Criteria-Based | Psychological Readiness | Re-injury Prevention
- Criteria-based RTS associated with 84% reduction in re-injury vs time-based alone
- Limb Symmetry Index (LSI) greater than 90% on hop tests and strength
- Hop test battery: single hop, triple hop, crossover hop, 6-meter timed hop
- Psychological readiness: ACL-RSI score greater than 70 associated with successful RTS
- Re-injury risk: Up to 25% in young athletes returning to high-level pivoting sport
- “Time alone is insufficient - criteria must be met
- “Fear of re-injury is major barrier to RTS
- “Quadriceps strength is most predictive single factor
- “ACL re-injury peak occurs 6-12 months post-RTS
Time alone is insufficient - Grindem 2016 showed 84% reduction in re-injury with criteria-based RTS. Must achieve LSI greater than 90% on strength and hop tests. Psychological readiness equally important as physical criteria.
LSI = Involved/Uninvolved x 100. Target greater than 90% (ideally greater than 95%). Apply to hop tests (single, triple, crossover, timed) and isokinetic strength (quadriceps/hamstrings). Low LSI predicts re-injury.
ACL-RSI scale (0-100) - score greater than 70 associated with successful RTS. Fear of re-injury is major barrier - 50% cite as reason for not returning. Tampa Scale of Kinesiophobia also used. Address early in rehabilitation.
Young age (less than 20 years) - highest risk. Early RTS (less than 9 months post-ACL reconstruction). Returning to pivoting sports. LSI less than 90%. Not meeting criteria - 4x increased re-injury rate.
Overview and Epidemiology
The philosophy of return to sport has evolved significantly over the past two decades. The traditional approach of clearing athletes based purely on time elapsed since injury or surgery has been replaced by evidence-based, criteria-driven protocols. ACL injury is the most studied RTS model, with a global incidence of roughly 30 to 80 per 100,000 person-years (several hundred per 100,000 in young pivoting-sport athletes) and a 2 to 3 times higher risk in females. Despite successful surgery, only about 65% of athletes return to pre-injury level and ~55% to competitive sport (Ardern 2014), while up to ~23% of young athletes who return to pivoting sport sustain a second ACL injury (Wiggins 2016).
The Continuum Model
Return to sport is not a single event but a continuum with distinct phases:
- Return to Participation: Athlete can participate in rehabilitation and modified training
- Return to Sport: Athlete can return to sport activities but may be at reduced level
- Return to Performance: Athlete performs at or above pre-injury level
Why Time Alone is Insufficient
Multiple studies demonstrate that time since surgery does not correlate with readiness:
- Athletes may achieve criteria at different rates
- Tissue healing does not guarantee functional recovery
- Psychological readiness often lags behind physical recovery
- Graft maturation in ACL reconstruction continues beyond 12 months
Risk Stratification
Athletes returning to sport should be stratified by risk:
- High-risk activities: Pivoting sports (football, netball, basketball, skiing)
- Moderate-risk activities: Running, tennis, golf
- Low-risk activities: Swimming, cycling, gym work
Risk stratification guides the stringency of criteria required before clearance and helps set realistic expectations with athletes.
Pathophysiology and Biological Rationale
The criteria-based timeline is grounded in tissue biology, neuromuscular recovery and psychological adaptation - each lags behind symptomatic recovery, which is why "feeling ready" is insufficient.
Graft Maturation (Ligamentisation)
After ACL reconstruction the graft undergoes avascular necrosis, revascularisation and remodelling (ligamentisation) over many months. Mechanical strength is lowest in the early remodelling phase and the graft does not approach mature ligament properties until well beyond 12 months, providing the biological basis for why premature return (especially before 9 months) increases graft-rupture risk.
Neuromuscular and Proprioceptive Deficits
Injury and surgery produce arthrogenic muscle inhibition and persistent quadriceps weakness, altered landing mechanics (dynamic knee valgus), and impaired postural control. These deficits independently predict second injury (Paterno 2010) and recover more slowly than range of motion or effusion.
Psychological Adaptation
Fear of re-injury, reduced confidence and altered risk appraisal frequently persist after physical recovery and independently predict failure to return (Ardern 2013). Psychological readiness must therefore be tracked as a distinct biological-behavioural domain, not assumed from physical milestones.
Clinical Assessment and Functional Testing - The ACL Paradigm
ACL reconstruction serves as the most extensively studied model for return to sport criteria. The principles established from ACL research apply broadly across orthopedic injuries.
