CKD-Mineral Bone Disorder | Secondary Hyperparathyroidism | Mixed Bone Disease
- CKD-MBD = chronic kidney disease mineral and bone disorder (umbrella term for bone, vascular, biochemical abnormalities)
- Pathogenesis: Phosphate retention and reduced calcitriol production lead to hypocalcemia and secondary hyperparathyroidism
- Rugger jersey spine = dense vertebral endplates (sandwich vertebrae) from subperiosteal bone formation
- Target PTH 2-9 times upper limit normal for CKD stage (not normal PTH - oversuppression causes adynamic bone)
- Vascular calcification is major complication - calcium-phosphate product should be less than 4.4 mmol squared per L squared
- “Secondary HPT in CKD is APPROPRIATE - do not parathyroidectomy unless medical management fails
- “Distinguish from primary HPT: CKD has low/normal calcium, primary HPT has high calcium
- “Adynamic bone disease from oversuppression - paradoxically increases fracture risk
- “Calciphylaxis is life-threatening vascular calcification (50% mortality) - avoid calcium-based phosphate binders if occurs
Three key defects in CKD: (1) Phosphate retention (reduced renal excretion), (2) Reduced 1-alpha hydroxylation (kidney is site of activation of vitamin D to calcitriol), (3) Hypocalcemia (reduced intestinal calcium absorption). These drive secondary hyperparathyroidism as compensatory mechanism.
High-turnover (osteitis fibrosa cystica) from severe secondary HPT - brown tumors, subperiosteal resorption. Low-turnover (adynamic bone) from oversuppressed PTH - paradoxically increased fracture risk. Mixed disease - most common, features of both. Cannot distinguish on imaging alone - bone biopsy gold standard.
Target PTH 2-9 times upper limit normal for CKD stage (NOT normal PTH). Example: CKD Stage 5 (dialysis) target PTH 150-300 pg/mL (normal is 10-65 pg/mL). Oversuppressing PTH to normal causes adynamic bone disease - low bone turnover, increased fracture risk, impaired bone healing.
Calcium-phosphate product greater than 4.4 mmol squared per L squared increases vascular calcification risk. Calcify heart valves, coronary arteries, peripheral vessels. Calciphylaxis (calcific uremic arteriolopathy) is life-threatening - painful skin necrosis from arteriolar calcification, 50% mortality. Avoid calcium-based phosphate binders if occurs.
Overview and Epidemiology
Definition
Renal osteodystrophy is the bone component of CKD-MBD (chronic kidney disease mineral and bone disorder), an umbrella term encompassing:
- Bone abnormalities - altered bone turnover, mineralization, volume, strength (renal osteodystrophy)
- Vascular/soft tissue calcification - calcium deposition in vessels, heart valves, soft tissues
- Biochemical abnormalities - disorders of calcium, phosphate, PTH, vitamin D metabolism
Renal osteodystrophy specifically refers to the spectrum of bone diseases that develop in chronic kidney disease, ranging from high-turnover (osteitis fibrosa cystica) to low-turnover (adynamic bone disease) states.
Epidemiology
- CKD Stage 3-4: 30-50% have secondary hyperparathyroidism and early bone disease
- CKD Stage 5 (dialysis): 90% have histological evidence of renal osteodystrophy
- Fracture incidence: 2-4 times higher than age-matched general population
- Vascular calcification: Present in 80% of dialysis patients
- Duration of CKD - longer duration, greater severity
- Dialysis vintage - longer time on dialysis associated with more bone disease
- Poor phosphate control - hyperphosphatemia drives PTH elevation
- Inadequate vitamin D replacement
- Aluminum exposure - historical cause of adynamic bone (now rare)
Pathophysiology
Cascade of CKD-MBD
- Reduced GFR leads to phosphate retention (kidneys cannot excrete phosphate)
- Impaired 1-alpha hydroxylase (kidney enzyme) reduces active vitamin D (calcitriol) production
- Reduced intestinal calcium absorption (low calcitriol) causes hypocalcemia
- FGF23 elevation (compensatory) further suppresses calcitriol and increases phosphate excretion (early CKD)
- Secondary hyperparathyroidism develops to maintain serum calcium
- PTH-mediated bone resorption releases calcium from skeleton
- PTH-mediated phosphate wasting (limited by reduced GFR)
- Skeletal resistance to PTH develops over time (parathyroid glands enlarge, become autonomous)
Progressive pathway:
- Early CKD (Stage 1-2): FGF23 elevates, phosphate normal, PTH begins to rise
- CKD Stage 3: Hyperphosphatemia develops, PTH rises significantly, calcitriol falls
- CKD Stage 4: Severe secondary hyperparathyroidism, high bone turnover (osteitis fibrosa)
- CKD Stage 5 (dialysis): Mixed bone disease, vascular calcification, skeletal fragility
- Post-transplant: May develop tertiary hyperparathyroidism (autonomous PTH secretion)
Spectrum of Bone Disease
- Bone Turnover
- High turnover
- PTH Level
- Very high (greater than 800 pg/mL)
- Pathophysiology
- Severe secondary HPT, excessive bone resorption
- Treatment
- Vitamin D, calcimimetics, parathyroidectomy
- Bone Turnover
- Low turnover
- PTH Level
- Low or normal
- Pathophysiology
- Oversuppressed PTH, impaired bone formation
- Treatment
- Reduce vitamin D, reduce calcium intake
- Bone Turnover
- Mixed features
- PTH Level
- Moderately elevated
- Pathophysiology
- Combination of high and low turnover
- Treatment
- Balanced approach, individualized
- Bone Turnover
- Low turnover
- PTH Level
- Variable
- Pathophysiology
- Vitamin D deficiency, aluminum toxicity (historical)
- Treatment
- Vitamin D replacement, remove aluminum
In CKD, the target PTH is 2-9 times the upper limit of normal for the CKD stage, NOT normal PTH. Example: For CKD Stage 5 (dialysis), target PTH is 150-300 pg/mL (normal is 10-65 pg/mL). Why? Because CKD patients have skeletal resistance to PTH - they need higher PTH to maintain bone turnover. Suppressing PTH to normal causes adynamic bone disease (low turnover bone) which paradoxically increases fracture risk and impairs bone healing.
