Definition | Risk Factors | Prevention | Management
- PJK definition: More than 10° kyphosis at UIV compared to preoperative
- Risk factors: Age, osteoporosis, over-correction, thoracic UIV
- Most occur 3-18 months postoperatively
- Prevention: Appropriate alignment targets, cement augmentation, soft tissue preservation
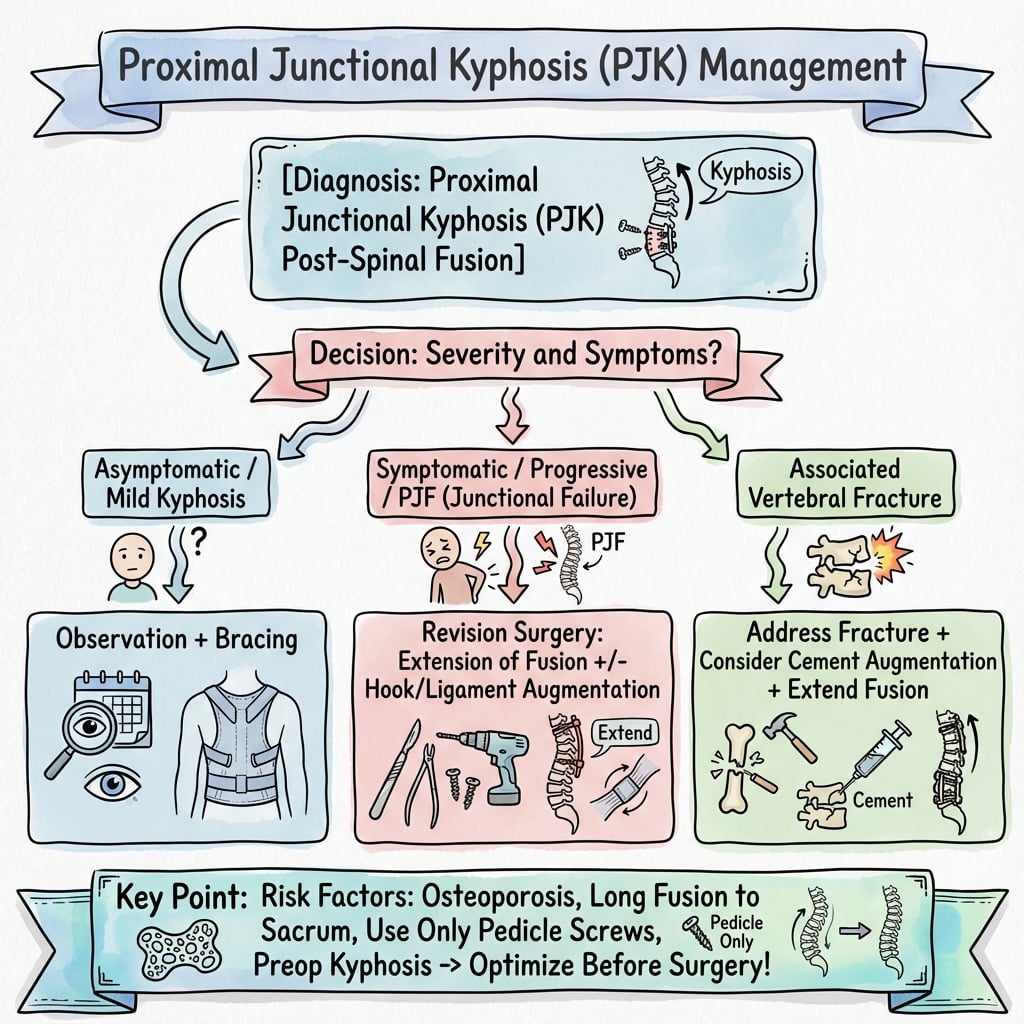
- Revision indications: Progressive deformity, neurological symptoms, significant pain
- “Not all PJK requires surgery - distinguish PJK from PJF
- “Over-correction of sagittal alignment increases PJK risk
- “Cement augmentation at UIV reduces PJK in osteoporotic patients
- “Upper thoracic UIV has higher PJK risk than thoracolumbar
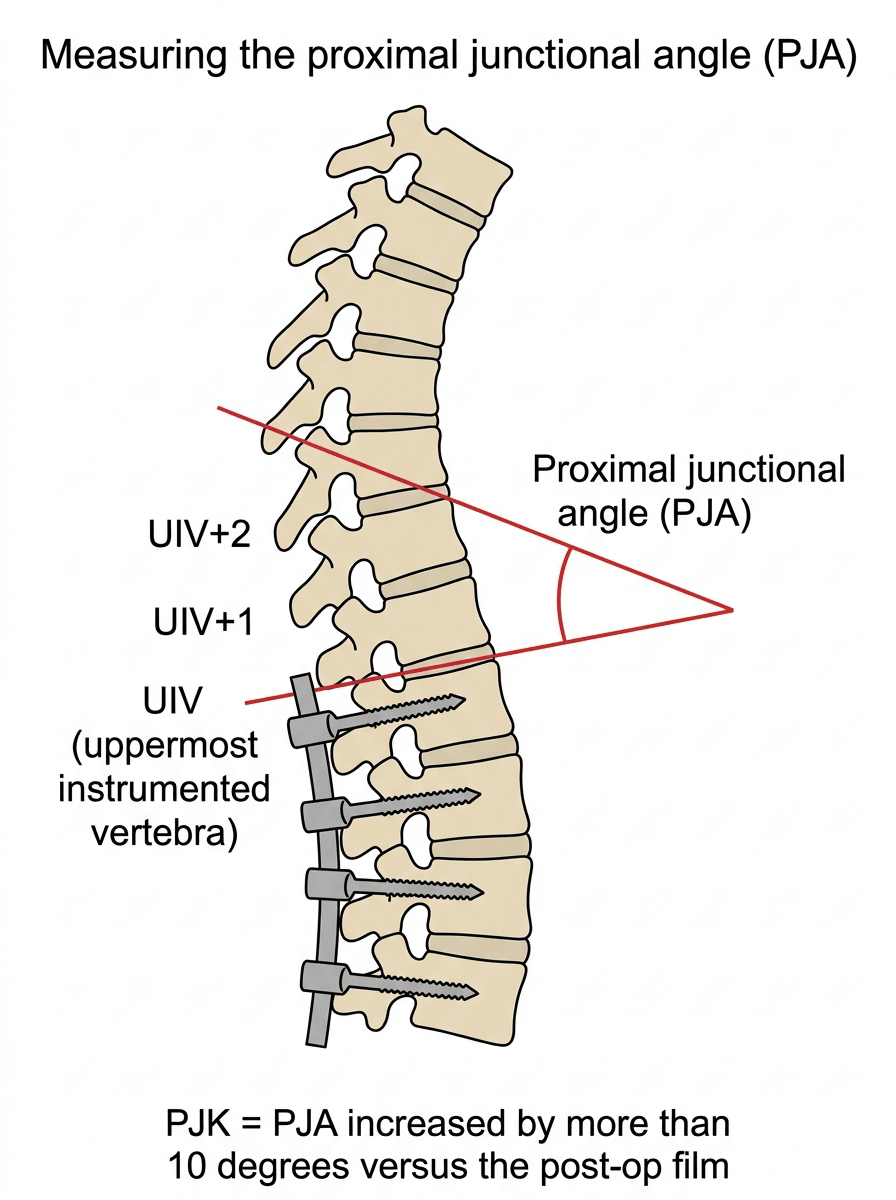
PJK is more than 10 degrees of kyphosis between the UIV inferior endplate and UIV+2 superior endplate, compared to immediate postoperative films. The Proximal Junction Angle (PJA) is measured at UIV to UIV+2 segment.
PJK: Radiographic finding, may be asymptomatic. PJF (Proximal Junctional Failure): Requires revision - includes vertebral fracture, ligament rupture, or implant failure. PJF is defined as PJA more than 28° or change more than 22°.
Key modifiable risk factors: over-correction of sagittal balance, excessive soft tissue disruption at UIV, inadequate bone quality without augmentation. Non-modifiable: age more than 60, osteoporosis, long fusion to pelvis.
Age-adjusted alignment goals in elderly patients to avoid over-correction. Cement augmentation at UIV and UIV+1 in osteoporotic bone. Soft tissue preservation and consider tethers or hooks at UIV.
