Motion-Preserving Wrist Salvage | Capitate Into Lunate Fossa | SLAC/SNAC Wrist | Kienbock Disease | Dorsal Approach | PIN Neurectomy
- PRC is a motion-preserving salvage procedure for scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist, and for Kienbock disease - it is NOT a primary arthroplasty
- The critical prerequisite is intact articular cartilage on both the capitate head and the lunate fossa of the radius - if either surface is degenerate, PRC will fail and four-corner fusion or total wrist fusion should be performed instead
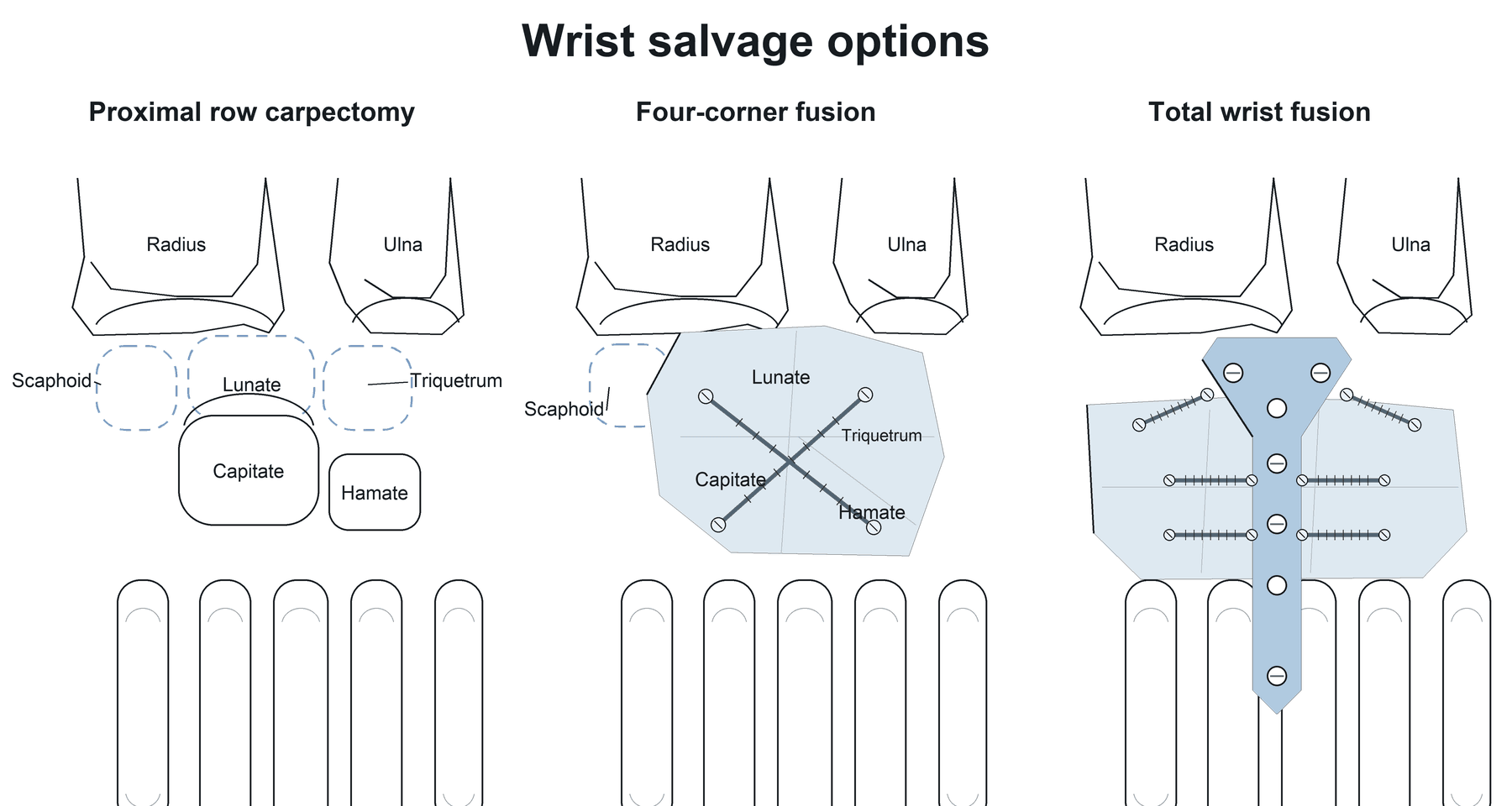
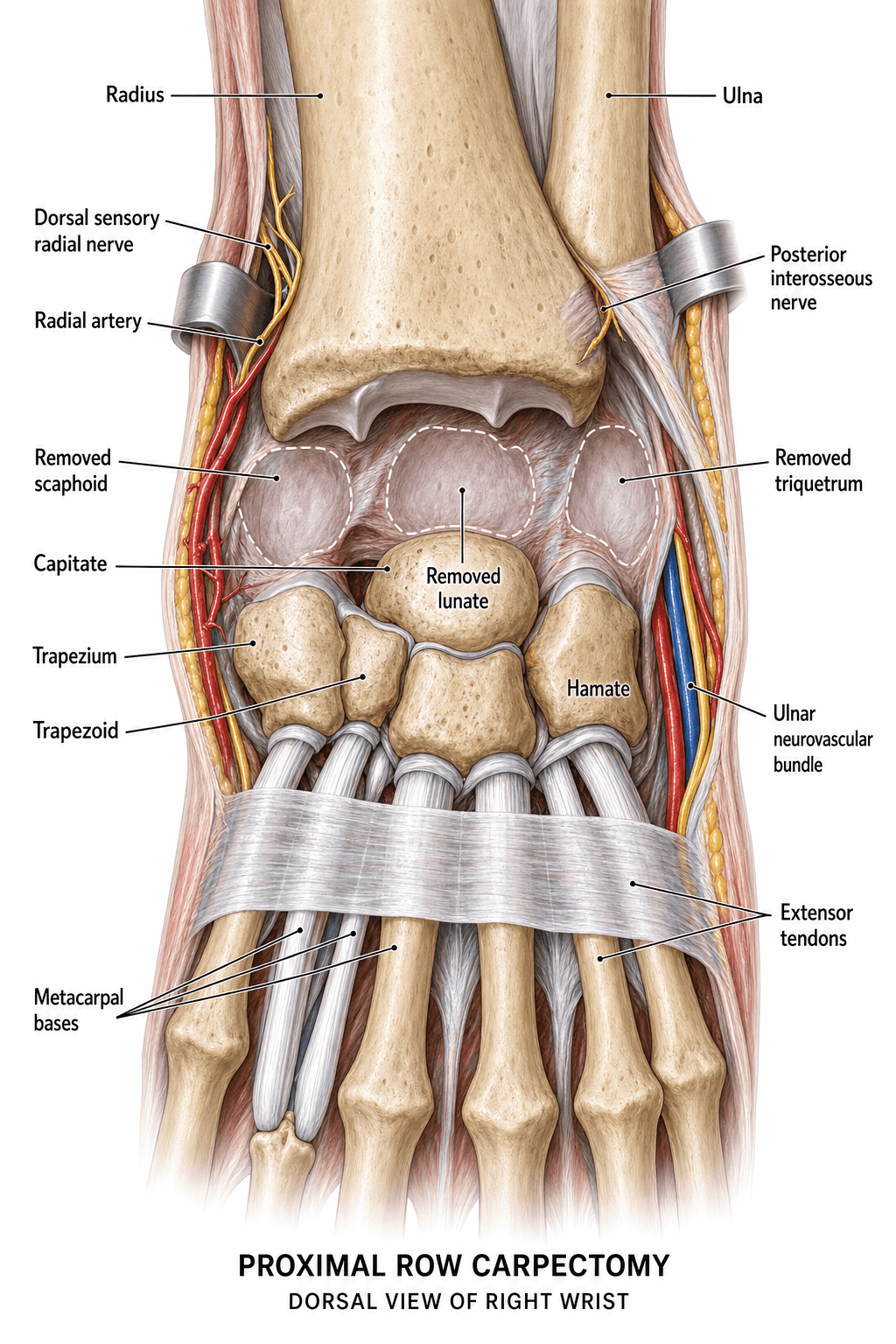
- PRC removes the scaphoid, lunate, and triquetrum and allows the capitate to migrate proximally and seat into the lunate fossa, creating a new simplified radiocarpal articulation
- Post-operative wrist flexion-extension arc is approximately 60-65% of the contralateral side, and grip strength is approximately 50-60% - patients must understand these expectations pre-operatively
- Dorsal approach with posterior interosseous nerve (PIN) neurectomy is the standard technique; PIN neurectomy provides partial denervation of the wrist joint and augments pain relief
- “Always begin a viva answer by confirming the lunate fossa and capitate head cartilage are intact - if not, PRC is contraindicated
