MCP, PIP, and CMC joint replacement for arthritis
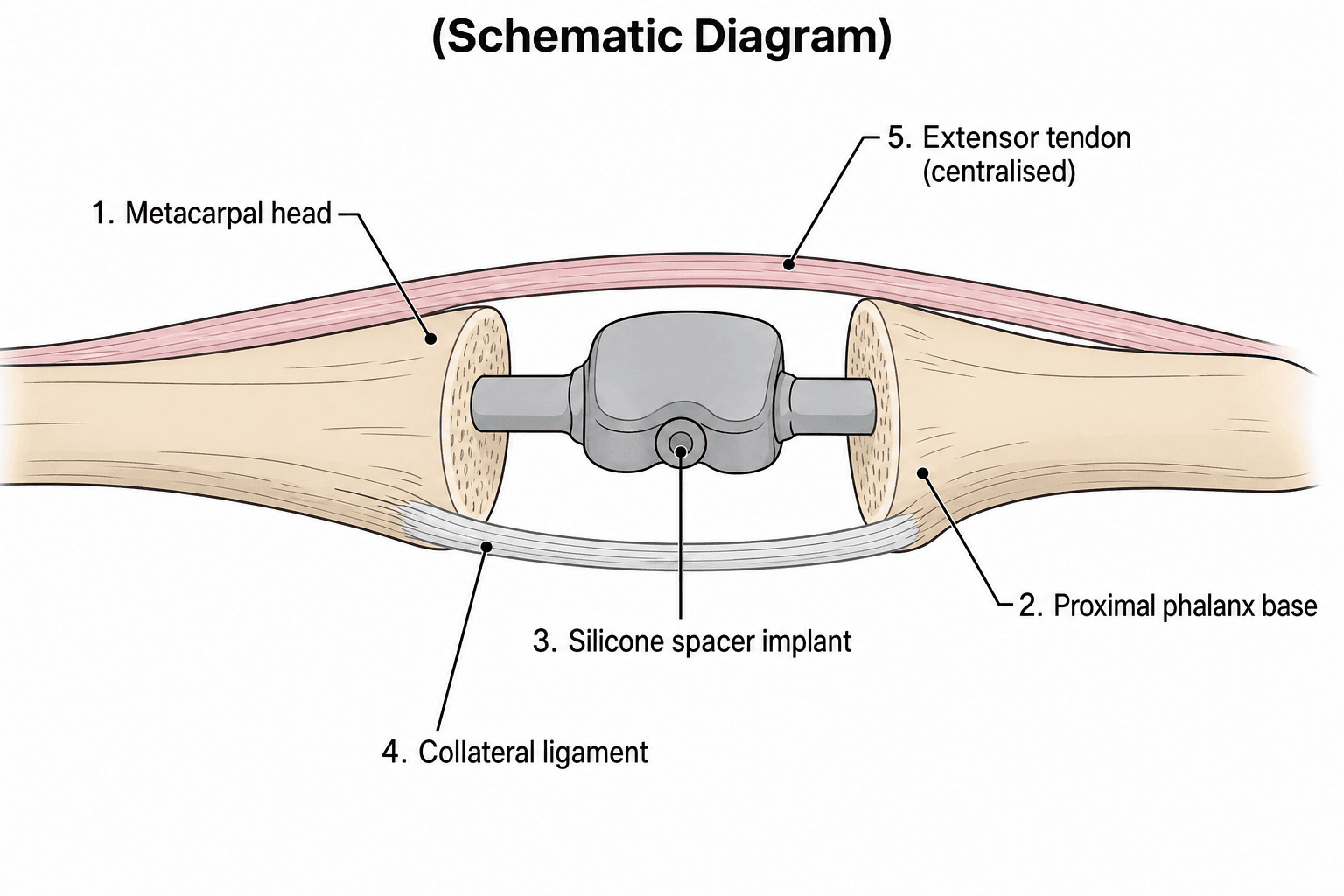
- Swanson silicone is a flexible SPACER, not anatomic joint - encapsulation provides stability
- Address wrist pathology BEFORE MCP, MCP BEFORE PIP in rheumatoid hand
- Index finger PIP: arthrodesis preferred over arthroplasty for pinch stability
- Simple trapeziectomy has equivalent outcomes to LRTI for thumb CMC OA (RCT-level evidence)
- Implant fracture is common but often clinically silent due to capsular integrity
- “MCP arthroplasty: RA is the indication; soft tissue balancing (RICE) critical; outcomes deteriorate with time
- “PIP arthroplasty: OA outcomes better than RA; pyrocarbon has a high complication/loosening rate
- “CMC arthroplasty: LRTI versus trapeziectomy alone - RCTs and reviews show no added benefit from LRTI
Small Joint Arthroplasty of the Hand
Core Exam Knowledge
Flexible spacer, NOT anatomic joint. Functions as an encapsulation arthroplasty. Silicone fracture is common (up to 70% at 10 years) but often asymptomatic. Silicone synovitis occurs in 5-10%.