- PJK
- PJA more than 10° vs preoperative
- PJF
- PJA more than 28° OR change more than 22°
- PJK
- 20-40%
- PJF
- 1.4-5.6%
- PJK
- Often asymptomatic
- PJF
- Pain, deformity, neurology
- PJK
- Usually observation
- PJF
- Often requires revision
Overview and Epidemiology
Proximal junctional kyphosis (PJK) is one of the most common mechanical complications following long-segment spinal fusion surgery, particularly in adult spinal deformity (ASD) correction. It represents excessive kyphosis development at the transition zone between the fused and unfused spine.
Definitions:
- PJK: Proximal junctional angle (PJA) more than 10 degrees compared to immediate postoperative values, measured between the UIV inferior endplate and UIV+2 superior endplate
- PJF (Proximal Junctional Failure): PJA more than 28 degrees OR change more than 22 degrees, often associated with fracture, ligament failure, or implant failure
Epidemiology:
- PJK Incidence
- 20-40%
- PJF Incidence
- 1.4-5.6%
- PJK Incidence
- 10-20%
- PJF Incidence
- Less than 2%
- PJK Incidence
- Up to 50%
- PJF Incidence
- 5-10%
- PJK Incidence
- 30-50%
- PJF Incidence
- 5-10%
Clinical Significance:
- PJK may be asymptomatic or cause significant morbidity
- PJF often requires revision surgery (40% revision rate)
- Healthcare costs substantially increased with PJK/PJF
- Most cases develop within first 18 months postoperatively
Distinguish PJK (a radiographic finding that may be stable) from PJF (a clinical/radiographic diagnosis requiring intervention). Not all PJK progresses to PJF, and many cases can be observed if stable and asymptomatic.
Pathophysiology and Anatomy
Mechanism of Development
PJK results from a mismatch between the mechanical demands at the proximal junction and the capacity of the adjacent tissues to withstand these loads.
Contributing Factors:
- Abrupt stiffness transition: Rigid fused construct meets mobile unfused spine
- Altered load distribution: Stress concentration at junctional level
- Sagittal imbalance: Forward trunk shift increases moment arm at UIV
- Tissue failure: Bone, ligament, or disc cannot withstand new loads
Anatomical Structures at Risk
- UIV vertebral body compression
- UIV+1 vertebral body fracture
- Superior endplate failure
- Posterior ligamentous complex (PLC)
- Interspinous and supraspinous ligaments
- Paraspinal musculature
- UIV/UIV+1 disc degeneration
- Accelerated adjacent segment disease
Biomechanical Principles
Stress Concentration:
The junctional zone experiences increased stress due to:
- Transition from fused to mobile segments
- Lever arm effect of long constructs
- Loss of shock absorption from fused discs
Sagittal Compensation:
When PJK develops, the body attempts to compensate:
- Cervical hyperlordosis
- Pelvic retroversion
- Knee flexion
Bone Quality Impact:
- Osteoporotic bone cannot resist vertebral compression
- Reduced pull-out strength of UIV screws
- Cortical thinning increases fracture risk
Classification Systems
PJK Radiographic Definition
Standard Definition (Glattes et al.):
PJK is present when the proximal junctional angle (PJA) exceeds 10 degrees compared to the first erect postoperative radiograph.
Measurement Technique:
- Identify the Upper Instrumented Vertebra (UIV)
- Measure angle between:
- Inferior endplate of UIV
- Superior endplate of UIV+2 (two levels above)
- Compare to immediate postoperative value
- PJK present if change is more than 10 degrees
Severity Grading:
- PJA Change
- 10-20°
- Clinical Significance
- Often asymptomatic, observe
- PJA Change
- 20-30°
- Clinical Significance
- May be symptomatic
- PJA Change
- More than 30°
- Clinical Significance
- Usually requires intervention
This classification helps standardize reporting and guide treatment decisions.
Clinical Assessment
History
- When was the index surgery? (Most PJK occurs 3-18 months)
- New or worsening back pain? (Character, location, severity)
- Change in posture or balance?
- Neurological symptoms? (Weakness, numbness, bowel/bladder)
- Functional limitations? (Walking tolerance, ADLs)
- Acute pain after minor trauma or sudden onset
- New neurological deficit
- Visible or palpable step-off at fusion end
- Rapidly progressive kyphosis
Physical Examination
- Standing posture - increased thoracic kyphosis
- Forward trunk lean
- Compensatory cervical hyperlordosis
- Visible prominence at UIV level
- Tenderness over UIV area
- Step-off or prominence at junctional level
- Muscle spasm
- Full motor examination (especially if PJF suspected)
- Sensory examination
- Reflexes
- Gait assessment
- Can the kyphosis correct with prone positioning?