Vascular Calcification
- Elevated calcium-phosphate product (Ca x PO4 greater than 4.4 mmol squared per L squared)
- Calcium hydroxyapatite precipitates in vessel walls, heart valves, soft tissues
- Transformation of vascular smooth muscle cells to osteoblast-like cells
- Mediated by uremic toxins, inflammation, oxidative stress
- Vascular calcification - coronary arteries, peripheral vessels (increased cardiovascular mortality)
- Valvular calcification - aortic stenosis, mitral regurgitation
- Calciphylaxis (calcific uremic arteriolopathy) - life-threatening arteriolar calcification with painful skin necrosis, 50% mortality
Classification
Bone Disease Spectrum Classification
- High-Turnover (Osteitis Fibrosa Cystica): Severe secondary hyperparathyroidism driving excessive bone resorption
- Low-Turnover (Adynamic Bone Disease): Oversuppressed PTH causing reduced bone formation
- Mixed Uremic Osteodystrophy: Combined features, most common type
- T = Turnover (high, normal, low)
- M = Mineralization (normal, abnormal)
- V = Volume (high, normal, low)
- Mild: Biochemical abnormalities only, no symptoms
- Moderate: Bone pain, fracture risk, radiographic changes
- Severe: Brown tumors, pathological fractures, calciphylaxis
Clinical Presentation
Symptoms
- Diffuse bone pain - worse with weight-bearing, activity
- Joint pain - secondary to renal osteodystrophy or crystal arthropathy (gout, pseudogout)
- Pathological fractures - minimal trauma, increased risk 2-4 times general population
- Skeletal deformities - in children with CKD (rickets-like changes)
- Brown tumors (lytic lesions) - jaw, ribs, pelvis, long bones
- Bone pain and tenderness
- Pathological fractures at brown tumor sites
- Rarely: pruritus (itching from calcium-phosphate deposition in skin)
- Often asymptomatic
- Increased fracture risk despite absence of pain
- Poor bone healing after fracture
- Increased risk of hypercalcemia (reduced buffering capacity)
Additional information is provided within the section.
Examination Findings
- Bone tenderness - sternum, ribs, long bones
- Skeletal deformities - in children (rickets-like bowing, short stature)
- Pathological fractures - vertebral compression, proximal femur
- Proximal muscle weakness - from concurrent vitamin D deficiency or uremic myopathy
- Calcified arteries - palpable, hardened peripheral vessels
- Vascular bruits - from stenotic calcified vessels
- Peripheral ischemia - cool extremities, poor pulses, gangrene (severe cases)
- Pruritus - scratch marks, excoriations
- Calciphylaxis lesions - painful, violaceous plaques with central necrosis
Investigations
Laboratory Investigations
Biochemical monitoring in CKD-MBD:
- CKD Stage 3-4
- 2.2-2.5 mmol/L (normal range)
- CKD Stage 5 (Dialysis)
- 2.2-2.5 mmol/L
- Rationale
- Avoid hypercalcemia (vascular calcification risk)
- CKD Stage 3-4
- 0.8-1.5 mmol/L
- CKD Stage 5 (Dialysis)
- Less than 1.5 mmol/L
- Rationale
- Control hyperphosphatemia to reduce PTH drive
- CKD Stage 3-4
- 2-4x upper limit normal
- CKD Stage 5 (Dialysis)
- 2-9x upper limit normal (150-300 pg/mL)
- Rationale
- Maintain bone turnover, avoid adynamic bone
- CKD Stage 3-4
- Greater than 75 nmol/L
- CKD Stage 5 (Dialysis)
- Greater than 75 nmol/L
- Rationale
- Adequate substrate for calcitriol production
- CKD Stage 3-4
- Monitor trend
- CKD Stage 5 (Dialysis)
- Monitor trend
- Rationale
- Marker of bone turnover (high in osteitis fibrosa)
- CKD Stage 3-4
- Less than 4.4 mmol squared per L squared
- CKD Stage 5 (Dialysis)
- Less than 4.4 mmol squared per L squared
- Rationale
- Prevent vascular calcification