MCP: Rheumatoid arthritis (main indication; function improves but deteriorates over years). PIP: Osteoarthritis better than RA (stiffer results in RA). Arthrodesis often preferred for index PIP (pinch stability).
Ulnar drift + MCP subluxation. Address wrist pathology FIRST. Correct MCP before PIP. Extensor tendon realignment (centralization) essential at surgery.
LRTI remains gold standard for thumb CMC OA. Simple trapeziectomy equally effective. Implant arthroplasty (pyrocarbon, total joint) has higher complication rate.
Implant Types and Selection
- mechanism
- Flexible spacer (encapsulation arthroplasty)
- indications
- MCP in RA (gold standard), PIP in RA
- advantages
- Reliable pain relief, corrects deformity, long track record
- disadvantages
- Fracture rate high (50-70%), silicone synovitis, limited motion gain
- mechanism
- Pre-flexed silicone spacer (30 degrees neutral)
- indications
- MCP and PIP arthroplasty
- advantages
- Reduced implant fatigue at hinge, improved biomechanics
- disadvantages
- Similar fracture rates, silicone wear particles
- mechanism
- Anatomic resurfacing (CoCr or titanium)
- indications
- PIP OA with intact collaterals and bone stock
- advantages
- Preserves bone, better motion potential, anatomic kinematics
- disadvantages
- Requires intact ligaments, loosening risk, technically demanding
- mechanism
- Unconstrained anatomic implant
- indications
- PIP OA, post-traumatic arthritis, younger patients
- advantages
- Modulus similar to bone, wear resistant, theoretically motion-preserving
- disadvantages
- High cost, squeaking, dislocation; high loosening/migration rate in some series (motion may worsen)
- mechanism
- Excision + FCR tendon interposition + suspension
- indications
- Thumb CMC osteoarthritis (Eaton Stage II-IV)
- advantages
- Gold standard, reliable pain relief, good pinch strength
- disadvantages
- Proximal metacarpal migration, prolonged recovery (3-6 months)
- 208 arthroplasties, mean 14-year follow-up: 63% of implants broken, 22% deformed
- Arc of motion fell from 46 degrees postoperatively to 36 degrees; extension deficit recurred to 23 degrees
- Ulnar drift recurred to a mean of 16 degrees; implant fracture correlated with increased ulnar drift
- Patients satisfied with only 38% of hands and only 27% of hands were pain-free at final follow-up
Indications and Contraindications
Indications for Small Joint Arthroplasty
- Rheumatoid arthritis with painful joint destruction and ulnar drift (primary indication)
- Post-traumatic arthritis with preserved bone stock
- Osteoarthritis (less common, generally good bone stock)
- Failed previous arthroplasty requiring revision
- Osteoarthritis with stiffness greater than 30 degrees flexion contracture (motion desired)
- Rheumatoid arthritis (more guarded outcomes than MCP)
- Post-traumatic arthritis
- Select cases of psoriatic arthritis with adequate bone stock
- Eaton Stage II-IV thumb CMC osteoarthritis refractory to conservative management
- Post-traumatic arthritis of first CMC
- Failed previous CMC surgery
- Pantrapezial arthritis (may require STT arthrodesis in addition)
Contraindications
- Active infection (local or systemic)
- Absent or severely deficient extensor mechanism
- Severe bone loss precluding implant fixation
- Fixed deformity not correctable at surgery (consider arthrodesis)
- Non-functional hand (no reconstructive benefit)
- Young, high-demand manual laborers (consider arthrodesis)
- Index finger PIP (arthrodesis preferred for pinch stability)
- Severe soft tissue contractures
- Inadequately controlled inflammatory arthritis
- Non-compliant patient unable to follow postoperative protocol
Anatomy and Biomechanics
MCP Joint Anatomy
The metacarpophalangeal joint is a condyloid (ellipsoid) joint permitting flexion, extension, abduction, adduction, and limited rotation. Key anatomical structures include the collateral ligaments (taut in flexion, lax in extension - critical for rehabilitation), accessory collateral ligaments, volar plate, and the dorsal extensor hood mechanism. In rheumatoid arthritis, synovitis leads to progressive destruction with stretching of the radial sagittal band, ulnar subluxation of the extensor tendons, and the characteristic ulnar drift deformity. The intrinsic muscles (interossei and lumbricals) contribute to deformity through their altered line of pull.
