High Risk, High Vigilance
- Vascular Risk: Popliteal artery is tethered. Hyperextension injuries are highest risk.
- Compartment Syndrome: Common secondary to vascular injury or direct trauma.
- Anatomical Reduction: Essential for all types.
- Growth Arrest: 20-30% risk. Follow for at least 2 years.
- Ligaments Protect Physis: Injuries often associated with high energy.
- “Check pulses and compartments carefully
- “Low threshold for angiography
- “Valgus stress tests ligament vs physis
- “Follow for growth disturbance
The proximal tibia has the HIGHEST vascular injury risk of pediatric physeal fractures around the knee.
- The popliteal artery is tethered as it passes under the soleal arch.
- In hyperextension injuries, the artery can be stretched, intima can tear, or thrombosis can occur.
- An absent pulse after injury requires URGENT assessment (ABI, CTA, vascular surgery).
- Compartment syndrome commonly follows vascular injury (reperfusion or direct ischemia).
- Importance
- 55% of tibia, 25% of leg
- Clinical Relevance
- Second highest in lower limb
- Importance
- Popliteal artery tethered
- Clinical Relevance
- Highest of knee physes
- Importance
- 20-30%
- Clinical Relevance
- Less than distal femur but significant
- Importance
- Collateral ligaments attach to epiphysis
- Clinical Relevance
- Relatively protected area
PCNEvaluation Priorities
Hook:PCN - Primary Check Neurovasc.
Overview/Epidemiology
Proximal Tibial Physeal Injuries are relatively uncommon due to the protected nature of the physis.
- Epidemiology:
- Account for less than 3% of all physeal injuries.
- Mean age 12-14 years.
- Boys are more commonly affected.
- Mechanism:
- Hyperextension: Highest vascular risk.
- Varus/Valgus Stress: May be mistaken for ligament injury.
