Childhood Vitamin D Deficiency | Defective Endochondral Ossification | Growth Plate Disorder
- Rickets = defective mineralization of growth plate in children (vs osteomalacia in adults)
- Rachitic rosary, bowing, widened wrists/ankles = classic skeletal features
- X-ray shows widened, irregular, frayed metaphyses with cupping
- Treatment: vitamin D 2000-6000 IU daily until healing, then 400-600 IU maintenance
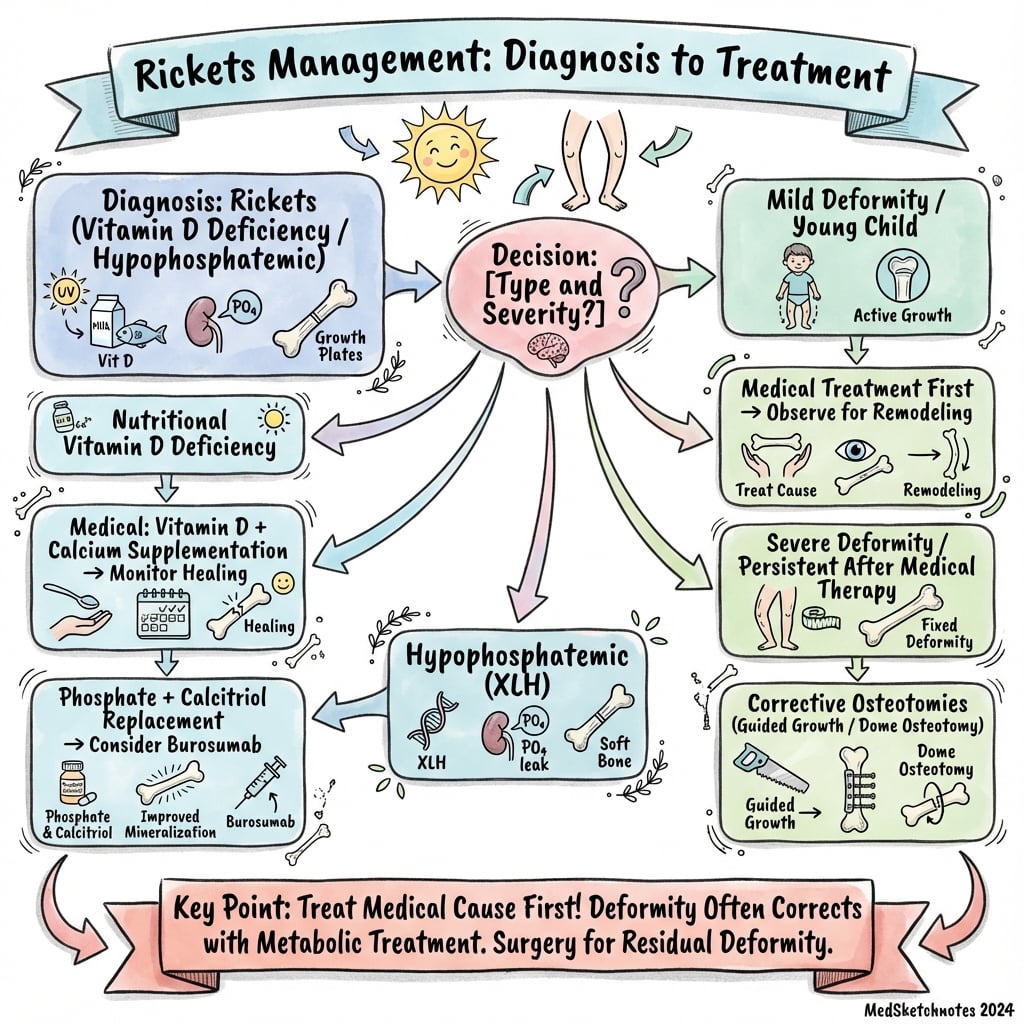
- Surgical correction (osteotomy) ONLY after medical optimization - 12-18 months treatment
- “Distinguish nutritional rickets (low vitamin D) from X-linked hypophosphatemia (normal vitamin D, low phosphate)
- “Rachitic rosary = swelling at costochondral junctions (palpable beading along sternum)
- “Bowing deformities: genu varum (most common), genu valgum, windswept deformity
- “Delayed surgical correction until biochemistry normalized prevents recurrence
Defective endochondral ossification at physis. Unmineralized hypertrophic zone accumulates, causing widened, irregular growth plates. Unlike osteomalacia (affects osteoid in mature bone), rickets affects cartilage mineralization in growing bones.
Rachitic rosary (costochondral swelling), bowing (genu varum/valgum), widened wrists and ankles, frontal bossing, delayed fontanelle closure. Craniotabes (soft skull) in infants.
Widened, frayed, cupped metaphyses. Loss of sharp zone of provisional calcification. Osteopenia. Looser zones in long-standing cases. Most visible at distal radius, knee (distal femur, proximal tibia).
Never operate on active rickets. Optimize vitamin D (greater than 75 nmol/L), normalize calcium/phosphate/ALP. Wait 12-18 months for spontaneous deformity correction. Surgery only for residual deformity after healing.