PIP Joint Anatomy
The proximal interphalangeal joint is a bicondylar hinge joint with primary motion in the sagittal plane (flexion-extension). Stability is provided by proper and accessory collateral ligaments, the volar plate, and the central slip of the extensor mechanism. The PIP joint withstands forces up to 3 times body weight during pinch grip. In osteoarthritis, marginal osteophytes (Bouchard nodes) form dorsally and laterally. In rheumatoid arthritis, progressive synovitis leads to boutonniere deformity (central slip attenuation, PIP flexion, DIP hyperextension) or swan neck deformity (PIP hyperextension, DIP flexion).
CMC Joint Anatomy
The thumb carpometacarpal joint is a saddle (sellar) joint between the trapezium and first metacarpal base, permitting opposition, flexion, extension, abduction, and adduction. The joint is stabilized by the anterior oblique (beak) ligament (most important for stability), dorsoradial ligament, posterior oblique ligament, and intermetacarpal ligament. Primary osteoarthritis preferentially affects this joint in postmenopausal women due to ligamentous laxity and repetitive loading. Pantrapezial arthritis extends to the scaphotrapezial and trapeziotrapezoid joints.
SPACERSwanson Implant Principles
Hook:Think of Swanson as a SPACER that maintains the joint space while the body forms a new capsule around it
Differential Diagnosis of the Painful Arthritic Hand Joint
Before committing to arthroplasty, confirm the correct diagnosis and joint. Several conditions mimic primary degenerative or rheumatoid joint destruction and change the operation entirely.
- distribution
- DIP (Heberden), PIP (Bouchard), thumb CMC
- keyFeatures
- Bony nodes, osteophytes, joint-space loss, subchondral sclerosis; MCPs usually spared
- pitfall
- Thumb CMC OA may coexist with carpal tunnel - assess median nerve
- distribution
- MCP and PIP, wrist; symmetrical; DIP spared
- keyFeatures
- Synovitis, ulnar drift, MCP volar subluxation, marginal erosions, positive RF/anti-CCP
- pitfall
- Address wrist and tendons first; deformity is the surgical target, not just pain
- distribution
- DIP predominant, ray/dactylitis pattern, asymmetrical
- keyFeatures
- Nail pitting, dactylitis, 'pencil-in-cup', new bone formation, RF negative
- pitfall
- Bone stock and skin make implant and wound healing less predictable
- distribution
- Any joint; often acute monoarthritis
- keyFeatures
- Tophi or chondrocalcinosis, crystals on aspiration, erosions with overhanging edges
- pitfall
- Mimics infection and inflammatory flare - aspirate before any implant surgery
- distribution
- Single joint, history of fracture/dislocation
- keyFeatures
- Incongruity, malunion, localised degeneration with otherwise normal joints
- pitfall
- Young high-demand patient - weigh arthrodesis vs arthroplasty carefully
- distribution
- Single joint, acute, systemic features
- keyFeatures
- Hot, swollen, exquisitely tender; raised inflammatory markers; positive aspirate
- pitfall
- Absolute contraindication to arthroplasty - must be excluded and treated first
- Landmark paper establishing the silicone flexible-implant resection arthroplasty concept
- Implant functions as a flexible hinge spacer maintaining the joint space after resection
- Fibrous encapsulation forms around the implant and provides the working stability of the joint
- Foundational principle: the new capsule, not the implant, is the arthroplasty
MOTIONPIP Arthroplasty Patient Selection
Hook:Use MOTION criteria to select patients who will gain the most from PIP arthroplasty rather than fusion
Surgical Technique
MCP Silicone Arthroplasty (Swanson Procedure)
- Assess wrist pathology (address BEFORE MCP surgery)
- Document range of motion, ulnar drift, extensor lag
- Radiographic templating for implant sizing
- Optimize disease control (RA: rheumatology review)
