Center of Rotation of Angulation | Mechanical Axis Deviation | Osteotomy Planning
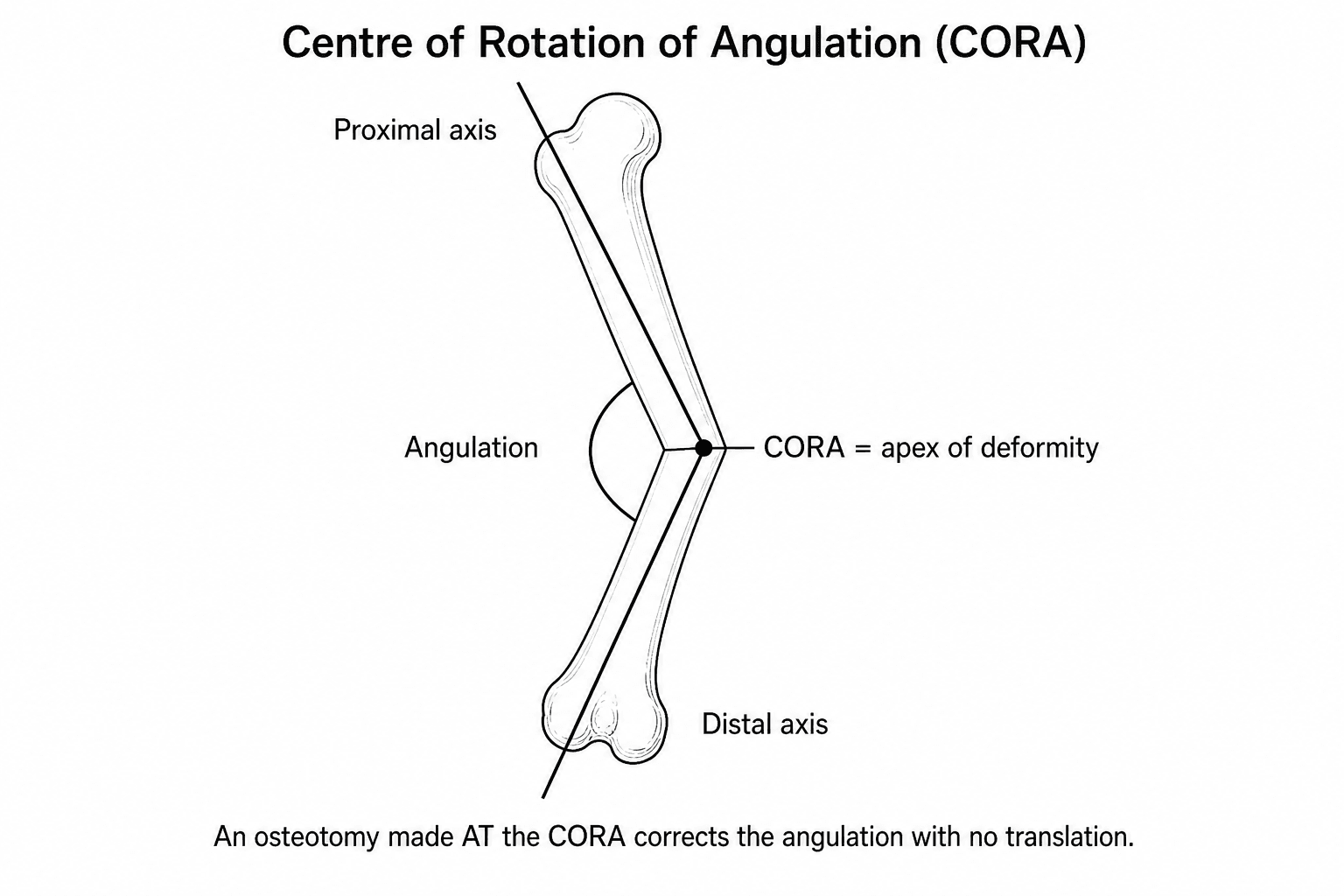
- CORA = intersection of proximal and distal anatomic/mechanical axes
- MAD = distance from mechanical axis to center of knee (normal 0-10mm medial)
- Osteotomy at CORA corrects deformity without translation
- LDFA and MPTA both normally 87 degrees
- Joint line obliquity must be assessed and corrected if abnormal
- “Proximal tibial osteotomy corrects up to 15 degrees safely
- “Distal femoral osteotomy for valgus greater than 12-15 degrees
- “Medial opening wedge HTO changes tibial slope posteriorly
- “CORA method allows precise osteotomy planning
CORA is where the proximal and distal axes intersect. This is the apex of the deformity. An osteotomy at CORA corrects angulation without creating translation. Away from CORA, you get angulation AND translation.