- Bone-specific alkaline phosphatase - marker of bone formation (high in high-turnover disease)
- FGF23 - elevated early in CKD, promotes phosphate excretion
- Sclerostin - elevated in CKD, inhibits bone formation
- Albumin-corrected calcium - adjust for hypoalbuminemia
- CKD Stage 3: Calcium, phosphate, PTH every 6-12 months
- CKD Stage 4: Every 3-6 months
- CKD Stage 5 (dialysis): Monthly calcium and phosphate, PTH every 3 months
Imaging Studies
Plain radiographs:
- Subperiosteal resorption: Radial side of middle phalanges (hand X-ray) - pathognomonic
- Rugger jersey spine: Dense vertebral endplates (sandwich vertebrae) from subperiosteal bone formation
- Salt and pepper skull: Granular loss of skull trabeculation
- Brown tumors: Lytic expansile lesions (jaw, ribs, pelvis)
- Bone cysts: Multiple lytic lesions
- Soft tissue calcification: Vascular calcification (arteries), periarticular deposits
- Osteopenia: Generalized bone density loss
- Pathological fractures: Vertebral compression, proximal femur
- Growth plate abnormalities: Rickets-like changes in children
- Chondrocalcinosis: Calcium pyrophosphate deposition
Advanced imaging:
- DEXA scan: Assesses bone mineral density (often osteopenic or osteoporotic)
- Lateral abdominal X-ray: Screens for aortic calcification
- Echocardiogram: Detects valvular calcification (aortic stenosis, mitral regurgitation)
- CT scan: Quantifies coronary artery calcium score (cardiovascular risk assessment)
Bone Biopsy (Gold Standard)
- Diagnostic uncertainty regarding bone disease type (high vs low turnover)
- Unexplained bone pain or fractures
- Hypercalcemia with low PTH (suggestive of adynamic bone)
- Aluminum toxicity suspected (historical)
- Research purposes
- Iliac crest biopsy with tetracycline double-labeling
- Undecalcified sections for histomorphometry
- Quantifies bone volume, turnover, mineralization
- High-turnover disease (osteitis fibrosa cystica): Increased osteoid, osteoblast and osteoclast activity, marrow fibrosis
- Low-turnover disease (adynamic bone): Reduced osteoid, few osteoblasts/osteoclasts, no marrow fibrosis
- Mixed disease: Features of both high and low turnover
- Osteomalacia: Increased osteoid with prolonged mineralization lag time (rare in modern era)
Bone biopsy is rarely needed in clinical practice - treatment is guided by biochemistry (PTH, calcium, phosphate).
Differential Diagnosis
- Secondary HPT (CKD)
- Low or normal
- Primary HPT
- Elevated
- Tertiary HPT
- Elevated
- Secondary HPT (CKD)
- Elevated (CKD)
- Primary HPT
- Low or normal
- Tertiary HPT
- Variable
- Secondary HPT (CKD)
- Elevated (appropriate response)
- Primary HPT
- Elevated or inappropriately normal
- Tertiary HPT
- Elevated (autonomous)
- Secondary HPT (CKD)
- Impaired (eGFR less than 60)
- Primary HPT
- Normal or mildly impaired
- Tertiary HPT
- Improved (post-transplant) or impaired
- Secondary HPT (CKD)
- Compensatory to hypocalcemia
- Primary HPT
- Autonomous PTH secretion (adenoma)
- Tertiary HPT
- Autonomous after prolonged secondary
- Secondary HPT (CKD)
- Medical (vitamin D, binders, calcimimetics)
- Primary HPT
- Parathyroidectomy
- Tertiary HPT
- Parathyroidectomy
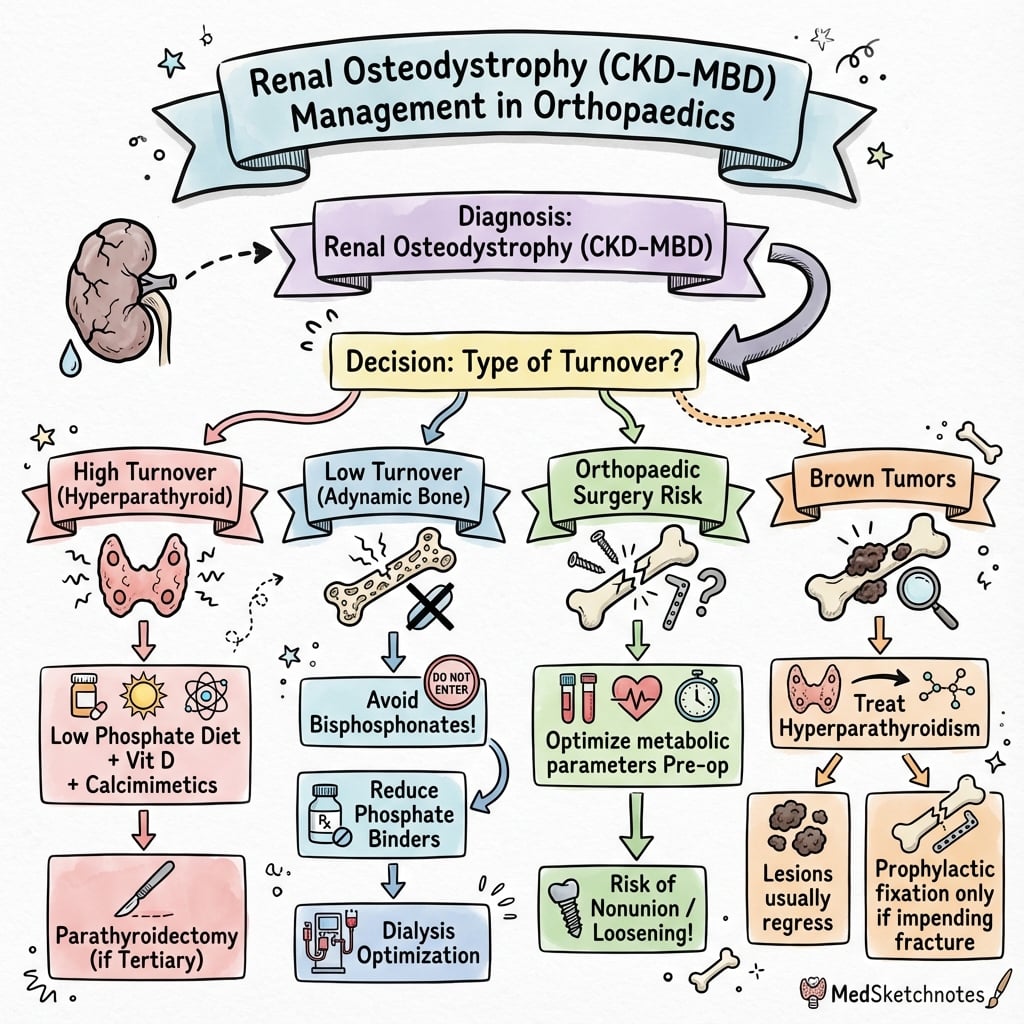
Management Algorithm
Phosphate Management
Target: Phosphate less than 1.5 mmol/L
Dietary restriction:
- Low-phosphate diet: Limit dairy products, processed foods, cola drinks, nuts
- Protein restriction: 0.8-1.0 grams per kg per day (excessive restriction causes malnutrition)
- Dietitian consultation: Essential for education and compliance
Phosphate binders:
- Example
- Calcium carbonate
- Dose
- 1-3 grams elemental calcium per day with meals
