The Tailor's Muscle
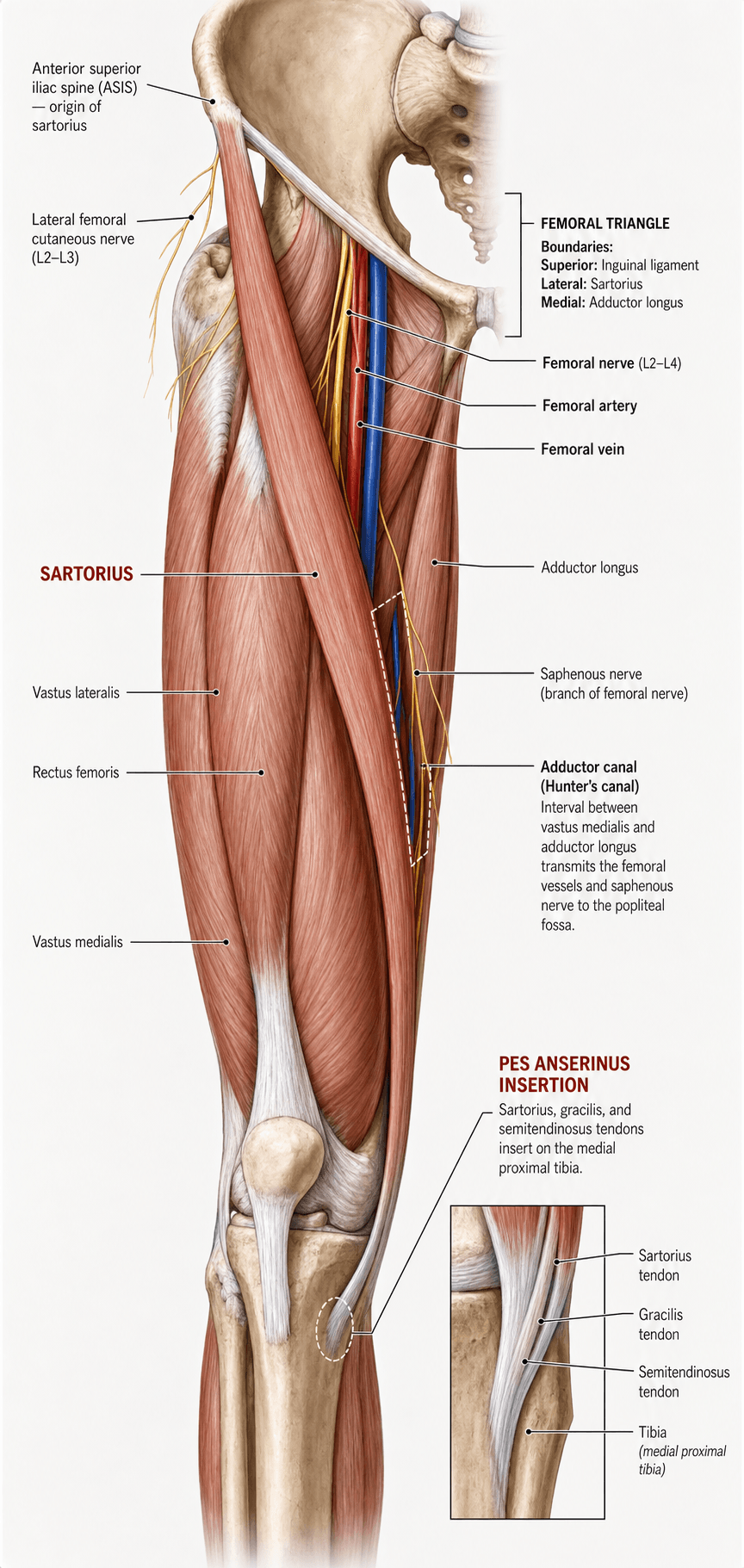
- Originates from the ASIS (Anterior Superior Iliac Spine).
- Inserts onto the Proximal Medial Tibia (Pes Anserinus).
- Longest muscle in the human body.