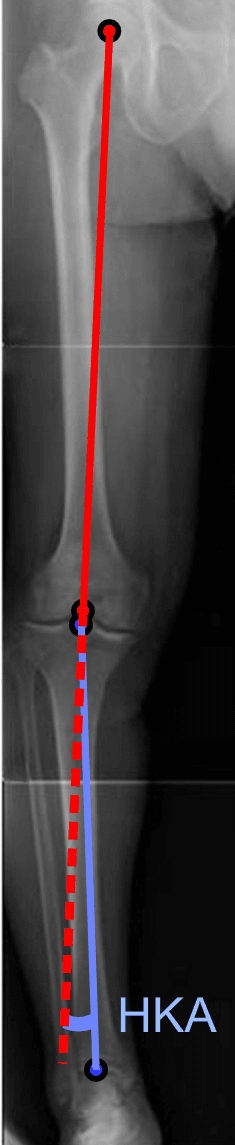
Mechanical axis runs from hip center to ankle center. Should pass through or just medial (0-10mm) to knee center. MAD measures deviation from this ideal. Positive = lateral; negative = medial.
LDFA (lateral distal femoral angle) = 87° ± 3°. MPTA (medial proximal tibial angle) = 87° ± 3°. JLCA (joint line congruence angle) = 0-2°. Deviations localize the deformity to femur, tibia, or joint.
Tibial osteotomy for tibial deformity (MPTA abnormal). Femoral osteotomy for femoral deformity (LDFA abnormal). Choose level to correct CORA. May need combined osteotomies for biplanar or oblique JLCA.
Overview and Epidemiology
Deformity analysis is the systematic evaluation of limb alignment to identify the location and magnitude of angular and translational deformities. The CORA (Center of Rotation of Angulation) method, developed by Dror Paley, provides a mathematical approach to osteotomy planning.
- Angular deformity correction
- Limb length discrepancy with deformity
- Malunion correction
- Developmental deformity
- Post-traumatic reconstruction
- Accurate analysis prevents secondary deformities from osteotomy
- Guides osteotomy level selection
- Predicts outcomes of correction
- Essential for examination success
The CORA method revolutionized deformity correction by providing a mathematical basis for osteotomy planning. The key insight: an osteotomy at CORA produces pure angular correction without translation, while an osteotomy away from CORA creates both angulation and translation.
Pathophysiology
Understanding the geometry of deformity analysis is fundamental to correct application.
Mechanical Axis
- Line from center of femoral head to center of ankle (talus)
- Represents weight-bearing axis of the limb
- Normally passes through or just medial to center of knee
- Distance from mechanical axis to center of knee
- Positive = axis lateral to knee (valgus)
- Negative = axis medial to knee (varus)
- Normal: 0 to 10mm medial to knee center
Anatomic Axis
- Line through the center of the bone diaphysis
- Femoral anatomic axis is not collinear with mechanical axis
- Tibial anatomic axis approximately equals mechanical axis
- Approximately 6 degrees
- Femoral anatomic axis is lateral to mechanical axis
CORA Determination
- Draw proximal anatomic or mechanical axis (line along proximal segment)
- Draw distal anatomic or mechanical axis (line along distal segment)
- Point where these lines intersect = CORA
- CORA represents the apex of deformity
- Single-plane deformity has one CORA
- Multiplanar deformity has multiple CORAs
- Oblique plane deformity appears different in AP and lateral views
ACA (Angulation Correction Axis) is perpendicular to the plane of deformity at CORA. When the osteotomy is made at CORA and rotated around ACA, perfect correction occurs. The ACA is a theoretical axis essential for 3D deformity correction.