- Direct Trauma: High-energy mechanisms (MVA, sports).
- Why Less Common?
- The medial and lateral collateral ligaments attach to the tibial epiphysis (below the physis), providing protection.
- Valgus stress that would injure the MCL in an adult may cause a proximal tibial physeal fracture in a child.
Anatomy and Pathomechanics
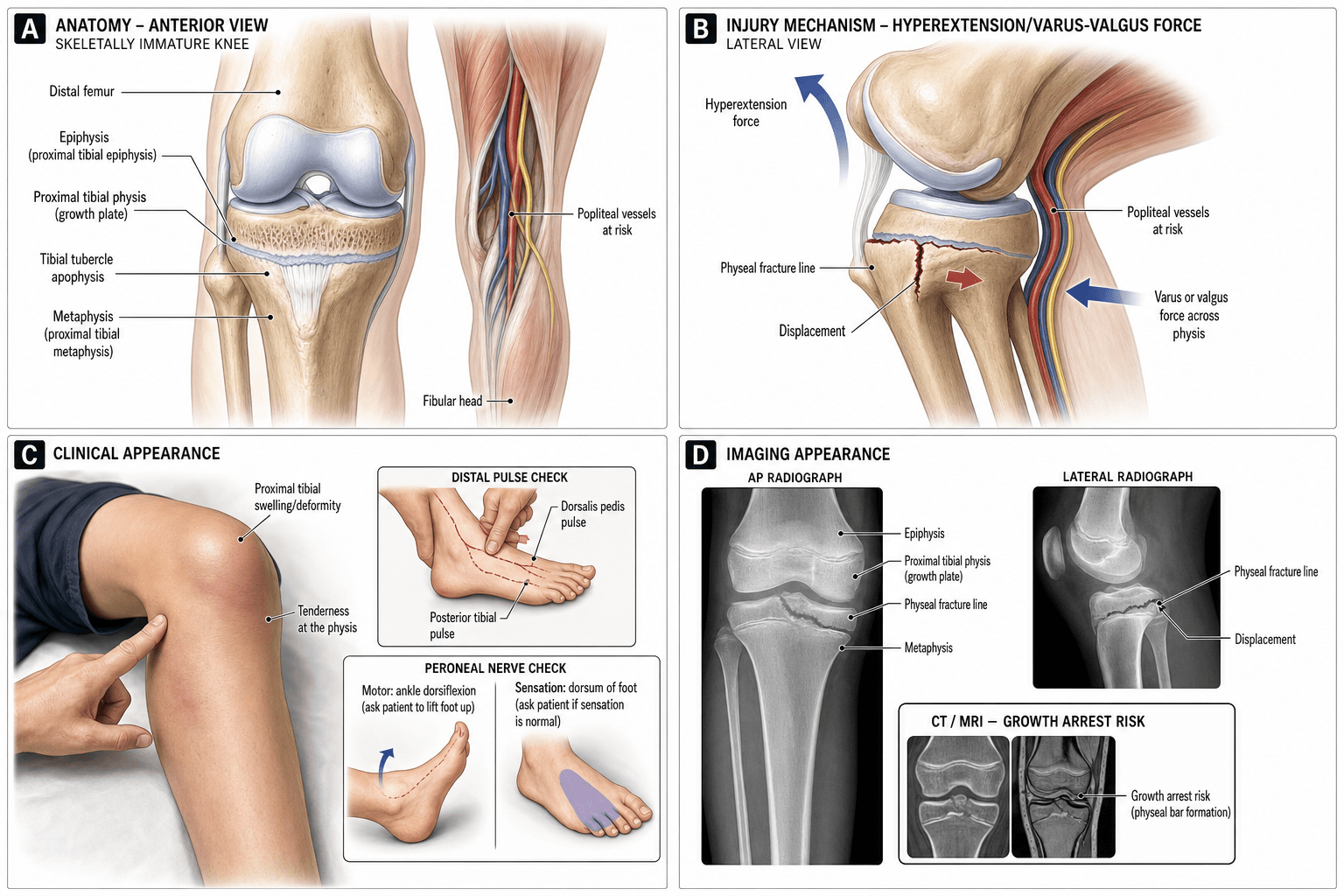
Physeal Anatomy
- The proximal tibial physis is an irregular physis with mamillary processes.
- It contributes 55% of tibial length (approximately 6mm/year).
- The tibial tubercle apophysis is contiguous with the proximal physis anteriorly.
Vascular Anatomy
- The popliteal artery passes close to the posterior aspect of the physis.
- It is tethered at the soleal arch (where it becomes the anterior and posterior tibial arteries).
- Hyperextension can stretch the artery over the posterior tibial metaphysis.
- Vascular injury risk is higher than distal femoral injuries.
Nerve Anatomy
- The common peroneal nerve winds around the fibular neck.
- It can be injured in varus injuries or direct trauma.
Classification Systems
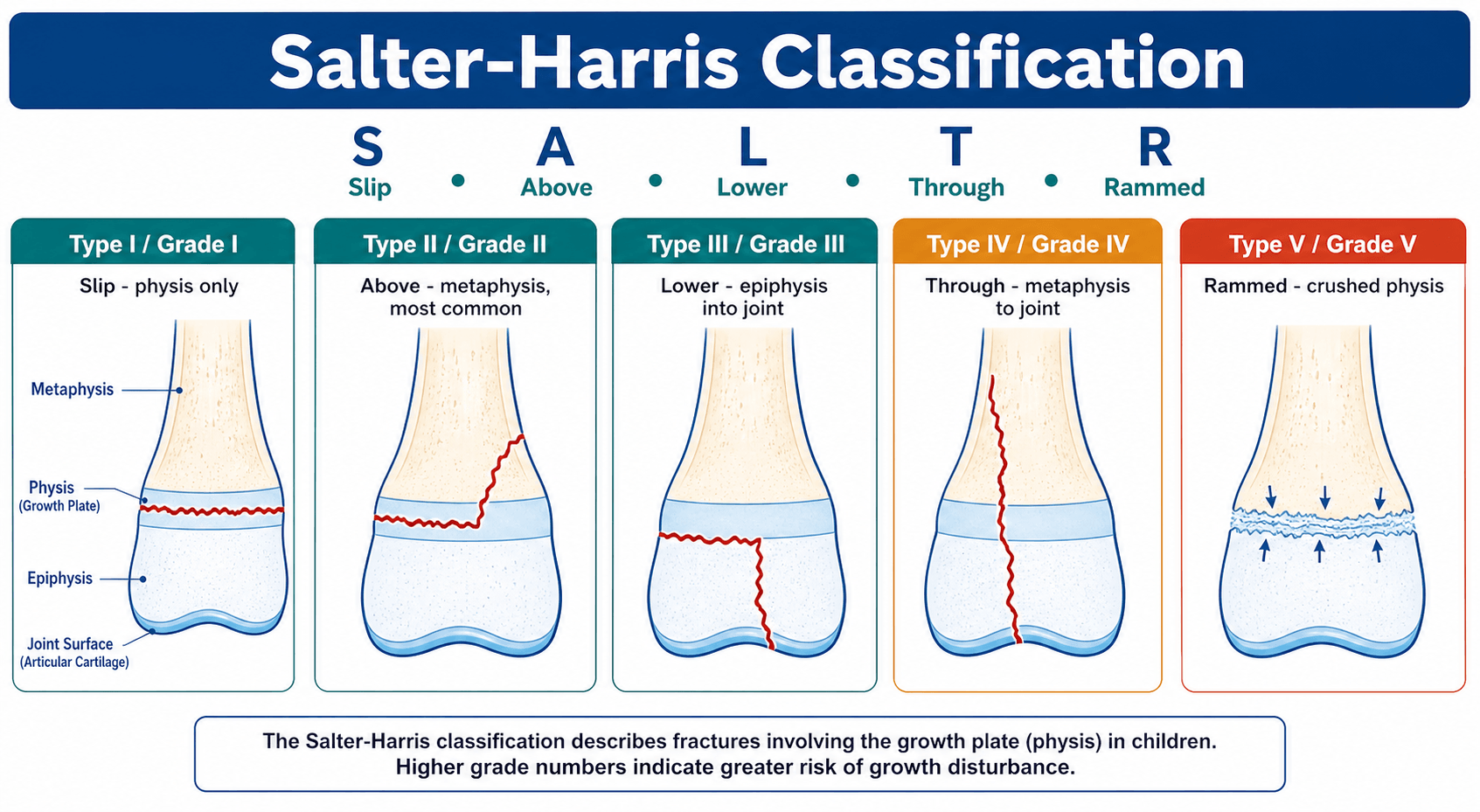
Salter-Harris Classification
Type I: Through the physis only. May be occult on X-ray.
Type II: Most common (60%). Metaphyseal fragment (posterolateral or posteromedial).
Type III: Intra-articular. Usually tibial eminence avulsions are managed separately.
Type IV: Crosses all layers. High arrest risk. ORIF required.
Clinical Assessment
- Mechanism: Hyperextension? Valgus stress? Direct blow?
- Neurovascular Symptoms: Numbness, cold foot, weakness?
- Inspection: Swelling, deformity, skin tenting, ecchymosis.
- Palpation: Tenderness over the proximal tibial physis.
- Neurovascular (CRITICAL): Popliteal pulse, DP, PT. Capillary refill. Peroneal nerve function.
