Allopurinol CV Safety
- Primary MACE endpoint non-inferior (HR 1.03, upper 98.5% CI 1.23)
- All-cause death HR 1.22 (95% CI 1.01-1.47); CV death HR 1.34 (95% CI 1.03-1.73)
- About 45% of participants discontinued follow-up, a major limitation
Imaging Modalities for Gout Classification (Meta-analysis)
- DECT pooled sensitivity 0.87 (95% CI 0.79-0.93), specificity 0.84 (95% CI 0.75-0.90)
- Ultrasound double contour sign sensitivity 0.83, specificity 0.76
- Most evidence derived from longstanding established disease (mean duration over 7 years) - sensitivity is lower in early gout
Nurse-led Treat-to-Target Care for Gout (RCT)
- Urate target achieved: 95% nurse-led vs 30% usual care (RR 3.18)
- All secondary outcomes (flares, tophi, quality of life) favoured nurse-led care at 2 years
- Education and shared decision-making drove high ULT uptake and adherence
FAST Trial - Long-term CV Safety of Febuxostat
- Primary CV endpoint HR 0.85 (95% CI 0.70-1.03), non-inferior to allopurinol
- No increase in all-cause death (febuxostat 7.2% vs allopurinol 8.6%)
- Open-label design and high discontinuation are limitations, but lower drop-out than CARES
Global Epidemiology of Gout
- Prevalence under 1% to 6.8%; higher in men, with age, and in some ethnic groups (e.g. Taiwanese aboriginal, Maori, Pacific peoples)
- Only one-third to one-half of patients receive ULT; fewer than half adhere
- Established links to CKD and CV disease, plus newer associations (AF, OSA, VTE)
2020 ACR Guideline for the Management of Gout
- Allopurinol preferred first-line over febuxostat (cost and CV safety)
- Start ULT low (allopurinol 100 mg/day or less; lower in CKD) and titrate to target
- Treat-to-target serum urate below 6 mg/dL with serial monitoring