Infection of the Intervertebral Disc and Adjacent Vertebral Bodies
- Back pain + CRP elevation = Discitis until proven otherwise.
- MRI with Gadolinium is the Gold Standard for diagnosis.
- Do NOT start antibiotics before biopsy unless the patient is septic or has neurological compromise.
- Biopsy yield is only ~50-70%. Negative biopsy may require open biopsy.
- Treatment duration is typically 6 weeks minimum.
- “Batson's Venous Plexus is valveless - allows retrograde spread from pelvis/UTI.
- “The disc is avascular in adults - infection starts in the vertebral endplate.
- “IVDU patients are prone to Pseudomonas (Gram Negative).
- “Epidural Abscess is the most feared complication (Cord Compression).
Overview and Epidemiology
Pathophysiology In adults, the intervertebral disc is avascular. Bacteria lodge in the end-arterioles of the vertebral metaphysis (endplate). The infection sets up an osteomyelitis, then breaks through the endplate into the disc, rapidly destroying it (proteolytic enzymes). From the disc, it spreads to the adjacent vertebra.
Spread
- Hematogenous (Arterial): Nutrient arteries.
- Hematogenous (Venous): Batson's Plexus (valveless venous system connecting pelvis/bladder to spine). Explains UTI link.
Epidemiology
- Bimodal distribution (under 20yo and over 50yo).
- Lumbar is more common than thoracic, which is more common than cervical.
- Note: TB spine prefers the thoracic region.
Pathophysiology and Mechanisms
The Intervertebral Disc
- Adult: Avascular. Nutrition via diffusion from endplates.
- Child: Vascular channels persist (explains direct discitis in children).
The Endplate
- The "Metaphysis" of the spine.
- Rich vascular loop system (slow flow) → Predisposes to bacterial lodging.
Venous Anatomy (Batson's Plexus)
- A valveless system of vertebral veins.
- Connections: It communicates freely with the pelvic, abdominal, and thoracic venous systems.
- Mechanism: Increases in intra-abdominal or intra-thoracic pressure (e.g., coughing, straining, lifting) can reverse blood flow.
- Clinical Relevance: This retrograde flow allows bacteria from the pelvis (UTI, Prostatitis) or abdomen to bypass the liver/lung filters and lodge directly in the spine.
- This explains the strong association between Urinary Tract Infections and Vertebral Osteomyelitis.
Biomechanics
- Infection weakens the anterior column (body/disc).
- Leads to Kyphosis (Gibbus deformity).
- If greater than 50% body destruction → Mechanical Instability.
Childhood Discitis: A Distinct, More Benign Entity
The pathophysiology above notes that vascular channels persist across the child's endplate ("explains direct discitis in children") and the epidemiology is bimodal with a peak under 20 years — but paediatric discitis behaves so differently from adult vertebral osteomyelitis that it deserves separate treatment.
Why it differs
- In young children the disc still has a direct vascular supply, so infection (or a low-grade inflammatory process) can settle in the disc itself rather than starting in the endplate as it does in adults. It is usually a single lumbar level (commonly L3-4 or L4-5), low-virulence, and frequently culture- and even blood-culture-negative.
How it presents
- The classic picture is a young child (often 1 to 5 years) who refuses to walk, sit or bear weight, or who is irritable with back/abdominal/hip pain, rather than the toxic septic adult. Fever and inflammatory markers are often only mildly raised; loss of normal lumbar lordosis and reluctance to flex the spine are typical.
How it is managed (much less aggressively)
- It is largely a clinical/MRI diagnosis; routine biopsy is not required in the typical case. Management is usually immobilisation/rest and a course of anti-staphylococcal antibiotics, with the threshold for biopsy reserved for atypical, non-responding or destructive disease.
- The prognosis is good — most children recover fully, in contrast to the high residual-morbidity, deformity and mortality figures quoted for adult pyogenic vertebral osteomyelitis.
Paediatric discitis is not a small version of adult spondylodiscitis: the child's disc is still vascular, so it is a single-level, low-virulence, often culture-negative process in a toddler who refuses to walk or sit. It is usually treated with rest and anti-staphylococcal antibiotics without biopsy, and the outcome is good — a deliberately less aggressive pathway than the biopsy-driven adult algorithm.