- Biochemistry
- Low Ca/vitamin D, low-normal PO4, high ALP
- Inheritance
- Environmental (dietary, sunlight)
- Treatment
- Vitamin D 2000-6000 IU daily + calcium
- Biochemistry
- Low PO4, normal Ca/vitamin D, high ALP, high FGF23
- Inheritance
- X-linked dominant (PHEX gene)
- Treatment
- Phosphate 20-60 mg/kg/day + calcitriol
- Biochemistry
- Low Ca, normal vitamin D, low 1,25-OH D
- Inheritance
- Autosomal recessive (CYP27B1 gene)
- Treatment
- Calcitriol 0.25-2 micrograms daily
- Biochemistry
- Low Ca, high 1,25-OH D (receptor resistance)
- Inheritance
- Autosomal recessive (VDR gene)
- Treatment
- Very high-dose calcitriol or IV calcium
Overview and Definition
Definition
Rickets is a metabolic bone disease of childhood characterized by defective mineralization of growing bone, specifically at the growth plate (physis) and osteoid. It is the pediatric equivalent of osteomalacia, which affects mature bone in adults. The hallmark is failure of endochondral ossification, leading to accumulation of unmineralized cartilage matrix, skeletal deformities, and growth disturbance.
Epidemiology
Rickets remains a significant global health problem despite being preventable:
- Exclusively breastfed infants without vitamin D supplementation
- Dark-skinned individuals in high-latitude countries (reduced UV-B cutaneous synthesis)
- Cultural/religious practices limiting sun exposure (covering clothing)
- Preterm infants (increased vitamin D requirements)
- Maternal vitamin D deficiency during pregnancy
- Vegan/vegetarian diets without fortified foods
- Malabsorption syndromes (celiac disease, cystic fibrosis, inflammatory bowel disease)
- Chronic kidney disease (impaired 1-alpha hydroxylation)
- Higher incidence in Northern Europe, Canada, Northern US (limited sunlight)
- Re-emergence in developed countries due to decreased sun exposure and increased breastfeeding without supplementation
- Endemic in Middle East, South Asia (cultural sun avoidance despite abundant sunlight)
Pathophysiology
Vitamin D Metabolism and Calcium Homeostasis
- Cutaneous synthesis - UV-B radiation converts 7-dehydrocholesterol to cholecalciferol (vitamin D3) in skin
- Hepatic hydroxylation - 25-hydroxylase converts D3 to 25-OH vitamin D (calcidiol) - main storage form
- Renal activation - 1-alpha hydroxylase converts 25-OH D to 1,25-OH vitamin D (calcitriol) - active hormone
- Target organ effects - calcitriol increases intestinal calcium and phosphate absorption, promotes skeletal mineralization
- PTH stimulates 1-alpha hydroxylase (increases active vitamin D production)
- Hypocalcemia triggers PTH release → secondary hyperparathyroidism
- FGF23 inhibits 1-alpha hydroxylase and increases renal phosphate excretion
Molecular Cascade at the Physis
Normal endochondral ossification requires adequate calcium, phosphate, and vitamin D. In rickets, deficiency of vitamin D (or phosphate) disrupts the mineralization of cartilage matrix at the growth plate:
Pathologic sequence:
- Reduced calcium and phosphate availability at the growth plate
- Chondrocyte proliferation and hypertrophy proceed normally - cartilage matrix production continues
- Mineralization fails - calcium-phosphate crystals (hydroxyapatite) cannot be deposited
- Accumulation of unmineralized hypertrophic cartilage - widened, irregular growth plate (10-20x normal thickness)
- Loss of columnar organization - disorganized chondrocyte arrangement
- Irregular zone of provisional calcification - patchy, incomplete mineralization
- Disorganized vascular invasion and osteoblast/osteoclast activity at metaphysis
- Metaphyseal widening, cupping, and fraying (radiographic hallmark)
- Mechanical deformation of soft unmineralized bone under weight-bearing stress → bowing deformities
- Growth retardation from disrupted longitudinal bone growth
Type-Specific Mechanisms
- Vitamin D deficiency → reduced intestinal calcium/phosphate absorption
- Hypocalcemia → secondary hyperparathyroidism
- PTH → increased renal phosphate loss, bone resorption
- Net effect: low calcium AND phosphate, inadequate mineralization
- PHEX gene mutation → elevated FGF23 (fibroblast growth factor 23)
- FGF23 → renal phosphate wasting (reduced proximal tubule phosphate reabsorption)
- FGF23 → inhibits 1-alpha hydroxylase (reduced active vitamin D despite normal 25-OH D)
- Net effect: severe isolated hypophosphatemia, normal calcium
- Type I: CYP27B1 mutation → 1-alpha hydroxylase deficiency → cannot produce active vitamin D
- Type II: VDR mutation → vitamin D receptor defect → resistance to calcitriol (very high 1,25-OH D levels)
- Widened hypertrophic zone (10-20x normal thickness)
- Loss of columnar organization of chondrocytes
- Irregular zone of provisional calcification (patchy, incomplete)
- Metaphyseal cupping and fraying on X-ray
- Persistent hypertrophic chondrocytes (failed apoptosis)
- Bowing deformities from weight-bearing (genu varum/valgum)
- Frontal bossing and delayed fontanelle closure
- Rachitic rosary (costochondral swelling)
- Growth failure and short stature
- Skeletal fragility (pathologic fractures)
DEFICIENTCauses of Rickets
Hook:Children become DEFICIENT in vitamin D through dietary, environmental, or genetic causes!
