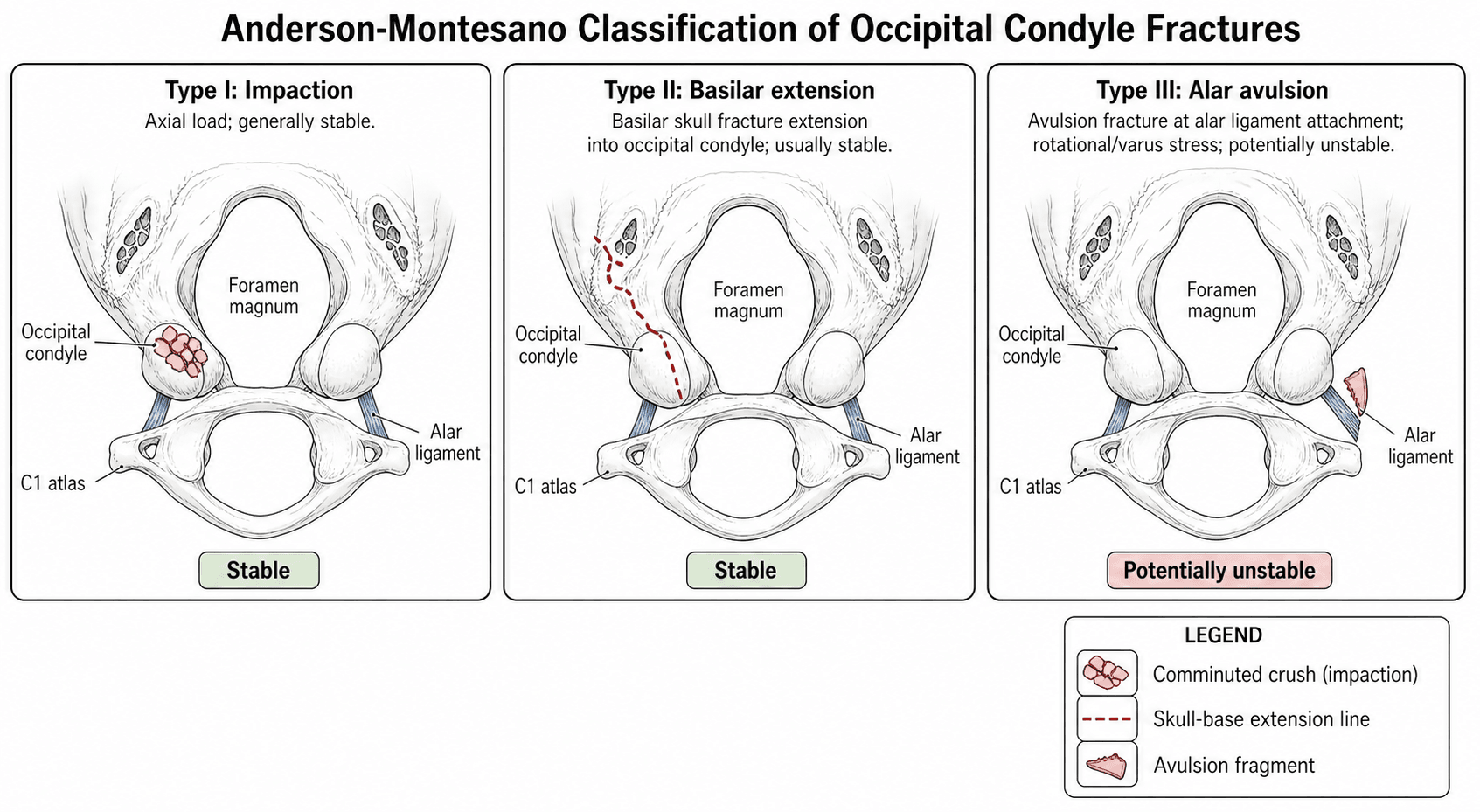
Anderson-Montesano Classification of Occipital Condyle Fractures
Know all three types and their mechanisms: Type I — impaction/comminution (axial load), Type II — basilar skull extension (direct blow), Type III — alar ligament avulsion (rotation/shear). Type III is the unstable one and the viva trigger. Always say you would order a CT with sagittal and coronal reformats — plain films are inadequate. State that you would assess for associated cranio-cervical injuries and lower cranial nerve deficits before focusing on the condyle alone.
