Cerebral Palsy | Dynamic vs Fixed Deformity | SPLATT | Tendon Transfers | Gait Analysis
- Equinovarus = ankle plantarflexion + hindfoot varus + forefoot supination from spastic muscle imbalance
- Tibialis posterior overactivity drives hindfoot varus; tibialis anterior drives forefoot supination and first ray plantarflexion
- Distinguish dynamic (supple under anaesthesia) from fixed deformity before choosing surgery
- SPLATT (split tibialis anterior transfer) is the workhorse operation for dynamic forefoot supination
- Single-event multilevel surgery (SEMLS) is the modern paradigm combining all corrections in one procedure
- “Dynamic equinovarus is correctable under GA; fixed is not - this distinction changes the operation
- “SPLATT splits the TA tendon, half stays anterior, half passes through the interosseous membrane to the peroneal side
- “GMFCS level is the single most important prognostic factor for ambulatory outcome
- “Gait analysis (3-D) guides surgical planning by quantifying which muscles are overactive and when in the gait cycle
Tibialis posterior inverts and plantarflexes the hindfoot. Tibialis anterior dorsiflexes and inverts (supinates) the forefoot. Overactivity of either or both muscles creates the equinovarus pattern. The peroneus longus and brevis are the antagonists (evertors).
Dynamic deformity corrects under general anaesthesia - spasticity alone. Fixed deformity persists under GA - contracture or bony change. This distinction is critical: dynamic deformity may respond to BTX-A or tendon transfer; fixed deformity requires lengthening, release, or osteotomy.
Address equinus first (gastrocnemius recession or TAL), then varus (TP release or transfer), then forefoot supination (SPLATT). Plan all levels in one sitting (SEMLS principle) to avoid repeated anaesthetics and cast immobilisation in children.
GMFCS I-II: Community ambulators, excellent surgical outcomes. GMFCS III: Household ambulators with assistive devices, good outcomes with careful selection. GMFCS IV-V: Limited ambulation, surgery focused on comfort, bracing, and seating. Always state GMFCS level in your exam answer.
- Diagnosis
- Correctable under GA, 3-D gait analysis shows premature heel rise
- Treatment
- Gastrocnemius recession + SPLATT ± TP intramuscular lengthening
- Key Pearl
- Single-event multilevel surgery (SEMLS) preferred
- Diagnosis
- Not correctable under GA, weight-bearing lateral X-ray shows varus
- Treatment
- TAL + TP Z-lengthening or transfer + SPLATT
- Key Pearl
- Must distinguish TA-driven from TP-driven varus
- Diagnosis
- Fixed deformity with skin breakdown risk, seating issues
- Treatment
- Talectomy or subtalar fusion for positioning
- Key Pearl
- Goals shift from gait to comfort and hygiene
STEPMuscles Driving Equinovarus
Hook:STEP through the equinovarus muscles: Soleus for equinus, Tibialis posterior for varus, EHL for claw toe, Peroneals too weak to resist!
GRABSSurgical Options for Equinovarus
Hook:GRABS the equinovarus: Gastrocnemius recession, Rectify varus, Anterior tibialis transfer, Botox, SEMLS!
STAGGait Analysis Phases in Equinovarus
Hook:STAGger through gait analysis: Swing phase inversion, Terminal swing toe-strike, Absent heel strike, Ground reaction deviation!
Overview and Epidemiology
Spastic equinovarus is the most common foot deformity in cerebral palsy and a high-yield FRACS/FRCS paediatric orthopaedic topic. It exemplifies the principle of muscle imbalance: spastic overactivity of invertors and plantarflexors overwhelms weak evertors and dorsiflexors. The surgical management requires a systematic approach - distinguishing dynamic from fixed deformity, identifying which muscles are overactive and when in the gait cycle, and planning single-event multilevel surgery.