Classification Systems
Pola Classification (Eur Spine J 2017) A treatment-oriented system based on bone, epidural and neurological involvement.
- Type A: Bone or disc involvement without instability, epidural abscess or neurology. Subtypes A1 to A4. (Conservative).
- Type B: Epidural abscess without neurological deficit. Subtypes B1 (no instability) and B2 (with instability). (Conservative or surgery).
- Type C: Neurological deficit, with or without instability/abscess. Subtypes C1 to C4. (Surgery).
Clinical Assessment
History
- Pain: Constant, non-mechanical (night pain), progressively worsening.
- Constitutional: Fever, rigors, weight loss (often absent).
- Neurology: Weakness/Numbness (Epidural abscess).
Examination
- Tenderness: Percussion tenderness is highly sensitive.
- Spasm: Paravertebral muscle spasm ("Board-like").
- Neurology: Detailed myotomal/dermatomal exam.
Imaging and Investigations
Workup Protocol
- ESR/CRP: Elevated in over 90%. Used to monitor response.
- WCC: Often normal!
- Blood Cultures: Positive in ~50%. If positive, may avoid biopsy.
- T1: Hypointense (Dark) disc and endplates.
- T2: Hyperintense (Bright) "Fluid in the disc".
- T1+Gad: Enhancement of disc/endplates/abscess.
- "Hot Disc Sign": Highly specific.

Workup Protocol (continued)
- CT Guided: Standard of care.
- Yield: Only 50-70%.
- Must hold antibiotics for 48-72hrs prior if safe.
MRI Pitfall: Infection versus Degenerative (Modic) Endplate Change
MRI is the gold standard here, and the post-op follow-up note already warns that "post-op changes mimic infection" — so the commonest false positive deserves to be explicit: degenerative Modic type 1 endplate change produces endplate marrow oedema that looks like early infection (T1 dark, T2/STIR bright), and distinguishing the two is a classic examiner trap.
- Infection (spondylodiscitis)
- Bright (high signal), with loss of the normal intranuclear cleft
- Degenerative (Modic type 1)
- Dark (low signal) - a degenerate, desiccated disc
- Infection (spondylodiscitis)
- Eroded, irregular, destroyed
- Degenerative (Modic type 1)
- Intact, preserved cortical line
- Infection (spondylodiscitis)
- Disc, endplate and paravertebral/epidural enhancement, often with abscess
- Degenerative (Modic type 1)
- Little or no abnormal disc/soft-tissue enhancement
- Infection (spondylodiscitis)
- Phlegmon or abscess present
- Degenerative (Modic type 1)
- Absent
The single most useful discriminator is the disc itself: a T2-bright disc with endplate destruction and paradiscal/epidural enhancement points to infection, whereas a T2-dark degenerate disc with intact endplates and no soft-tissue enhancement is Modic type 1 degeneration.
Endplate oedema (T1 dark / T2 bright) is shared by early infection AND degenerative Modic type 1 change. Separate them by the disc and the soft tissues: infection gives a bright T2 disc, eroded endplates and enhancing paradiscal/epidural tissue (abscess); Modic type 1 gives a dark degenerate disc, intact endplates and no soft-tissue enhancement. The same caveat explains why a routine post-operative MRI mimics infection.