- Compartments: Palpate all four leg compartments. Pain on passive stretch of toes is a key sign.
- Ligaments: Valgus stress may reveal physeal opening vs MCL laxity (physis is weaker in children).
Investigations
- X-ray (AP and Lateral): Standard. Include the knee and distal tibia.
- Stress Views: With caution. Under anesthesia if needed.
- CT Scan: For Type III/IV to map the fracture.
- MRI: If occult injury suspected or to assess ligaments.
- Ankle-Brachial Index (ABI): If pulses are asymmetric or diminished.
- Doppler Ultrasound: If equipment available.
- CT Angiography: If vascular injury suspected.
Differential Diagnosis
- Key Distinguishing Feature
- Point tenderness over the physis; valgus opens the plate not the joint line
- Confirmatory Step
- Physeal widening on X-ray, stress view if occult
- Key Distinguishing Feature
- Rare in children; tenderness at MCL not physis
- Confirmatory Step
- Valgus laxity with a firm endpoint; MRI if unclear
- Key Distinguishing Feature
- Tense haemarthrosis, extension block
- Confirmatory Step
- Lateral X-ray shows eminence fragment; MRI
- Key Distinguishing Feature
- Tenderness over tubercle, extensor lag
- Confirmatory Step
- Lateral X-ray; CT for intra-articular extension
- Key Distinguishing Feature
- Tenderness above the joint over the distal femoral physis
- Confirmatory Step
- X-ray; even higher arrest risk than proximal tibia
- Key Distinguishing Feature
- Apprehension, may have spontaneously reduced
- Confirmatory Step
- Skyline view, osteochondral fragment, MRI
Management Algorithm
Non-Displaced / Minimally Displaced Fractures
- Long Leg Cast: Knee in slight flexion (20 degrees).
- Duration: 6 weeks.
- Close follow-up with weekly X-rays to monitor for displacement.
