Quadriceps Strain - Distal vs Proximal Intrasubstance
- RECTUS FEMORIS STRAIN is a common quadriceps muscle injury; the rectus femoris is the only quadriceps muscle crossing BOTH the HIP and the KNEE (a two-joint muscle), which makes it especially prone to ECCENTRIC STRAIN during KICKING and SPRINTING (and to proximal apophyseal avulsion of the anterior inferior iliac spine in adolescents).
- The 'CLASSIC' rectus femoris strain occurs at the DISTAL muscle-tendon junction of the quadriceps tendon (in the distal thigh) - a typical muscle strain presentation with acute pain, swelling/bruising and weakness on resisted knee extension/hip flexion.
- A distinct and characteristic pattern is an INCOMPLETE INTRASUBSTANCE tear at the muscle-tendon junction formed by the INDIRECT (deep) head's INTRAMUSCULAR TENDON; these injuries lie MORE PROXIMALLY in the thigh than the classic distal strain, and present with CHRONIC thigh pain and an anterior-thigh MASS.
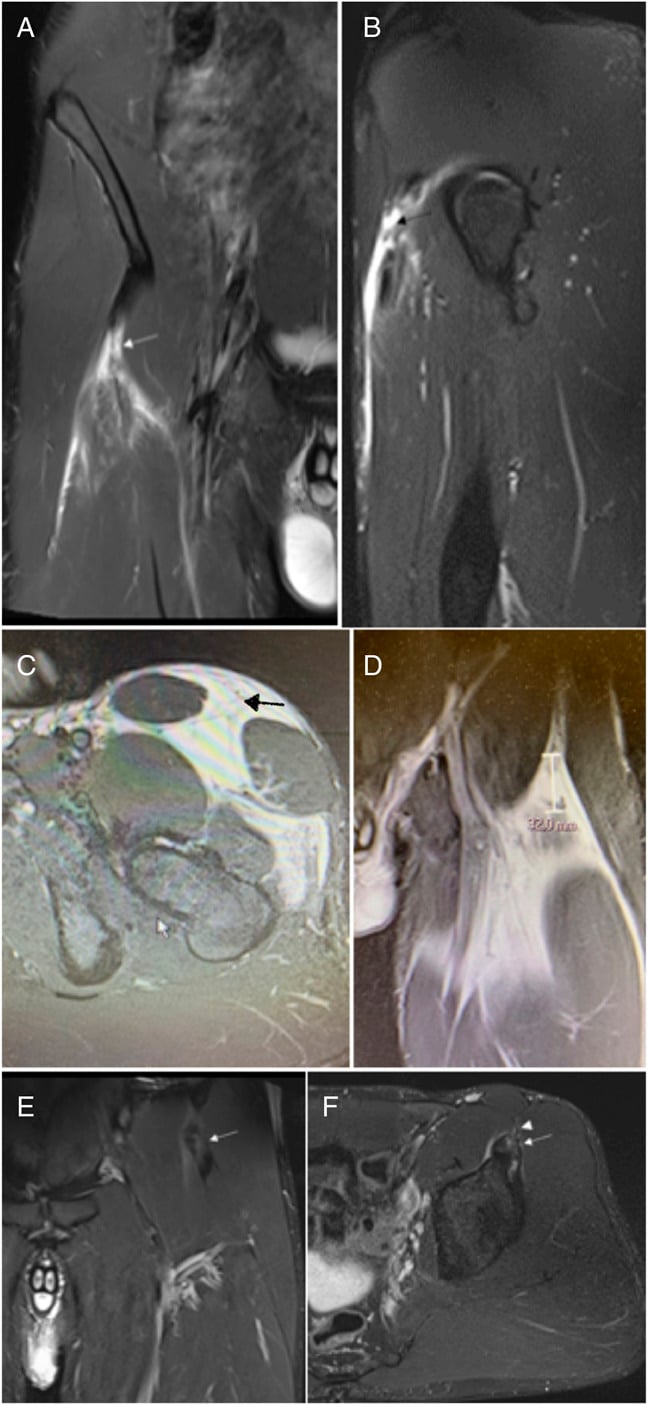
- The clinically important point about the proximal intrasubstance tear is that the resulting MASS (a fibrous scar with fatty tissue encasing the deep tendon) can MIMIC a SOFT-TISSUE NEOPLASM - so it must be distinguished from a tumour, with MRI showing abnormal signal centred on the intramuscular tendon of the indirect head (rather than the features of a sarcoma).