Rotational (Torsional) Deformity: the Fourth Dimension
The CORA method handles angulation, translation and length; rotation (torsion) is the axial deformity it does not capture on the coronal film and must be assessed separately - a high-yield omission in many answers.
- Femoral anteversion: about 15 degrees in adults (higher in infancy, decreasing through growth).
- Tibial torsion: about 15 to 20 degrees of external (lateral) torsion in adults.
- Hip internal and external rotation (femoral version - excess internal rotation suggests increased anteversion).
- Thigh-foot angle and the transmalleolar axis (tibial torsion).
- Foot progression angle (net in- or out-toeing) and foot shape (to exclude metatarsus adductus).
the clinical profile screens, but a CT (or MRI) rotational study is the gold standard for quantifying femoral version and tibial torsion when surgery is considered.
- Malrotation after femoral or tibial intramedullary nailing - a common iatrogenic torsional deformity; compare with the contralateral limb on CT.
- "Miserable malalignment syndrome" - increased femoral anteversion plus external tibial torsion, producing squinting patellae, an increased Q-angle and patellofemoral pain.
- Symptomatic torsion is corrected by a derotation osteotomy (femoral or tibial), planned from the version difference relative to the normal or contralateral side.
Classification Systems
Deformity is classified by plane, by source segment and by the Paley osteotomy rule that the chosen cut will obey.
By plane of deformity
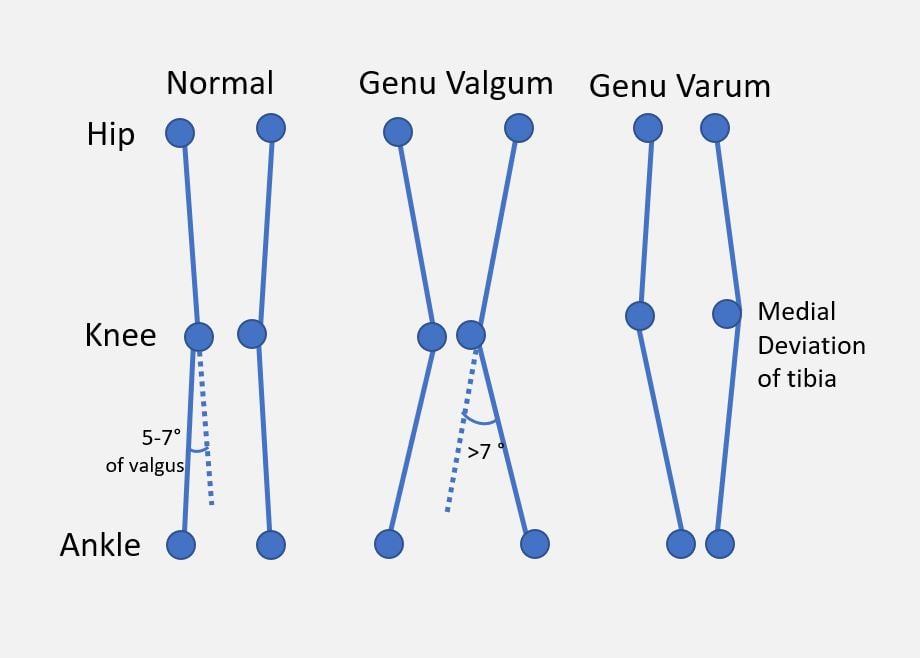
- Frontal (coronal): varus / valgus - measured on the long-leg AP (LDFA, MPTA, MAD).
- Sagittal: procurvatum / recurvatum - measured on the lateral (posterior proximal tibial angle, anterior/posterior distal femoral angle).
- Axial (rotational): internal / external torsion - assessed clinically and on CT rotational profile.
- Oblique-plane: the true apex lies between the cardinal planes; the deformity looks different on AP and lateral, and the correction axis (ACA) must be set in the oblique plane.
- Translational and length: pure axis shift (no angulation) and limb-length discrepancy frequently coexist with angular deformity.