- Consider prophylactic pinning given the high stakes.
RSSManagement Principles
Hook:RSS - Reduce, Stabilize, Surveil.
Surgical Techniques
Closed Reduction and Percutaneous Pinning
Indications: Displaced Type I/II with acceptable closed reduction.
Technique: Reduction under fluoroscopy. For hyperextension injuries, flex the knee and apply anterior force to the proximal fragment. Once reduced, pass 2-3 smooth K-wires from the metaphysis, crossing the fracture into the epiphysis. Diverge wires for stability. Cut flush or bury.
Post-op: Long leg cast for 6 weeks. Pin removal at 4-6 weeks.
Key Surgical Points
- Single reduction attempt to minimize physis damage.
- Document neurovascular status before and after every manipulation.
- Low threshold for fasciotomy if compartments are tense post-reduction.
Complications
- Rate
- 2-7%
- Prevention/Management
- Vascular assessment. Urgent repair.
- Rate
- Variable
- Prevention/Management
- Low threshold for fasciotomy.
- Rate
- 20-30%
- Prevention/Management
- Anatomical reduction. Monitor long-term.
- Rate
- Common with partial arrest
- Prevention/Management
- Bar excision or osteotomy.
- Rate
- Common
- Prevention/Management
- Epiphysiodesis or lengthening.
- Rate
- Rare
- Prevention/Management
- Document pre-op. Avoid traction.
Postoperative Care
- Immobilization: Long leg cast for 6 weeks minimum.
- Weight Bearing: Non-weight bearing initially.
- Pin Removal: 4-6 weeks.
- Vascular Monitoring: Close observation post-op for any vascular repair.
- Follow-Up Schedule:
- Weekly X-rays for first 2-3 weeks.
- 6-week X-ray (assess healing).
- 6-month and 12-month scanograms.
- Annual follow-up until skeletal maturity.
Rehabilitation Protocol
Phase 1: Immobilization (0-6 weeks)
- Long leg cast with knee in slight flexion.
- Non-weight bearing.
- Toe wiggling and calf pumps.
Phase 2: Early Mobilization (6-10 weeks)
- Cast removal when healed.
- Hinged knee brace initially.
- Progressive weight bearing.
- Active and passive ROM.
Phase 3: Strengthening (10-16 weeks)
- Progressive resistance exercises.
- Closed kinetic chain exercises.
- Proprioception training.
Phase 4: Return to Sport (4-6 months)
- Sport-specific training.
- Full ROM and strength.
- Clearance by surgeon.
Outcomes/Prognosis
- Growth Arrest: Occurs in 20-30% of cases.
- Vascular Injury: If unrecognized, can lead to limb loss.
- Compartment Syndrome: Early fasciotomy leads to good outcomes.
- Functional Outcomes: Generally good if complications are managed promptly.
Guidelines, Registries & Global Practice
Global Epidemiology
- Proximal tibial physeal fractures are rare, accounting for under 3% of all physeal injuries; the proximal tibia is one of the least frequently fractured physes in the lower limb because the collateral ligaments insert on the epiphysis and shield the plate.
- In the population-based Olmsted County cohort, physeal fractures overall show a 2:1 male predominance, peak at 11-12 years (girls) and 14 years (boys), and are most often Salter-Harris II (Peterson 1994).
- Mechanism distribution varies by region: sport and road-traffic trauma dominate in high-income settings, whereas falls and pedestrian/vehicle injuries predominate where helmet/seatbelt legislation and traffic segregation are limited.
Side-by-Side Principles (no single-country frame)
- Emphasis relevant to this injury
- Mandatory documentation of pulses and compartments; CT for intra-articular (SH-III/IV) patterns; anatomical reduction of the joint surface
- Emphasis relevant to this injury
- Open fractures and limb-threatening vascular injury are time-critical transfers to a combined ortho-plastic/vascular centre; serial neurovascular observation
- Emphasis relevant to this injury
- Smooth K-wires across an open physis; avoid threaded implants crossing the plate; single gentle reduction to limit iatrogenic physeal damage
- Emphasis relevant to this injury
- Hard signs of arterial injury mandate immediate exploration; ABI under 0.9 or asymmetry warrants CT angiography
These sources converge on the same clinical pathway (urgent neurovascular assessment, anatomical reduction, physis-sparing fixation, surveillance to maturity); genuine disagreement is minimal and mostly concerns imaging thresholds.