Hop Test Battery:
The four-hop test battery is the gold standard functional assessment:
- Single Hop for Distance: Maximum distance on single-leg hop
- Triple Hop for Distance: Total distance of three consecutive hops
- Crossover Hop for Distance: Three hops crossing midline alternately
- 6-Meter Timed Hop: Time to complete 6 meters hopping
Interpretation:
- Calculate Limb Symmetry Index (LSI) = Involved leg/Uninvolved leg x 100
- Target: LSI greater than 90% on all four tests
- Ideal: LSI greater than 95% associated with lower re-injury rates
- All four tests should be passed - not averaged
Limitations:
Hop tests assess quantity but not quality. Movement quality assessment (landing mechanics, valgus control) should supplement hop testing. Video analysis of hop performance provides additional information about movement patterns.
Investigation of Psychological Readiness
Psychological factors are increasingly recognized as critical determinants of successful return to sport. Fear of re-injury is the most commonly cited barrier to RTS.
ACL Return to Sport after Injury (ACL-RSI) Scale:
The ACL-RSI is a 12-item validated questionnaire assessing psychological readiness:
Domains Assessed:
- Emotions (confidence, fear, frustration)
- Confidence in performance
- Risk appraisal (perceived re-injury risk)
Scoring:
- Range: 0-100
- Higher scores indicate better psychological readiness
- Score greater than 70: Associated with successful RTS
- Score less than 56: Associated with failure to return to sport
Clinical Use:
- Administer at rehabilitation milestones
- Track progress longitudinally
- Identify athletes needing psychological intervention
- Include in RTS decision-making alongside physical criteria
Athletes with low ACL-RSI scores despite meeting physical criteria should be considered for psychology referral and may benefit from delayed RTS.
Management and RTS Criteria Across Other Injuries
While ACL reconstruction is the paradigm, RTS principles apply across orthopedic injuries with condition-specific modifications.
Return to Sport After Shoulder Stabilization:
Surgical vs Non-operative:
- Surgical stabilization in athletes has lower recurrence (10-15% vs 50-70%)
- RTS typically 4-6 months post-Latarjet, 5-6 months post-Bankart
Criteria for RTS:
- Range of Motion: Full symmetric ROM, especially external rotation
- Strength: Isokinetic strength LSI greater than 90% (rotator cuff, deltoid)
- Apprehension Testing: Negative apprehension test critical
- Functional Testing: Sport-specific overhead or contact activities
Outcome Measures:
- Rowe Score: 100-point scale for shoulder instability outcomes
- WOSI (Western Ontario Shoulder Instability Index): Quality of life measure
- Athletic Shoulder Outcome Score (ASES)
Sport-Specific Considerations:
- Overhead athletes (swimmers, throwers): Focus on external rotation and overhead stability
- Contact athletes (rugby, football): Focus on impact tolerance
- Collision sports may require bracing initially
Psychological readiness is less studied in shoulder instability but fear of apprehension position should be addressed during rehabilitation.
Complications and Prognosis
Premature or poorly assessed return to sport carries quantifiable harms; the prognosis after a well-executed criteria-based RTS is correspondingly better.
Key Complications of Inadequate RTS
- Graft rupture / second ACL injury - up to ~23% in young athletes returning to pivoting sport (Wiggins 2016); 4-fold higher if discharge criteria are not met (Kyritsis 2016).
- Contralateral ACL injury - roughly equal to ipsilateral risk (~8% vs ~7% overall; Wiggins 2016), reflecting systemic neuromuscular and biomechanical risk factors, not just the graft.
- Post-traumatic osteoarthritis - persistent quadriceps weakness and repeated injury accelerate cartilage degeneration.
- Failure to return - ~35% never reach pre-injury level and ~45% never reach competitive level despite surgery (Ardern 2014); psychological non-readiness is a leading driver.
- Recurrent muscle strain - hamstring re-injury rate up to ~30% when RTS precedes restored eccentric strength and symmetry.
Differentiating the Athlete Who Is Ready vs Not Ready
- Ready for RTS
- LSI greater than 90% (ideally greater than 95%)
- Not Ready (delay / intervene)
- LSI less than 90% - targeted strengthening, retest
- Ready for RTS
- All four tests LSI greater than 90%
- Not Ready (delay / intervene)
- Any single test LSI less than 90% (not averaged)
- Ready for RTS
- Controlled landing, no dynamic valgus
- Not Ready (delay / intervene)
- Dynamic knee valgus, hip drop, trunk lean
- Ready for RTS
- ACL-RSI greater than 70
- Not Ready (delay / intervene)
- ACL-RSI less than 56 - psychology referral, graded exposure
- Ready for RTS
- Full extension, no effusion, stable
- Not Ready (delay / intervene)
- Effusion, extension deficit, instability
- Ready for RTS
- Completed graded return to training at match intensity
- Not Ready (delay / intervene)
- Not yet exposed to cutting/pivoting at full intensity
Guidelines, Registries & Global Practice
Return to sport is a worldwide clinical problem. ACL injury - the most studied RTS model - has a global incidence of roughly 30 to 80 per 100,000 person-years, rising to several hundred per 100,000 in young athletes playing pivoting sports (football/soccer, basketball, netball, handball, alpine skiing, Australian football, rugby). Female athletes carry a 2 to 3 times higher ACL injury risk than males in equivalent sports. No single national approach dominates; recommendations converge on a criteria-based, biopsychosocial continuum.