- DIAGNOSIS is clinical (mechanism, site of pain/tenderness, an anterior-thigh mass in the intrasubstance type) supported by MRI (or CT), which characterises the strain/tear, localises it (distal vs proximal/indirect-head), and crucially distinguishes the intrasubstance tear-mass from a soft-tissue tumour.
- MANAGEMENT is PREDOMINANTLY NON-OPERATIVE - relative rest, analgesia, a graded rehabilitation programme and return to sport - for most strains; SURGERY is reserved for selected cases (e.g. a symptomatic proximal intrasubstance mass), and correct diagnosis (excluding tumour) precedes any intervention. Quote the evidence honestly: the claim that excision is curative rests on 2 operated patients within a 10-athlete series from 1995, with no control group and no stated follow-up.
- KNOW THE RETURN-TO-TRAINING NUMBERS. In 38 rectus femoris injuries in 27 elite track-and-field athletes, rehabilitation-managed injuries returned to full training at a mean of 20.4 days (SD 14.8) - the spread is nearly as wide as the mean, so avoid promising 'about three weeks'. Grade 1 returned faster than grades 2 and 3, and INTRATENDINOUS (c) and surgically managed injuries returned significantly LATER than all other classes.
- BE PRECISE ABOUT RECURRENCE - a common exam error. The rule that intratendinous 'c' injuries re-tear more is from the elite HAMSTRING data. In the rectus-femoris-specific series, myofascial (a) injuries re-injured least, but the increased repeat-injury rate attached to GRADE 3, not to c. So in the rectus femoris: c predicts a SLOWER RETURN; grade 3 predicts RECURRENCE.
- “Rectus femoris = only quadriceps muscle crossing BOTH hip and knee (two-joint) -> prone to eccentric strain in kicking/sprinting (and AIIS apophyseal avulsion in adolescents).
- “Two patterns: typical DISTAL muscle-tendon-junction strain; and the characteristic PROXIMAL INTRASUBSTANCE tear of the INDIRECT (deep) head's intramuscular tendon - which forms an anterior-thigh MASS that can MIMIC a tumour.
- “MRI characterises and distinguishes the intrasubstance tear-mass from a soft-tissue NEOPLASM. Management predominantly NON-OPERATIVE (rest/rehab/graded return); surgery for selected cases (symptomatic proximal mass) - though 'excision is curative' rests on just 2 operated patients from 1995.
- “NUMBERS: mean return to full training 20.4 days (SD 14.8) in elite athletes; c-class and surgical cases return LATER; but the higher REPEAT-injury rate attached to GRADE 3, not c - 'c re-tears more' is the hamstring finding.
Kicking/sprinting athlete with thigh pain. Distal strain (muscle-tendon junction) vs the proximal intrasubstance tear of the indirect-head tendon -> chronic pain + an anterior-thigh mass.
The proximal intrasubstance mass (fibrous scar) can mimic a soft-tissue tumour - MRI distinguishes it (signal centred on the indirect-head intramuscular tendon).
Proximal Anatomy: Two Heads and the Central Tendon
- Two proximal origins. The rectus femoris arises by two heads: the direct (straight) head from the anterior inferior iliac spine (AIIS), and the reflected (indirect) head from the groove above the acetabulum (supra-acetabular ridge) and the hip-joint capsule. (The direct head's AIIS apophysis is the one that avulses in adolescents.)
- The central (intramuscular) tendon. The reflected/indirect head's tendon does not simply end proximally - it continues distally as a long intramuscular "central tendon" running within the muscle belly, which is bipennate around it. This deep intramuscular tendon and the fibres arising from it are the site of the proximal intrasubstance tear - the muscle-tendon junction is effectively inside the muscle, not at its ends, which is why this tear is intrasubstance and forms a proximal mass.
- Distal insertion. Distally the rectus femoris joins the vastus medialis, lateralis and intermedius to form the quadriceps tendon, which inserts via the patella and patellar tendon onto the tibial tubercle - so the muscle crosses both the hip and the knee.
Q: Describe the proximal anatomy of the rectus femoris and why it produces an intrasubstance tear.