Management Algorithm
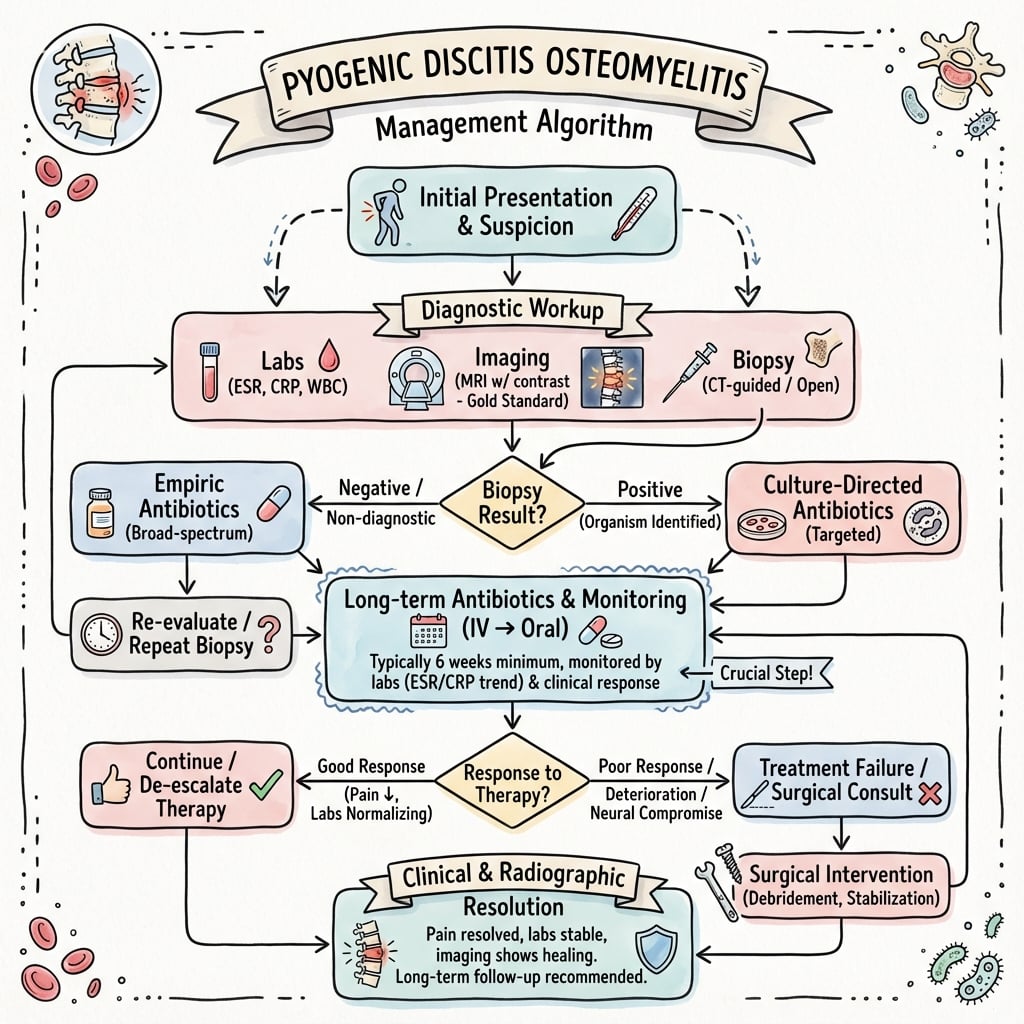
- 1
Suspected Discitis (Pain + CRP)
- 2
Neuro Deficit or Sepsis?
- 3
Biopsy Positive?
Treatment Protocols
Antimicrobial Therapy
- Empiric: Vancomycin + Ceftriaxone (coverage for MRSA and Gram Negatives).
- Targeted: Narrow spectrum based on sensitivities.
- Duration: Traditionally 6 weeks IV. Modern evidence (OVIVA Trial) suggests Oral is non-inferior if bioavailable.
Bracing
- TLSO: Often used for pain control and to prevent deformity (kyphosis).
- Worn for 6-12 weeks while bone heals.
Surgical Technique
Decompression (Laminectomy)
- Indication: Epidural Abscess with cord/cauda equina compression.
- Technique:
- Midline approach.
- Laminectomy (wide).
- Drainage of abscess (often minimal 'pus', mostly granulation tissue).
- Do NOT destabilize the facets if possible.
- Pitfall: Laminectomy alone in a destroyed spine causes rapid kyphosis. Must instrument if unstable.
Complications
- Risk
- 15-20%
- Note
- Can cause rapid onset paraplegia.
- Risk
- 10%
- Note
- Infection inhibits fusion.
- Risk
- Common
- Note
- Collapse of disc and endplates.
- Risk
- 1-5%
- Note
- Always auscultate the heart (Echo if murmur).
Postoperative Rehab
Antibiotics
- Continue for 6 weeks minimum.
- Stop when CRP normalizes and radiographic healing seen.
Follow-up
- Weekly CRP.
- X-rays at 6 weeks/3 months to check fusion/alignment.
- MRI only if symptoms worsen (post-op changes mimic infection).
Outcomes and Prognosis
Mortality
- High (2-20%) depending on comorbidities (Age, Diabetes).