- Advantages
- Inexpensive, provides calcium
- Disadvantages
- Vascular calcification risk, hypercalcemia
- Example
- Sevelamer carbonate
- Dose
- 800-1600 mg three times daily with meals
- Advantages
- No calcium load, reduces vascular calcification
- Disadvantages
- Expensive, GI side effects
- Example
- Lanthanum carbonate
- Dose
- 500-1000 mg three times daily with meals
- Advantages
- Potent, low pill burden
- Disadvantages
- Expensive, GI side effects, theoretical toxicity
Dialysis optimization:
- Adequate dialysis removes phosphate (3-4 sessions per week, 4 hours per session)
- High-flux membranes improve phosphate clearance
- Longer or more frequent dialysis for refractory hyperphosphatemia
The primary goal is to control phosphate to reduce PTH drive and vascular calcification risk.
Management Summary and Escalation
Management Algorithm Summary
- PTH: 2-9 times upper limit normal for CKD stage (NOT normal)
- Calcium: 2.2-2.5 mmol/L
- Phosphate: Less than 1.5 mmol/L
- Ca x PO4 product: Less than 4.4 mmol squared per L squared
- Phosphate control: Dietary restriction + phosphate binders
- Vitamin D: Nutritional then activated forms
- Calcimimetics: For refractory secondary HPT
- Parathyroidectomy: For medical management failure
- CKD Stage 3: Calcium, phosphate, PTH every 6-12 months
- CKD Stage 4: Every 3-6 months
- CKD Stage 5: Monthly calcium/phosphate, PTH every 3 months
The Mechanisms Behind Calciphylaxis Therapy
The topic devotes a full section and a viva to calciphylaxis and instructs you to stop warfarin and give sodium thiosulfate - and viva scenario 3 explicitly asks the mechanism of each - but the body never explains why.
- Why warfarin causes it. Calciphylaxis reflects loss of the body's natural inhibitors of vascular calcification. Matrix Gla protein (MGP) is a potent local inhibitor of arterial-media calcification, but it must be carboxylated by a vitamin-K-dependent enzyme to be active. Warfarin blocks vitamin-K recycling, leaving MGP undercarboxylated and inactive, so calcium deposits freely in the arteriolar media - hence warfarin is a major modifiable precipitant and is stopped (switch to heparin or a direct oral anticoagulant).
- Why sodium thiosulfate helps. IV sodium thiosulfate (25 g three times weekly with dialysis) is thought to work by chelating calcium to form the far more soluble calcium thiosulfate (mobilising and dissolving vascular calcium deposits), and by acting as an antioxidant and vasodilator that improves the ischaemic microcirculation. The evidence is largely case-series, but it is the standard pharmacological agent.
- The wider principle. These sit alongside the other measures the topic lists - lowering the calcium load (stop calcium-based binders), aggressive phosphate control to reduce the calcium-phosphate product, treating severe hyperparathyroidism, meticulous wound care and analgesia - because calciphylaxis reflects an overwhelmed balance between pro-calcific drive and lost inhibition.
Q: How does warfarin contribute to calciphylaxis, and how does sodium thiosulfate treat it? A: Warfarin inhibits vitamin-K-dependent carboxylation of matrix Gla protein, the key inhibitor of arterial-media calcification; undercarboxylated MGP is inactive, so arteriolar calcification proceeds - hence warfarin is stopped and switched to heparin or a DOAC. Sodium thiosulfate chelates calcium to form soluble calcium thiosulfate (dissolving vascular deposits) and acts as an antioxidant/vasodilator, alongside removing the calcium load (stop calcium binders), controlling phosphate, wound care and analgesia.