- “SLAC wrist pattern: arthritis begins at the radioscaphoid joint and progresses to the scaphocapitate joint, but the radiolunate joint is preserved until late - this is why PRC works
- “SNAC wrist: arthritis pattern is similar but the scaphoid nonunion site determines the distribution; the proximal pole fragment articulates with the radius
- “The key advantage of PRC over four-corner fusion is simplicity: no hardware, no nonunion risk, shorter immobilisation, and faster rehabilitation
Proximal Row Carpectomy
PRC fails when the capitate head cartilage or the lunate fossa of the radius is damaged. In SLAC/SNAC stage III (scaphocapitate arthritis with capitate head degeneration) or stage IV (pancarpal arthritis), PRC is contraindicated. Examiners want to see you inspect both articular surfaces intra-operatively before excising the proximal row. If either surface is worn, convert to four-corner fusion or total wrist fusion.
- Best option
- Proximal row carpectomy (PRC)
- Reasoning
- Simpler surgery, no hardware, retains functional wrist motion, faster recovery; contraindicated if capitate head or lunate fossa cartilage is damaged
- Best option
- Four-corner fusion (4CF) with scaphoidectomy
- Reasoning
- Preserves the radiolunate articulation; capitate degeneration is irrelevant because midcarpal joint is fused; better grip strength than PRC
- Best option
- Total wrist fusion (TWF)
- Reasoning
- Reliable pain relief; sacrifices all wrist motion; best salvage option when both radiocarpal and midcarpal joints are destroyed
- Best option
- Proximal row carpectomy (PRC)
- Reasoning
- Removes the fragmented lunate and creates a stable articulation between capitate and lunate fossa; effective in stages where lunate is beyond salvage
Overview and Indications
The proximal row carpectomy (PRC) is a motion-preserving salvage procedure for wrist arthritis in which the scaphoid, lunate, and triquetrum are excised, allowing the capitate to migrate proximally and articulate directly with the lunate fossa of the radius. The procedure was first described by Stamm in 1946 and has since become a well-established treatment for selected patients with SLAC and SNAC wrist arthritis, as well as Kienbock disease.

by removing the arthritic proximal carpal row and creating a simplified radiocarpal joint (capitate head into lunate fossa), pain is relieved while retaining a functional arc of wrist flexion and extension. The native lunate fossa cartilage is preserved in SLAC/SNAC wrist because arthritis characteristically spares the radiolunate articulation until very late stages.