Classification
Classification by Etiology
Calcipenic Rickets (Calcium Deficiency)
- Nutritional vitamin D deficiency (most common)
- Dietary calcium deficiency
- Malabsorption syndromes (celiac, cystic fibrosis)
- Drug-induced (anticonvulsants)
Phosphopenic Rickets (Phosphate Deficiency)
- X-linked hypophosphatemia (PHEX mutation)
- Autosomal dominant hypophosphatemic rickets
- Tumor-induced osteomalacia (FGF23-secreting tumors)
- Fanconi syndrome (renal tubular phosphate wasting)
Vitamin D-Dependent Rickets
- Type I: 1-alpha hydroxylase deficiency (CYP27B1 mutation)
- Type II: Vitamin D receptor defect (VDR mutation)
Clinical Presentation
Age-Dependent Features
Infant Rickets
- Craniotabes - soft skull bones (ping-pong ball sensation)
- Frontal bossing - prominent forehead
- Delayed fontanelle closure
- Rachitic rosary - costochondral junction swelling
- Harrison's groove - indentation along diaphragm attachment
- Hypotonia - floppy baby
- Delayed motor milestones - sitting, crawling
- Hypocalcemic seizures (if severe deficiency)
- Laryngospasm and stridor (tetany)
- Failure to thrive
- Growth retardation
Early diagnosis critical to prevent permanent skeletal deformities.
Metaphyseal fractures in rickets can mimic abuse. Both cause corner fractures and metaphyseal lucencies. Distinguish by:
- Rickets: symmetric metaphyseal changes, rachitic rosary, biochemical abnormalities (low vitamin D, high ALP), no bruising
- NAI: asymmetric injuries, multiple fractures of different ages, soft tissue bruising, normal biochemistry
Always consider rickets in differential diagnosis of metaphyseal fractures in infants. However, rickets does not exclude abuse - both can coexist.

RICKETSClinical Features of Rickets
Hook:Kids with RICKETS have visible skeletal changes - rosary, widened joints, bowing, and growth problems!
Laboratory Findings
Biochemistry by Type
- Calcium
- Low-normal
- Phosphate
- Low-normal
- 25-OH Vit D
- Very low
- 1,25-OH Vit D
- Low
- ALP
- Very high
- PTH
- High
- Calcium
- Normal
- Phosphate
- Very low
- 25-OH Vit D
- Normal
- 1,25-OH Vit D
- Low-normal
- ALP
- High
- PTH
- Normal
- Calcium
- Low
- Phosphate
- Low
- 25-OH Vit D
- Normal
- 1,25-OH Vit D
- Very low
- ALP
- High
- PTH
- High
- Calcium
- Low
- Phosphate
- Low
- 25-OH Vit D
- Normal
- 1,25-OH Vit D
- Very high
- ALP
- High
- PTH
- High
Additional Investigations
- FGF23 level: elevated in X-linked hypophosphatemia and tumor-induced osteomalacia
- Genetic testing: PHEX gene (X-linked hypophosphatemia), CYP27B1 (vitamin D-dependent type I), VDR (type II)
- Renal tubular function: urinary phosphate, amino acids, glucose (Fanconi syndrome)
- Parental vitamin D levels: assess familial risk
Imaging
Radiographic Features
Pathognomonic findings:
- Widened growth plates (greater than 3 mm)
- Loss of sharp zone of provisional calcification
- Frayed, irregular metaphyses - "paintbrush" appearance
- Metaphyseal cupping - concave deformity
- Generalized osteopenia
- Coarsened trabecular pattern
- Cortical thinning
- Bowing deformities (varus/valgus)
- Looser zones in long-standing cases
- Wrists (AP) - distal radius and ulna metaphyses highly sensitive
- Knees (AP) - distal femur, proximal tibia metaphyses
- Chest - rachitic rosary (not usually visible radiographically)
- Long bones - for assessment of bowing severity
- Return of sharp zone of provisional calcification (earliest sign)
- Narrowing of growth plates
- Metaphyseal sclerosis (healing line)
- Improved bone density



Grading Rickets Severity and Healing on Radiographs
The topic's own burosumab EvidenceCards report outcomes as a "Thacher rickets severity total score" (Carpenter) and the "Radiographic Global Impression of Change" (Imel), but the body never explains these radiographic tools - how you actually grade rickets severity and healing.
- The Thacher rickets severity score (grading severity). A validated 10-point radiographic score based on the wrist (distal radius and ulna) and the knee (distal femur and proximal tibia). Each site is graded for the degree of metaphyseal fraying, cupping/concavity and the proportion of the growth plate affected (the wrist contributing up to 4 points and each knee physis up to 3), summing to 0 (normal) to 10 (most severe). It lets you objectively grade a child at baseline and track change - it fell from about 1.9 to under 1 on burosumab in the trials.
- The RGI-C (Radiographic Global Impression of Change - grading healing). A paired-comparison tool in which a blinded radiologist scores the change between baseline and follow-up films (roughly -3 markedly worse to +3 completely healed, 0 = no change). It was the primary endpoint of the burosumab phase 3 trial (+1.9 burosumab vs +0.8 conventional) and captures healing that the severity score alone can miss.