Anatomy of the Occipital Condyles
The occipital condyles are paired oval articular surfaces on the anterolateral aspect of the foramen magnum. They articulate with the superior facets of the atlas (C1), forming the occiput-C1 (OC) joints.
Key anatomical relationships:
- Alar ligaments — paired, running from the dens tip to the medial aspect of each occipital condyle; resist excessive rotation and lateral flexion. An avulsion of the condylar insertion disrupts this checkrein.
- Tectorial membrane — the upward continuation of the posterior longitudinal ligament, attaching to the anterior foramen magnum; limits anterior translation of the occiput on the atlas.
- Cruciform ligament (transverse band) — the primary restraint of the dens, maintaining the C1-C2 articulation.
- Hypoglossal canal — traverses the condyle medially; fracture displacement can injure CN XII.
- Vertebral artery — ascends through the foramen transversarium of C1, curves posteromedially above the posterior arch of C1, and enters the foramen magnum just lateral to the condyle — at risk in displaced fractures.
Occipitocervical stability depends on the alar ligaments, tectorial membrane, and the OC joint capsules. A Type III condyle fracture disrupts the alar ligament insertion; if bilateral or accompanied by tectorial membrane disruption, gross instability ensues.
Plain radiographs (lateral cervical spine view) have very poor sensitivity for occipital condyle fractures because the condyles are obscured by overlapping mandible and skull-base structures. Up to half are only diagnosed on CT, and many are found incidentally during trauma-series CT of the head and cervical spine.


Anderson-Montesano Classification
Described by Anderson and Montesano in 1988, this is the most widely taught classification system for occipital condyle fractures. It divides them into three types based on morphology, mechanism, and implied stability.
- Type I — Impaction
- Axial compressive load (to vertex of skull)
- Type II — Basilar Extension
- Direct blow to skull base
- Type III — Avulsion
- Rotational or shear force with contralateral rotation
- Type I — Impaction
- Comminuted or impacted condyle fragment; minimal displacement
- Type II — Basilar Extension
- Basilar skull fracture line extending into the condyle
- Type III — Avulsion
- Small bony fragment avulsed from the medial condyle at the alar ligament insertion
- Type I — Impaction
- Ligaments intact
- Type II — Basilar Extension
- Ligaments intact
- Type III — Avulsion
- Alar ligament disrupted at condylar insertion
- Type I — Impaction
- Stable
- Type II — Basilar Extension
- Stable
- Type III — Avulsion
- Potentially unstable (unilateral may be stable; bilateral is highly unstable)
- Type I — Impaction
- Rigid cervical collar (6 to 12 weeks)
- Type II — Basilar Extension
- Rigid cervical collar; treat the basilar skull fracture
- Type III — Avulsion
- Halo vest if minimal displacement; occipitocervical fusion if significant instability or bilateral
- Type I — Impaction
- Good; heals reliably
- Type II — Basilar Extension
- Good; governed by associated TBI
- Type III — Avulsion
- Variable; depends on ligament healing and associated injuries
IBAAnderson-Montesano Types — IBA
Hook:I-B-A: Impaction is stable, Basilar extension is stable, Avulsion is the unstable one — Alar = Alert.
ALER (Alar = Alert)Stability rule — check the alar ligament
Hook:Alar = Alert: a Type III at the alar-ligament insertion means MRI before declaring stability; bilateral or torn tectorial membrane → fixation.
HALOAssociated injuries to name in the viva
Hook:Think HALO — it names the associations AND the halo vest you may need for an unstable condyle fracture.
In viva, if shown a CT with a small bony fleck at the medial aspect of the occipital condyle, think Type III avulsion first. Describe the fragment's location relative to the alar ligament insertion and state you would order an MRI to assess ligamentous integrity before declaring the injury stable.