- Regional anaesthesia (axillary block preferred) or general
- Arm tourniquet (250 mmHg)
- Hand table, loupe magnification
- Incision: Transverse or longitudinal dorsal incision centered over MCP joints
- Interval: Between extensor tendons (may use single incision for multiple joints)
- Capsular exposure: Incise extensor hood longitudinally, radial to extensor tendon
- Synovectomy: Thorough removal of inflamed synovium
- Excise metacarpal head with oscillating saw (preserve collateral ligament origins if possible)
- Remove base of proximal phalanx (minimal resection, 2-3 mm)
- Open medullary canals with broach/reamer
- Size implant using trial sizers
- Insert Swanson silicone implant (or NeuFlex)
- Confirm smooth flexion-extension arc
- No cement required (press-fit)
- Extensor realignment: Centralize extensor tendon over MCP
- Radial sagittal band repair/imbrication: Critical for preventing recurrent ulnar drift
- Intrinsic release: Release ulnar intrinsics if contracted
- Capsular repair: Secure closure over implant
- Layered closure
- Bulky dressing with MCP extension splint (slight radial deviation)
- Dynamic extension splinting at 3-5 days
- Protected motion for 6-8 weeks
The Swanson implant functions through encapsulation arthroplasty - the capsule that forms around the implant provides stability. Clinical function often maintained despite implant fracture because the capsule remains intact.
RICESoft Tissue Steps in MCP Arthroplasty
Hook:After implanting, remember to RICE the soft tissues to prevent recurrent ulnar drift
Complications
Implant-Related Complications
- Incidence: 50-70% at 10-year follow-up
- Often asymptomatic due to maintained capsular integrity
- Clinical significance: Only treat if symptomatic (pain, instability, crepitus)
- Management: Observation if asymptomatic; revision arthroplasty or arthrodesis if symptomatic
- Incidence: 5-10% of silicone arthroplasties
- Pathophysiology: Foreign body reaction to silicone particles
- Clinical features: Swelling, pain, osteolysis on radiographs, may mimic infection
- Management: Synovectomy with implant exchange or conversion to arthrodesis; titanium grommets may reduce wear particle generation
- More common with anatomic designs (SRA, pyrocarbon) than silicone
- Risk factors: Poor bone quality, malalignment, high activity level
- Presents with progressive pain and loss of motion
- Management: Revision with bone grafting or conversion to arthrodesis
Deformity Recurrence
- Results from inadequate soft tissue balancing at index surgery
- Progressive stretching of radial sagittal band repair
- Continued rheumatoid disease activity
- Prevention: Meticulous soft tissue technique, disease control
- Management: Revision soft tissue procedure or revision arthroplasty
- Central slip attenuation leads to boutonniere recurrence
- Lateral band subluxation causes swan neck
- May require extensor reconstruction or conversion to arthrodesis
Other Complications
- Early: Wound infection, treat with antibiotics and wound care
- Deep/chronic: Implant removal, debridement, delayed reconstruction
- Rheumatoid patients at higher risk due to immunosuppression
- Common, especially at PIP level
- Prevention: Early protected motion, compliant patient
- Treatment: Aggressive therapy; manipulation under anesthesia rarely helpful
- Results from ligament insufficiency or bone loss
- May require revision with constrained implant or arthrodesis
- 1336 silastic MCP implants in 404 operations on 381 rheumatoid patients
- Survivorship was 63% at 17 years (failure = revision OR radiographic fracture)
- Two-thirds of implants were radiographically broken on review
- Soft-tissue balancing, crossed intrinsic transfer and wrist realignment improved survival; grommets did NOT protect against fracture
- Systematic review of 35 studies across the 8 most common procedures for trapeziometacarpal OA