Side-by-side guidance on RTS after ACL reconstruction:
- Key Position
- RTS is a continuum; use StARRT risk framework and a biopsychosocial model; shared decision between clinician, athlete and coach
- Key Position
- Supports rehabilitation and objective functional testing; notes limited high-level evidence for any single time-based threshold
- Key Position
- Endorses criteria-based progression, psychological readiness assessment and shared decision-making rather than fixed timelines
- Key Position
- Battery of discharge criteria (isokinetic strength, hop battery, running) before team training; basis of the Kyritsis 4x-risk data
- Key Position
- Emphasise standardised outcome reporting, shared decision-making and that no validated single criterion guarantees safe RTS
The common thread across AAOS, BOA, AO/AOSSM, EFORT-aligned European groups and the IOC is convergence on objective criteria plus psychological readiness, with explicit acknowledgement that the evidence base for precise thresholds remains limited.
Bern (international), AAOS, BOA/BASEM, Aspetar and IOC consensus all favour a criteria-based, biopsychosocial continuum over fixed time thresholds.
Hop battery, single-leg strength symmetry and the paper-based ACL-RSI deliver valid criteria-based RTS even without isokinetic dynamometry.
Controversies and Areas of Uncertainty
Despite broad consensus on a criteria-based continuum, several questions remain genuinely unresolved and are favourite viva discussion points.
- Optimal LSI threshold and its limitations - 90% is conventional, but LSI can be falsely reassuring when the uninvolved limb has also deconditioned ("both legs weak"). Some advocate comparison with pre-injury or normative values, or estimated pre-injury capacity, rather than simple limb symmetry.
- No single validated test battery - the commonly used criteria are not prospectively validated against a definitive threshold (Bern consensus, Kyritsis), and different centres use different cut-offs.
- Timing vs criteria - Grindem suggests both matter (delay to 9 months and criteria), so the relative weight of calendar time versus function is debated.
- Psychological cut-offs - ACL-RSI thresholds (greater than 70 favourable, less than 56 unfavourable) are associations, not validated decision rules, and the best instrument is unsettled.
- Role of imaging / graft maturation - MRI signal and ligamentisation status are not reliable RTS criteria; their predictive value remains uncertain.
- Generalisability beyond ACL - hop/strength symmetry criteria are extrapolated to shoulder, ankle and muscle injuries with limited high-level evidence.
- Lateral extra-articular tenodesis - whether adjunct procedures meaningfully lower the young-athlete reinjury rate enough to alter RTS counselling continues to be studied.
The StARRT Framework in Three Steps
The topic names the StARRT framework in the Bern card and the guideline table but never spells out its three steps.
- Step 1 - Tissue health. Assess the medical/tissue factors: healing status, strength, range of motion, pain, effusion and (where relevant) imaging - 'how healthy is the tissue?'
- Step 2 - Tissue stress. Assess the load the specific sport, position and level would place on that tissue, and whether it can be protected (bracing, taping). Steps 1 and 2 together define the risk of re-injury.
- Step 3 - Risk-tolerance modifiers. Weigh the non-medical factors that change how much risk is acceptable: timing (season, championship), pressure (athlete, coach, family), ability to mask the injury (painkillers/injections are a hazard), and conflict of interest of the decision-maker. These modify the decision, not the risk.
Q: What are the three steps of the StARRT return-to-sport framework?
A: StARRT (Strategic Assessment of Risk and Risk Tolerance, Shrier): (1) tissue health - the medical factors (healing, strength, ROM, pain, imaging); (2) tissue stress - the load the specific sport/position/level imposes (with or without protection) - steps 1 and 2 together give the risk of re-injury; (3) risk-tolerance modifiers - non-medical factors that change acceptable risk (timing/season, pressure from athlete/coach, ability to mask the injury [a hazard], conflict of interest). The risk is then weighed against the tolerance in a shared decision.