- Hip flexion contracture (Thomas test)
Clinical Indicators for Intervention
Surgical Indications:
- Neurological deficit from compression
- Progressive deformity on serial imaging
- Intractable pain despite conservative measures
- Documented instability on dynamic films
- Skin breakdown risk from hardware prominence
New onset myelopathy or progressive neurological deficit in a patient with PJK/PJF requires urgent evaluation. Cord compression from kyphotic collapse or subluxation may necessitate emergent surgical intervention.
Differential Diagnosis of New Junctional Symptoms After Fusion
New pain or kyphosis above a fusion is not always mechanical PJK. The following must be considered and excluded.
- Distinguishing Feature
- Gradual angular change more than 10 deg vs post-op, often asymptomatic
- Key Investigation
- Standing long-cassette radiographs
- Distinguishing Feature
- UIV/UIV+1 fracture, ligamentous rupture or implant failure, acute pain
- Key Investigation
- CT (fracture/implant), MRI (cord/soft tissue)
- Distinguishing Feature
- Disc/facet degeneration above UIV without acute collapse
- Key Investigation
- MRI
- Distinguishing Feature
- Fracture remote from instrumentation, low-energy
- Key Investigation
- Radiograph/CT, DEXA
- Distinguishing Feature
- Pain, raised CRP/ESR, wound issues, sometimes loosening
- Key Investigation
- Inflammatory markers, MRI, aspiration
- Distinguishing Feature
- Failure at the caudal end of the construct
- Key Investigation
- Standing radiographs of whole construct
- Distinguishing Feature
- Constitutional symptoms, lytic lesion at junction
- Key Investigation
- MRI whole spine, staging
Investigations
Imaging Protocol
Step 1: Standing Full-Length Radiographs
- Compare to immediate postoperative films
- Measure PJA at UIV to UIV+2
- Assess global sagittal alignment (SVA, PI-LL)
- Evaluate hardware position
Step 2: CT Scan (If Indicated)
- Detect vertebral fracture at UIV/UIV+1
- Assess fusion mass (pseudarthrosis)
- Hardware evaluation (loosening, breakage)
- Bone quality assessment (HU values)
Step 3: MRI (If Neurological Symptoms)
- Cord compression assessment
- Soft tissue changes
- Disc pathology
- Posterior element integrity
Key Radiographic Measurements
Essential Measurements:
- Measurement
- UIV inferior to UIV+2 superior
- Significance
- More than 10° = PJK
- Measurement
- Compare to post-op film
- Significance
- More than 22° = PJF
- Measurement
- C7 plumb to S1
- Significance
- Global balance
- Measurement
- Document exact level
- Significance
- Upper thoracic = higher risk
Because over-correction of sagittal alignment is the key modifiable driver of PJK, the spinopelvic parameters must be understood. Pelvic incidence (PI) is a fixed morphological constant: PI = pelvic tilt (PT) + sacral slope (SS). The classic Schwab/SRS correction goals are a PI-LL mismatch within about 10 degrees, an SVA (sagittal vertical axis) under 5 cm, and a pelvic tilt under about 20 to 25 degrees (the T1 pelvic angle, TPA, combines trunk and pelvic malalignment in a single measure). The crucial PJK lesson (Lafage) is that these "ideal" young-adult numbers should be age-adjusted: older patients normally stand with a larger PI-LL mismatch, a more positive SVA and a higher pelvic tilt, so correcting an elderly patient to a young-adult profile is functional over-correction and the single most avoidable cause of PJK. Plan to a proportioned, age-appropriate target (the GAP score operationalises this proportionality, albeit with inconsistent external validation) rather than to fixed absolute values.