- SLAC wrist (Watson and Ballet classification): stage I (radioscaphoid arthritis) and stage II (radioscaphoid + scaphocapitate arthritis) with intact lunate fossa and capitate head
- SNAC wrist: analogous stages with preserved lunate fossa and capitate head cartilage
- Kienbock disease (Lichtman stage IIIA or early IIIB): when the lunate is fragmented and beyond salvage but the lunate fossa and capitate head are preserved
- Chronic carpal instability with secondary arthritis limited to the radioscaphoid and midcarpal joints
- Failed prior procedures such as radial shortening or capitate-shortening osteotomy for Kienbock disease
- Elderly or low-demand patients who prioritise pain relief over maximum grip strength (PRC is simpler than 4CF in this group)
- Manual labourers who understand the functional trade-offs (approximately 50-60% grip strength, approximately 60-65% motion arc)
- Patients who cannot comply with prolonged immobilisation required for four-corner fusion
Examiners test your ability to exclude unsuitable patients. Key contraindications: capitate head cartilage degeneration, lunate fossa arthritis (radiolunate involvement), inflammatory arthritis (rheumatoid, psoriatic), SLAC/SNAC stage IV (pancarpal), active wrist infection, severe osteoporosis (poor bone quality for new articulation), and pre-operative wrist flexion-extension arc less than 30 degrees (indicating severe capsular contracture that will not improve with PRC).
Relevant Anatomy and Biomechanical Principles
- The proximal carpal row (scaphoid, lunate, triquetrum) functions as an intercalated segment between the radius/ulna and the distal carpal row. Its removal fundamentally alters wrist kinematics, converting a complex two-row system into a simplified hinge.
- The lunate fossa is the concave articular surface on the distal radius that normally articulates with the lunate. In SLAC/SNAC wrist, this surface is characteristically preserved because the pathological mechanics of scaphoid collapse and rotatory subluxation load the radioscaphoid joint first.
- The capitate head is the convex proximal surface of the capitate that normally articulates with the scaphoid and lunate at the midcarpal joint. It is slightly smaller in radius of curvature than the lunate fossa, which means the contact area after PRC is reduced compared to the native joint. This size mismatch is the theoretical basis for long-term concern about capitate-lunate fossa degeneration.
- Scapholunate ligament disruption leads to scaphoid flexion (rotatory subluxation) and lunate extension (dorsal intercalated segment instability, DISI).
- The altered scaphoid position concentrates load at the radioscaphoid joint, leading to progressive arthritis.
- Because the lunate extends and rotates dorsally, the radiolunate joint is unloaded and its cartilage is preserved.
- The arthritis cascade follows a predictable sequence: radioscaphoid (stage I), then scaphocapitate (stage II), then capitate head degeneration (stage III), and finally pancarpal involvement including radiolunate (stage IV).
- Similar to SLAC but the initiating event is a scaphoid nonunion rather than scapholunate ligament rupture.
- The fracture creates two fragments: the distal pole (which remains connected to the distal row and maintains some motion) and the proximal pole (which may behave like a free fragment).
- Arthritis develops at the radioscaphoid joint and at the fracture site, but the radiolunate joint is again preserved until late stages.
while the SLAC sequence is the Watson radioscaphoid → scaphocapitate → capitolunate progression, the SNAC wrist has its own recognised stages:
- SNAC I — arthritis between the distal scaphoid fragment and the radial styloid (styloid–scaphoid).
- SNAC II — arthritis at the scaphocapitate joint.
- SNAC III — arthritis at the capitolunate (periscaphoid/midcarpal) joint. As with SLAC, the radiolunate joint is preserved until late, which is exactly why PRC (which relies on an intact lunate fossa) remains viable through these stages provided the capitate head is also intact.
- In Lichtman stage IIIA (lunate collapse without fixed scaphoid rotation) and early IIIB (lunate collapse with fixed scaphoid rotation), the lunate is fragmented and avascular beyond salvage.
- PRC removes the diseased lunate and creates a stable capitate-lunate fossa articulation, provided both surfaces are intact.
- This is an alternative to radial shortening osteotomy (for stage II-IIIA with ulnar-neutral or ulnar-positive variance) or lunate replacement/revascularisation procedures.