Surgical Management - Parathyroidectomy
Indications for Parathyroidectomy in CKD
- Refractory severe secondary hyperparathyroidism - PTH persistently greater than 800-1000 pg/mL despite maximal medical therapy (vitamin D, calcimimetics, phosphate control)
- Hypercalcemia with elevated PTH - calcium persistently greater than 2.65 mmol/L
- Calciphylaxis - calcific uremic arteriolopathy with severe secondary hyperparathyroidism
- Symptomatic bone disease - brown tumors, pathological fractures, intractable bone pain
- Pruritus refractory to medical management (elevated calcium-phosphate product)
- Progressive vascular or soft tissue calcification
- Tertiary hyperparathyroidism post-renal transplant (autonomous PTH secretion with hypercalcemia)
Surgical Options
- Technique
- Remove 3.5 glands (leave half of one gland)
- Advantages
- Preserves parathyroid function, avoids hypoparathyroidism
- Disadvantages
- 10-15% recurrence rate
- Technique
- Remove all 4 glands, transplant 50-100 mg parathyroid tissue to forearm
- Advantages
- Easy access for reoperation (forearm), lower recurrence
- Disadvantages
- Risk of graft failure (5-10%), hypoparathyroidism
- Technique
- Remove all 4 glands, lifelong calcium and calcitriol
- Advantages
- Lowest recurrence rate
- Disadvantages
- Permanent hypoparathyroidism, lifelong supplementation
Preoperative preparation:
- Optimize medical management - continue phosphate binders, vitamin D
- Imaging: Sestamibi scan and ultrasound to localize glands (less sensitive than primary HPT)
- Cardiovascular assessment - high perioperative risk in dialysis patients
- Informed consent - discuss hungry bone syndrome risk
Postoperative Management
- Occurs in 30-50% of patients after parathyroidectomy for severe secondary hyperparathyroidism
- Profound hypocalcemia and hypophosphatemia as demineralized skeleton avidly takes up minerals
- Risk factors: Preoperative PTH greater than 1000 pg/mL, large adenomas, elevated alkaline phosphatase
- Aggressive calcium replacement:
- Oral calcium 3-6 grams daily (divided doses)
- IV calcium gluconate if symptomatic (1-2 grams every 6 hours)
- Calcitriol: 0.5-2 micrograms daily
- Magnesium replacement: Often depleted, impairs PTH secretion
- Daily monitoring: Calcium, phosphate, magnesium for first week
- Gradual weaning: Over weeks to months as skeleton remineralizes
- PTH normalizes or becomes low - may develop adynamic bone disease
- Bone pain improves within weeks to months
- Brown tumors regress over 6-12 months
- Fracture risk decreases
- Pruritus resolves in 70-80%
Complications and Special Considerations
Calciphylaxis (Calcific Uremic Arteriolopathy)
Life-threatening arteriolar calcification causing painful skin necrosis
1-4% of dialysis patients per year
- Female gender
- Obesity
- Warfarin use
- High calcium-phosphate product
- Diabetes mellitus
- Severe secondary hyperparathyroidism
- Painful violaceous skin lesions progressing to necrosis
- Distribution: Lower legs, thighs, abdomen (areas with high adiposity)
- Livedo reticularis pattern
- Eschar formation with ulceration
- Skin biopsy: Calcification of dermal arterioles and adipose tissue (caution - may worsen necrosis)
- Imaging: Soft tissue calcification on plain X-rays
- Stop warfarin immediately - switch to heparin or direct oral anticoagulants
- Aggressive wound care - debridement, infection control
- Sodium thiosulfate - IV 25 grams three times weekly with dialysis (calcium chelator)
- Optimize phosphate and calcium control - avoid calcium-based binders
- Parathyroidectomy if severe secondary hyperparathyroidism
- Pain management - often requires opioids
50% mortality (sepsis from infected wounds)
Fracture Management in CKD
- 2-4 times higher than age-matched general population
- Hip fracture most common, highest morbidity and mortality
- Vertebral compression fractures often asymptomatic
- Optimize medical management preoperatively - control PTH, calcium, phosphate
- High cardiovascular risk - careful anesthetic assessment
- Poor bone quality - soft bone (high-turnover disease) or brittle bone (low-turnover disease)
- Risk of hypercalcemia postoperatively - mobilization of immobilized calcium stores
- Soft bone in high-turnover disease - poor screw purchase, consider cement augmentation
- Brittle bone in low-turnover disease - increased periprosthetic fracture risk
- Delayed healing - impaired bone remodeling
- Higher infection risk - uremia impairs immune function
- Continue dialysis - optimize schedule around surgery
- Aggressive mobilization - reduce immobilization complications
- Thromboprophylaxis - balance bleeding risk (uremic platelet dysfunction) vs thrombosis risk
- Nutrition optimization - adequate protein (healing), avoid malnutrition
Postoperative Care
Post-Parathyroidectomy Care
- Calcium levels every 6 hours initially
- Watch for hungry bone syndrome (profound hypocalcemia)
- Symptoms: Perioral tingling, Chvostek sign, tetany
- Oral calcium 3-6 grams daily in divided doses
- IV calcium gluconate if symptomatic (1-2 grams every 6 hours)
- Calcitriol 0.5-2 micrograms daily
- Magnesium replacement often needed
- Continue dialysis schedule around surgery
- Optimize nutrition (protein for healing)
- Early mobilization when stable
- Thromboprophylaxis (balance bleeding vs clot risk)
Outcomes
Treatment Outcomes
- Phosphate control: Achievable in 60-70% with compliance
- PTH suppression: Target achieved in 40-50% with aggressive management
- Fracture prevention: Improved with optimized bone turnover
- Perioperative mortality: 2-3% (cardiovascular risk)
- PTH normalization: 85-95%
- Bone pain improvement: 70-80%
- Pruritus resolution: 70-80%
- Hip fracture 1-year mortality: 30% (2x general population)
- Delayed healing common
- Fixation failure higher due to poor bone quality
The Rugger Jersey Spine Mechanism
Viva scenario 2 explicitly asks "what is the mechanism of rugger jersey spine formation?" and the term appears throughout, but the body only says "dense vertebral endplates from subperiosteal bone formation" without explaining the actual mechanism.