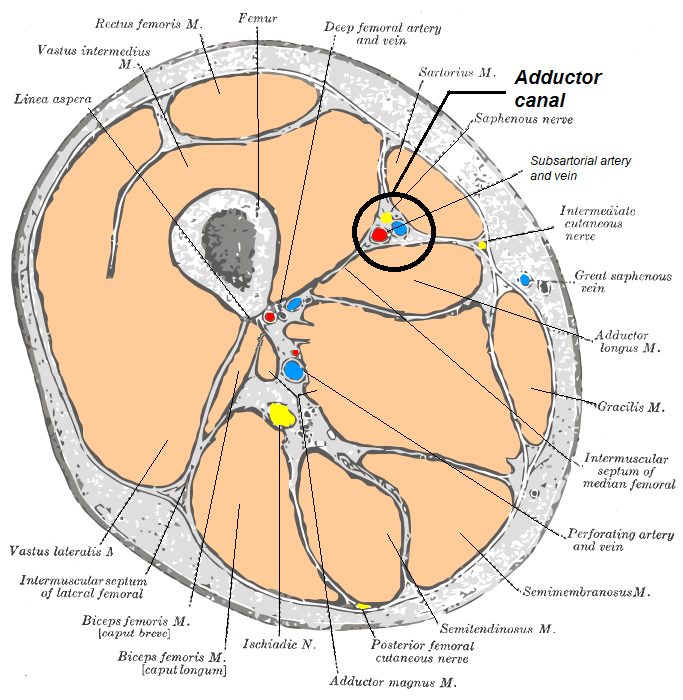
- Forms the ROOF of the Adductor (Hunter's) Canal.
- Innervated by the Femoral Nerve (L2, L3).
- “The Sartorius is the lateral border of the Femoral Triangle and the medial border of the proximal thigh compartments.
- “It crosses TWO joints (Hip and Knee), acting on both.
- “Pes Anserinus ('Goose's Foot') receives innervation from three different nerves (Femoral, Obturator, Sciatic).
- “The Saphenous Nerve exits the Adductor Canal between the Sartorius and Gracilis.
Iatrogenic Injury.
- Runs deep to the Sartorius in the Adductor Canal.
- Pierces the fascia lata between Sartorius and Gracilis to become subcutaneous.
- Risk: Identifying the interval incorrectly during hamstring harvest or medial knee approaches can transect the nerve.
- Result: Numbness/Neuroma on medial leg.
Origin Relation.
- Passes medial (or sometimes through) the origin of Sartorius at the ASIS.
- Risk: Smith-Petersen approach or ASIS graft harvest.
- Consequence: Meralgia Paresthetica (Lateral thigh numbness).
- Sartorius
- ASIS
- Gracilis
- Pubis
- Semitendinosus
- Ischial Tuberosity
- Sartorius
- Femoral (L2/3)
- Gracilis
- Obturator (L2/3)
- Semitendinosus
- Sciatic (Tibial L5/S1/2)
- Sartorius
- Pes (Anterior)
- Gracilis
- Pes (Middle)
- Semitendinosus
- Pes (Posterior)
- Sartorius
- Flex/Abd/ER Hip + Flex Knee
- Gracilis
- Adduct Hip + Flex Knee
- Semitendinosus
- Extend Hip + Flex Knee
SGTPes Anserinus Order
Hook:Say Grace before Tea. (Anterior to Posterior).
FABERAction (Tailor's Position)
Hook:The position a tailor sits in (cross-legged).
SAILFemoral Triangle
Hook:Sartorius sets SAIL for the knee.