Dynamic Films (If Instability Suspected):
- Flexion-extension lateral radiographs
- Assess motion at UIV segment
- Document any subluxation
Bone Density Assessment
- Pre-existing T-score for baseline
- Repeat if osteoporosis treatment initiated
- UIV and UIV+1 vertebral body density
- Less than 110 HU suggests osteoporosis
- Guides cement augmentation need in revision
Management
Non-Operative Management
- Stable PJK (not progressing)
- Asymptomatic or minimally symptomatic
- Patient preference
- High surgical risk
- Serial radiographs every 3-6 months
- Monitor for progression
- Assess symptoms
- Analgesics (paracetamol, NSAIDs)
- Neuropathic agents if radicular pain
- Activity modification
- Core strengthening
- Postural training
- Maintain mobility
- Limited evidence for efficacy
- May provide symptom relief
- Consider TLSO for stabilization
- Treat osteoporosis (bisphosphonates, denosumab)
- Calcium and vitamin D supplementation
- Fall prevention
Patients with documented PJK should be monitored with standing radiographs every 3-6 months for the first 2 years to detect progression. Stable PJK can transition to annual surveillance.
Conservative management is appropriate for stable, asymptomatic PJK but requires ongoing surveillance for progression.
Surgical Technique
Revision Surgical Principles
- Extend to stable, horizontal vertebra
- Typically add 2-4 levels proximally
- Upper thoracic extension (T4 or higher) for recurrent PJK
- Consider cervical extension in severe cases
- Prophylactic vertebroplasty at new UIV and UIV+1
- Improves screw purchase in osteoporotic bone
- Reduces fracture risk
- Preserve interspinous/supraspinous ligaments at new UIV
- Consider hooks or sublaminar bands instead of screws at UIV
- Transition rods to reduce stiffness gradient
- Interbody cage at UIV level if disc space collapse
- Restores anterior column support
- Improves fusion potential
- Remove all posterior elements below UIV before extension
- Ensure adequate bone quality at new UIV
- Consider tethers or ligament augmentation at new UIV
- Rod flexibility at junction (cobalt chrome, transition rods)
Complication Prevention
At Revision:
- Address all risk factors for recurrence
- Cement augmentation in osteoporotic patients
- Age-adjusted alignment goals
- Avoid over-correction
Comprehensive prevention strategies implemented at primary surgery remain the most effective approach to reduce PJK incidence.
Complications
Complications of PJK/PJF
Direct Complications:
- Incidence
- 5-10% of PJF
- Management
- Urgent decompression
- Incidence
- 50-70% of PJF
- Management
- Revision surgery
- Incidence
- 30-50% of PJK
- Management
- Monitoring/revision
- Incidence
- Rare
- Management
- Revision if threatened
Complications of Revision Surgery
- Neurological injury (1-5%)
- Dural tear (5-10%)
- Wound infection (5-10%)
- Blood loss (significant)
- Recurrent PJK (20-30%)
- Pseudarthrosis (10-20%)
- Adjacent segment disease
- Chronic pain
Risk Factors for Recurrence
- Advanced age
- Poor bone quality
- Long fusion extent
- Over-correction of alignment
- Inadequate proximal extension
- Failure to address osteoporosis
- Poor soft tissue preservation
Recurrent PJK occurs in 20-30% of revision cases. This emphasizes the importance of prevention during primary surgery and addressing all modifiable risk factors at revision.
PJK has a mirror image at the bottom of the construct — distal junctional kyphosis (DJK) and distal junctional failure (DJF) at or below the lowest instrumented vertebra (LIV). It is the analogous problem of a rigid construct meeting mobile distal segments, and is most relevant when a long fusion stops in the lower lumbar spine rather than extending to the pelvis. The key preventive principle is LIV selection: a construct that must span the thoracolumbar and lumbar spine for adult deformity is generally extended to the pelvis (using S2-alar-iliac or iliac screws) rather than ending at L4, L5 or S1, because stopping short leaves a high lumbosacral stress riser prone to distal failure and L5-S1 pseudarthrosis. Sacropelvic fixation protects the distal junction but, as the meta-analyses show, simultaneously raises proximal junctional risk — so a long fusion to the pelvis must pair distal pelvic fixation with proximal junction protection above.