Differential Classification Systems
Anderson-Montesano is the most commonly examined system, but examiners may ask about alternatives:
- Year
- 1988
- Basis
- Mechanism and morphology
- Types
- 3 types (I, II, III)
- Key Difference from Anderson-Montesano
- Most widely taught; emphasises stability via ligament assessment
- Year
- 1997
- Basis
- Displacement and ligament integrity
- Types
- Type 1 (undisplaced), Type 2A (displaced, stable), Type 2B (displaced, unstable)
- Key Difference from Anderson-Montesano
- Simplifies into displaced vs undisplaced; incorporates ligamentous assessment more directly
In practice, both systems lead to the same clinical question: is the cranio-cervical junction stable? The answer depends on alar ligament and tectorial membrane integrity, best assessed by MRI. The specific classification label matters less than the stability assessment.
Diagnosis and Imaging
Radiographic evaluation of suspected occipital condyle fractures:
- Role
- Very poor sensitivity; may show prevertebral soft-tissue widening or indirect signs only
- Limitations
- Condyles obscured by mandible and skull-base overlap; cannot rule out a fracture
- Role
- Gold standard for fracture detection and classification; sagittal and coronal reformats essential
- Limitations
- Does not directly visualise ligaments; cannot confirm stability in Type III
- Role
- Assesses alar ligaments, tectorial membrane, and transverse ligament integrity; detects oedema and haemorrhage
- Limitations
- Limited bony detail; not a first-line fracture-detection tool; difficult in unstable trauma patients
- Role
- May demonstrate dynamic instability in doubtful cases
- Limitations
- Contraindicated in the acute setting if the patient cannot be cleared clinically; risk of neurological deterioration
Never clear a cervical spine on plain radiographs alone when an occipital condyle fracture is clinically suspected (high-energy mechanism, lower cranial nerve signs, upper cervical pain). CT of the cervical spine with sagittal and coronal reformats is the minimum standard of care.
Key CT signs to describe in the viva:
- Fracture line orientation (sagittal, coronal, or comminuted)
- Fragment displacement (millimetres)
- Involvement of the hypoglossal canal
- Presence of a small medial fleck (hallmark of Type III avulsion)
- Associated C1 ring, odontoid, or foramen magnum involvement
- Soft-tissue swelling anterior to the condyle or at the cranio-cervical junction
Because a condyle fracture is a red flag for occipitocervical dissociation (atlanto-occipital dislocation, AOD), examiners expect the craniocervical-junction measurements you would make on the reconstructed CT (and MRI):
- Condyle–C1 interval (CCI) — the gap between the occipital condyle and the C1 superior facet; the most sensitive and specific CT sign of occipitocervical injury. A CCI over roughly 1.5 to 2 mm, or marked side-to-side asymmetry, is abnormal.
- Basion–dens interval (BDI) and basion–axial interval (BAI) — Harris's "rule of twelves": each should measure under about 12 mm, and a larger value suggests longitudinal or anteroposterior dissociation.
- Powers ratio — basion-to-posterior-arch divided by opisthion-to-anterior-arch; a ratio over 1.0 suggests anterior AOD (but it misses pure distraction and posterior dislocation).
- Wackenheim's clival line — a line drawn down the clivus should just touch the tip of the dens; displacement implies AOD.
Traynelis classifies AOD by the direction of occipital displacement: Type I anterior, Type II longitudinal (vertical distraction — the most unstable), and Type III posterior. Any AOD is a highly unstable, frequently fatal injury that mandates occipitocervical fusion, and traction is contraindicated in the distraction (Type II) pattern.
Management by Type
Type I — Impaction
- Stable injury; ligaments intact
- Rigid cervical orthosis (e.g., Aspen or Miami J collar) for 6 to 12 weeks
- Follow-up imaging at 6 weeks to confirm healing and maintenance of alignment
- Excellent prognosis; non-union is rare
- Return to activity guided by clinical comfort and radiographic union
Type II — Basilar Extension
- Stable as far as the OC joint is concerned; the clinical picture is dominated by the basilar skull fracture
- Cervical collar for protection during the acute phase
- Management directed at the basilar skull fracture: observe for CSF leak, hearing loss, facial nerve injury
- Neurosurgical consultation for intracranial involvement
- Prognosis determined by the severity of associated traumatic brain injury
Type III — Avulsion (Potentially Unstable)
This is the type that generates exam questions and clinical concern.