- What "healing" looks like on these scores. Recovery is scored as the return of the sharp zone of provisional calcification (the earliest sign), then narrowing of the widened physis, filling-in of the cupped and frayed metaphysis, and a dense metaphyseal healing line - the same radiographic sequence the topic lists under healing, now quantified.
- Why it matters. Objective scoring underpins the evidence base (drug trials), helps decide how long to treat before considering surgery, and gives a defensible viva answer to "how do you know the rickets is healing?" beyond "the X-ray looks better."
Q: How do you objectively grade rickets severity and healing on radiographs? A: Use the Thacher rickets severity score - a validated 0-10 radiographic score of metaphyseal fraying, cupping and the proportion of physis affected at the wrist (distal radius/ulna) and knee (distal femur/proximal tibia) - to grade severity and track it (it fell to under 1 on burosumab). Grade healing with the Radiographic Global Impression of Change (RGI-C), a blinded paired comparison (about -3 worse to +3 fully healed) that was the burosumab phase 3 primary endpoint. Both follow the healing sequence - return of the provisional calcification zone first, then physeal narrowing and a metaphyseal healing line.
WIDENEDRadiographic Features of Rickets
Hook:Growth plates become WIDENED and irregular in rickets - the classic X-ray finding!
Differential Diagnosis
- Age
- 6-24 months peak
- Biochemistry
- Low vitamin D, high ALP
- X-Ray Features
- Widened, frayed metaphyses, osteopenia
- Age
- Under 2 years
- Biochemistry
- Normal
- X-Ray Features
- Normal growth plates, mild symmetric bowing
- Age
- Under 3 years (infantile) or 8-15 years (adolescent)
- Biochemistry
- Normal
- X-Ray Features
- Beaking of medial tibial metaphysis, fragmented medial epiphysis
- Age
- Variable
- Biochemistry
- Low ALP (diagnostic)
- X-Ray Features
- Widened growth plates, but low ALP distinguishes from rickets
Management
Medical Treatment
Nutritional (Calcipenic) Rickets
- Vitamin D3 (cholecalciferol) 2000-6000 IU daily for 8-12 weeks
- Dose based on severity and age
- Alternative: single dose 50,000-150,000 IU (Stoss therapy)
- Elemental calcium 500-1000 mg daily (divided doses)
- Essential in first 4-6 weeks to prevent hungry bone syndrome
- Calcium, phosphate, ALP at 1, 3, 6 months
- 25-OH vitamin D at 3 months - target greater than 75 nmol/L
- X-rays at 3-6 months - assess healing (return of zone of provisional calcification)
- Vitamin D 400-600 IU daily lifelong
- Dietary calcium 800-1000 mg daily
- Biochemistry normalizes by 3-6 months
- Radiographic healing by 6-12 months
- Spontaneous deformity correction by 12-18 months (if mild-moderate)
Medical optimization is the primary treatment for nutritional rickets.
After initiating vitamin D and calcium replacement, severe rickets can develop profound hypocalcemia and hypophosphatemia as the skeleton avidly takes up minerals. Monitor calcium closely in first 2 weeks. Symptoms: tetany, seizures, carpopedal spasm. Treat with IV calcium gluconate if symptomatic.
Orthopaedic Management
Indications for Surgery
- Residual deformity after medical optimization (12-18 months treatment)
- Mechanical axis deviation greater than 10-15 degrees
- Functional impairment (gait disturbance, pain)
- Progressive deformity despite treatment (especially XLH)
- Active rickets (biochemistry not normalized)
- Age under 2-3 years (spontaneous correction possible)
- Mild deformity (less than 10 degrees) with good function
- Poor compliance with medical treatment
Surgical Options
-
Guided growth (hemiepiphysiodesis):
- Medial or lateral tension band plating (eight-plate)
- Stapling (less commonly used now)
- Allows gradual correction over 12-24 months
- Reversible if overcorrection
- Requires compliant follow-up (every 3-6 months)
-
Corrective osteotomy:
- For severe deformities (greater than 20-30 degrees)
- Proximal tibial or distal femoral osteotomy
- Acute or gradual correction (external fixator)
- Corrective osteotomy (definitive treatment):
- Single-level (proximal tibia or distal femur) for unifocal deformity
- Double-level for multi-apical deformity
- Dome, wedge, or opening/closing wedge osteotomy
- Internal fixation (plate and screws) or external fixator
Pre- and Postoperative Management
- Normalize biochemistry - 25-OH vitamin D greater than 75 nmol/L, normal calcium/phosphate/ALP
- Radiographic evidence of healing - return of zone of provisional calcification
- No active rickets clinically or radiographically
- Continue vitamin D and calcium indefinitely
- Protected weight-bearing for 6-12 weeks (delayed healing in metabolic bone disease)
- Serial radiographs to assess osteotomy healing
- Maintain medical optimization to prevent recurrence
Surgical Technique
Guided Growth (Hemiepiphysiodesis)
Indications
- Growing child with open physes
- Residual deformity greater than 10-15 degrees after medical optimization
- Genu varum or valgum
Eight-Plate Technique
- Position: Supine on radiolucent table
- Fluoroscopy to confirm physis level
- Small incision over target physis (medial for varus, lateral for valgus)
- Position plate straddling physis with 2 screws (one epiphyseal, one metaphyseal)
- Confirm position fluoroscopically
Corrective Osteotomy
- For severe deformity (greater than 30 degrees) or closed physes
- Location: Proximal tibia or distal femur
- Fixation: Plate and screws or external fixator
- Opening or closing wedge based on deformity
Complications
Medical Complications
Acute (Untreated Rickets):
- Tetany - carpopedal spasm, positive Chvostek and Trousseau signs
- Seizures - generalized tonic-clonic (hypocalcemic)
- Laryngospasm - stridor, respiratory compromise
- Cardiac arrhythmias - prolonged QT interval (rare)
IV calcium gluconate 10% 1-2 mL/kg over 10 minutes, cardiac monitoring, airway support if laryngospasm.