Registry Note
- There is no dedicated paediatric physeal-fracture registry equivalent to arthroplasty registries (NJR, AJRR, AOANJRR). Evidence rests on single-centre series (Shelton-Canale, Wozasek) and population datasets (Olmsted County), so absolute complication rates carry wide confidence intervals.
High- vs Limited-Resource Practice
- High-resource: ready CT angiography, 24/7 vascular and fasciotomy capability, scanograms/EOS for limb-length surveillance.
- Limited-resource: handheld Doppler and ABI replace CTA; clinical compartment monitoring substitutes for pressure transducers; surveillance relies on long-leg radiographs and clinical leg-length blocks. Delayed presentation raises the proportion of established ischaemia and growth arrest.
Deep Dive: Popliteal Artery Injury
Why is it at Risk?
- The popliteal artery is tethered both proximally (at the adductor hiatus) and distally (at the soleal arch).
- In hyperextension injuries, the artery is stretched over the posterior tibial metaphysis.
- The artery can be lacerated, intima torn (leading to thrombosis), or go into spasm.
Signs of Vascular Injury
- Hard Signs: Absent pulse, expanding hematoma, bruit, active bleeding.
- Soft Signs: Diminished pulse, proximity to major vessel, history of hemorrhage.
Management
- Any hard sign = urgent exploration.
- Soft signs = ABI (less than 0.9 is concerning) and CTA.
- If confirmed injury: Reduce fracture, stabilize with external fixation, vascular repair.
- Fasciotomy is often needed for reperfusion injury.
Golden Time
- 6 hours of warm ischemia is the limit before irreversible muscle necrosis.
- Earlier is better.
Deep Dive: Physeal Bar Resection (Langenskiold Procedure)
The complications table, Viva 4 and the Xiao card all invoke "bar excision with fat interposition" — here is the procedure those references rely on.
When to resect. A partial physeal arrest (a bony bar tethering part of the plate while the rest keeps growing) produces progressive angular deformity, shortening, or both. Resection is considered when the bar is less than about 50% of the physeal area and the child has meaningful growth remaining (commonly quoted as at least 2 years or 2 cm). A near-mature child, or a bar over 50%, is usually better served by completion epiphysiodesis (with contralateral epiphysiodesis as needed) and a deformity correction rather than resection. The detailed guided-growth and epiphysiodesis decision-making is developed in the limb-length-discrepancy-epiphysiodesis and guided-growth-angular-deformity-correction topics.
Mapping the bar. Quantify the bar's size and location with a CT or MRI physeal map (the percentage of the physis involved, and whether it is central or peripheral). Post-traumatic bars at the proximal tibia are typically peripheral — which both drives the angular deformity and makes the bar accessible from the side.
Technique (Langenskiold).
- Approach the bar directly (peripheral bar) or through a metaphyseal window (central bar), using fluoroscopy and loupe/headlight or arthroscopic illumination to see the cartilage-bone interface.
- Excise the entire bony bridge back to healthy, glistening physeal cartilage on every margin, confirming normal physis circumferentially.
- Interpose a material to stop the bar re-forming — autologous fat is the commonest (cranioplast/PMMA or silastic are used in some series).
- Place metallic markers in the epiphysis and metaphysis to track resumption of growth on serial radiographs.
- At the proximal tibia, protect the popliteal vessels and common peroneal nerve and avoid the tubercle apophysis.
What to expect. Resection most reliably halts or improves the angular deformity but is unreliable for restoring length — in the Xiao 2023 series angular deformity improved by over 5 degrees in most children, yet leg-length discrepancy still increased in a substantial minority. Counsel families that a separate length plan (epiphysiodesis or lengthening) is often still required, and that the bar can recur.
Q: A 7-year-old has a small lateral proximal-tibial bar with progressive valgus and years of growth left. What does bar resection achieve? A: It can release the tether and improve or halt the valgus, but it does not reliably restore lost length — plan separately for any residual leg-length discrepancy. Reserve resection for a bar under about 50% with growth remaining; interpose fat and mark with metal for surveillance.
Diagnosing the Occult or Equivocal Physeal Injury
A non-displaced Salter-Harris I can spring back into alignment and look normal on static films — Shelton and Canale found stress radiographs were essential to the diagnosis in 3 of their patients, and this topic flags both "may be occult on X-ray" and the valgus-injury mimic of an MCL sprain. Two tools resolve the equivocal case.