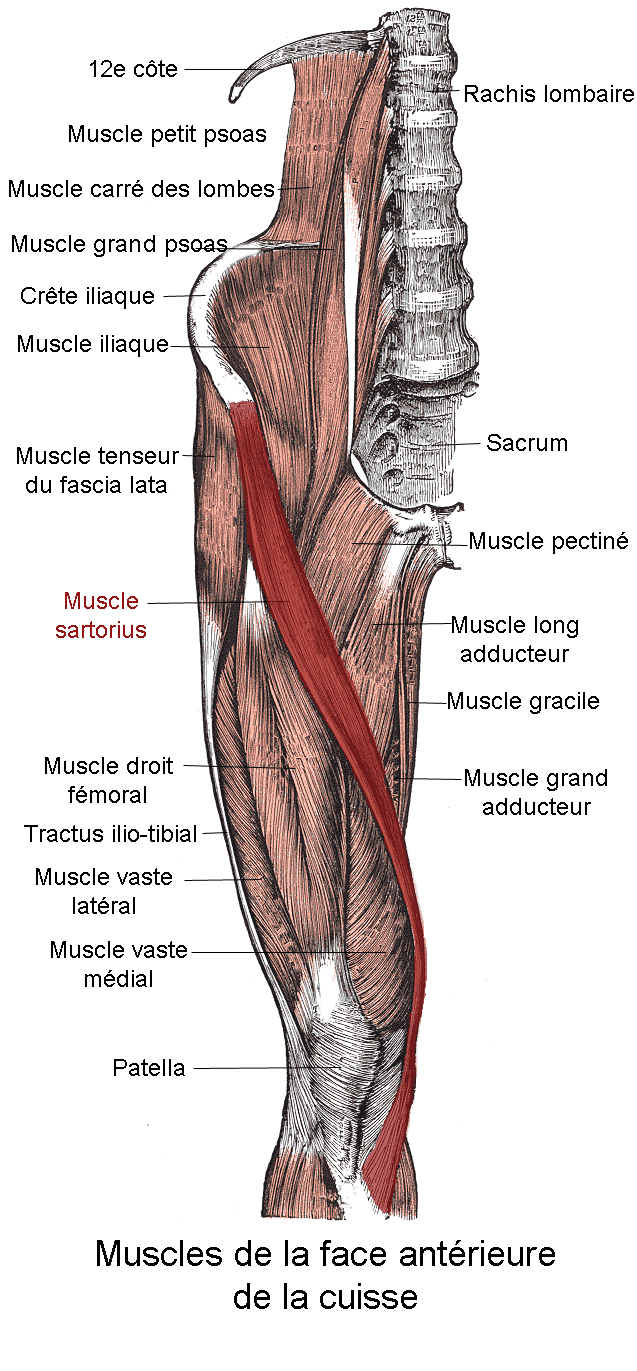
Overview
The Sartorius is a unique, strap-like muscle that spirals obliquely across the anterior thigh. It is the longest muscle in the human body, with long parallel fascicles giving it a large excursion but relatively modest force. Its name derives from the Latin sartor (tailor), referencing the cross-legged sitting position (flexion, abduction, external rotation) that tailors traditionally adopted while working.
For the exam candidate, the Sartorius matters far more for its topographical relationships than for its (largely redundant) motor function:
- It is the lateral border of the femoral triangle and the roof of the adductor (subsartorial / Hunter's) canal — making it the surface landmark for the femoral artery and the saphenous nerve.
- Its distal insertion forms the most superficial / anterior limb of the pes anserinus, the site of pes anserine bursitis and the working layer during hamstring (gracilis/semitendinosus) graft harvest.
- Its proximal origin from the ASIS is the apophysis avulsed by sprinting adolescents.
These three "danger and landmark" zones — origin (ASIS), roof of the canal, and pes insertion — are the high-yield core of every Sartorius viva.
Neurovascular
Origin
- ASIS: Anterior Superior Iliac Spine.
- Notch: Also attaches to the upper half of the notch immediately below the ASIS.
Course
- Runs obliquely across the upper and middle thirds of the thigh.
- Moves from Lateral (ASIS) to Medial (Tibia).
- Spirals around the medial aspect of the thigh to reach the posterior aspect of the medial condyle, then curves forward.
Insertion
- Pes Anserinus: Upper part of the medial surface of the tibia.
- Arrangement: Inserts ANTERIOR and SUPERIOR to the Gracilis and Semitendinosus.
- Expansion: Sends an expansion to the capsule of the knee joint and crural fascia.