- Growth retardation - short stature (may be permanent if untreated)
- Delayed motor milestones - sitting, standing, walking
- Hypotonia - muscle weakness, floppy baby
- Developmental delay (if severe chronic hypocalcemia)
- Dental problems - delayed tooth eruption, enamel hypoplasia, increased caries risk
- Pathologic fractures - metaphyseal fractures with minimal trauma (greenstick, Salter-Harris II)
- Progressive deformities - genu varum/valgum, coxa vara, spinal deformities (scoliosis, kyphosis)
- Slipped capital femoral epiphysis (SCFE) - increased risk in untreated/undertreated rickets
- Craniosynostosis - premature fusion of skull sutures (rare complication)
- Respiratory compromise - severe rachitic rosary causing chest wall deformity
- Cardiomyopathy - dilated cardiomyopathy in severe chronic hypocalcemia (rare)
- Immune dysfunction - vitamin D plays role in immune regulation; increased infection risk
- Muscle weakness - proximal myopathy, waddling gait
- Bone pain - diffuse skeletal pain, difficulty walking
Treatment-Related Complications
- Severe hypocalcemia and hypophosphatemia after initiating vitamin D replacement
- Skeleton avidly takes up minerals once vitamin D replenished
- Risk factors: severe rickets, very high ALP, prolonged deficiency
- Presentation: tetany, seizures within first 2 weeks of treatment
- Prevention: concurrent calcium supplementation, close monitoring (calcium q48h for first 2 weeks)
- Treatment: IV calcium gluconate, increase oral calcium dose
- Hypercalcemia - nausea, vomiting, polyuria, constipation, altered mental status
- Hypercalciuria - nephrocalcinosis, renal stones
- Risk factors: excessive supplementation (greater than 10,000 IU daily for prolonged periods), vitamin D-dependent rickets type I on calcitriol
- Monitoring: serum calcium, urinary calcium/creatinine ratio
- Management: reduce or stop vitamin D, hydration, loop diuretics if severe
- Complication of conventional therapy (oral phosphate + calcitriol)
- Mechanism: hypercalciuria from high-dose calcitriol + phosphate load
- Screening: renal ultrasound annually in children on conventional therapy
- Reduced risk with burosumab (anti-FGF23 therapy)
Surgical Complications
- Most common complication if surgery performed on active rickets
- Risk: recurrence is high when surgery is performed on biochemically uncontrolled rickets, and substantially lower once metabolic control and radiographic healing are established (wait 12-18 months)
- Prevention: confirm biochemical normalization, radiographic healing, adequate treatment duration before surgery
- Management: repeat medical optimization, consider revision surgery only after full healing
- Risk factors: active rickets, inadequate medical optimization, poor compliance with vitamin D
- Management: optimize vitamin D and calcium, bone stimulation, revision surgery if persistent nonunion
- Mechanism: unpredictable correction rate with hemiepiphysiodesis, especially in metabolic bone disease
- Prevention: close follow-up (every 3-6 months), standing alignment radiographs, remove implants promptly when corrected
- Management: observation if mild, contralateral surgery if asymmetric, osteotomy if severe
- Implant fracture - plates/screws in osteopenic bone
- Migration - eight-plate migration in soft bone
- Infection - surgical site infection (standard orthopedic risk)
Long-Term Sequelae
- Permanent short stature - growth potential lost if treated after puberty
- Residual skeletal deformities - bow legs, knock knees, coxa vara requiring adult reconstruction
- Early osteoarthritis - knee (tibial-femoral), hip from malalignment and abnormal loading
- Chronic pain - skeletal deformities causing mechanical pain
- Gait abnormalities - waddling gait, limping
- X-linked hypophosphatemia: often requires multiple surgeries despite good medical control, residual short stature common
- Vitamin D-dependent type II: some patients resistant to all therapy, permanent skeletal changes
- Dental issues: enamel defects from critical period of deficiency persist despite treatment
Immediate assessment and treatment required for:
- Seizures - hypocalcemic seizures are emergencies (IV calcium gluconate)
- Stridor/laryngospasm - airway compromise from tetany (IV calcium, intubation if severe)
- Suspected pathologic fracture - especially metaphyseal fractures (rule out NAI)
- Cardiac arrhythmia - prolonged QT interval (hypocalcemia-induced)
- Severe hypocalcemia (less than 1.8 mmol/L) even if asymptomatic
All children with rickets need baseline ECG if calcium less than 2.0 mmol/L to assess QT interval.