- What it looks like. On the lateral spine radiograph each vertebral body shows dense sclerotic bands along its superior and inferior margins (the endplate regions) around a relatively lucent central band - a horizontally striped "sandwich vertebra" resembling the hoops of a rugby (rugger) jersey.
- The mechanism. It is osteosclerosis driven by secondary hyperparathyroidism, not simple periosteal new bone. In high-turnover disease, high PTH stimulates osteoblastic deposition of new (often woven) bone preferentially in the metabolically most active subchondral trabecular bone next to the vertebral endplates, while the central body is comparatively spared - producing the banded appearance. (This is why "subperiosteal" is a loose label; the process is subchondral endplate osteosclerosis.)
- What it signifies. Rugger jersey spine is essentially pathognomonic of the high-turnover renal osteodystrophy of CKD and therefore of significant secondary hyperparathyroidism; it should prompt review of PTH, calcium, phosphate and the adequacy of CKD-MBD control. It is distinct from the "sandwich vertebra" of osteopetrosis (uniform, sharply marginated endplate sclerosis from failed osteoclastic resorption) and from Paget or haemangioma striping.
Q: What is the mechanism of rugger jersey spine? A: It is osteosclerosis of the subchondral bone at the vertebral endplates driven by secondary hyperparathyroidism in high-turnover renal osteodystrophy - high PTH stimulates osteoblastic new-bone deposition in the metabolically active endplate regions, giving dense superior and inferior bands around a lucent central body (the striped "sandwich" appearance). It is essentially pathognomonic of CKD-MBD and should prompt review of PTH/calcium/phosphate control; distinguish it from the uniform endplate sclerosis of osteopetrosis.
Guidelines, Registries & Global Practice
Global Epidemiology and Guidelines
CKD-MBD is a worldwide problem tied to the rising global burden of diabetes and hypertension. Roughly 90% of long-term dialysis patients have histological renal osteodystrophy, fracture rates run 2-4 times the general population, and CKD-MBD is a major driver of the excess cardiovascular mortality seen across all dialysis registries (ANZDATA, USRDS, ERA Registry, UK Renal Registry).
Side-by-side guidance:
- PTH target (dialysis)
- 2-9x upper limit normal; act on trends
- Binder/calcium stance
- Restrict calcium-based binders; lower phosphate toward normal
- Bone biopsy
- Reasonable before antiresorptives if it changes management
- PTH target (dialysis)
- Aligns with KDIGO range
- Binder/calcium stance
- Favours non-calcium binders if calcification/adynamic bone
- Bone biopsy
- Selective, not routine
- PTH target (dialysis)
- Within KDIGO band; individualise
- Binder/calcium stance
- NICE supports sevelamer/lanthanum where calcium load a concern
- Bone biopsy
- Reserved for diagnostic uncertainty
- PTH target (dialysis)
- Consistent with KDIGO; emphasise phosphate control first
- Binder/calcium stance
- Stepwise; calcimimetics for refractory HPT
- Bone biopsy
- Selective
Controversies and Areas of Uncertainty
The 2-9x upper limit normal range is wide and graded weak (2C). Inter-assay variability in PTH measurement is large, and the relationship between any single PTH value and bone histology is imperfect. Trends matter more than absolute numbers.
Despite mechanistic concern about calcium loading and vascular calcification, RCT data (DCOR) did not show a clear mortality advantage for non-calcium binders. Choice balances cost, calcium load and calcification risk rather than proven survival benefit.
EVOLVE was negative on its intention-to-treat primary cardiovascular endpoint. Calcimimetics reliably lower PTH and reduce parathyroidectomy referrals, but a mortality or fracture benefit is unproven.
Bisphosphonates and denosumab are used cautiously in advanced CKD: they may worsen adynamic (low-turnover) bone and provoke severe hypocalcaemia (denosumab). Bone biopsy to exclude adynamic disease before antiresorptives is debated but reasonable.