The canal the sartorius roofs runs from the apex of the femoral triangle to the adductor hiatus - a gap in the tendinous femoral insertion of adductor magnus. Knowing what does and does not pass through the hiatus is the high-yield exit anatomy:
- The femoral artery and vein pass through the hiatus and are renamed the popliteal artery and vein as they enter the popliteal fossa - the canal is the conduit carrying the main vessels from the anterior thigh to the back of the knee.
- The saphenous nerve does NOT pass through the hiatus - it leaves the canal by piercing the roof (emerging between sartorius and gracilis) to become subcutaneous and supply the medial leg down to the medial malleolus.
- The nerve to vastus medialis leaves more proximally to enter its muscle, and the descending genicular artery branches off near the hiatus to supply the knee.
So the hiatus is an arterio-venous exit only; the nerves have already left the canal. This is why an adductor canal block is essentially a sensory (saphenous) block, and why vascular surgeons reach the femoro-popliteal segment through this sartorius-roofed interval.
Surface Anatomy
Palpation
- Origin: Easily palpable at the ASIS.
- Belly: Can be made prominent by asking the patient to lift the heel and cross the legs (FABER position).
- Adductor Canal: The muscle belly is the guide. The pulse of the femoral artery can be felt DEEP to the sartorius in the mid-thigh.
Surgical Marking
- A line from ASIS to the Medial Femoral Condyle approximates the course.
- The upper 1/3 forms the lateral border of the femoral triangle.
- The middle 1/3 covers the Hunter's Canal.
Identifying the medial border of the Sartorius is the key step in the anterior approach to the Femoral Artery.
Pathology: Pes Anserine Bursitis
Pathophysiology
- Inflammation: Of the bursa lying between the Pes Anserinus insertion and the MCL/Tibia.
- Causes: Overuse (Runners), Tight hamstrings, Obesity, Valgus deformity (Osteoarthritis).
- Association: Strongly associated with early OA of the medial compartment.
The term "Cyclist's Knee" generally refers to ITB, but "Breaststroker's Knee" can involve the Pes Anserinus (or MCL).
Differential Diagnosis of Medial Knee Pain
The single most examined skill here is distinguishing pes anserine pathology from the other causes of medial-sided knee pain by anatomical localisation of tenderness.
- Tenderness Location
- 2-3 cm distal to medial joint line, over proximal tibia
- Key Discriminator
- Below the joint line; negative valgus stress and McMurray
- First-Line Test
- Ultrasound (fluid deep to SGT)
- Tenderness Location
- Medial joint LINE
- Key Discriminator
- Positive McMurray; mechanical locking/catching
- First-Line Test
- MRI
- Tenderness Location
- Along the MCL (femoral/tibial attachment)
- Key Discriminator
- History of valgus trauma; pain on valgus stress
- First-Line Test
- Clinical + stress radiograph
- Tenderness Location
- Diffuse medial joint line
- Key Discriminator
- Crepitus, age, radiographic joint-space loss
- First-Line Test
- Weight-bearing radiograph
- Tenderness Location
- Diffuse medial, often nocturnal
- Key Discriminator
- Sudden severe pain in older patient; normal early radiograph
- First-Line Test
- MRI (subchondral oedema)
- Tenderness Location
- Proximal medial tibia
- Key Discriminator
- Insidious load-related pain in runner; positive bone scan/MRI
- First-Line Test
- MRI
- Tenderness Location
- Medial leg distal to canal
- Key Discriminator
- Burning/numbness, Tinel sign; prior medial surgery
- First-Line Test
- Diagnostic nerve block
Classification Systems
Coxa Saltans (Snapping Hip) Classification
Sartorius pathology fits into the external/extra-articular types.
- External Type:
- Iliotibial Band (ITB): Most common. Snaps over Greater Trochanter.
- Gluteus Maximus: Anterior fibers snapping over GT.
- Internal Type:
- Iliopsoas: Snaps over Iliopectineal eminence or femoral head.
- Rare Variants:
- Sartorius: Snapping over the ASIS or AIIS (rare).
- Biceps Femoris: Long head snapping over Ischial Tuberosity.
Although Sartorius snapping is rare, it must be considered in athletes with anterior hip snapping that mimics intra-articular pathology.
Clinical Assessment
Patrick's Test.