A: It has two origins - a direct (straight) head from the AIIS and a reflected (indirect) head from the supra-acetabular ridge and hip capsule. The indirect head's tendon continues distally as a long intramuscular "central tendon" within the (bipennate) muscle belly, so the muscle-tendon junction is inside the muscle - a strain there is an intrasubstance tear forming a proximal thigh mass, rather than the classic distal muscle-tendon-junction strain. Distally the four quads form the quadriceps tendon to the tibial tubercle, crossing both hip and knee.
Patterns, Diagnosis & Management
The rectus femoris is the only quadriceps muscle crossing both the hip and knee, so it is prone to eccentric strain in kicking/sprinting. The classic strain is at the distal muscle-tendon junction; the characteristic alternative is a proximal intrasubstance tear of the indirect (deep) head's intramuscular tendon, which presents with chronic thigh pain and an anterior-thigh mass (fibrous scar) that can mimic a soft-tissue tumour. MRI characterises and localises the injury and distinguishes the intrasubstance tear-mass from a neoplasm. Management is predominantly non-operative (rest, rehabilitation, graded return), with surgery in selected cases (e.g. a symptomatic proximal mass) - after the diagnosis (excluding tumour) is secure.
The key safety point in rectus femoris injury is the proximal intrasubstance tear. Unlike the classic distal muscle-tendon-junction strain, the intrasubstance tear of the indirect (deep) head's intramuscular tendon lies more proximally in the thigh and produces a firm anterior-thigh mass of fibrous scar and fatty tissue encasing the deep tendon, which presents with chronic thigh pain and a palpable mass - and can closely mimic a soft-tissue tumour. The error to avoid is at both ends: treating an undiagnosed thigh mass as a simple muscle injury when it is in fact a sarcoma, and conversely subjecting a benign post-strain fibrous mass to inappropriate oncological work-up or excision. MRI is decisive: in the intrasubstance tear it shows abnormal signal centred on the intramuscular tendon of the indirect head, distinct from the features of a neoplasm. Most rectus femoris strains are managed non-operatively with rest, rehabilitation and graded return; surgery is reserved for selected cases, such as a symptomatic proximal intrasubstance mass, where removing the fibrous mass can be curative - always after the diagnosis is confirmed and a tumour excluded.
Grading and Why the Central-Tendon Injury Behaves Worse
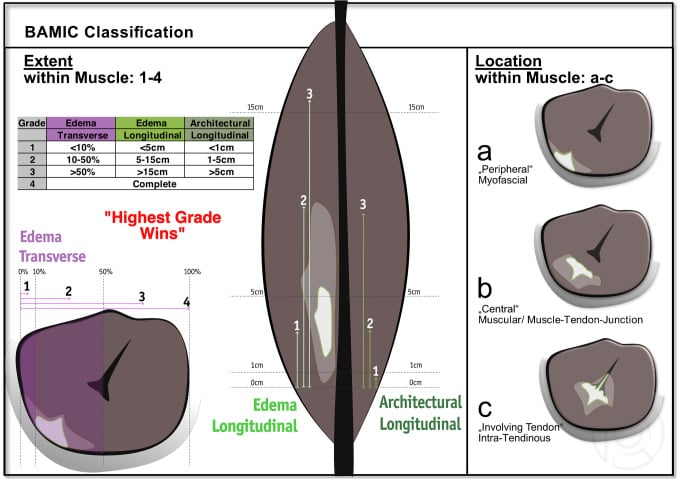
- Grading. Muscle strains are traditionally graded I-III: Grade I (minor fibre disruption, minimal strength loss), Grade II (partial tear, definite weakness/pain), Grade III (complete tear/rupture). The modern British Athletics Muscle Injury Classification (BAMIC) grades 0-4 by MRI extent and adds a site letter - a (myofascial), b (musculotendinous/muscle belly) or c (intratendinous, involving the tendon itself).
- The numbers, from the only rectus-femoris-specific BAMIC study. In 38 rectus femoris injuries among 27 elite track-and-field athletes followed over nine years, the average time to return to full training for rehabilitation-managed injuries was 20.4 days (SD 14.8) - note the standard deviation is nearly as large as the mean, so quoting "about three weeks" to an athlete conceals a range from a few days to well over a month. Grade 1 injuries returned significantly faster than grade 2 or grade 3.