- Higher in MRSA infections.
Recurrence
- 5-10%.
- Risk factors: Inadequate duration of Abx, Undrained abscess, Retained hardware (if loose).
Functional Outcome
- Majority (greater than 70%) have significant residual back pain.
- Functional impairment is worse than standard degenerative spine surgery.
Long-term Sequelae
- Chronic Pain: Due to facet joint destruction and altered biomechanics (kyphosis).
- Instability: Degenerative spondylolisthesis may develop years later above or below the fused level (Adjacent Segment Disease).
- Quality of Life: Studies (e.g., Carragee et al.) show scores similar to chronic heart failure.
Prognostic Factors (Poor Outcome)
- Age greater than 60.
- Concurrent Endocarditis.
- Disseminated S. aureus infection.
- Delay in diagnosis (greater than 3 months).
- Presence of neurological deficit at presentation (often permanent).
Guidelines, Registries & Global Practice
Global epidemiology
- Incidence is rising worldwide (ageing populations, IV drug use, more spinal instrumentation and intravascular devices). Reported population incidence is roughly 1 to 7 per 100,000 person-years in high-income settings.
- Strong male predominance and a peak in patients over 50 years. Staphylococcus aureus is the dominant pathogen globally; Gram-negative organisms cluster with urinary sources and IV drug use.
- In TB-endemic regions (much of South Asia, sub-Saharan Africa), Mycobacterium tuberculosis (Pott disease) is a major differential and may outnumber pyogenic cases; Brucella spondylitis is important around the Mediterranean, Middle East and Central Asia.
- Diagnosis emphasis
- MRI + blood cultures; image-guided biopsy if cultures negative
- Antibiotic strategy
- Hold empirical Abx if stable; about 6 weeks total
- Diagnosis emphasis
- MRI gold standard; emphasise culture before therapy
- Antibiotic strategy
- Targeted therapy, oral switch supported by OVIVA
- Diagnosis emphasis
- Classify by neurology, instability, abscess (Pola)
- Antibiotic strategy
- Surgery for deficit, instability, sepsis, failed medical Tx
Registry and practice variation
- No dedicated international spondylodiscitis registry exists; arthroplasty/implant registries (NJR, AJRR, AOANJRR, SHAR) inform biofilm and revision principles that carry over to instrumented spinal infection.
- High-resource settings: routine MRI, CT-guided biopsy, prolonged targeted therapy, single-stage instrumented debridement, OPAT or early oral switch.
- Limited-resource settings: empirical therapy is often started before biopsy due to limited imaging/microbiology; high TB prevalence lowers the threshold for empirical anti-tuberculous treatment; surgical capacity for instrumented reconstruction may be constrained.
Controversies & Areas of Uncertainty
- Empirical antibiotics before biopsy: Guidelines advise holding antibiotics in stable patients to maximise culture yield, yet real-world practice often starts therapy early. The optimal antibiotic-free window before biopsy (commonly quoted as 48 to 72 hours) is not firmly evidence-based.
- Total duration: The Bernard RCT supports 6 weeks for uncomplicated disease, but undrained abscess, implant-associated infection, endocarditis or persistently raised CRP frequently prompt longer courses; the right duration for these subgroups is unresolved.
- Oral versus IV: OVIVA supports early oral switch, but uptake varies and selection of a reliably bioavailable oral agent (and adherence) remains the practical limitation.
- Single-stage instrumentation in active infection: Increasingly accepted with radical debridement, but the threshold for instrumenting, choice of anterior versus posterior approach, and use of titanium versus PEEK cages are debated.
- Role of nuclear imaging: FDG-PET/CT is useful when MRI is contraindicated or equivocal and for monitoring, but is not universally available and its role in defining cure is not standardised.
Mnemonics
DISCITISRisk Factors
Hook:Who gets infected?
SEC POrganisms
Hook:Common bugs.
BIOPSYManagement
Hook:Workflow.
MCQ Practice Points
Q: What is the earliest MRI sign of discitis? A: Endplate Edema. High signal on T2/STIR in the subchondral bone.
Q: Why does infection start in the endplate, not the disc? A: Vascular Supply. The adult disc is avascular. Bacteria lodge in the vascular loops of the endplate.