Postoperative Care
Postoperative Protocol
After Guided Growth
- Weight-bearing as tolerated immediately
- No cast or immobilization required
- Follow-up at 6 weeks, then every 3-6 months
- Standing alignment radiographs at each visit
- Continue vitamin D and calcium supplementation
After Osteotomy
- Protected weight-bearing 6-12 weeks (longer than typical due to metabolic bone disease)
- Cast or brace immobilization
- Serial radiographs to assess healing
- Progress weight-bearing based on callus formation
Medical Management
- Continue vitamin D supplementation lifelong
- Maintain calcium intake
- Monitor biochemistry during healing
Outcomes
Treatment Outcomes
Medical Treatment (Nutritional Rickets)
- Biochemistry normalizes: 3-6 months
- Radiographic healing: 6-12 months
- Spontaneous deformity correction: 12-18 months
- Growth catch-up: Variable, better if treated early
Surgical Outcomes
- Guided growth success rate: greater than 90% correction
- Osteotomy union rate: 85-95% (lower than normal bone)
- Recurrence rate after proper optimization: less than 10%
Long-Term Prognosis
- Excellent if treated early and completely
- Full height potential achievable in nutritional rickets
- Hereditary forms require lifelong management
Guidelines, Registries & Global Practice
Global Epidemiology
- Nutritional rickets is a preventable global public health problem that has re-emerged in high-income countries and remains endemic in parts of Africa, the Middle East and South Asia.
- Two distinct geographies of cause: vitamin D-deficiency rickets predominates at high latitude / low sunlight, while dietary calcium-deficiency rickets predominates in sun-rich, low-dairy populations (Pfitzner/Thacher, Nigeria).
- Highest-risk infants worldwide: exclusively breastfed without supplementation, born to vitamin D-deficient mothers, with darkly pigmented skin, or with covering clothing / limited sun exposure.
- X-linked hypophosphataemia is the commonest inherited (non-nutritional) rickets, incidence roughly 1 in 20,000.
Side-by-Side Guideline Comparison
- Core recommendation
- 25-OH D over 50 nmol/L sufficient; treat with vitamin D at least 2000 IU/day for 12+ weeks PLUS calcium 500 mg/day; infants 400 IU/day from birth
- Core recommendation
- All infants/children at least 400 IU/day vitamin D from soon after birth
- Core recommendation
- Routine infant supplementation; "Healthy Start" vitamins; treat deficiency, fortify staple foods
- Core recommendation
- Higher treatment/maintenance doses acceptable; targets 25-OH D over 75 nmol/L in at-risk groups
High- vs Limited-Resource Practice
- High-resource: ready 25-OH D / FGF23 / genetic testing, multidisciplinary metabolic bone clinics, and access to burosumab for XLH.
- Limited-resource: diagnosis often clinical/radiographic; treatment relies on affordable cholecalciferol and dietary calcium (calcium-deficiency rickets is frequently missed if only vitamin D is treated). Food fortification (milk, flour) is the key population-level strategy.
Why the Deformity Pattern Changes with Age
The three age tabs state that infants show craniotabes, toddlers develop genu varum, and older children develop genu valgum or a windswept deformity - but the topic never explains why the deformity pattern changes with age.
- Rickets amplifies the age-appropriate physiological alignment. Normal tibiofemoral alignment evolves: infants are physiologically varus, passing through neutral at around 18-24 months, reaching peak physiological valgus at about 3-4 years, then settling to the adult angle by roughly 7 years. Because rickets softens the metaphysis and physis so the bone deforms under load, it exaggerates whatever alignment prevails at the age of peak disease activity - hence genu varum in the walking toddler (deforming during the physiological-varus phase) and genu valgum in the older child (deforming during the physiological-valgus phase).
- Windswept deformity (varus in one limb, valgus in the other) reflects asymmetric loading and growth on top of the same soft-bone mechanism.
- The worst change is at the fastest-growing, most-loaded physes. The florid metaphyseal fraying and cupping cluster around the knee (distal femur, proximal tibia) and the wrist (distal radius) - the physes contributing most to longitudinal growth - which is exactly why these are the best radiographs for diagnosis and scoring.
- Practical consequence. The direction of the deformity does not change the medical treatment, but it shapes the surgical plan (which physis to tether in guided growth - medial for varus, lateral for valgus) and is a reminder that a young child's mild symmetric bowing may still be physiological, so the biochemistry and the metaphyseal appearance, not the bowing alone, make the diagnosis.
Q: Why do toddlers with rickets get bow legs but older children get knock knees? A: Rickets softens bone so it deforms under load, exaggerating the age-appropriate physiological alignment. Normal alignment runs from infant varus → neutral at ~18-24 months → peak valgus at ~3-4 years → adult angle by ~7 years, so a child deforming as a walking toddler bows into genu varum, while one deforming later bows into genu valgum (or a windswept pattern with asymmetric loading). The most florid metaphyseal change is at the fastest-growing physes (knee and wrist), which is why those films are used for diagnosis - and the deformity direction guides which physis to tether at guided growth.
Controversies & Areas of Uncertainty
There is no universal agreement on the ideal 25-OH D threshold. The Global Consensus sets sufficiency at over 50 nmol/L, while the Endocrine Society and some surgeons target over 75 nmol/L peri-operatively. Routine high-dose supplementation in vitamin D-replete populations has not shown skeletal benefit and risks hypercalciuria.