Postoperative Care and Rehabilitation
Early Postoperative Phase
- Mobilisation: early supervised mobilisation once the construct is judged stable; a thoracolumbosacral orthosis (TLSO) may be used for comfort, though high-level evidence for brace prevention of PJK is lacking
- Neurological monitoring: regular neurological observation, especially after revision for PJF or after deformity correction
- Pain control: multimodal analgesia; expect a settling period after revision extension
Bone Health Optimisation
Because low bone mineral density is an independent predictor of proximal junctional failure (Yagi et al., pmid 28902106), bone health is a core part of postoperative and perioperative care:
- DEXA assessment and treatment of osteoporosis (bisphosphonates or denosumab)
- Calcium and vitamin D repletion
- In elective primary surgery, consider deferring 3-6 months for anabolic or antiresorptive optimisation in severe osteoporosis
- Anabolic agents (e.g. teriparatide) are of particular interest where bone quality is the limiting factor, though their specific role in PJK prevention remains under study
Surveillance Protocol
- Imaging
- Standing long-cassette radiographs
- Purpose
- Baseline post-op alignment, detect early failure
- Imaging
- Standing radiographs
- Purpose
- Detect PJK/PJF during peak-risk window
- Imaging
- Standing radiographs
- Purpose
- Confirm stability, assess fusion
- Imaging
- Standing radiographs
- Purpose
- Long-term surveillance
The first 3-6 months are the peak-risk window for acute failure (mean time to acute PJF 11.4 weeks; Hostin et al., pmid 22986834), so surveillance should be most intensive early.
Counsel patients to avoid heavy lifting and high-impact loading in the early postoperative period, and to report new junctional pain, a palpable step or new neurological symptoms promptly, as these may herald proximal junctional failure.
Outcomes and Prognosis
Natural History
- Many cases remain stable
- Progression rate approximately 20-30%
- Symptomatic improvement possible in some
- Generally progressive
- Neurological risk if cord involvement
- Poor quality of life outcomes
Revision Surgery Outcomes
- PJA correction: 70-80%
- Global alignment improvement: 60-70%
- Fusion rate: 80-90%
- Pain improvement: 60-70%
- Functional improvement: 50-70%
- Patient satisfaction: 60-75%
- Reoperation rate: 20-30%
Prognosis Factors
- Younger age
- Good bone quality
- First revision
- Successful alignment correction
- No neurological deficit
- Multiple prior revisions
- Severe osteoporosis
- Persistent sagittal imbalance
- Neurological complications
- Medical comorbidities
The best management of PJK is prevention during primary surgery. Once established, revision surgery has significant morbidity and recurrence risk. Emphasis should be on proper patient selection, appropriate alignment targets, and addressing bone quality in the primary procedure.
Guidelines, Registries & Global Practice
Global Epidemiology
Adult spinal deformity surgery is increasing worldwide as populations age, and PJK is consistently the most common mechanical complication of long-segment fusion across health systems. Reported incidence is broadly consistent internationally: radiographic PJK occurs in roughly a quarter to a half of patients fused to the pelvis (26% in the original Glattes series, 45.1% in a 679-patient multicentre cohort), while acute proximal junctional failure occurs in around 5-6% within the first 6 months (Hostin et al.). Female sex, advanced age and osteoporosis are recurrent risk factors in cohorts from North America, Europe and Asia, and large meta-analyses pooling these international series confirm osteoporosis (OR 1.58) and pelvic fixation (OR 2.08) as drivers.
Society and Guideline Guidance
There is no single randomised-trial-based clinical practice guideline that dictates PJK prevention; guidance is largely consensus and registry-informed:
- Guidance / Output
- Standardised PJK/PJF definitions and outcome reporting; the SRS-Schwab classification underpins sagittal modifiers used in alignment planning
- Evidence base
- Expert consensus / observational
- Guidance / Output
- Multicentre deformity datasets and educational consensus on UIV selection, junctional protection and alignment targets
- Evidence base
- Observational cohorts, consensus
- Guidance / Output
- Source of much of the age-adjusted alignment and GAP-related evidence used globally
- Evidence base
- Prospective multicentre cohorts
- Guidance / Output
- No PJK-specific guideline; deformity surgery is delivered through specialist spinal networks with MDT governance
- Evidence base
- Service standards / consensus
- Guidance / Output
- DEXA screening and treatment thresholds inform preoperative bone optimisation
- Evidence base
- Guideline (osteoporosis)
Key practice principles with the strongest evidence are: individualised, age-adjusted alignment targets (avoid over-correction), proportional correction (GAP concept, acknowledging inconsistent external validation), proximal junction protection (ligamentous augmentation/hooks) and bone optimisation in osteoporotic patients.