- Cerebral palsy is the most common motor disability in childhood, with an incidence of approximately 2 to 3 per 1000 live births globally
- Equinovarus deformity affects roughly 15 to 30 percent of children with spastic CP, making it the most prevalent foot deformity
- Spastic diplegia (bilateral CP) carries the highest prevalence of equinovarus, followed by hemiplegia
- Unilateral involvement (hemiplegia) often shows more severe varus due to unopposed tibialis posterior spasticity
- Gait disturbance: Toe-walking, lateral border weight-bearing, tripping, and poor push-off
- Pain: Lateral foot pain from overloaded peroneal tubercle and fifth metatarsal base
- Skin breakdown: Callus formation over lateral border, risk of ulceration in severe cases
- Bracing difficulty: AFOs cannot adequately control dynamic varus, leading to poor compliance
- Progression: Untreated dynamic deformity progresses to fixed contracture with secondary bony changes
Pathophysiology
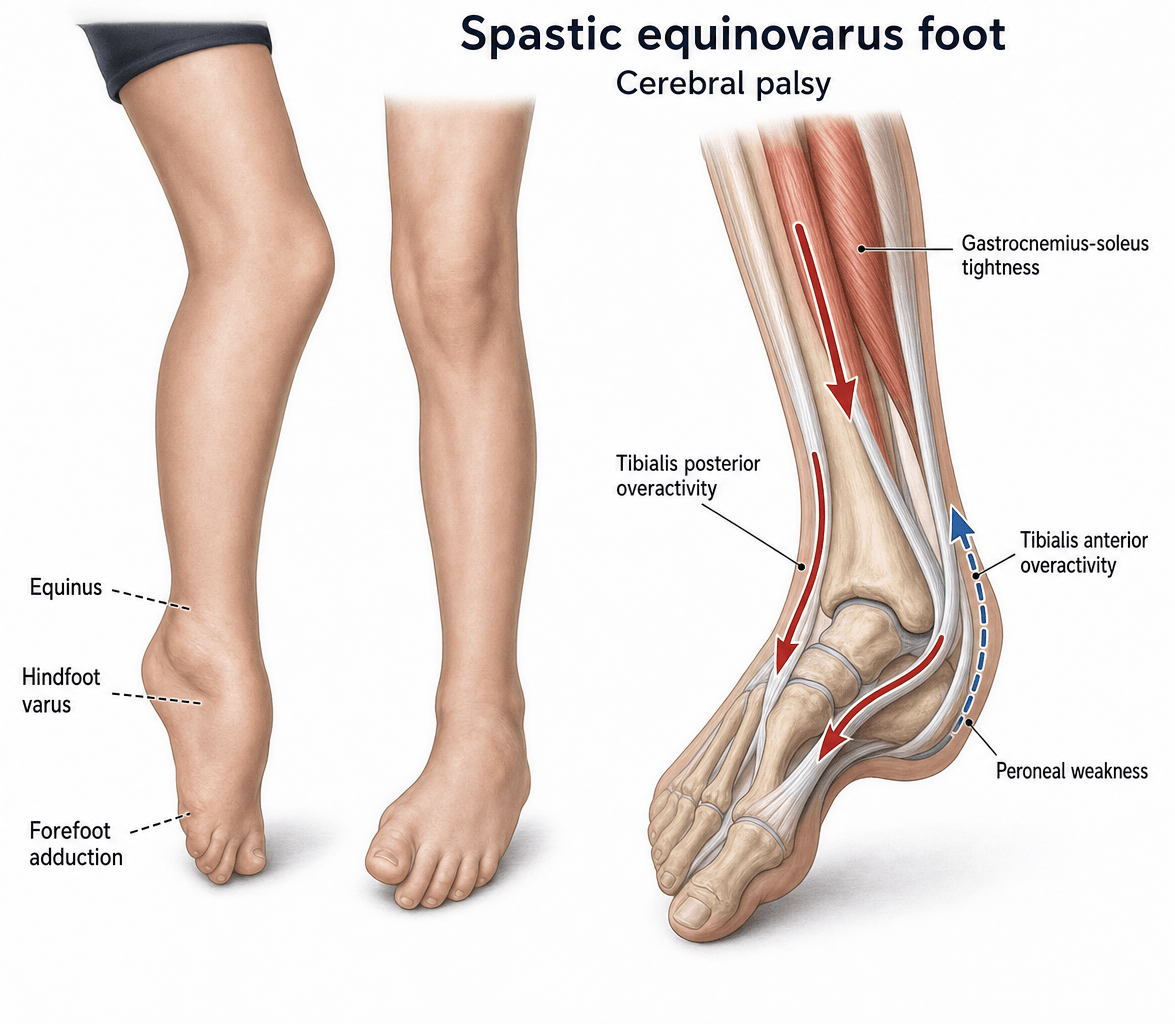
The equinovarus deformity results from spastic overactivity of plantarflexors and invertors combined with relative weakness of dorsiflexors and evertors. The key muscles driving the deformity are:
- Gastrocnemius-soleus complex: Spastic equinus (ankle plantarflexion)
- Tibialis posterior: Spastic hindfoot inversion (varus); active in both stance and swing
- Tibialis anterior: Spastic forefoot supination and first ray plantarflexion; most active in swing phase
The antagonists (peroneus longus, peroneus brevis, extensor digitorum longus) are typically weak or underactive, failing to counterbalance the invertors. Over time, dynamic spasticity leads to muscle contracture, ligamentous shortening, and eventually bony deformation of the growing foot.
- Spastic Action
- Ankle plantarflexion
- Deformity Produced
- Equinus (toe-walking)
- Phase of Overactivity
- Stance phase (premature heel rise)
- Spastic Action
- Hindfoot inversion + plantarflexion
- Deformity Produced
- Hindfoot varus
- Phase of Overactivity
- Stance and swing (persistent)
- Spastic Action
- Forefoot supination + first ray plantarflexion
- Deformity Produced
- Forefoot varus / supination