Clinical Presentation
Patient Assessment
- Etiology of deformity (congenital, developmental, post-traumatic)
- Duration and progression
- Symptoms: pain, instability, functional limitation
- Previous surgery
- Gait analysis
- Limb alignment (standing, supine)
- Joint range of motion
- Ligamentous stability
- Limb length measurement
- Rotational profile
Indications for Correction
- Pain related to malalignment
- Gait abnormality
- Progressive deformity
- Accelerated compartmental wear
- Prevent arthrosis progression
- Improve joint preservation
- Optimize alignment before or instead of arthroplasty
Investigations
Imaging
- Full-length AP from hip to ankle
- Weight-bearing essential
- Single cassette or stitched images
- Mechanical axis (hip center to ankle center)
- MAD (deviation at knee)
- LDFA, MPTA, LDTA
- JLCA (joint line congruence angle)
- Limb length
- Assess sagittal plane alignment
- Posterior tibial slope (normal 10°)
- Recurvatum/procurvatum deformity
- Accurate length measurement
- Rotational profile assessment
- 3D deformity analysis possible
Intraoperative Technique
Once planning is complete, correction is executed and confirmed intra-operatively. A temporary external fixator (rail fixator with swivel clamps) or a guide-wire construct holds the planned correction while an alignment rod (cautery cord or long metal rod from femoral head centre to ankle centre) is screened across the knee to confirm the mechanical axis passes through the desired point before definitive internal fixation (plate or nail) is applied.
Stress Radiographs
Varus/valgus stress views:
- Assess ligament integrity
- Determine reducibility of deformity
- Distinguish bony from ligamentous deformity
Differential Localization of Malalignment
The single most examined skill is using joint orientation angles to decide WHERE the deformity sits. The same overall mechanical axis deviation can arise from very different sources, and each implies a different osteotomy. Work through the angles before naming a procedure.
- LDFA
- Normal (~87°)
- MPTA
- Decreased (e.g. 82°)
- JLCA
- Normal (0-2°)
- Interpretation / Osteotomy
- Tibia is the source → proximal tibial (HTO) realignment
- LDFA
- Increased (e.g. 93°)
- MPTA
- Normal (~87°)
- JLCA
- Normal (0-2°)
- Interpretation / Osteotomy
- Femur is the source → distal femoral osteotomy
- LDFA
- Abnormal
- MPTA
- Abnormal
- JLCA
- Normal
- Interpretation / Osteotomy
- Both bones contribute → consider double-level osteotomy in young patients
- LDFA
- Normal
- MPTA
- Normal
- JLCA
- Increased (greater than 3°)
- Interpretation / Osteotomy
- Deformity is in the joint (cartilage wear or laxity), NOT bone → osteotomy alone will not correct it
- LDFA
- ~87°
- MPTA
- ~87°
- JLCA
- 0-2°
- Interpretation / Osteotomy
- MAD within 0-10mm medial → no bony realignment indicated
Always check the JLCA before planning. A high JLCA means part of the apparent deformity comes from the joint itself (cartilage loss or collateral laxity), not the bone. Subtracting the intra-articular component prevents over-correction of the bony osteotomy. This is a classic viva discriminator between a pass and a strong pass.
Management
CORA Method Planning
Step 1: Draw mechanical axes
- Proximal mechanical axis from hip to knee
- Distal mechanical axis from knee to ankle
- Note intersection point (CORA)
Step 2: Measure joint orientation angles
- LDFA: Should be 87°
- MPTA: Should be 87°
- JLCA: Should be 0-2°
- Identify which angle is abnormal
Step 3: Localize the deformity
- Abnormal LDFA = femoral deformity
- Abnormal MPTA = tibial deformity
- Abnormal both = combined deformity
- Abnormal JLCA = joint line obliquity
Step 4: Plan osteotomy
- Ideal: Osteotomy at CORA (angulation only)
- Alternative: Osteotomy away from CORA (accept translation)
- Calculate correction angle
Step 5: Determine correction magnitude
- Target MAD: 0 to 10mm medial for neutral alignment
- For medial compartment OA: 3-5mm lateral (slight overcorrection)
- For lateral compartment OA: Neutral to slight medial
This section covers CORA method planning.