- Position: Flexion, Abduction, External Rotation (Figure-4).
- Action: Engages the Sartorius.
- Pain: Anterior groin pain may indicate hip pathology or Iliopsoas/Sartorius strain. Posterior pain indicates SI Joint.
Medial Knee Pain.
- Palpate 2-3cm distal to the medial joint line.
- Tenderness: Suggests Pes Anserine Bursitis.
- Differentiate: Joint line tenderness (Meniscus) vs Tibial tenderness (Stress fracture) vs Pes tenderness (Bursitis).
Muscle Testing
- Resistance: Resisted flexion and external rotation of the hip.
- Grading: MRC Scale 0-5.
- Weakness: Often subtle as other muscles compensate (Iliopsoas for flexion, Glutes for abduction).
Investigations
X-Ray
- AP/Lat Knee: Usually normal for bursitis. Assessing for OA (Osteophytes) or Stress Fracture (proximal tibia).
- Proximal Tibia Exostosis: Can irritate the overlying SGT tendons.
Ultrasound
- Diagnostic: Shows fluid filled bursa deep to SGT tendons.
- Guided Injection: Target for corticosteroid injection.
MRI
- Gold Standard.
- Shows local inflammation, tendonitis, or bursitis.
- Excludes meniscal tears or subchondral insufficiency fractures.
MRI is particularly useful to rule out a subtle tibial stress fracture in runners.
Management Strategy
Treatment Protocol
- Action
- RICE, NSAIDs
- Goal
- Reduce inflammation
- Action
- Physiotherapy (Hamstring stretching)
- Goal
- Reduce tension
- Action
- Corticosteroid Injection
- Goal
- Therapeutic
- Action
- Bursectomy (Rare)
- Goal
- Last resort
- Physiotherapy: Focus on correcting Valgus mechanics and stretching tight adducts/hamstrings.
- Injection: Highly effective. Must be placed into the bursa, avoiding the tendon substance.
Ultrasound guidance significantly improves the accuracy of bursal injections compared to landmark-based techniques.
Surgical Technique
Pes Anserinus Harvest (ACL)
- Incision: Vertical, medial to tibial tubercle.
- Sartorius Fascia: Incise the fascia in line with the Sartorius fibers (or L-shaped incision).
- Exposure: Reflect Sartorius fascia to reveal Gracilis and Semitendinosus deep to it.
- Preservation: Usually Sartorius is PRESERVED and repaired over the tunnels.
The Sartorius acts as the "Check Rein" or covering layer. Meticulous repair of the sartorius fascia prevents hematoma formation and assists with healing.
Complications
- Saphenous Nerve Neuralgia: Numbness or pain on medial leg/foot.
- Hematoma: Rich blood supply from segmental arteries.
- Muscle Rupture: Rare, usually at origin (ASIS avulsion in sprinters).
- Knee Instability? Sartorius plays a negligible role in stability compared to MCL/ACL.
The ASIS (sartorius) avulsion is one node in a classic adolescent-athlete map - examiners expect you to match each apophysis to its muscle, because the unfused apophysis is the weak link before physeal closure:
- ASIS to sartorius (and tensor fasciae latae) - sprinting.
- AIIS to rectus femoris (straight/direct head) - kicking.
- Ischial tuberosity to the hamstrings (the commonest and most troublesome) - sprinting, hurdling, the splits.
- Lesser trochanter to iliopsoas - resisted hip flexion. In a child a lesser-trochanter avulsion is essentially an apophyseal injury; in an adult an apparently "spontaneous" lesser-trochanter avulsion should raise suspicion of underlying metastatic bone disease.
- Iliac crest to the abdominal wall / oblique muscles - a sudden trunk twist.
- Pubic symphysis / ramus to the adductors - kicking and change of direction.
Most heal non-operatively; fixation is reserved for large displacement (commonly cited threshold around 2 to 3 cm) or a symptomatic ischial-tuberosity non-union.
Rehabilitation Protocol
- Bursitis: Relative rest for 2-4 weeks. Eccentric loading not typically emphasized as much as Achilles/Patella.
- Harvest: As per ACL protocol. Hamstring strength may be reduced (Sartorius contribution is minimal).