- No technique was proven superior to trapeziectomy for pain, function or strength
- Trapeziectomy with LRTI was associated with a HIGHER complication rate without added benefit
- Higher-evidence studies had only 12-month follow-up; CMC arthrodesis had nonunion rates of 8-21%
Outcomes
MCP Arthroplasty Outcomes
- Early gains: arc of motion improves (around 30 to 46 degrees) and ulnar drift and extensor lag correct substantially in the first year
- Deterioration with time: by 14 years arc falls back toward 36 degrees, extension deficit recurs to around 23 degrees, and ulnar drift recurs to a mean of 16 degrees (Goldfarb & Stern)
- Long-term satisfaction is modest - patients satisfied with only 38% of hands and 27% pain-free at 14 years in the Goldfarb series
- Implant survival: 63% at 17 years (failure = revision or radiographic fracture; Trail)
- Implant fracture: roughly 60-67% radiographically by long-term follow-up, but frequently clinically silent
- Despite this, prospective comparison with medical therapy alone shows surgery still improves patient-reported hand function and corrects deformity better than non-operative management (Chung, level II)
- Rheumatoid arthritis (better than OA or post-traumatic)
- Adequate bone stock
- Good soft tissue quality
- Compliant with therapy protocol
- Well-controlled systemic disease
PIP Arthroplasty Outcomes
- Motion gain: Modest (average arc 40-50 degrees)
- Pain relief: 75-80%
- Stiffness more common than at MCP level
- Outcomes are inconsistent and series-dependent; pain relief can be good but motion often does not improve
- In a single-surgeon pyrocarbon PIP series (Sweets & Stern), arc of motion actually FELL from 57 to 31 degrees, with frequent loosening, migration, dislocation and squeaking - the authors abandoned the implant
- Higher reoperation and loosening rate than silicone; best reserved for OA with intact collateral ligaments and good bone stock
- Counsel patients that motion preservation is not guaranteed and that arthrodesis is a reliable fallback
Thumb CMC Arthroplasty Outcomes
Trapeziectomy (with or without LRTI):
- Good pain relief in roughly 78% of patients in long-term RCT follow-up (Gangopadhyay), and higher in observational series
- Grip and pinch strength recover, although pinch may decline slowly over years irrespective of technique
- Subsidence (proximal metacarpal migration) is near-universal but correlates poorly with symptoms
- Return to function: 3-6 months (longer than digit arthroplasty)
- Total joint (dual-mobility) prostheses show faster early recovery in some series but lack the long-track-record durability data of trapeziectomy
Cost-Effectiveness and the Value Case for Silicone MCP Arthroplasty
The long-term series paint a pessimistic radiographic picture (deteriorating motion, recurrent drift, majority implant fracture), which raises a fair examiner question: is silicone MCP arthroplasty worth doing and worth funding? The health-economic evidence answers this more favourably than the survivorship data alone would suggest. The critical point is that the value of the operation depends heavily on which outcome instrument is used - a hand-specific, patient-rated measure captures the real benefit far better than a whole-body arthritis-impact scale.
- Outcomes are durable when measured well. In the Squitieri prospective cohort, the functional gains of surgery were maintained across the full 5-year follow-up rather than eroding, when measured with the hand-specific Michigan Hand Outcomes Questionnaire.
- Cost per unit of benefit is modest. Improved hand-specific outcomes were achieved at a relatively low incremental cost, so silicone MCP arthroplasty looks cost-effective on a hand-specific measure even after accounting for the possibility of complications and revision.