Stress radiography. Under adequate analgesia or anaesthesia, a gentle valgus/varus (or hyperextension) stress is applied under fluoroscopy: in a child the physis opens (confirming a physeal fracture) whereas a true collateral-ligament injury opens the joint line. This both makes the occult SH-I diagnosis and distinguishes it from ligament laxity. The caveat — and why the topic says "with caution" — is that forced stress can displace or further injure the physis, so it is gentle, single and image-guided.
MRI has become the preferred alternative where available because it shows the physeal injury, marrow oedema and any ligament damage without stressing the plate, and it clarifies SH-III/IV geometry alongside CT. Reserve provocative stress views for settings without ready MRI access.
The key teaching point: a normal-looking radiograph after a valgus knee injury in a child does not exclude a physeal fracture — treat the tender physis as injured and confirm with stress views or MRI rather than labelling it a sprain.
Controversies & Areas of Uncertainty
- Prophylactic pinning of non-displaced fractures. Some surgeons pin all proximal tibial physeal fractures given the high stakes of late displacement near the popliteal vessels; others reserve fixation for displaced or unstable patterns and manage stable injuries in a cast with close radiographic review. No randomised data exist; the choice is driven by stability, reliability of follow-up and surgeon preference.
- The "true" growth-arrest rate. Frequently quoted as 20-30%, but the figure derives from small, old, single-centre series with heterogeneous fracture types (Shelton-Canale, Wozasek). Higher-grade (SH-III/IV) and high-energy injuries skew the rate upward; isolated non-displaced SH-I/II fractures likely sit well below it. Treat the number as a counselling range, not a precise risk.
- Reduce-first vs image-first in the pulseless limb. With a malaligned, pulseless limb the pragmatic teaching is to reduce immediately (alignment alone may restore flow) rather than delay for angiography. The counter-argument is that reduction can mask an intimal injury; persistent pulse deficit after reduction always mandates CT angiography and vascular involvement.
- Routine cross-sectional imaging. CT improves mapping of SH-III/IV and reveals intra-articular extension missed on plain films in up to half of complex cases (Pandya/Mubarak); the trade-off is radiation in a child, so its use is selective rather than universal.
- Bar resection expectations. Physeal bar excision improves angular deformity but is unreliable for restoring length (Xiao 2023); whether to add concurrent hemi-epiphysiodesis, accept the deformity, or plan staged correction remains individualised.
Parent's Guide: Understanding Proximal Tibial Injuries
What is the proximal tibial growth plate? The proximal tibia (shinbone near the knee) has a growth plate that is responsible for about 55% of the shinbone's growth. Injury here is serious because it can affect how your child's leg grows.
Why is this injury particularly concerning? The major artery and nerve that supply the leg pass very close to this growth plate. Injury here can sometimes damage these structures, which requires urgent treatment.
What signs should we watch for?
- A cold or pale foot.
- Numbness or tingling in the foot.
- Severe pain that is not relieved by medication.
- A calf that feels very tight or hard.
If any of these occur, seek medical attention immediately.
What follow-up is needed? Regular X-rays for at least 2 years to monitor the growth plate.
Surgical Pearls
Reduction Technique
- Apply longitudinal traction with the knee slightly flexed.
- For hyperextension injuries (posterior displacement of the proximal metaphysis), flex the knee and push the metaphysis anteriorly.
- Avoid excessive force. Single gentle reduction attempt is preferred.
Pinning Technique
- Enter from the lateral and medial metaphysis, superior to the physis.
- Direct the wires distally, crossing the fracture into the epiphysis.
- Diverge the wires for stability (3-point fixation concept).
- Image in two planes (AP and lateral) to confirm position.
- Avoid the tibial tubercle apophysis and the articular surface.
Post-Reduction Checks
- Check neurovascular status immediately after reduction.
- Document pulses both before and after manipulation.
- Confirm reduction on X-ray before leaving the operating room.
- Low threshold for fasciotomy if there is any compartment concern.
Comparison: Proximal Tibia vs Other Physes
- Proximal Tibia
- Less than 3% of physeal injuries
- Distal Femur
- 1-5% of physeal injuries
- Proximal Tibia
- 55% of tibia
- Distal Femur
- 70% of femur
- Proximal Tibia
- Highest of all knee physes
- Distal Femur
- High but lower than prox tib
- Proximal Tibia
- 20-30%
- Distal Femur
- 30-50%
VCGProximal Tibia Dangers
Hook:VCG - The three dangers.