- ASIS Avulsion: Conservative management (crutches) for 4 weeks. Surgery only for large displacement (greater than 2-3cm).
Prognosis
- Bursitis: Excellent prognosis with conservative care. Check for underlying OA.
- Avulsion: Good return to sport (sprinting) after 3-4 months.
- Transfer: Sartorius transfer (for Quadriceps paralysis) has poor power generation but provides some active flexion.
Guidelines, Registries & Global Practice
Global Epidemiology
- Pes anserine pain syndrome is a common cause of medial knee pain in middle-aged and older adults, with a clear female predominance; community surveys (Mexican COPCORD data) place anserine bursitis among the more frequent regional rheumatic pain syndromes (~0.34% prevalence).
- ASIS apophyseal avulsions cluster in adolescent athletes (mean age ~14-15 years), the ASIS accounting for roughly a third of pelvic apophyseal avulsions, the anterior inferior iliac spine being the commonest.
Side-by-Side Guidance (where recommendations differ)
- Position
- Hamstring (gracilis/semitendinosus) and BPTB both endorsed; surgeon/patient-specific selection
- Source / Society
- AAOS ACL Clinical Practice Guideline (US)
- Position
- Registry data inform graft and fixation choice and revision risk
- Source / Society
- NLR (Norwegian) & Swedish/Danish ACL registries
- Position
- Multimodal, opioid-sparing regional analgesia; motor-sparing blocks favoured to enable rapid recovery
- Source / Society
- PROSPECT / ERAS arthroplasty consensus
- Position
- Preferred over femoral nerve block for quadriceps-sparing analgesia after TKA
- Source / Society
- Level 1 RCT evidence (Jaeger 2013)
- Position
- Non-operative for minimally displaced; ORIF for large/displaced fragments or failed conservative care
- Source / Society
- International case-series consensus
Registry Notes
- Although the Sartorius itself is not implanted, national ACL registries (Scandinavian, UK, and others) track the hamstring grafts harvested through the sartorius layer, informing graft survival, re-rupture and revision rates that guide graft selection globally.
High- vs Limited-Resource Practice Variation
- Adductor canal block depends on ultrasound availability; in high-resource settings it is routine for TKA, whereas landmark-based femoral nerve blocks or systemic analgesia may dominate where ultrasound is scarce.
- Pes anserine bursitis is largely a clinical diagnosis worldwide; MRI/ultrasound confirmation is reserved for atypical cases or where stress fracture/SIFK must be excluded - imaging access varies markedly by setting.
- ASIS avulsion is managed conservatively in the great majority of cases everywhere, which keeps treatment robust to resource constraints; operative fixation is selective.
Controversies & Areas of Uncertainty
The term "pes anserine bursitis" is increasingly questioned. Imaging frequently shows tendinopathy of the SGT insertion without a distended bursa, and some authors prefer "pes anserinus pain syndrome." The bursa is often anatomically inconstant.
Classic teaching links it to obesity, diabetes and medial OA. The case-control evidence (Alvarez-Nemegyei) found no association with those factors and instead implicated valgus alignment and collateral instability - a mechanical rather than metabolic model.
Corticosteroid relieves symptoms short-term, but high-quality comparative data are scarce and concerns about tendon weakening persist. The roles of PRP, hyaluronic acid and ultrasound versus landmark guidance for the injection remain unresolved.
Debate continues over the true proximal/distal boundary of the canal, whether the block is "adductor canal" versus "subsartorial femoral triangle," and how much spread to the obturator/nerve-to-vastus-medialis contributes to analgesia and to any residual quadriceps weakness.
MCQ Practice Points
Q: The Sartorius muscle is innervated by which nerve? A: Femoral Nerve.
Q: Which muscle forms the most anterior part of the Pes Anserinus? A: Sartorius. (SGT order).
Q: Which structure forms the roof of the Adductor Canal? A: Sartorius.
Q: Which muscle acts to flex, abduct, and externally rotate the hip? A: Sartorius.
Q: An avulsion fracture of the ASIS involves the origin of which muscle? A: Sartorius. (Rectus Femoris is AIIS).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the anatomy of the Pes Anserinus.”