- Unilateral Type III with intact tectorial membrane: may be managed in a halo vest for 8 to 12 weeks, but only if close radiographic follow-up confirms no progressive displacement
- Bilateral Type III, or Type III with tectorial membrane disruption: grossly unstable — surgical occipitocervical fusion (O-C2 or O-C3) is indicated
- MRI is mandatory before deciding between halo and surgery — you must visualise the tectorial membrane and both alar ligaments
- Vertebral artery injury should be excluded with CTA or MRA in displaced fractures
- Lower cranial nerve function (gag, tongue protrusion, shoulder shrug, sternocleidomastoid strength) must be documented at presentation and monitored
When asked to manage a Type III fracture in the viva, always say: "I would obtain an MRI to assess ligamentous integrity, specifically the tectorial membrane and the contralateral alar ligament. If the tectorial membrane is intact and the injury is unilateral, I would consider a halo vest with close follow-up. If bilateral or the tectorial membrane is disrupted, I would recommend occipitocervical fusion."
Since the answer to an unstable bilateral Type III, or to any occipitocervical dissociation, is occipitocervical fusion, be ready to outline it:
- Construct: a midline occipital plate anchored into the thick bone of the external occipital protuberance/keel, connected by rods to C1 lateral-mass screws and C2 pedicle, pars or translaminar screws (a Goel–Harms-type segmental construct); older techniques used sublaminar wires with an onlay corticocancellous (iliac crest or rib) graft. The construct is extended to C3 if C1–C2 fixation is inadequate.
- Set the angle correctly: the occiput–C2 angle must be fixed in a neutral, slightly extended position. Fusing in excessive flexion narrows the oropharyngeal airway and causes dysphagia and even dyspnoea — a recognised and serious pitfall.
- Functional cost: the craniocervical junction provides roughly half of cervical rotation (at C1–C2) and a large share of flexion–extension (at the occiput–C1 joint), so fusion permanently sacrifices much of that motion — important to consent for.
- Complications: vertebral artery injury during C1/C2 screw placement, dural tear and CSF leak, dysphagia or airway compromise from malalignment, hardware failure or pseudarthrosis, and wound infection.
Guidelines, Registries and Global Practice
- Global epidemiology: Occipital condyle fractures are reported in approximately 3 to 5 percent of blunt cervical spine trauma patients screened by CT, though the true incidence is likely higher as many go undetected on plain films. Mortality is driven by associated traumatic brain injury rather than the condyle fracture itself.
- AO Spine: The AO Spine upper cervical injury classification system incorporates occipital condyle fractures within the occiput-C1 injury module, grading them by stability. Type III Anderson-Montesano injuries map to the unstable category, consistent with the need for surgical assessment. AO Spine recommends CT as the primary imaging modality and MRI for ligamentous evaluation when instability is suspected.
- NICE / BOA (UK): The 2022 NICE guideline (NG41 update) on trauma imaging recommends CT of the cervical spine (including the cranio-cervical junction) for all high-risk patients, which effectively mandates CT coverage of the occipital condyles. No specific treatment guideline exists for condyle fractures; management follows general cranio-cervical stability principles.
- Eastern Association for the Surgery of Trauma (EAST): EAST practice management guidelines recommend CT for cervical spine clearance in high-energy blunt trauma; they support MRI for ligamentous assessment before clearing the cervical spine in obtunded or unreliable patients, which would detect Type III injuries with ligament disruption.