Registry and Multicentre Evidence
Most high-quality PJK evidence comes from prospective multicentre deformity databases (e.g. the International Spine Study Group and European multicentre series) rather than national arthroplasty-style registries, because deformity volumes are comparatively low and constructs are heterogeneous. These collaboratives have produced the predictive models (Yagi), proportional scores (GAP) and age-adjusted target work that now guide practice globally. The lack of a dedicated high-volume PJK registry is itself a recognised gap.
Practice Variation
Practice varies internationally in the routine use of preventive adjuncts: prophylactic vertebroplasty/cement augmentation, transverse-process hooks and ligamentous "topping-off" devices are used selectively rather than universally, reflecting cost, availability and the absence of definitive randomised evidence. Thresholds for revising radiographic PJK also differ, with most centres reserving surgery for progressive deformity, intractable pain, instability or neurological compromise. Across health systems, complex deformity and PJK revision surgery is concentrated in tertiary specialist spine units with intraoperative neuromonitoring, advanced imaging and intensive care, with patients from regional or lower-resource settings typically transferred for complex revision.
MCQ Practice Points
Q: What is the radiographic definition of proximal junctional kyphosis?
A: PJK is defined as more than 10 degrees of kyphosis at the proximal junction angle (UIV inferior endplate to UIV+2 superior endplate) compared to immediate postoperative radiographs. This is the standard Glattes definition used in most literature.
Q: What distinguishes proximal junctional failure (PJF) from PJK?
A: PJF is defined as PJA more than 28 degrees OR change more than 22 degrees, associated with vertebral fracture, ligament failure, or implant failure. PJF typically requires revision surgery, while PJK may be observed if stable and asymptomatic.
Q: What is the reported incidence of PJK after adult spinal deformity surgery?
A: PJK occurs in 20-40% of patients after ASD surgery. The incidence is lower in adolescent idiopathic scoliosis (10-20%) and higher in ankylosing spondylitis (up to 50%) and revision surgery (30-50%).
Q: What are the major risk factors for developing PJK?
A: Major risk factors include: age more than 55 years, osteoporosis, fusion to sacrum/pelvis, upper thoracic UIV, over-correction of sagittal alignment, and combined anterior-posterior approach. Many of these can be addressed with prevention strategies.
Q: What is the role of cement augmentation in PJK prevention?
A: Prophylactic cement augmentation at UIV and UIV+1 reduces PJK risk in osteoporotic patients by improving screw purchase and reducing vertebral compression fracture risk. It is a cost-effective prevention strategy supported by Level II evidence.
At a Glance
Proximal junctional kyphosis (PJK) is defined as greater than 10° kyphosis at the upper instrumented vertebra (UIV) compared to preoperative alignment, occurring in 20-40% of adult spinal deformity surgeries. PJK must be distinguished from PJF (proximal junctional failure)—which includes vertebral fracture, ligament rupture, or implant failure at UIV and often requires revision (PJA greater than 28° or change greater than 22°). Risk factors include age over 60, osteoporosis, thoracic UIV, and critically over-correction of sagittal alignment. Most PJK occurs within 3-18 months postoperatively. Prevention strategies include age-adjusted alignment targets (avoid over-correction in elderly), cement augmentation at UIV and UIV+1 in osteoporotic bone, and soft tissue preservation at the proximal junction.
PJKPJK RISK - Risk Factor Mnemonic
Hook:PJK RISK factors predict who will develop proximal junctional complications
PREVENTPREVENT - PJK Prevention Strategies
Hook:PREVENT PJK by addressing modifiable risk factors
ABCDABCD - PJF Classification
Hook:ABCD of PJF - any of these elements defines failure requiring intervention
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman underwent T10-pelvis fusion for adult spinal deformity 8 months ago. She presents with new thoracic pain and difficulty standing upright. Radiographs show 22 degrees of kyphosis at T9-10 compared to immediate postoperative films where this was 5 degrees.”
“A 72-year-old man with ankylosing spondylitis underwent T4-pelvis fusion 6 months ago. He presents after a fall with severe back pain and new bilateral leg weakness (4/5 strength). Radiographs show 35 degrees of kyphosis at T3-4 with apparent fracture of T4 vertebral body.”
“You are planning T10-pelvis fusion for a 70-year-old woman with adult spinal deformity. Her DEXA shows T-score of -2.8 at the hip. PI is 60 degrees, current LL is 20 degrees. SVA is 10cm positive.”