- The instrument matters enormously. The same improvement looks very expensive when forced onto a generic whole-body arthritis-impact scale, because rebuilding a few finger joints barely moves a systemic disease score. This is a general trap in rheumatoid hand surgery: judging a focal hand operation by a whole-patient outcome measure understates its true value.
- Revision does not sink the economics. The favourable cost-effectiveness held even when the observed and previously published revision rates (around 5 to 6 percent) were built into the model.
This reconciles the apparent contradiction between the gloomy long-term radiographic series and continued use of the procedure: for the severely deformed, painful rheumatoid hand, silicone MCP arthroplasty delivers durable, patient-valued functional improvement at acceptable cost - provided it is judged by what the hand can do, not by a systemic disease score.
- 5-year prospective cohort of 170 rheumatoid patients (73 surgical, 97 non-surgical) with cost-effectiveness analysis using Medicare outpatient claims
- Short-term hand-specific gains (Michigan Hand Outcomes Questionnaire) were maintained across the full 5-year follow-up in the surgical group
- Cost associated with improved outcomes was low measured by the hand-specific MHQ but appeared far higher when measured by the generic Arthritis Impact Measurement Scale
- Cost-effectiveness was not substantially worsened by the observed 5.5% revision rate or published long-term revision rates around 6.2%
When challenged on whether silicone MCP arthroplasty is worth doing despite high fracture rates, cite Squitieri: 5-year functional gains are maintained and cost-effective on the hand-specific MHQ. The examiner's hook is the instrument - a focal hand operation looks poor value on a whole-body arthritis score but good value on a hand-specific one.
Guidelines, Registries & Global Practice
Global Epidemiology
- Thumb CMC (trapeziometacarpal) osteoarthritis is the most common small-joint indication worldwide, with a strong female and post-menopausal predominance; radiographic basal-joint OA is found in roughly a third of post-menopausal women.
- Rheumatoid arthritis affects approximately 0.5-1% of adults globally. The classic severely deformed rheumatoid MCP hand requiring arthroplasty is becoming less common as early biologic and conventional DMARD therapy controls disease before joint destruction.
- Erosive/inflammatory hand OA and post-traumatic arthritis make up most remaining PIP and MCP arthroplasty caseload.
Side-by-Side Guidance
- Position relevant to small joint arthroplasty
- Thumb CMC OA managed conservatively first; surgery (trapeziectomy +/- suspension, arthrodesis, or replacement) reserved for refractory disease; no single procedure mandated
- Position relevant to small joint arthroplasty
- Trapeziectomy is the benchmark for thumb base OA; routine addition of LRTI not supported by evidence; rheumatoid hand surgery integrated with rheumatology and hand therapy
- Position relevant to small joint arthroplasty
- Hand OA: education, exercise and orthoses first; surgery for thumb base OA only after failed conservative care; trapeziectomy effective
- Position relevant to small joint arthroplasty
- Emphasises soft-tissue balancing and extensor centralisation as determinants of MCP arthroplasty durability
Registry and Evidence Notes
- Unlike hip and knee arthroplasty, small joint arthroplasty is poorly captured by national joint registries; most outcome data come from single-centre series and a small number of RCTs (Gangopadhyay; Chung). This limits implant-level comparative survivorship data.
- The consistent registry-independent message: trapeziectomy-based procedures are durable and additional ligament reconstruction adds morbidity without benefit; silicone MCP implants fracture frequently but the encapsulation arthroplasty continues to function.
High- vs Limited-Resource Practice Variation
- In well-resourced settings, certified hand therapists and dynamic splinting protocols are integral to MCP arthroplasty outcomes, and pyrocarbon or total joint implants are available at higher cost for selected motion-preserving indications.
- In limited-resource settings, arthrodesis and simple trapeziectomy are favoured because they are cheap, reliable, and require less specialised post-operative therapy and follow-up. The reduced dependence on hand-therapy infrastructure is a legitimate driver of procedure choice, not a compromise of standards.
Controversies and Areas of Uncertainty
Long-term series (Goldfarb, Trail) show deteriorating motion, recurrent deformity and high fracture rates, while the prospective Chung trial shows real functional gains over medical therapy. The honest position: it is a reasonable option for the severely deformed, painful rheumatoid hand, but expectations must be measured and it is being performed less often as biologic disease control improves.