Other unresolved questions:
- Role of bone biopsy - gold standard but rarely performed; non-invasive surrogates (TBS, HR-pQCT, bone turnover markers) are promising but not yet definitive substitutes
- Surgical vs medical parathyroidectomy - threshold for surgery versus escalating calcimimetics is not standardised, and varies with drug availability
- Subtotal vs total parathyroidectomy with autotransplantation - trade-off between recurrence and permanent hypoparathyroidism remains unsettled
- DXA in CKD - now endorsed by KDIGO 2017 for fracture risk in CKD G3a-G5D if results change management, reversing earlier scepticism
MCQ Practice Points
Q: What is the target PTH for a patient on hemodialysis (CKD Stage 5)?
A: 2-9 times the upper limit of normal, which translates to approximately 150-300 pg/mL (normal PTH is 10-65 pg/mL). This elevated PTH target maintains adequate bone turnover. Suppressing PTH to normal causes adynamic bone disease (low turnover) which paradoxically increases fracture risk and impairs bone healing.
Q: What is rugger jersey spine and what does it indicate?
A: Rugger jersey spine is dense vertebral endplates (sandwich vertebrae) creating horizontal bands on lateral spine X-ray, resembling a rugby jersey. It results from subperiosteal bone formation in high-turnover renal osteodystrophy (secondary hyperparathyroidism). Pathognomonic for CKD-mineral bone disorder.
Q: A dialysis patient develops painful violaceous skin lesions with necrosis on the thighs. What is the diagnosis and immediate management?
A: Calciphylaxis (calcific uremic arteriolopathy). Life-threatening with 50% mortality. Immediate management: (1) stop warfarin (major risk factor), (2) aggressive wound care (debridement, infection control), (3) IV sodium thiosulfate 25 grams three times weekly with dialysis, (4) stop calcium-based phosphate binders, (5) optimize calcium-phosphate product to less than 4.4 mmol squared per L squared.
Q: How do you distinguish secondary from tertiary hyperparathyroidism?
A: Secondary HPT: Low or normal calcium with elevated PTH (appropriate compensatory response to hypocalcemia in CKD). Tertiary HPT: Elevated calcium with elevated PTH (autonomous PTH secretion after prolonged secondary HPT, typically post-renal transplant). Treatment differs - secondary HPT is medical (vitamin D, phosphate binders, calcimimetics), tertiary HPT requires parathyroidectomy.
At a Glance
Renal osteodystrophy (part of CKD-MBD) affects 90% of dialysis patients with bone disease. The pathogenesis triad is: phosphate retention, reduced calcitriol production, and hypocalcemia, driving secondary hyperparathyroidism. The bone disease spectrum ranges from osteitis fibrosa cystica (high-turnover, brown tumors) to adynamic bone disease (low-turnover from oversuppressed PTH—paradoxically increases fracture risk). The radiographic rugger jersey spine (dense vertebral endplates) is pathognomonic. Target PTH is 2-9× upper limit normal (NOT normal—oversuppression is harmful). Monitor the calcium-phosphate product (keep under 4.4 mmol²/L²) to prevent vascular calcification; calciphylaxis carries 50% mortality.
KIDNEYSPathogenesis of Renal Osteodystrophy
Hook:Remember KIDNEYS fail, causing the cascade of mineral and bone disease!
PHOSPHATEMedical Management of CKD-MBD
Hook:Control PHOSPHATE to manage renal osteodystrophy!
RUGGERRadiographic Features of Renal Osteodystrophy
Hook:RUGGER jersey spine is pathognomonic for renal osteodystrophy!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man on hemodialysis for 8 years presents with diffuse bone pain. Blood tests show calcium 2.1 mmol/L, phosphate 2.2 mmol/L, PTH 650 pg/mL, alkaline phosphatase 320 U/L. He is taking calcium carbonate 1500 mg three times daily with meals as a phosphate binder. What is your assessment and management?”
“A 48-year-old woman on peritoneal dialysis for 10 years presents with a painful swelling of the jaw. X-rays show a lytic expansile lesion of the mandible. Spine X-rays show dense vertebral endplates (rugger jersey spine). Blood tests show calcium 2.8 mmol/L, PTH 1200 pg/mL. How do you assess and manage this patient?”
“A 62-year-old obese diabetic woman on hemodialysis develops painful violaceous skin lesions on her thighs with central necrosis. She is on warfarin for atrial fibrillation. Blood tests show calcium 2.6 mmol/L, phosphate 2.0 mmol/L, PTH 420 pg/mL. She is taking calcium carbonate as a phosphate binder. What is your diagnosis and management?”