Internervous Plane and Surgical Interval
- Interval: the approach is developed through the third extensor compartment (containing the extensor pollicis longus, EPL) or in the interval between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis (ECRB). There is no true internervous plane at the wrist because the extensor tendons are all innervated by the posterior interosseous nerve (PIN), but the interval between EDC and ECRB is most commonly used.
- The dorsal retinaculum is divided over the third compartment and the EPL is transposed radially. A radial-based or ulnar-based retinacular flap is raised to expose the underlying extensor tendons and the dorsal wrist capsule.
- The dorsal wrist capsule is opened longitudinally or in an H-shaped fashion to provide wide exposure of the carpus. The capsular flaps are preserved for later repair.
- The posterior interosseous nerve (PIN) is identified on the floor of the fourth extensor compartment, lying on the interosseous membrane just distal to the radial styloid. It is divided for the PIN neurectomy component.
- EPL (third compartment): mobilised and protected; usually transposed subcutaneously
- EDC (fourth compartment): retracted ulnarly
- ECRB and ECRL (second compartment): retracted radially
- Radial sensory nerve branches: cross the radial aspect of the wrist in the subcutaneous tissue; must be protected during superficial dissection
- Dorsal capsular ligaments (dorsal radiocarpal ligament, dorsal intercarpal ligament): divided to access the carpus; repair is attempted during closure
The posterior interosseous nerve (PIN) provides sensation to the dorsal wrist capsule. Dividing it (PIN neurectomy) denervates the dorsal capsule and contributes to pain relief after PRC. It is found on the floor of the fourth extensor compartment, deep to the EDC tendons, just proximal to the radiocarpal joint. It is not the same as the motor PIN (which innervates the extensor muscles more proximally in the forearm) - the terminal sensory branch is what is divided here.
Patient Positioning and Setup
- Position: supine with the arm extended on a hand table (arm board). The shoulder is abducted approximately 60-80 degrees and the elbow is flexed. A padded bolster or rolled towel under the wrist facilitates dorsiflexion and exposure.
- Anaesthesia: general or regional anaesthesia (brachial plexus block - supraclavicular, infraclavicular, or axillary). Regional anaesthesia provides excellent post-operative analgesia and is commonly used.
- Tourniquet: a pneumatic tourniquet on the upper arm at 250 mmHg (or 100 mmHg above systolic BP) provides a bloodless field. Exsanguinate with an Esmarch bandage before inflation. Tourniquet time should be kept under 120 minutes.
- Fluoroscopy: an image intensifier is used to confirm complete excision of the proximal carpal row, proper seating of the capitate into the lunate fossa, and to check that no retained bone fragments remain. It is brought in from the head or foot of the table.
- Instrumentation: standard hand surgery instruments, osteotomes, rongeurs, Freer elevator, small Hohmann retractors, and a power burr (for smoothing any irregular bone surfaces). K-wires may be used for temporary fixation if needed.
- Magnification: loupe magnification (2.5x-4.5x) is recommended for precision during dissection and protection of volar ligamentous structures.
Surgical Technique
The standard approach for proximal row carpectomy. A longitudinal dorsal skin incision (approximately 6-8 cm) is centred over Lister tubercle, extending from the distal radius to the mid-metacarpal level. The subcutaneous tissue is carefully dissected to protect branches of the radial sensory nerve and the superficial radial nerve.
The third extensor compartment is opened and the EPL tendon is mobilised and transposed radially. A radially-based retinacular flap is raised from the fourth compartment, exposing the EDC tendons. The EDC tendons are retracted ulnarly and the ECRB/ECRL tendons are retracted radially.
The dorsal wrist capsule is opened longitudinally. The wrist joint is inspected - this is the critical decision point. The capitate head and the lunate fossa of the radius must be carefully examined. If both surfaces show intact cartilage, proceed with PRC. If either surface is significantly degenerate, abandon PRC and convert to four-corner fusion or total wrist fusion.