The Limb Symmetry Index Pitfall
The topic notes in the controversies that a 90 percent limb symmetry index can be falsely reassuring when both legs are weak, but never explains the pitfall or the alternatives.
- Why LSI can mislead. The Limb Symmetry Index assumes the uninvolved limb is a valid reference, but after injury and surgery the uninvolved limb often deconditions too (reduced training, cross-education effects). An athlete can therefore reach 90 percent symmetry while both limbs are weak, so LSI overestimates true recovery.
- The alternatives. Where possible, compare with pre-injury (baseline) values or an estimated pre-injury capacity, or with normative/population data, and express strength relative to body mass (for example quadriceps peak torque in newton-metres per kilogram) rather than pure symmetry.
- The practical rule. Use LSI as a screen, but confirm that the absolute strength - not just the symmetry - is adequate, and always pair it with a movement-quality assessment.
Q: What is the main pitfall of the Limb Symmetry Index, and how do you avoid it?
A: LSI (involved / uninvolved times 100) assumes the uninvolved limb is a valid reference, but after surgery that limb often deconditions too - so an athlete can hit 90 percent while both limbs are weak ('both legs weak'), and LSI overestimates recovery. Avoid it by also comparing with pre-injury / estimated pre-injury or normative values, expressing strength relative to body mass (e.g. newton-metres per kilogram), and confirming the absolute strength (not just symmetry) plus movement quality.
At a Glance
Return to sport (RTS) after orthopedic injury or surgery is a critical decision point that significantly impacts re-injury risk and long-term outcomes. The paradigm has shifted from time-based decisions to criteria-based approaches. Evidence demonstrates that athletes who meet specific objective criteria before returning to sport have significantly lower re-injury rates. The ACL reconstruction model is the most extensively studied and serves as the template for RTS protocols across orthopedic injuries.
Key elements of modern RTS include: Limb Symmetry Index (LSI) greater than 90% on functional hop tests and isokinetic strength testing, full range of motion, absence of pain and effusion, and critically, psychological readiness assessed via validated tools such as the ACL-RSI scale. Re-injury rates remain concerning, with up to 25% of young athletes sustaining re-injury (ipsilateral or contralateral ACL rupture) when returning to high-level pivoting sports. This underscores the importance of comprehensive assessment and realistic patient counseling.
- Time-Based Approach
- Calendar time since surgery (e.g., 9 months post-ACL)
- Criteria-Based Approach
- Objective criteria met regardless of time
- Time-Based Approach
- Higher re-injury rates (up to 25%)
- Criteria-Based Approach
- 84% reduction in re-injury (Grindem 2016)
- Time-Based Approach
- Clinical assessment, time elapsed
- Criteria-Based Approach
- LSI, hop tests, isokinetic strength, ACL-RSI
- Time-Based Approach
- Often ignored or underemphasized
- Criteria-Based Approach
- Formally assessed with validated scales
- Time-Based Approach
- Same timeline for all patients
- Criteria-Based Approach
- Tailored to individual recovery trajectory
- Time-Based Approach
- Historical practice, weak evidence
- Criteria-Based Approach
- Strong evidence from prospective studies
SHARPRTS Criteria Components
Hook:SHARP criteria = SHARP return to sport without re-injury!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old netball player is 9 months post-ACL reconstruction with hamstring autograft. She wants to return to competitive netball. How do you assess if she is ready?”
“The same netball player has hop test LSI of 85% and quadriceps LSI of 82% at 9 months. She is frustrated and says her friend returned at 6 months. How do you counsel her?”
“A 25-year-old footballer has passed all physical criteria at 10 months post-ACL reconstruction but says he is terrified of re-injury and does not feel ready. His ACL-RSI score is 48. How do you manage this?”