Despite LRTI's enduring popularity, the highest-level evidence (Gangopadhyay RCT, Vermeulen review) shows no benefit over trapeziectomy alone and more complications. Many surgeons nonetheless retain a suspension step. The debate is now shifting toward whether modern total joint replacement offers faster recovery worth its revision risk.
Marketed for motion preservation, yet independent series (Sweets & Stern) report motion loss, loosening, migration and high reoperation. Whether better patient selection (intact collaterals, OA not RA, well-aligned joint) rescues these designs remains unresolved.
For the index PIP, the border digits, and young manual workers, fusion trades motion for durable, pain-free stability. There is no consensus threshold; the decision is individualised to joint, demand and the value the patient places on motion versus reliability.
- Prospective 3-centre (US and England) comparison of silicone MCP arthroplasty plus medical therapy versus medical therapy alone
- All patients had severe ulnar drift and/or extensor lag; 1-year data on 45 surgical and 72 non-surgical patients
- Surgery produced significant improvement in overall Michigan Hand Outcomes Questionnaire score, ulnar deviation and extensor lag
- Grip and pinch strength did not significantly improve in either group
- RCT of 174 thumbs randomised to simple trapeziectomy, trapeziectomy with palmaris interposition, or trapeziectomy with FCR LRTI
- At minimum 5-year follow-up (median 6 years) there was NO difference in pain relief, grip, pinch or range of motion between groups
- Good pain relief at 1 year was maintained long-term irrespective of technique
- Complications were few and evenly distributed; pinch strength declined with time in all groups
- 31 pyrocarbon PIP arthroplasties in 17 patients, mean 55-month follow-up
- Arc of motion DECREASED from 57 to 31 degrees after early postoperative gains
- High complication rate: loosening (15 joints), contracture (20), dislocation (5), squeaking (11); 6 joints required reoperation
- The authors discontinued use of the implant in their practice
- Defines the radiographic Eaton-Littler/Eaton-Glickel staging of thumb basal joint arthrosis (Stages I-IV)
- Stage progresses from a painful hypermobile joint with preserved cartilage to pantrapezial degeneration
- Staging is used to rationalise treatment selection; intra-operative findings may upstage the disease
Exam Day Preparation
Indications by Joint
- MCP: RA is gold standard indication; address wrist first; silicone preferred
- PIP: OA better outcomes than RA; index finger prefers arthrodesis; SRA/pyrocarbon if collaterals intact
- CMC: Eaton Stage II-IV OA; LRTI or simple trapeziectomy; equivalent outcomes proven
Implant Selection
- Swanson silicone: Flexible spacer, encapsulation arthroplasty, 50-70% fracture rate but often asymptomatic
- Pyrocarbon: Modulus similar to bone, unconstrained, requires intact ligaments, higher cost
- SRA: Anatomic resurfacing, best bone preservation, technically demanding
- LRTI: FCR tendon interposition and suspension, gold standard for CMC but equivalent to trapeziectomy alone
MCP Arthroplasty Technique
- Dorsal approach, longitudinal capsulotomy radial to extensor
- Metacarpal head excision, minimal phalanx base resection
- RICE soft tissue balancing: Radial sagittal band, Intrinsic release, Centralize extensor, Encapsulation repair
- Dynamic extension splinting postoperatively
Complications
- Silicone fracture: Common but often asymptomatic due to capsular integrity
- Silicone synovitis: 5-10%, foreign body reaction, osteolysis, may mimic infection
- Recurrent deformity: Inadequate soft tissue balancing, ongoing disease activity
- Stiffness: Common at PIP level, early protected motion essential
Critical Exam Points
- Swanson is a spacer not an anatomic joint - encapsulation provides stability
- Address wrist before MCP, MCP before PIP in RA
- Index PIP: Arthrodesis preferred (pinch stability more important than motion)
- CMC: Simple trapeziectomy equals LRTI outcomes - added procedure without proven benefit
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman with rheumatoid arthritis presents with painful MCP joints of the dominant hand with 30 degrees ulnar drift, MCP subluxation, and extensor lag. She has been on stable disease-modifying therapy. Radiographs show joint destruction with preserved bone stock. How would you manage this patient?”