Scaphoid excision is performed first. The scaphoid is removed piecemeal using a rongeur and osteotome, or en bloc by dividing the scapholunate ligament, the scaphotrapezial ligament, and the volar capsular attachments. The scaphoid is often fragmented or sclerotic in SLAC/SNAC wrist, making piecemeal removal practical.
Lunate excision follows. The scapholunate and lunotriquetral ligaments are divided. The lunate is grasped with a towel clip or bone clamp and carefully mobilised by releasing the volar capsular attachments. The volar capsuloligamentous structures (especially the radioscaphocapitate ligament and the long radiolunate ligament) must be preserved to maintain carpal stability.
Triquetral excision completes the proximal row removal. The triquetrum is the easiest bone to remove, being the most ulnar and accessible.
After excision, the capitate is assessed for its reduction into the lunate fossa. Manual traction and ulnar deviation of the wrist help the capitate head migrate proximally into the lunate fossa. Fluoroscopy confirms concentric seating and adequate reduction. Any osteophytes or irregular surfaces on the capitate head or radial fossa are smoothed with a rongeur or power burr.
PIN neurectomy is performed by identifying the terminal PIN on the floor of the fourth extensor compartment, proximal to the radiocarpal joint. A 1-2 cm segment is excised and submitted for histological confirmation if desired.
During removal of the scaphoid and lunate, aggressive dissection volarly can damage the radioscaphocapitate (RSC) ligament, the long radiolunate (LRL) ligament, and the volar wrist capsule. These structures provide secondary stability to the capitate-lunate fossa articulation after PRC. If they are disrupted, the capitate may subluxate volarly. Dissect immediately against bone, staying subperiosteal, and avoid plunging through the volar capsule.
Structures at Risk and Complications
PRC has a favourable complication profile compared to four-corner fusion, largely because it avoids hardware-related problems and nonunion risk. However, specific complications must be understood:
-
Capitate-lunate fossa degeneration - the most significant long-term concern. Because the capitate head has a slightly smaller radius of curvature than the lunate fossa, contact pressures are higher than in the native joint. Over 10-20 years, degenerative changes may develop at this new articulation, leading to recurrent pain and the need for total wrist fusion. This is the principal argument against PRC in very young patients (under 40-45).
-
Volar subluxation of the capitate - if the volar capsuloligamentous structures (RSC ligament, LRL ligament) are damaged during proximal row excision, the capitate may subluxate volarly out of the lunate fossa. This causes pain, weakness, and a palpable volar prominence. Treatment requires capsular reconstruction or conversion to TWF.
-
Radial sensory nerve injury - branches of the superficial radial nerve cross the dorsal wrist in the subcutaneous tissue and are at risk during superficial dissection. Neuroma formation causes dorsal wrist and thumb dysesthesia. Meticulous handling and retraction of these branches is essential.
-
Extensor tendon irritation or rupture - chronic tenosynovitis or attrition over prominent bone edges (especially a retained scaphoid ridge) may irritate or rupture the EPL, EDC, or EIP tendons. Smooth all bone edges and ensure the retinaculum is repaired to provide a gliding surface.
-
Persistent pain - despite technically successful PRC, some patients experience residual wrist pain, particularly with heavy loading or end-range motion. PIN neurectomy reduces but does not eliminate this risk. Patients who smoke or who perform heavy manual labour are at higher risk for persistent symptoms.
-
Wrist stiffness - some loss of wrist motion is inherent to the procedure (the new articulation is less mobile than the native two-row system). Post-operative stiffness greater than expected may result from capsular contracture, prolonged immobilisation, or arthrofibrosis. Early protected mobilisation after 3-4 weeks reduces this risk.
-
Carpal tunnel syndrome - oedema or haematoma in the carpal tunnel after surgery may compress the median nerve. Pre-operative carpal tunnel symptoms should be addressed with concurrent release.