MCQ Practice Points
Q: What percentage of tibial length does the proximal tibial physis contribute? A: 55%. This is the largest growth contributor in the tibia.
Q: What vascular structure is at highest risk in proximal tibial physeal injuries? A: Popliteal Artery. It is tethered at the soleal arch.
Q: What is the approximate growth arrest rate for proximal tibial physeal fractures? A: 20-30%.
Q: A child has a valgus stress injury with physeal widening. What does this represent? A: Physeal fracture (not MCL injury). The physis is weaker than the ligament in children.
Q: What is the most feared early complication after proximal tibial physeal injury? A: Compartment syndrome - requires low threshold for fasciotomy due to tight leg compartments.
Q: When is physeal bar excision indicated for growth arrest? A: When the bar is less than 50% of physis width with at least 2 years of growth remaining.
Self-Assessment Quiz
Additional Self-Assessment Questions
Additional Self-Assessment Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“11-year-old cyclist thrown over handlebars. Hyperextension injury to the knee. Obvious deformity. Foot is cold and pale. No palpable DP pulse.”
“Same patient. Vascular repair was successful. 6 hours later, the leg is tense and the child is in severe pain despite analgesia.”
“13-year-old tackled while playing football. Valgus force to the knee. Tender medially over the proximal tibia. X-ray shows widening of the proximal tibial physis medially.”
“9-year-old, 1 year post Type II proximal tibial physeal fracture. Now has progressive valgus of 12 degrees and 1.5cm LLD.”
“9-year-old MVA. Multiple injuries including a displaced proximal tibial physeal fracture. Hemodynamically stable after resuscitation.”
“12-year-old with knee pain after football. Tender over the proximal tibial physis. X-ray shows subtle physeal widening medially.”
KEY FACTS
- 55% Tibial Growth
- 25% Leg Length
- Highest Vascular Risk
- 20-30% Arrest Risk
DANGERS
- Popliteal Artery
- Compartment Syndrome
- Peroneal Nerve
- Growth Arrest
TREATMENT
- Anatomical Reduction
- Smooth K-Wire Pinning
- ORIF for Type III/IV
- 6+ Week Immobilization
SURVEILLANCE
- Weekly X-rays Early
- 6-Month Scanogram
- Annual to Maturity
- Low Threshold Angio
Evidence Base
- 39 proximal tibial epiphyseal fractures over 25 years (Campbell Clinic)
- 2 patients had popliteal artery disruption, both with posterior shaft displacement
- 24 of 28 fractures had satisfactory results at mean 7.1-year follow-up; failures from neurovascular insufficiency, growth disturbance or arthritis
- Stress radiographs were essential to diagnosis in 3 patients
- 30 proximal tibial epiphyseal injuries over 28 years; 53% displaced
- 3 patients had peripheral ischaemia at presentation; 1 developed delayed popliteal thrombosis
- 1 above-knee amputation resulted from delayed diagnosis of the vascular lesion
- Worst outcomes associated with leg-length discrepancy after concomitant ipsilateral femoral/tibial fracture
- 29 physeal fractures about the knee; 13 involved the proximal tibia
- 14 of 29 (48%) had ligament instability at mean 66-month follow-up
- 8 of 13 proximal tibial fractures had ligament laxity (anterior drawer/Lachman or valgus)
- First report of complex proximal tibial physeal fracture with concomitant MCL rupture
- Population-based study: 850 children sustained 951 physeal fractures (1979-1988)
- Male:female ratio 2:1; peak incidence at 11-12 years (girls) and 14 years (boys)
- Salter-Harris type II was the most common pattern overall (54%)
- Overall age- and sex-adjusted incidence 279 per 100,000 person-years
- 41 operative tibial tubercle/proximal tibial physeal fractures (all male, mean age 15)
- Compartment syndrome or vascular compromise in nearly 10% — all in the physeal (type B) subgroup
- Lateral radiograph alone underestimated injury in 50% of cases; CT/MRI advised
- Proposed a development-based classification accounting for intra-articular extension
- 19 children with distal femoral, proximal tibial or distal tibial physeal bars
- Bar resection (+/- hemi-epiphysiodesis) improved angular deformity over 5 degrees in 63%
- Length correction was unreliable — LLD increased over 5 mm in 37% despite surgery
- No neurovascular injury, infection or fracture; followed to maturity or minimum 2 years