Surgical Management
Paley's Osteotomy Rules
Rule 1: Osteotomy at CORA
- When osteotomy is made at CORA and angulated
- Result is pure angular correction
- No translation created
- Ideal scenario for deformity correction
- Osteotomy level matches apex of deformity
- Hinge at CORA allows rotation around ACA
- Clean angular correction
- No secondary deformity
- Predictable outcome
- May not always be practical (CORA in joint, periarticular)
- May require intra-articular osteotomy
This section covers Rule 1.
Choosing Opening vs Closing Wedge (and the Wedge Magnitude)
Beyond locating the CORA, the examiner wants the opening-versus-closing decision and its trade-offs, plus a feel for the wedge size:
- Opening wedge
- Cut on the CONCAVE side and distract it open
- Closing wedge
- Remove a wedge from the CONVEX side and close it
- Opening wedge
- Lengthens
- Closing wedge
- Shortens
- Opening wedge
- Needs graft or substitute to fill the gap; slower union
- Closing wedge
- Bone-on-bone, no graft; faster and more inherently stable union
- Opening wedge
- Single cut, easier fine-tuning, but relies on an intact far hinge
- Closing wedge
- Two cuts, less adjustable but inherently stable
- Opening wedge
- Medial opening-wedge HTO increases posterior tibial slope and can cause patella baja
- Closing wedge
- Lateral closing-wedge HTO risks the common peroneal nerve and usually needs a proximal fibular osteotomy or division
Wedge magnitude (rule of thumb): each degree of coronal correction shifts the weight-bearing line roughly 3 to 4 mm across the tibial plateau (Dugdale), and any joint-space opening from lateral laxity must be subtracted to avoid over-correction. The opening-wedge gap height is approximately the osteotomy width multiplied by the tangent of the correction angle.
So choose the wedge by the desired length change and the cortex you wish to preserve, protect the far hinge in an opening wedge, and always remember the common peroneal nerve in a lateral closing-wedge HTO.
Complications
Planning Errors
- Incorrect axis drawing: Leads to wrong CORA location
- Measurement errors: Wrong correction magnitude
- Ignoring JLCA: Joint line obliquity persists
- Sagittal plane neglect: Changes tibial slope unexpectedly
Surgical Complications
- Under/over correction: Inadequate planning or execution
- Secondary deformity: Translation from osteotomy away from CORA
- Joint line obliquity: Uncorrected or created
- Slope changes: Particularly with opening wedge HTO
Postoperative Care
Rehabilitation protects the osteotomy hinge and fixation while restoring motion.
- Weight-bearing: opening-wedge osteotomies (a tension construct relying on the intact far hinge) are usually protected with toe-touch/partial weight-bearing for ~6 weeks; closing-wedge and compressed constructs (more inherently stable) allow earlier loading at surgeon discretion.
- Hinge protection: avoid premature full load that can fracture or collapse the far cortex (loss of correction).
- Motion: early knee range of motion to prevent stiffness; quadriceps activation and patellar mobilisation, especially after opening-wedge HTO where patella baja can develop.
- Graft / gap: opening wedges filled with autograft, allograft or substitute; monitor for delayed union at the gap.
- Frame care (gradual correction): pin-site care, scheduled strut/ring adjustments per the planned schedule, and serial alignment radiographs.
- Imaging: check correction and union with standing long-leg films; confirm the mechanical axis has reached the planned target rather than just "looks straight".
- Thromboprophylaxis per unit protocol; remove temporary external fixation once internal fixation/union is secure.
Outcomes and Prognosis
- Alignment is the dominant survival factor. After valgus tibial osteotomy, achieving at least ~8° valgus (slight overcorrection) gave ~90% 5-year and ≥65% 10-year survival; under-correction in an overweight patient dropped 10-year survival to ~19% (Coventry 1993).
- Disease modification: because frontal-plane malalignment multiplies the odds of compartmental OA progression 4-5 fold (Sharma 2001), restoring the mechanical axis genuinely slows medial (or lateral) wear, not just symptoms.