“A 52-year-old male tradesman presents with painful stiff PIP joint of his ring finger following a fracture-dislocation 2 years ago. Examination shows 40 degrees fixed flexion with arc of motion 40-80 degrees. Radiographs confirm post-traumatic arthritis with osteophytes but preserved bone stock. What are your treatment options?”
“A 62-year-old woman presents with thumb base pain affecting activities of daily living. Clinical examination shows positive grind test, CMC subluxation, and adduction contracture. Radiographs show Eaton Stage III CMC osteoarthritis with STT joint involvement. What is your management plan?”
Titanium Grommets: Rationale and the Evidence Against Them
Two of the classic failings of the silicone spacer - implant fracture and particulate silicone synovitis - were both attributed, in part, to abrasion of the flexible stem against the sharp cut edge of bone at the mouth of the medullary canal. To counter this, Swanson introduced grommets: small titanium eyelets seated in the canal entrance at the bone-implant junction, interposing a smooth, rigid collar between the silicone and the bone so the stem no longer chafes against a bony edge. The theoretical case is attractive - protect the weakest part of the hinge and reduce the shedding of the silicone particles that provoke synovitis and osteolysis.
The clinical evidence has not supported it. In Trail's large 17-year survivorship series the use of grommets did NOT protect the implant from fracture, and grommets add cost, technical steps, and their own potential for malposition or loosening. The modifiable factors that genuinely prolonged survival in that series were soft-tissue balancing, crossed intrinsic transfer, and wrist realignment - not the hardware. Grommets may still be considered where the priority is limiting particulate wear and synovitis rather than fracture, but they should never be relied on to prevent implant breakage, and many surgeons now omit them.
Grommets are titanium eyelets meant to stop the silicone stem abrading on cut bone. Know the exam trap: their rationale is protection from wear and fracture, but Trail's series showed grommets do NOT reduce implant fracture - soft-tissue technique and wrist realignment do.
References
-
Swanson AB. Flexible implant resection arthroplasty. Hand. 1972;4(2):119-134.
-
Goldfarb CA, Stern PJ. Metacarpophalangeal joint arthroplasty in rheumatoid arthritis. A long-term assessment. J Bone Joint Surg Am. 2003;85(10):1869-1878.
-
Trail IA, Martin JA, Nuttall D, Stanley JK. Seventeen-year survivorship analysis of silastic metacarpophalangeal joint replacement. J Bone Joint Surg Br. 2004;86(7):1002-1006.
-
Vermeulen GM, Slijper H, Feitz R, et al. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg Am. 2011;36(1):157-169.
-
Gangopadhyay S, McKenna H, Burke FD, Davis TRC. Five- to 18-year follow-up for treatment of trapeziometacarpal osteoarthritis. J Hand Surg Am. 2012;37(3):411-417.
-
Sweets TM, Stern PJ. Pyrolytic carbon resurfacing arthroplasty for osteoarthritis of the proximal interphalangeal joint of the finger. J Bone Joint Surg Am. 2011;93(15):1417-1425.
-
Chung KC, Burns PB, Wilgis EFS, et al. A multicenter clinical trial in rheumatoid arthritis comparing silicone metacarpophalangeal joint arthroplasty with medical treatment. J Hand Surg Am. 2009;34(5):815-823.
-
Eaton RG, Glickel SZ. Trapeziometacarpal osteoarthritis. Staging as a rationale for treatment. Hand Clin. 1987;3(4):455-471.
-
Squitieri L, Chung KC, Hutton DW, et al. A 5-year cost-effectiveness analysis of silicone metacarpophalangeal arthroplasty in patients with rheumatoid arthritis. Plast Reconstr Surg. 2015;136(2):305-314.
-
Burton RI, Pellegrini VD Jr. Surgical management of basal joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplasty. J Hand Surg Am. 1986;11(3):324-332.