- Global practice variation: Most major trauma centres worldwide now use CT-first protocols for cervical spine clearance, which has increased the detection rate of occipital condyle fractures. Management of Type III injuries varies between halo immobilisation (common in North America and parts of Europe) and early surgical occipitocervical fusion (preferred when MRI confirms gross ligamentous disruption or bilateral injury). Resource-limited settings may rely more on clinical assessment and plain radiographs, with a higher miss rate.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 38-year-old man is involved in a high-speed motor vehicle collision. He complains of severe upper neck pain and headache. A CT of the cervical spine shows a small bony fragment avulsed from the medial aspect of the right occipital condyle. The left condyle appears intact. How would you classify this injury and what is your management plan?”
“A 52-year-old woman falls from a horse and lands on her head. She has a Glasgow Coma Score of 14 and complains of severe occipital headache and neck pain. CT shows a comminuted fracture of the left occipital condyle without displacement and a non-displaced right C1 posterior arch fracture. There is no evidence of transverse ligament disruption. How would you manage this?”
The three types (I-B-A)
- Type I — Impaction: axial load, comminuted condyle, stable, treat in collar
- Type II — Basilar extension: skull-base fracture line reaches the condyle, stable, treat skull-base injury
- Type III — Avulsion: alar ligament pulls off a medial condylar fragment, potentially unstable, MRI mandatory
Imaging and diagnosis
- CT with thin cuts and sagittal/coronal reformats is the minimum; plain films miss most fractures
- MRI for ligamentous assessment in Type III (alar ligaments, tectorial membrane)
- CTA or MRA to exclude vertebral artery injury in displaced fractures
- Look for the medial fleck sign — pathognomonic for Type III avulsion
Management thresholds
- Types I and II: rigid cervical collar for 6 to 12 weeks
- Type III unilateral, tectorial membrane intact: consider halo vest with close follow-up
- Type III bilateral or with tectorial membrane disruption: occipitocervical fusion (O-C2 or O-C3)
- Always exclude associated injuries: TBI, C1/odontoid fracture, vertebral artery injury, cranial nerve IX through XII palsies
Viva safety nets
- Never declare stability without MRI in a Type III fracture
- Always name associated injuries (H-A-L-O: Head injury, Atlas/C1, Lower cranial nerves, Occipitocervical dissociation)
- If unsure about stability, err toward halo or surgical fixation — the consequences of undertreating cranio-cervical instability are catastrophic
Evidence Base
Every citation below has been checked against its source record in PubMed. Anderson-Montesano (1988) and Tuli (1997) created the two classifications; Hanson (2002) is the large CT series showing inferomedial avulsions are the commonest type and that plain films miss many injuries; and — importantly — Maserati (2009) argues that classification adds little and that craniocervical MISALIGNMENT on reconstructed CT is the decisive criterion for surgery. Musbahi (2018) is the systematic review confirming the evidence base is low-level overall.
Morphology and treatment of occipital condyle fractures
- Six cases from the authors plus a literature review of 20 reported fractures; defined the three-type classification by morphology and mechanism
- Type I (impaction) and Type II (basilar extension) were considered stable and treated in a semiconstrained orthosis; Type III (alar avulsion) potentially unstable and treated with rigid immobilisation
- The single death occurred in a patient with a displaced Type III avulsion, underscoring the instability risk of that subtype
Occipital condyle fractures
- Proposed an alternative classification by displacement and ligamentous stability: Type 1 undisplaced (stable), Type 2A displaced without ligamentous instability (stable), Type 2B displaced with ligamentous instability (unstable)
- Plain cervical radiographs were normal in 96% of reported cases, so CT of O-C2 is needed when there are lower cranial nerve deficits, head/basal skull injury, or persistent neck pain
- Across the literature, cranial nerve deficits occurred in 31% of patients and were delayed in 38% of those
Radiologic and clinical spectrum of occipital condyle fractures: retrospective review of 107 consecutive fractures in 95 patients
- Large CT series (107 fractures in 95 patients): inferomedial avulsions (Anderson-Montesano Type III) were the commonest type at 80/107 (75%)
- Most unilateral fractures were treated non-operatively; occipitocervical fusion or halo was needed mainly for bilateral occipito-atlanto-axial joint disruption (often with normal plain radiographs)
- Associated cervical spine injuries were present in 31% — occipital condyle fractures are markers of high-energy trauma