-
Reflex sympathetic dystrophy / complex regional pain syndrome (CRPS) - reported in approximately 2-5% of wrist surgery cases. Early recognition and multidisciplinary management are essential.
The capitate-lunate fossa articulation created by PRC is a size-mismatched joint. Over 15-20 years, many patients develop degenerative changes at this interface. This is why PRC is generally recommended for patients aged 50-60 years or older in some practices, while younger patients may be steered toward four-corner fusion (which preserves the native radiolunate joint). However, this age threshold is debated, and many surgeons offer PRC to younger patients who understand the potential need for future fusion.
Guidelines, Registries and Global Practice
There is no single universal guideline specifically for PRC; clinical practice follows evidence-based principles of carpal arthritis management and shared decision-making. Several international hand surgery societies have published consensus guidance:
- ASSH (American Society for Surgery of the Hand, US): PRC is recognised as a motion-preserving salvage option for SLAC/SNAC wrist and Kienbock disease when the lunate fossa and capitate head are preserved. The choice between PRC and four-corner fusion should be individualised based on patient age, demands, articular surface integrity, and surgeon experience.
- BSSH (British Society for Surgery of the Hand, UK): PRC is supported in national guidance as a treatment option for stage II and early stage III SLAC/SNAC wrist. The BSSH outcomes standards recognise both PRC and four-corner fusion as acceptable salvage procedures.
- FESSH (Federation of European Societies for Surgery of the Hand): European practice tends to favour four-corner fusion more than North American practice, though the gap has narrowed. FESSH position papers support both PRC and four-corner fusion as valid options, with the key discriminator being capitate head integrity.
- Large-scale national registries for wrist salvage procedures are less developed than arthroplasty registries. However, institutional series and systematic reviews consistently report approximately 80-90% patient satisfaction at 5-10 years and approximately 70-80% satisfaction at 15+ years after PRC.
- Conversion to total wrist fusion after failed PRC is reported in approximately 5-15% of patients at long-term follow-up, with higher conversion rates in younger patients and heavy manual labourers.
- European centres have historically favoured four-corner fusion over PRC, reflecting training traditions and concern about long-term capitate-lunate fossa degeneration. However, PRC adoption has increased as long-term data demonstrate acceptable durability.
- North American hand surgeons more commonly perform PRC, particularly in older or lower-demand patients, valuing its simplicity and lower complication rate.
- In Asia-Pacific practice, both procedures are widely used, with some centres reporting excellent results with PRC for Kienbock disease (reflecting the higher prevalence of Kienbock disease in this population).
- In low- and middle-income settings, PRC is valued for its simplicity (no expensive implants, no bone graft harvesting for fusion, shorter operative time) and predictable outcomes.
- Total wrist fusion after failed PRC is technically straightforward (no prior hardware to remove, no nonunion to address) and provides reliable pain relief.
- Patients should be counselled pre-operatively about the possibility of future fusion, particularly if they are young or perform heavy manual work.
Memory Aids
PRCPatient Selection for PRC - SLIC It Right
Hook:SLIC the wrist correctly - if the lunate fossa or capitate head is degenerate, PRC will fail
SLACSLAC Wrist Arthritis Progression - RAYS
Hook:RAYS tracks the sequential arthritis pattern - radioscaphoid to scaphocapitate to capitate to pancarpal
PRCPRC Surgical Steps - DICE It
Hook:DICE - Dorsal approach, Inspect surfaces, Cut the proximal row, Evaluate capitate seating and PIN neurectomy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old office worker presents with progressive right wrist pain and stiffness. She had a scapholunate ligament injury 8 years ago that was not treated. Radiographs show scapholunate dissociation with radioscaphoid arthritis and scaphocapitate joint narrowing. The radiolunate joint appears preserved. She wants to retain as much wrist motion as possible. Discuss your management.”