- Valgus correction is different: distal femoral osteotomy should aim for neutral, since over-correction into varus sharply overloads the medial compartment (Wu 2022).
- Joint-line obliquity left uncorrected (single-level fix of a double-level deformity) is associated with shear and less durable results - the rationale for double-level osteotomy in the young.
- Conversion to arthroplasty: a prior osteotomy does not preclude later TKA but can modestly increase technical difficulty; osteotomy is best viewed as an arthroplasty-sparing, time-buying procedure in the young active patient.
- Prognostic modifiers: obesity, smoking, large corrections, advanced cartilage loss and inaccurate planning all worsen outcome; accurate CORA-based planning and adequate (not excessive) correction optimise it.
Guidelines, Registries & Global Practice
Deformity analysis using the Paley CORA framework is the internationally accepted standard, taught in FRCS (Tr & Orth), FRACS, EBOT/FEBOT, ABOS and DNB/MS curricula. Practice differs mainly in imaging access, fixation philosophy and resource availability rather than in the underlying geometry.
Global Epidemiology and Burden
- Symptomatic knee osteoarthritis affects an estimated 250 to 300 million people worldwide, and frontal-plane malalignment is one of the strongest modifiable mechanical risk factors for progression (Sharma et al, JAMA 2001).
- Realignment osteotomy volume is rising in younger, active patients (typically under 60) as an arthroplasty-sparing option, with the highest relative use in regions where joint preservation is prioritised.
- Post-traumatic and developmental (rickets, Blount disease, physeal injury, skeletal dysplasia) deformities form a larger share of the caseload in limited-resource and high-prevalence settings.
Society Guidance and Frameworks (side by side)
- Position on realignment around the knee
- Osteotomy is an accepted option for unicompartmental OA with malalignment in younger, active patients; emphasises full-length weight-bearing alignment assessment
- Position on realignment around the knee
- Recognises osteotomy as a joint-preserving alternative to arthroplasty in selected younger patients; alignment correction central to decision-making
- Position on realignment around the knee
- Provides the operative technique standards and the Paley malalignment test / CORA planning method as the reference for osteotomy execution
- Position on realignment around the knee
- Consensus supports osteotomy for early compartmental OA with correctable malalignment; target alignment individualised, avoiding routine large overcorrection
The named-society positions above are guideline-level statements rather than primary trial data.
Registry and Outcome Notes
- National arthroplasty registries (NJR UK, AJRR US, AOANJRR Australia, SHAR Sweden, NZJR New Zealand) record prior osteotomy as a factor in subsequent knee arthroplasty; prior osteotomy does not preclude later conversion but can modestly increase technical complexity.
- Long-term cohort data (Coventry et al, JBJS 1993) anchor the principle that adequate, slightly over-corrected alignment is the dominant survival factor after valgus tibial osteotomy.
High- vs Limited-Resource Practice Variation
- Typical workflow
- Long-leg weight-bearing or EOS imaging, digital templating (TraumaCad, Bone Ninja, mediCAD), patient-specific cutting guides and locking-plate fixation; CT for rotational and 3D analysis
- Typical workflow
- Stitched/composite plain films or clinical alignment assessment, manual acetate templating, circular (Ilizarov/Taylor Spatial Frame) or monolateral external fixators that allow gradual, adjustable correction without advanced imaging
Gradual correction with circular frames remains a globally important technique because it tolerates planning imprecision, corrects multi-apical and large deformities, and manages associated limb-length discrepancy and soft-tissue contracture.
Controversies & Areas of Uncertainty
- Target alignment - neutral vs constitutional varus. The traditional teaching is to overcorrect a varus knee to roughly 3-5mm lateral MAD (around 8 degrees valgus per Coventry). More recent debate around "constitutional varus" questions whether driving every patient to mechanical neutral is necessary or even ideal; correction should be individualised to the patient's native alignment and pathology rather than applied as a fixed formula.