Q: Most common organism in IV Drug Users? A: Pseudomonas aeruginosa. (Though S. aureus is still common).
Q: What clinical sign suggests an Epidural Abscess? A: Neurological Deficit or severe radicular pain.
Q: What is the primary indication for surgery in discitis? A: Neurological Deficit. Failure of medical management and instability are secondary.
At a Glance
- Pyogenic
- Destroyed Early
- Tuberculosis (Pott's)
- Preserved Late
- Pyogenic
- Usually 2 (contiguous)
- Tuberculosis (Pott's)
- Multiple (skip lesions)
- Pyogenic
- Small / Epidural
- Tuberculosis (Pott's)
- Large / Psoas (Cold Abscess)
- Pyogenic
- Less Common
- Tuberculosis (Pott's)
- Common (Gibbus)
Exam Day Cheat Sheet
Key Facts
- S. aureus #1
- MRI is Gold Standard
- Biopsy BEFORE Abx
- 6 weeks Tx
Red Flags
- Neuro Deficit (Abscess)
- Sepsis (Systemic)
- IVDU (Pseudomonas)
- Endocarditis
Workup
- Blood Cx x3
- MRI Gadolinium
- CT Biopsy
- Echo
Risks
- Paralysis
- Sepsis
- Deformity (Kyphosis)
- Chronic Pain
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“60M with L4/5 Discitis. Blood Cx neg. CT Biopsy neg. CRP 150. Stable Neuro. What now?”
“You need to stabilize an L3/4 infection. Is it safe to put Titanium screws into pus?”
“A 45-year-old from a TB-endemic region presents with 3 months of thoracic back pain, night sweats and a large left psoas collection. How do you distinguish pyogenic from tuberculous spondylodiscitis, and how does it change management?”
Evidence Base
OVIVA Trial
- Oral vs intravenous antibiotics for bone and joint infection; 1054 adults across 26 UK centres.
- Treatment failure at 1 year: 13.2% oral vs 14.6% IV (difference -1.4 points, within the 7.5-point non-inferiority margin).
- Oral therapy was NON-INFERIOR to IV therapy.
- Catheter complications were more common with IV (9.4% vs 1.0%).
Duration of Therapy
- Open-label non-inferiority RCT, 351 patients analysed, 6 weeks vs 12 weeks of antibiotics.
- Clinical cure at 1 year identical at 90.9% in both arms (difference 0.05%, 95% CI -6.2 to 6.3).
- 6 weeks was non-inferior for microbiologically confirmed pyogenic vertebral osteomyelitis.
- Shorter course reduces antibiotic burden and resistance pressure.
Image-Guided Biopsy Yield
- Systematic review and meta-analysis of 7 studies (482 patients) of image-guided spinal biopsy.
- Pooled sensitivity only 52.2% (95% CI 45.8-58.5) but specificity 99.9%.
- A positive biopsy strongly confirms infection, but a negative result does NOT rule it out.
- Diagnostic odds ratio 45.5; supports biopsy in the work-up of suspected native vertebral osteomyelitis.
Instrumentation in Spinal Infection
- 11 patients with spinal tuberculosis treated by debridement, anterior fusion and posterior instrumentation.
- No persistence or recurrence of infection after surgery; instrumentation gave immediate stability and prevented kyphosis.
- In vitro adherence of M. tuberculosis to stainless steel was low.
- Concluded posterior instrumentation is not a hazard when combined with radical debridement and chemotherapy.
Spinal Epidural Abscess
- Authoritative review establishing spinal epidural abscess (SEA) as a neurosurgical emergency.
- The classic triad of fever, back pain and neurological deficit is present in a minority of patients.
- MRI with gadolinium is mandatory for any back pain plus fever or new neurology.
- Early decompression and drainage improve neurological recovery; deficit duration predicts outcome.
IDSA Native Vertebral Osteomyelitis Guideline
- Obtain blood cultures and ESR/CRP in all suspected cases; MRI is the imaging of choice.
- Image-guided biopsy is recommended when blood cultures are negative and the patient is haemodynamically stable.
- Withhold empirical antibiotics in stable patients until a microbiological diagnosis is secured.
- Recommend approximately 6 weeks of antimicrobial therapy for most pyogenic cases, monitoring ESR/CRP.