“What forms the roof of the Adductor Canal and what structures are at risk during investigation?”
“A 60F with medial knee pain. X-ray shows mild medial OA. She has exquisite tenderness 3cm distal to the joint line. Diagnosis?”
“You are harvesting gracilis and semitendinosus for an ACL reconstruction. How do you find the tendons, and what nerve is at risk?”
“A patient develops burning numbness over the lateral thigh after an anterior approach to the hip. Which nerve, and how does it relate to the Sartorius?”
Anatomy
- Origin: ASIS
- Insert: Pes Anserinus
- Nerve: Femoral (L2/3)
- Longest muscle
Relationships
- Roof of Hunter's Canal
- Lat border Femoral Triangle
- Saphenous N runs deep
- SGT: Sartorius, Gracilis, SemiT
Clinical
- Action: FABER
- Pathology: Pes Bursitis
- Hazard: ASIS Avulsion
- Block: Adductor Canal
Evidence Base
Pes Anserinus & Anserine Bursa: Cadaveric Anatomy
- 86 legs from 45 cadavers: Sartorius inserts into the superficial layer; Gracilis and Semitendinosus into the deep layer of the medial tibia
- Semitendinosus had a single tendon in 66%, two in 31%, three in 3% - confirming variable banding
- Anserine bursa is irregularly circular and follows the line of the Sartorius
- Recommended landmark injection: ~20 mm medial and 12 mm superior to the inferomedial point of the tibial tuberosity, 15-20 mm deep
Pes Anserinus Tendon Arrangement: Surgical Variations
- 60 limbs from 30 cadavers: in every specimen only THREE muscles (sartorius, gracilis, semitendinosus) formed the pes anserinus
- Despite the constant three-muscle composition, the disposition and interconnection of the tendons varied considerably
- Reinforces the S-G-T anterior-to-posterior order relevant to hamstring graft harvest
Adductor Canal Block Preserves Quadriceps Strength (Volunteers)
- Randomised, double-blind, placebo-controlled crossover in healthy volunteers (11 analysed)
- Quadriceps strength fell only 8% from baseline with adductor canal block versus 49% with femoral nerve block
- Adductor canal block preserved ambulation ability better than femoral nerve block
- Confirms the canal block is predominantly a SENSORY blockade (saphenous nerve), with the Sartorius as the roof/sonic landmark
Adductor Canal Block vs Femoral Nerve Block after TKA
- Randomised, double-blind trial in TKA patients (48 analysed)
- Quadriceps strength was 52% of baseline with adductor canal block versus only 18% with femoral nerve block (p=0.004)
- No significant difference in morphine consumption or pain scores between groups
- Translates the volunteer findings into a clinical arthroplasty population
Risk Factors for Pes Anserinus Tendinitis/Bursitis
- Case-control study (22 cases, 38 controls), all mature women
- Valgus knee deformity was the dominant risk factor (OR 5.2; 95% CI 1.1-25.5), rising to OR 6.0 with collateral instability
- Contrary to common teaching, NO association was found with diabetes, knee osteoarthritis or obesity in this cohort
- Suggests altered medial mechanics, not metabolic factors, drive the syndrome
Operative Outcomes of Pelvic Apophyseal (incl. ASIS) Avulsions
- 32 young athletes (mean 16.8 years) treated operatively for pelvic apophyseal avulsions, including ASIS (Sartorius origin)
- Over 80% returned to pre-injury sport after surgery
- Large displacement (over 20 mm) or delayed (over 3 months) surgery was NOT associated with inferior outcomes
- Most avulsions are still managed non-operatively; surgery is reserved for large/displaced fragments or failed conservative care
Sartorius Transposition Flap for Femoral Vessel Coverage
- States the sartorius muscle transposition flap is the TRADITIONAL method of covering the femoral vessels after inguinal lymphadenectomy
- Limitations of the sartorius flap: thin at its insertion, intimately related to several nerves, and contained within the field in an irradiated groin
- Describes the gracilis flap as a viable alternative when the sartorius lies within prior radiation