“A 40-year-old right-hand-dominant carpenter presents with progressive left wrist pain and stiffness. MRI shows Lichtman stage IIIB Kienbock disease with lunate collapse and early scaphoid flexion. The lunate is fragmented and avascular. He wants to continue working as a carpenter. Discuss the surgical options and justify your recommendation.”
One-liner
- Motion-preserving salvage: excision of scaphoid, lunate, and triquetrum with capitate seating into the lunate fossa
- Described by Stamm (1946); principle is to remove the arthritic proximal row and create a simplified radiocarpal joint
Indications
- SLAC wrist stage I-II (and early III if capitate head preserved)
- SNAC wrist analogous stages
- Kienbock disease Lichtman IIIA / early IIIB
- Chronic carpal instability with secondary arthritis
- Elderly or low-demand patients prioritising pain relief with motion
Absolute prerequisites (SLIC)
- Intact lunate fossa articular cartilage on the radius
- Intact capitate head cartilage
- No inflammatory arthritis, no pancarpal disease
- Both surfaces must be inspected intra-operatively before committing
Contraindications
- Capitate head degeneration (SLAC stage III)
- Radiolunate arthritis (SLAC stage IV, rheumatoid)
- Inflammatory arthritis involving the wrist
- Active infection, severe osteoporosis
- Pre-operative wrist motion less than 30 degrees flexion-extension
Surgical technique (DICE)
- Dorsal approach through third or fourth extensor compartment
- Inspect capitate head and lunate fossa first - critical decision point
- Excise scaphoid (piecemeal), lunate, then triquetrum
- Protect volar capsuloligamentous structures (RSC, LRL ligaments)
- PIN neurectomy on floor of fourth compartment
- Confirm concentric capitate seating with fluoroscopy
- Immobilise 3-4 weeks then progressive mobilisation
PRC vs Four-Corner Fusion
- PRC: simpler, no hardware, no nonunion risk, shorter recovery, slightly less grip strength
- 4CF: better grip strength, preserves radiolunate joint, but has hardware issues and nonunion risk
- Both provide comparable pain relief and patient satisfaction
- Choice depends on age, demands, articular integrity, and surgeon/patient preference
Outcomes
- Flexion-extension arc: approximately 60-65% of contralateral
- Grip strength: approximately 50-60% of contralateral
- Patient satisfaction: approximately 80-90% at 5-10 years
- Conversion to TWF: approximately 5-15% at long-term follow-up
- Long-term radiographic degeneration common but often asymptomatic
Complications
- Capitate-lunate fossa degeneration (long-term, 10-20 years)
- Volar subluxation of capitate if volar ligaments damaged
- Radial sensory nerve neuroma
- Extensor tendon irritation or rupture
- CRPS (approximately 2-5%)
- Persistent pain despite technically successful procedure
Evidence Base
- In a retrospective comparison of PRC (22 wrists) and four-corner fusion (23 wrists) for SLAC/SNAC wrist, both groups achieved significant pain relief. PRC patients had a shorter time to union (no fusion to wait for), fewer complications, and similar satisfaction rates. Four-corner fusion patients had slightly better grip strength but longer immobilisation and a nonunion rate of approximately 5-10%. The authors concluded that both procedures are effective but PRC is simpler and avoids nonunion risk.
- In 22 wrists with minimum 20-year follow-up after PRC, patient satisfaction remained high. The flexion-extension arc averaged 72 degrees. Radiographic degeneration at the capitate-radius articulation was common but often not symptomatic enough to require conversion to fusion in the majority of patients.
- Systematic review of outcomes after PRC versus four-corner fusion for SLAC/SNAC wrists showed both procedures provide good pain relief and patient satisfaction. PRC had lower complication rates and no nonunion risk, while four-corner fusion had slightly better grip strength in some studies.
- In 28 wrists with minimum 15-year follow-up after PRC, approximately 73% of patients were satisfied or very satisfied. Mean flexion-extension arc was approximately 85 degrees. Radiographic degeneration was present in the majority but only approximately 15% required conversion to total wrist fusion.