Definitions
- PJK: PJA more than 10° compared to post-op (UIV to UIV+2)
- PJF: PJA more than 28° OR change more than 22° OR fracture/failure
- Incidence: 20-40% PJK, 1.4-5.6% PJF
- Peak occurrence: 3-18 months postoperatively
Risk Factors (PJK RISK)
- Poor bone quality - osteoporosis (T-score less than -2.5)
- Junctional level - upper thoracic UIV
- Kyphosis - baseline segmental kyphosis at UIV
- Rigid constructs - all pedicle screw systems
- Improper alignment - over-correction of sagittal balance
- Soft tissue destruction - disruption at UIV
Prevention (PREVENT)
- Pedicle screws with cement augmentation
- Rod flexibility - transition rods, cobalt chrome
- End point selection - avoid kyphotic segment
- Vertebroplasty at UIV prophylactic
- Elderly - age-adjusted targets
- No over-correction - accept more SVA in elderly
Management
- Stable PJK: Observation, serial imaging, conservative
- Progressive PJK: Consider revision
- PJF: Usually requires revision surgery
- Neurological deficit: Urgent surgical decompression
Revision Surgery
- Extend to stable horizontal vertebra (add 2-4 levels)
- Cement augmentation at new UIV and UIV+1
- Age-adjusted alignment targets
- Address osteoporosis - continue bone treatment
- Recurrence rate 20-30%
Evidence and Guidelines
Glattes - Original Description of PJK
- Defining study: PJK present when proximal junctional angle exceeds 10 degrees versus immediate postoperative film
- Incidence of PJK was 26% in 81 adult deformity patients with mean 5.3-year follow-up
- PJK was more common when the UIV was in the upper thoracic spine (T3)
- SRS-24 outcome scores were NOT significantly worse in patients with PJK, and the C7 sagittal plumb was not more positive
Hostin - Incidence, Mode and Location of Acute Proximal Junctional Failure
- Acute PJF occurred in 5.6% of 1218 consecutive ASD surgeries across 10 centres (mean age 63)
- Mean time to failure was 11.4 weeks, with all failures within 28 weeks
- Fracture was the commonest failure mode (47%), followed by soft-tissue failure (44%)
- 66% of failures were thoracolumbar (fracture predominant) and 34% upper thoracic (soft-tissue predominant)
Zhao - Meta-analysis of PJK Risk Factors and Preventive Devices
- Osteoporosis increased PJK risk (OR 1.58) and female sex increased risk (OR 1.56)
- Fusion to S1 or pelvis significantly increased PJK risk (OR 2.08)
- Ligament augmentation reduced PJK risk (OR 0.34), more effectively than laminar hooks (OR 0.46)
- Higher preoperative SVA and lower lumbar lordosis were associated with PJK
Yagi - Predictive Model for Proximal Junctional Failure (BMD)
- PJF defined as 20-degree or greater increase in proximal junctional angle with deterioration of an SRS-Schwab modifier, or any PJK needing revision
- PJF incidence was 20% in surgically treated ASD patients over 50 years
- Strongest predictors in order were pelvic tilt, bone mineral density, LIV at pelvis and lower-thoracic UIV
- Adding BMD to the predictive model improved accuracy
Lafage - Age-Adjusted Alignment Goals Reduce PJK
- Overall PJK incidence was 45.1% in 679 ASD patients fused to the pelvis
- PJK incidence rose with age: 17.9% (under 40), 43.8% (40-65), 50.2% (over 65)
- Patients who developed PJK were OVER-corrected relative to age-adjusted alignment targets (smaller PI-LL mismatch)
- Individualised, age-specific alignment targets reduce the risk of over-correction
Yilgor - GAP Score for Mechanical Complications
- The Global Alignment and Proportion (GAP) score uses pelvic-incidence-based proportional parameters plus an age factor
- A proportioned postoperative GAP state had a 6% mechanical complication rate versus 47% (moderately) and 95% (severely) disproportioned
- Mechanical complications include PJK/PJF, distal junctional failure and rod breakage
- AUC for predicting mechanical complications was 0.92 in the validation cohort
Kwan - External Validation of the GAP Score (Controversy)
- Independent external validation in the Scoli-RISK-1 cohort (159 patients)
- A higher GAP score was NOT associated with increased mechanical complications (AUC 0.60)
- GAP score alone did not predict revision for mechanical complications (AUC 0.66)
- Parameters beyond the original GAP score are needed to explain mechanical failure