In sun-rich, low-dairy regions, rickets is driven by dietary calcium deficiency with normal vitamin D. Treating with vitamin D alone in these children is ineffective - yet calcium-only versus combined regimens, and the exact calcium dose, remain debated.
Burosumab is superior to conventional therapy in trials, but long-term safety, cardiovascular/ectopic-mineralisation outcomes, optimal start age and lifelong duration are unresolved, and cost restricts access. When to switch a stable child on conventional therapy is not standardised.
The "wait 12-18 months" rule is expert consensus, not trial-derived. The threshold deformity for surgery, guided growth versus osteotomy in XLH (where correction is slower and overcorrection/repeat procedures are common, Grote 2023), and rebound after implant removal all remain areas of genuine uncertainty.
State the principle and the evidence level rather than a false-precision number: "Medical optimisation before surgery is consensus-based; recurrence is high in uncontrolled disease and low after metabolic control." Acknowledge that calcium and vitamin D thresholds differ between guidelines and that burosumab's long-term role is still being defined. Examiners reward candidates who distinguish established evidence from convention.
MCQ Practice Points
Q: A child presents with rickets. Biochemistry shows normal calcium, very low phosphate (0.4 mmol/L), normal 25-OH vitamin D, and elevated alkaline phosphatase. What is the most likely diagnosis? A: X-linked hypophosphatemia (XLH). The key distinguishing features are normal vitamin D but severe hypophosphatemia. Nutritional rickets would have low vitamin D. XLH is caused by PHEX gene mutation leading to elevated FGF23, which causes renal phosphate wasting.
Q: What is the earliest radiographic sign of rickets healing after initiating vitamin D treatment? A: Return of the sharp zone of provisional calcification at the metaphysis. This appears within 2-4 weeks of adequate treatment. Subsequently, the growth plate narrows, metaphyseal cupping improves, and a dense metaphyseal healing line appears.
Q: A 12-month-old with active nutritional rickets and severe genu varum is referred for orthopedic management. What is the appropriate initial treatment? A: Medical optimization with vitamin D and calcium replacement, NOT surgery. Active rickets must be treated medically first. Vitamin D 2000-4000 IU daily for 8-12 weeks plus calcium supplementation. Surgical correction (if needed) only after biochemical normalization and 12-18 months of treatment. Many deformities correct spontaneously with medical therapy alone.
Q: When is surgical correction indicated for rickets-related deformities? A: After medical optimization (12-18 months treatment, biochemistry normalized) AND residual deformity greater than 10-15 degrees with functional impairment. Never operate on active rickets - very high recurrence rate. Guided growth (hemiepiphysiodesis) preferred in growing children; corrective osteotomy after skeletal maturity.
Q: What is hungry bone syndrome in rickets and how do you prevent it? A: Severe hypocalcemia and hypophosphatemia occurring in the first 2 weeks after initiating vitamin D treatment. The skeleton avidly takes up minerals once vitamin D is replenished. Prevention: give concurrent calcium supplementation (500-1000 mg daily) and monitor calcium closely (every 48 hours for first 2 weeks). Treatment: IV calcium gluconate if symptomatic (tetany, seizures).
Q: How do you distinguish X-linked hypophosphatemia from nutritional rickets? A: Key differences: (1) XLH has normal calcium and vitamin D but very low phosphate; nutritional rickets has low vitamin D and low-normal calcium/phosphate. (2) XLH shows X-linked dominant inheritance (family history); nutritional is environmental. (3) XLH persists despite vitamin D supplementation; nutritional improves rapidly. (4) Confirm XLH with elevated FGF23 and PHEX gene testing.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-month-old toddler presents with delayed walking and bow legs. Parents are vegan and the child is exclusively breastfed. Examination shows widened wrists and ankles, rachitic rosary, and bilateral genu varum. X-rays show widened, frayed metaphyses at wrists and knees. Blood tests show calcium 2.0 mmol/L, phosphate 0.9 mmol/L, alkaline phosphatase 650 U/L, 25-OH vitamin D 15 nmol/L. What is your diagnosis and management?”
“A 4-year-old boy presents with progressive bow legs and short stature. He has been on vitamin D supplementation since infancy without improvement. Family history reveals his mother and maternal grandfather had similar leg deformities. X-rays show active rickets changes and severe genu varum. Biochemistry shows normal calcium (2.3 mmol/L), low phosphate (0.5 mmol/L), normal 25-OH vitamin D (60 nmol/L), high alkaline phosphatase (400 U/L). What is your diagnosis and how do you manage this?”
“A 6-year-old girl with treated nutritional rickets (now biochemistry normal) has residual bilateral genu varum (mechanical axis deviation 20 degrees). Parents are requesting surgical correction. How do you assess and manage this?”