- Overcorrection in valgus knees is different. Unlike varus HTO, distal femoral osteotomy for valgus should generally aim only for neutral or very slight varus. Biomechanical data show that pushing into varus sharply loads the medial compartment and may accelerate medial OA (Wu et al 2022).
- Single- vs double-level correction. When both LDFA and MPTA are abnormal, a single large correction restores the mechanical axis but leaves an oblique joint line. Double-level osteotomy normalises both joint orientation and avoids joint-line obliquity, at the cost of a bigger operation. The threshold for accepting residual obliquity versus operating at two levels is not firmly defined.
- Acute internal fixation vs gradual external correction. Acute correction with plates is faster and avoids prolonged frame time but is less forgiving of planning error; gradual correction with circular frames allows fine adjustment and large/multi-apical correction but carries pin-site and patient-tolerance burden. Choice is driven by deformity magnitude, soft tissue, and resources, not by a single right answer.
- Sagittal-plane consequences. Medial opening-wedge HTO tends to increase posterior tibial slope and can alter patellar height; these secondary effects are real and must be planned for, but the precise magnitude and clinical significance remain debated.
MCQ Practice Points
Q: What is the CORA and why is osteotomy at it ideal? A: The Center of Rotation of Angulation - the point where the proximal and distal axes intersect (the apex of the deformity). An osteotomy made AT the CORA produces pure angular correction with NO translation (Paley Rule 1).
Q: What are the normal values of the LDFA and MPTA? A: Both are 87° (± 3°). An abnormal LDFA localises the deformity to the femur; an abnormal MPTA localises it to the tibia.
Q: A varus knee has normal LDFA and MPTA but a JLCA of 6°. Where is the deformity? A: In the joint (intra-articular cartilage loss or collateral laxity), not the bone. A bony osteotomy alone will not correct it, and failing to subtract the intra-articular component risks over-correction.
Q: Why is a high tibial osteotomy a Paley Rule 2 osteotomy? A: Because the CORA of a varus knee sits at the joint line, but the osteotomy is made below it. Correcting angulation therefore also creates a (usually acceptable) lateral translation of the distal tibia.
Q: What is the alignment target for an HTO in medial-compartment OA, and how does it differ for a valgus DFO? A: Slight OVERcorrection to ~3-5mm lateral MAD (≈8° valgus) for varus-OA HTO (maximises survival, Coventry); but a valgus distal femoral osteotomy should aim only for neutral, as overcorrection into varus overloads the medial compartment.
At a Glance: Quick Decision Guide
- Answer
- The intersection of the proximal and distal axes - the apex of the deformity
- Answer
- Distance from the mechanical axis (hip-to-ankle) to the knee centre; normal 0-10mm medial
- Answer
- Both 87° (± 3°)
- Answer
- Tibial deformity → proximal tibial (HTO) osteotomy
- Answer
- Femoral deformity → distal femoral osteotomy
- Answer
- Intra-articular/ligamentous component - not correctable by bony osteotomy alone
- Answer
- Pure angulation, no translation (Paley Rule 1)
- Answer
- Angulation PLUS translation (Paley Rule 2)
- Answer
- Slight overcorrection to ~3-5mm lateral MAD
- Answer
- Neutral to only slight varus - do NOT overcorrect
- Normal Value
- 87° ± 3°
- Location
- Lateral angle between femoral mechanical axis and knee joint line
- Normal Value
- 87° ± 3°
- Location
- Medial angle between tibial mechanical axis and knee joint line
- Normal Value
- 90° ± 5°
- Location
- Lateral angle between femoral mechanical axis and femoral neck axis
- Normal Value
- 89° ± 3°
- Location
- Lateral angle between tibial mechanical axis and ankle joint line
- Normal Value
- 0-10mm medial
- Location
- Mechanical axis deviation at knee
LLMM 87-87Joint Orientation Angles
Hook:LDFA and MPTA are both 87 degrees - easy to remember!
CORAOsteotomy Planning Steps
Hook:CORA method = systematic deformity analysis!