Key Pathophysiology
- CKD causes phosphate retention (reduced renal excretion) and reduced calcitriol production (impaired 1-alpha hydroxylation)
- Hypocalcemia and hyperphosphatemia drive secondary hyperparathyroidism (compensatory)
- PTH causes bone resorption (high-turnover disease - osteitis fibrosa cystica)
- Oversuppression of PTH causes low-turnover disease (adynamic bone) which increases fracture risk
Spectrum of Bone Disease
- Osteitis fibrosa cystica: High-turnover from severe secondary HPT (brown tumors, subperiosteal resorption)
- Adynamic bone disease: Low-turnover from oversuppressed PTH (increased fracture risk)
- Mixed disease: Most common, features of both high and low turnover
- Bone biopsy is gold standard but rarely needed (treat based on biochemistry)
Target Biochemistry
- PTH: 2-9x upper limit normal for CKD stage (150-300 pg/mL for dialysis, NOT normal)
- Calcium: 2.2-2.5 mmol/L (avoid hypercalcemia - vascular calcification risk)
- Phosphate: less than 1.5 mmol/L (phosphate binders plus dietary restriction)
- Ca x PO4 product: less than 4.4 mmol squared per L squared (prevent vascular calcification)
- 25-OH vitamin D: greater than 75 nmol/L (substrate for calcitriol production)
Radiographic Features
- Rugger jersey spine: Dense vertebral endplates (sandwich vertebrae) - pathognomonic
- Subperiosteal resorption: Radial side of middle phalanges (hand X-ray)
- Salt and pepper skull: Loss of skull trabeculation
- Brown tumors: Lytic lesions from severe secondary HPT (jaw, ribs, pelvis)
- Vascular calcification: Arteries, heart valves, soft tissues
Medical Management
- Phosphate control: Binders (calcium carbonate or sevelamer) plus dietary restriction
- Vitamin D: Replete 25-OH vitamin D, then activated vitamin D (calcitriol, paricalcitol) to suppress PTH
- Calcimimetics: Cinacalcet for refractory secondary HPT (PTH greater than 300-800 despite vitamin D)
- Calcium management: Target 2.2-2.5 mmol/L, avoid excess (vascular calcification risk)
- Dialysis optimization: Adequate sessions remove phosphate, maintain mineral balance
Parathyroidectomy Indications
- Refractory secondary HPT: PTH persistently greater than 800-1000 despite maximal medical therapy
- Hypercalcemia with elevated PTH (tertiary HPT)
- Symptomatic bone disease (brown tumors, pathological fractures, intractable pain)
- Calciphylaxis with severe secondary HPT
- Options: Subtotal (3.5 glands) or total with autotransplantation to forearm
Complications
- Hungry bone syndrome: Profound hypocalcemia post-parathyroidectomy (30-50% risk), requires aggressive calcium replacement
- Calciphylaxis: Painful skin necrosis from arteriolar calcification (50% mortality), stop warfarin, sodium thiosulfate
- Fracture risk: 2-4x higher than general population, poor bone quality (soft or brittle)
- Vascular calcification: Coronary arteries, heart valves, peripheral vessels (increased cardiovascular mortality)
Evidence Base and Key Studies
KDIGO 2017 CKD-MBD Guideline Update
- In CKD G5D, suggest maintaining intact PTH approximately 2-9 times the upper limit of normal for the assay (NOT normal PTH)
- Marked changes in PTH in either direction should prompt initiation or change in therapy rather than reacting to a single value
- Lowering elevated phosphate toward the normal range is suggested; avoid hypercalcaemia; restrict dose of calcium-based binders
- Bone biopsy is reasonable where knowledge of turnover/mineralisation type will change treatment (e.g. before antiresorptives)
Bone Mass and Microarchitecture in CKD Fracture
- Case-control of predialysis CKD: 32 patients with fracture vs 59 without, imaged by DXA and HR-pQCT
- Fracture patients had lower areal BMD at spine, hip and ultradistal radius (radius most discriminating)
- HR-pQCT showed lower cortical area/thickness, lower trabecular volumetric density and trabecular loss in fracture cases
- Structural cortical and trabecular deficits, not density alone, underlie skeletal fragility in CKD
EVOLVE: Cinacalcet and Cardiovascular Outcomes
- RCT of 3883 haemodialysis patients with moderate-to-severe secondary HPT (median PTH 693 pg/mL): cinacalcet vs placebo
- Primary composite (death, MI, unstable angina, heart failure, peripheral vascular event) reached in 48.2% vs 49.2%; unadjusted HR 0.93 (95% CI 0.85-1.02, P=0.11) - not significant
- Cinacalcet effectively lowered PTH but caused significantly more hypocalcaemia and gastrointestinal adverse events
- Prespecified age-adjusted and lag-censored analyses suggested possible benefit, but the intention-to-treat result was negative
Parathyroidectomy and Survival in Dialysis
- USRDS matched cohort: 4558 dialysis patients undergoing first parathyroidectomy vs 4558 matched controls
- 30-day postoperative mortality 3.1% (early excess risk from cardiovascular comorbidity)
- Long-term relative risk of death 10-15% lower after parathyroidectomy; survival curves crossed at approximately 587 days
- Median survival 53.4 vs 46.8 months favouring the parathyroidectomy group
DCOR: Sevelamer vs Calcium-Based Binders
- Intention-to-treat secondary analysis of the DCOR RCT using CMS claims data in haemodialysis patients
- All-cause mortality 17.7 vs 17.4 deaths per 100 patient-years (P=0.9 adjusted) - no significant difference vs calcium binders
- Cardiovascular mortality also not significantly different between sevelamer and calcium-based binders
- Sevelamer was associated with fewer multiple all-cause hospitalisations and fewer hospital days (secondary endpoints)
Calciphylaxis: Risk Factors and Prognosis
- Single-centre peritoneal dialysis cohort (n=63): 7 developed calciphylaxis (incidence 9.0 per 1000 patient-years)
- Female sex, obesity, prior haemodialysis, recurrent hypotension, high time-averaged phosphate, low albumin and warfarin associated with risk
- One-year mortality 71% despite sodium thiosulfate, hyperbaric oxygen, cinacalcet and wound debridement
- Reinforces avoidance of warfarin and aggressive mineral control as modifiable factors