- Intratendinous ("c") injuries return LATER - that much is confirmed in rectus femoris. Both c-class and surgically managed injuries had significantly longer times to return to full training than all other classes, plausibly reflecting the longer healing and remodelling time tendon requires.
- But be precise about re-injury - the page-level shorthand is borrowed from the hamstring. The familiar teaching that "c injuries re-tear more" comes from elite hamstring data, where intratendinous injury carried a significantly higher recurrence. In the rectus femoris series the pattern was not identical: myofascial (a) injuries had a reduced repeat-injury rate compared with b or c, but the class that stood out for increased repeat injury was grade 3, not c specifically. So in rectus femoris, say that c predicts a slower return and grade 3 predicts recurrence, and flag the c-recurrence link as extrapolated from hamstring evidence.
- A pattern worth knowing. All four complete (4c) proximal free-tendon injuries in that series occurred during sprinting and all four were in female athletes. With only four events this is an observation, not a demonstrated sex difference, and it must not be quoted as a risk factor.
- Return to sport. Graded rehabilitation (progressive eccentric loading, then sport-specific drills) with return guided by pain-free strength and function rather than time alone. No validated return-to-play criteria, functional test battery or discharge threshold specific to rectus femoris has been published - the timings above are observed averages from one elite cohort, not targets.
Q: How are rectus femoris strains graded, and why does the intrasubstance (central-tendon) tear behave worse?
A: Traditionally Grade I-III (minor fibre disruption / partial tear / complete rupture); the modern BAMIC grades 0-4 by MRI extent with a site letter - a (myofascial), b (musculotendinous) or c (intratendinous). The proximal intrasubstance tear involves the intramuscular central tendon - a "c" / intratendinous injury. In the only rectus-femoris-specific series (38 injuries, 27 elite athletes), rehabilitation-managed injuries returned to full training at a mean of 20.4 days (SD 14.8), and c-class and surgically managed injuries returned significantly later than all others. Be precise on recurrence: in that series myofascial (a) re-injured least, but the higher repeat-injury rate attached to grade 3, not to c - the "c re-tears more" rule is the elite hamstring finding, extrapolated. So: c predicts a slower return; grade 3 predicts recurrence.
Mnemonics & Memory Aids
RECTUS
Hook:RECTUS: Rectus (two-joint), Eccentric kicking/sprinting, Classic distal strain, indirecT-head intrasubstance tear, mass mimics tUmour, Surgery selected (else non-op).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A footballer has chronic anterior thigh pain and a palpable mass after a kicking injury. What rectus femoris injury is this, and what must you exclude?”
What it is
- Quadriceps strain; rectus femoris = only quadriceps crossing both hip + knee (two-joint)
- Mechanism: eccentric load in kicking/sprinting
- Adolescents: AIIS apophyseal avulsion
Two patterns
- Typical: distal muscle-tendon-junction strain (distal thigh)
- Characteristic: proximal intrasubstance tear of the indirect (deep) head's intramuscular tendon
- Proximal intrasubstance tear -> anterior-thigh mass (fibrous scar) that mimics a tumour
Diagnosis & management
- MRI characterises/localises; distinguishes the intrasubstance mass from a soft-tissue tumour
- Predominantly non-operative (rest, rehabilitation, graded return)
- Surgery for selected cases (symptomatic proximal mass) after excluding tumour - based on 2 operated patients (1995)
Prognosis - the numbers
- Mean return to full training 20.4 days (SD 14.8): 38 injuries, 27 elite track-and-field athletes
- Grade 1 returns faster than grades 2 and 3; c-class and surgically managed return significantly later
- GRADE 3 carried the higher repeat-injury rate; myofascial (a) re-injured least
- 'Intratendinous re-tears more' is the elite HAMSTRING finding - extrapolated, not reproduced as c-specific in rectus femoris
- No validated return-to-play criteria or functional test battery exists for the rectus femoris
Evidence & Key Studies
Incomplete, intrasubstance strain injuries of the rectus femoris muscle
- The paper that first described the pattern - a retrospective review of just 10 athletes, all imaged with CT and/or MRI. Rectus femoris strains commonly occur at the distal muscle-tendon junction of the quadriceps tendon, but a distinct pattern is an incomplete intrasubstance tear at the muscle-tendon junction formed by the deep (indirect) head's tendon, located more proximally in the thigh.