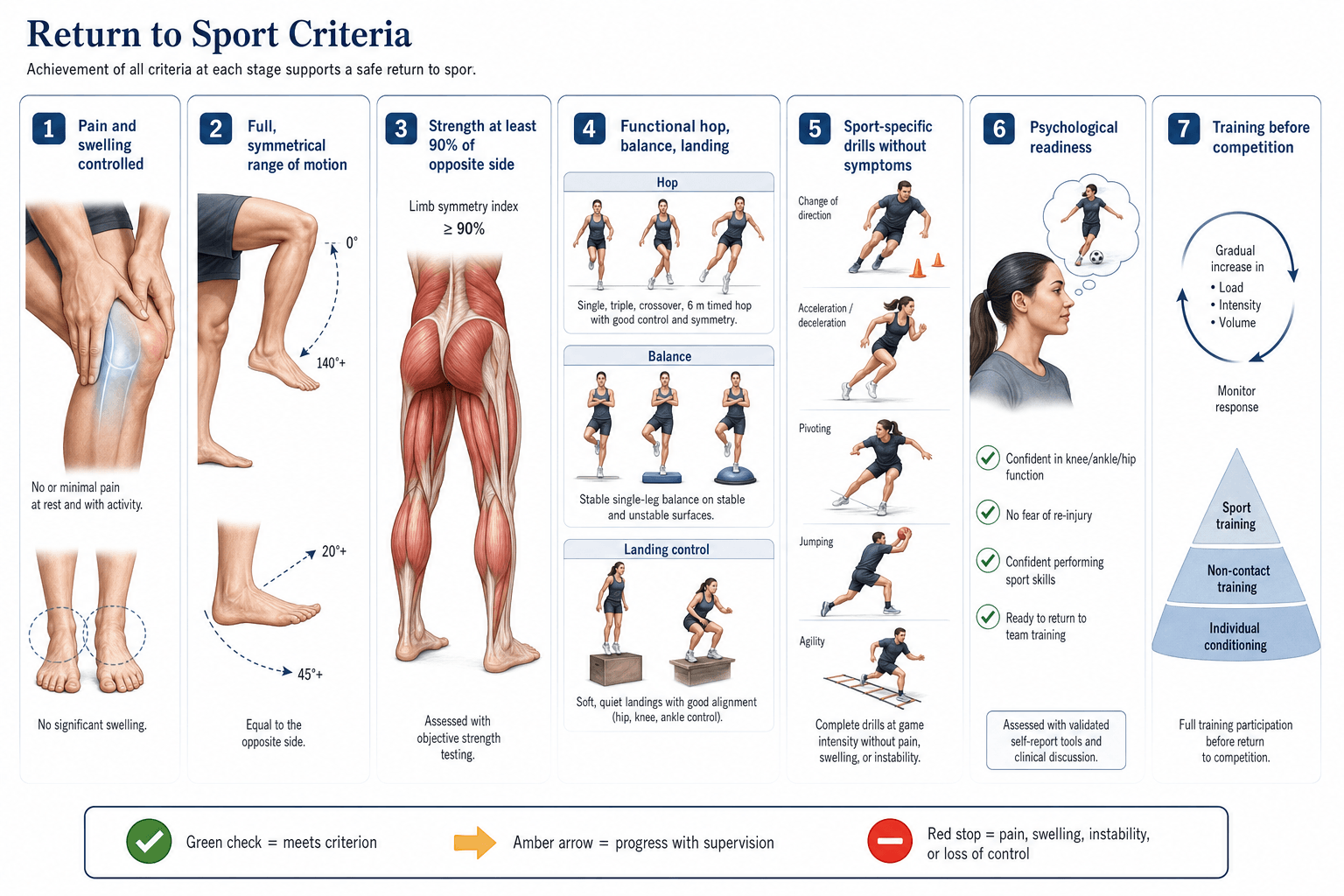
Criteria-Based RTS (SHARP)
- Strength: Isokinetic quad LSI greater than 90%
- Hop tests: Single, triple, crossover, timed LSI greater than 90%
- Absence of symptoms: No pain, effusion, instability
- Range of motion: Full extension, symmetric flexion
- Psychological: ACL-RSI greater than 70
Psychological Readiness
- ACL-RSI scale: 0-100, target greater than 70
- Score less than 56 associated with failure to RTS
- Fear of re-injury most common barrier (50%)
- Tampa Scale of Kinesiophobia also used
Re-injury Risk Factors
- Young age (less than 20 years) highest risk
- Return to pivoting sports
- RTS before criteria met (4x risk)
- Up to 25% second ACL injury in young athletes
Evidence Base
- Prospective 2-year cohort of 106 pivoting-sport athletes after ACL reconstruction
- Simple decision rules (KOS-ADL, global rating, quadriceps and hop symmetry all greater than 90) cut reinjury risk by 84%
- Failing the RTS criteria: 38.2% reinjured vs 5.6% who passed
- Reinjury rate fell 51% for each month RTS was delayed up to 9 months; more symmetrical quadriceps strength was protective
- 158 male professional athletes; 16.5% sustained graft rupture (mean 105 days after RTS)
- Not meeting all 6 discharge criteria gave a 4-fold higher graft-rupture risk (HR 4.1)
- Reduced hamstring-to-quadriceps ratio of the involved leg also raised rupture risk
- Criteria: isokinetic strength, running t-test, single/triple/triple-crossover hop