- Phase of Overactivity
- Swing phase (foot clearance)
- Spastic Action
- Great toe hyperextension
- Deformity Produced
- Claw great toe (recruited for dorsiflexion)
- Phase of Overactivity
- Swing phase (compensatory)
- Spastic Action
- Foot eversion (antagonists, weak)
- Deformity Produced
- Cannot oppose inversion
- Phase of Overactivity
- Underactive throughout gait cycle
Definition: Deformity present during activity but correctable passively and under anaesthesia
Mechanism: Spasticity alone without contracture
Key test: Examine under GA - full passive correction achieved
Management: BTX-A injections, AFO bracing, physical therapy, or tendon transfers (no lengthening needed)
Definition: Deformity persists even under general anaesthesia
Mechanism: Muscle contracture, joint capsule shortening, bony deformation
Key test: Examine under GA - passive correction incomplete or absent
Management: Surgical lengthening, release, osteotomy, or arthrodesis
Classification and Types
Gross Motor Function Classification System
The GMFCS level is the single most important prognostic factor in CP foot surgery. It determines treatment goals and expected outcomes.
- Ambulation
- Walks without limitations
- Surgical Goals
- Normalise gait pattern, improve efficiency
- Expected Outcome
- Excellent - near-normal gait achievable
- Ambulation
- Walks with limitations (no devices)
- Surgical Goals
- Improve gait, prevent progressive deformity
- Expected Outcome
- Very good - meaningful gait improvement
- Ambulation
- Walks with assistive devices
- Surgical Goals
- Maintain or improve community ambulation
- Expected Outcome
- Good - functional gains with realistic expectations
- Ambulation
- Self-mobility with limitations, may use powered mobility
- Surgical Goals
- Comfort, positioning, bracing tolerance, seating
- Expected Outcome
- Modest - focus shifts from gait to comfort
- Ambulation
- Transported manually
- Surgical Goals
- Comfort, hygiene, prevent skin breakdown
- Expected Outcome
- Limited - positioning procedures
Always state the GMFCS level when discussing surgical plans in exams. Surgical outcomes deteriorate significantly with higher GMFCS levels.