- Mechanism was usually kicking or sprinting. All 10 had chronic thigh pain, an anterior-thigh mass, or both; examination showed thigh asymmetry and a non-tender to mildly tender intrasubstance mass. MRI showed abnormal signal centred about the intramuscular tendon of the indirect head, and surgical findings were a mass of fibrous scar and fatty tissue encasing the deep tendon.
- ONLY 2 OF THE 10 required surgery, and it is in those two that removal of the fibrous mass 'appears curative' - the entire surgical recommendation for this injury rests on two patients reported in 1995, with no comparison group and no stated follow-up duration.
- Limitations: 10 patients, retrospective, single centre, published 1995 - it establishes that the entity exists and what it looks like on MRI. It cannot supply an incidence, a recurrence rate, or a return-to-play time.
Time to return to full training and recurrence of rectus femoris injuries in elite track and field athletes 2010-2019, using the British Athletics Muscle Injury Classification
- 38 rectus femoris injuries in 27 elite British Athletics athletes (mean age 24.7, 10 male / 17 female) over 9 years, all MRI-imaged within 7 days of acute anterior thigh pain and BAMIC-graded by a specialist musculoskeletal radiologist.
- Mean time to return to full training for rehabilitation-managed injuries was 20.4 days (SD 14.8). Grade 1 returned significantly faster than grade 2 and grade 3. Intratendinous (c) and surgically managed injuries each took significantly longer than all other classes.
- Recurrence did NOT track the same variable as return time: myofascial (a) injuries had a reduced repeat-injury rate compared with b or c, but it was GRADE 3 that showed the increased repeat-injury rate. The widely quoted 'intratendinous injuries re-tear more' rule is a hamstring finding and was not reproduced as a c-specific recurrence signal here.
- All 4 complete (4c) proximal free-tendon injuries occurred during sprinting and all 4 were in female athletes - 4 events, so an observation to be aware of, not a demonstrated risk factor.
- Limitations: retrospective single-programme cohort, elite track and field only (generalisation to footballers or recreational athletes is unproven), 38 injuries spread across many BAMIC subclasses, so several comparisons rest on very small subgroups.
Time to return to full training is delayed and recurrence rate is higher in intratendinous ('c') acute hamstring injury in elite track and field athletes
- The study behind the 'c injuries are worse' teaching - but it is a HAMSTRING study, included here because the rectus femoris page inherits its rule. 65 hamstring injuries in 44 elite track and field athletes over 4 years, MRI within 7 days, BAMIC-graded by two radiologists with the reviewing physicians blinded to the classification.
- Time to return to full training differed across grades: grade 3 and 'c' injuries took significantly longer, grade 0 the least. There were 12 re-injuries, and the recurrence rate was significantly higher in intratendinous (c) injuries.
- Notably, re-injury rate did NOT differ by number grade 1-3, by which hamstring muscle was affected, by proximal versus central versus distal location, or by age or sex - so within the hamstring it was tendon involvement specifically, not extent or site, that predicted recurrence.
- Applying this to the rectus femoris is an extrapolation across a different muscle with different architecture; the rectus-femoris-specific data found grade 3 rather than c to carry the recurrence signal.
The proximal intrasubstance tear of the indirect head's intramuscular tendon, its MRI appearance, the fibrous-scar mass that mimics a neoplasm, and the observation that excision "appears curative" come from Hughes (DOI) - a 1995 review of 10 athletes of whom only 2 were operated. The return-to-training figure of 20.4 days (SD 14.8), the delayed return for c-class and surgically managed injuries, the grade-3 recurrence signal and the four female sprinting 4c tendon injuries come from McAleer (DOI), 38 injuries in 27 elite track-and-field athletes. The "intratendinous injuries re-tear more" rule comes from Pollock's elite hamstring cohort (DOI) and is applied to the rectus femoris by extrapolation. The two-joint anatomy, the direct head's AIIS origin and the indirect head's supra-acetabular origin, the eccentric kicking and sprinting mechanism, and AIIS apophyseal avulsion in adolescents are standard, well-established teaching.
What does not exist: no incidence figure for the proximal intrasubstance tear, no recurrence rate for it, no controlled comparison of excision against continued rehabilitation, and no validated return-to-play criteria or functional test battery specific to the rectus femoris. Every timing above is an observed average in elite athletes, not a target or a discharge threshold.