Key Pathophysiology
- Defective mineralization of growth plate (physis) and osteoid in children
- Accumulation of unmineralized hypertrophic cartilage - widened growth plates
- Unlike osteomalacia (adults), rickets affects endochondral ossification
- Peak age 6-24 months (nutritional), older children (hereditary forms)
Classic Presentation (RICKETS)
- Rachitic rosary (costochondral swelling)
- Increased wrist and ankle size (widened metaphyses)
- Craniotabes (soft skull in infants)
- Knock knees or bow legs (genu valgum/varum)
- Epiphyseal widening on X-ray
- Tetany if severe hypocalcemia
- Short stature and growth delay
Biochemistry by Type
- Nutritional: low Ca/vitamin D, high ALP, low-normal PO4
- X-linked hypophosphatemia: normal Ca/vitamin D, very low PO4, high FGF23
- Vitamin D-dependent type I: low Ca, normal 25-OH D, very low 1,25-OH D
- Vitamin D-dependent type II: low Ca, normal 25-OH D, very high 1,25-OH D (receptor resistance)
X-Ray Hallmarks
- Widened, irregular, frayed metaphyses (paintbrush appearance)
- Loss of sharp zone of provisional calcification
- Metaphyseal cupping (concave deformity)
- Generalized osteopenia, bowing deformities
- Best views: wrists (AP), knees (AP)
Treatment Protocol
- Nutritional rickets: Vitamin D 2000-6000 IU daily for 8-12 weeks + calcium 500-1000 mg daily
- Maintenance: 400-600 IU daily lifelong
- X-linked hypophosphatemia: Burosumab (first-line) or phosphate 20-60 mg/kg/day + calcitriol
- Monitor: calcium/PO4/ALP at 1,3,6 months; X-rays at 3-6 months for healing
Surgical Pearls
- Medical optimization FIRST - never operate on biochemically active rickets (high recurrence)
- Wait 12-18 months after biochemical normalization for spontaneous correction
- Surgical indications: residual deformity greater than 10-15 degrees after 12-18 months treatment
- Guided growth (hemiepiphysiodesis) preferred in growing children
- Corrective osteotomy after skeletal maturity or if very severe deformity
- Continue vitamin D supplementation lifelong to prevent recurrence
Evidence Base and Key Studies
Global Consensus Recommendations on Nutritional Rickets
- GRADE-based consensus of 33 experts from 11 international scientific organizations - the global reference standard
- Defines nutritional rickets diagnostically as a combination of clinical, biochemical and radiographic abnormality
- Vitamin D sufficiency defined as 25-OH D over 50 nmol/L; deficiency under 30 nmol/L; insufficiency 30-50 nmol/L
- Treatment: minimum 2000 IU/day vitamin D for at least 12 weeks PLUS calcium 500 mg/day (dietary or supplement)
- Universal infant supplementation 400 IU/day from birth; food fortification advocated to eradicate rickets
Dietary Calcium Deficiency Causes Rickets Without Vitamin D Deficiency
- Cross-sectional study of 218 Nigerian children aged 6-35 months in a region where rickets is endemic
- NO child had 25-OH D under 10 ng/mL - vitamin D deficiency was absent in this sunny equatorial population
- 9.2% had clinical rickets; affected children had lower serum calcium (9.1 vs 9.4 mg/dL) but similar 25-OH D
- Children with and without rickets had no difference in vitamin D levels
- Landmark evidence that dietary calcium insufficiency alone can cause rickets
Prevention of Rickets and Vitamin D Deficiency (AAP Clinical Report)
- AAP clinical report: all infants, children and adolescents need a minimum 400 IU/day vitamin D from soon after birth
- Replaced the prior 200 IU/day recommendation based on new clinical trial evidence
- Exclusively breastfed infants at highest risk - human milk is a poor source of vitamin D
- Adequate sunlight cannot be reliably assumed and carries skin-cancer risk, so supplementation is advised universally
Burosumab vs Conventional Therapy in Children with XLH (Phase 3 RCT)
- Randomised (1:1), active-controlled, open-label phase 3 trial; 61 children aged 1-12 with XLH (29 burosumab, 32 conventional)
- Primary endpoint (Radiographic Global Impression of Change at week 40): +1.9 burosumab vs +0.8 conventional (difference 1.1, 95% CI 0.8-1.5, p under 0.0001)
- Burosumab produced greater improvement in rickets severity, growth and biochemistry than continued phosphate plus calcitriol
- Treatment-related adverse events more frequent with burosumab (59% vs 22%); serious events few and unrelated
Burosumab Improves Rickets, Phosphate and Growth in Children with XLH (Phase 2)
- Open-label phase 2 trial; 52 children with XLH randomised to burosumab every 2 vs every 4 weeks
- Mean Thacher rickets severity score fell from 1.9 to 0.8 (every 2 weeks) by week 40, sustained to week 64
- Over half of children reached normal serum phosphorus by week 6; tubular phosphate reabsorption and growth improved
- Mean serum alkaline phosphatase fell from 459 to 369 U/L; pain and physical function improved
Guided Growth for Lower Limb Deformity in Hypophosphataemic Rickets
- Retrospective series of guided growth (hemiepiphysiodesis) for coronal-plane knee deformity in X-linked hypophosphataemic rickets
- Indication: mechanical axis in Zone 2-3 despite one year of optimised medical treatment; mean age 10.3 years
- Neutral mechanical axis restored in 16/23 (70%) limbs; only one segment needed osteotomy for residual deformity; one recurrence
- Children with at least 3 years growth remaining responded significantly better (p=0.004); valgus corrected better than varus (p=0.007)