AT-AT-TPaley Osteotomy Rules
Hook:Rule 1 = AT CORA no translation; Rule 2 = Away from CORA = translation!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are shown a long-leg standing radiograph of a 55-year-old with medial compartment osteoarthritis. The LDFA is 87°, MPTA is 82°. Analyze this deformity.”
“A young adult has valgus malalignment with LDFA of 93° and MPTA of 93°. How do you analyze and plan correction?”
“Explain Paley's Rule 1 and Rule 2 for osteotomy planning.”
Normal Joint Orientation Angles
- LDFA: 87° ± 3° (lateral distal femoral angle)
- MPTA: 87° ± 3° (medial proximal tibial angle)
- LPFA: 90° ± 5° (lateral proximal femoral angle)
- MAD: 0-10mm medial to knee center
CORA Determination
- Draw proximal segment axis
- Draw distal segment axis
- Intersection = CORA (apex of deformity)
- Single plane = one CORA; multiplanar = multiple
Paley Osteotomy Rules
- Rule 1: At CORA = angulation only
- Rule 2: Away from CORA = angulation + translation
- Rule 3: Translation osteotomy = axis shift only
- HTO is a Rule 2 osteotomy
Localizing Deformity
- Abnormal LDFA = femoral deformity
- Abnormal MPTA = tibial deformity
- Both abnormal = double-level deformity
- Abnormal JLCA = joint line obliquity
HTO Planning for Varus OA
- Target MAD: 3-5mm lateral (overcorrection)
- CORA at joint line, osteotomy below
- Accept lateral translation of tibia
- Opening wedge increases posterior slope
DFO Planning for Valgus
- Target MAD: 0 to slight medial
- CORA at distal femur
- Lateral opening or medial closing wedge
- Consider combined osteotomy if biplanar
Evidence Base
Mechanical Axis Deviation - The CORA Concept (Landmark)
- Defined the apex of deformity using individual mechanical axis lines of each bone segment and joint reference lines of hip, knee and ankle
- Osteotomy at the apex (CORA) requires angulation only; an osteotomy proximal or distal to the apex additionally requires translation to correct accurately
- Frontal-plane angular deformity produces both mechanical axis deviation and malorientation of adjacent joints
Preoperative Planning for High Tibial Osteotomy
- Each degree of tibiofemoral angulation shifts the weight-bearing line 3 to 4 mm across the tibial plateau
- Every 1 mm of lateral tibiofemoral joint separation adds roughly 1 degree of varus, which must be subtracted to avoid overcorrection
- Provided a reproducible algorithm to calculate wedge size based on tibial and femoral length
Normal Axial Alignment of the Lower Extremity (Reference Values)
- In 25 normal young men the knee sat in a mean 1.1 to 1.5 degrees of varus between the tibial and femoral mechanical axes
- The knee transverse axis was a mean 2.6 to 3.0 degrees from perpendicular to the tibial mechanical axis
- The femoral anatomic axis does NOT pass through the centre of the knee, confirming the anatomic-mechanical offset
Malalignment Drives Knee OA Progression (Landmark Cohort)
- Varus alignment gave a 4-fold increase in odds of medial OA progression (adjusted OR 4.09, 95% CI 2.20-7.62) over 18 months
- Valgus alignment gave a near 5-fold increase in odds of lateral OA progression (adjusted OR 4.89, 95% CI 2.13-11.20)
- Greater malalignment severity correlated with greater joint-space loss and functional decline
Long-Term Survivorship After Valgus Tibial Osteotomy
- 87 valgus tibial osteotomies, median follow-up 10 years, with arthroplasty as the failure endpoint
- Valgus angulation of at least 8 degrees at 1 year gave a 90 percent 5-year and at least 65 percent 10-year survival
- Inadequate correction (under 8 degrees valgus) in an overweight patient dropped 10-year survival to 19 percent
Correction Angle in Distal Femoral Osteotomy for Valgus
- Compartment stresses were balanced near a neutral hip-knee-ankle angle of 178 to 180 degrees
- Correction into varus sharply raised medial compartment stress (90.9 percent increase) versus lateral unloading (19.3 percent)
- Optimal valgus-knee target is neutral to only slight varus (0 to 2 degrees); overcorrection risks medial OA