Clinical Assessment
- Birth history: Prematurity, birth asphyxia, neonatal complications
- Motor milestones: Delayed sitting, crawling, walking
- CP classification: Topography (hemiplegia, diplegia, quadriplegia), GMFCS level
- Gait pattern: Toe-walking onset, tripping frequency, falling pattern
- Previous treatment: BTX-A injections, AFO use, prior surgeries
- Functional level: Community ambulation distance, assistive devices used
- Patient and family goals: Realistic expectations discussion is essential
- Inspect: Standing posture, foot progression angle, toe-walking pattern, lateral border callus
- Look: From behind - too many toes sign (hindfoot valgus) vs no toes visible (varus); from side - heel contact pattern
- Feel: Tibialis posterior tendon during inversion (overactive? palpable spasm?); peroneal tendon bulk
- Move: Passive ROM ankle (equinus), subtalar (varus correctability), forefoot (supination)
- Silfverskiold test: Distinguish gastrocnemius (improves with knee flexion) from soleus equinus (no change with knee flexion)
- Spasticity grading: Modified Ashworth Scale for TA, TP, gastrocnemius-soleus
Technique: Passive ankle dorsiflexion measured with the knee extended and then flexed to 90 degrees.
Gastrocnemius tightness (positive Silfverskiold): Dorsiflexion improves by more than 10 degrees when the knee is flexed (relaxes gastrocnemius which crosses the knee joint).
Soleus tightness: Dorsiflexion does not significantly improve with knee flexion (soleus does not cross the knee).
Clinical implication: Isolated gastrocnemius tightness is treated with gastrocnemius recession (proximal release). Combined gastrocnemius-soleus tightness may require percutaneous or open TAL (Achilles tendon lengthening). Over-lengthening the Achilles in an ambulatory child must be avoided as it causes calcaneus gait (crouch gait).
- Technique
- Passive DF with knee extended vs flexed 90 degrees
- Positive Finding
- Greater than 10 degrees improvement with knee flexion
- Significance
- Isolated gastrocnemius tightness = recession, not TAL
- Technique
- Inject TP with local anaesthetic, reassess gait
- Positive Finding
- Varus corrects after block
- Significance
- TP is dominant varus driver, consider TP lengthening or transfer
- Technique
- Examine foot passive ROM under general anaesthesia
- Positive Finding
- Full correction (dynamic) vs residual deformity (fixed)
- Significance
- Determines whether soft tissue surgery alone suffices
- Technique
- Passive stretch of target muscle, grade 0 to 4
- Positive Finding
- Grade 3 or above = considerable spasticity
- Significance
- Guides BTX-A dosing and surgical planning
- Key Features
- Spasticity, hyperreflexia, upper motor neuron signs, dynamic component
- Discriminating Finding
- CP diagnosis established, GMFCS graded, dynamic deformity pattern
- Management Difference
- SEMLS, BTX-A, tendon transfers
- Key Features
- Present at birth, no neurological findings, fixed deformity from birth
- Discriminating Finding
- Congenital onset, Pirani scoring, no spasticity or hyperreflexia
- Management Difference
- Ponseti casting, posteromedial release if recurrent
- Key Features
- Progressive cavovarus, peroneal muscle wasting, sensory changes
- Discriminating Finding
- Bilateral cavovarus, family history, nerve conduction studies abnormal
- Management Difference
- Tendon transfers, osteotomies, genetic counselling
- Key Features
- Bilateral toe-walking, no neurological signs, normal development
- Discriminating Finding
- Can walk heel-toe on request, normal neurological exam, no spasticity
- Management Difference
- Observation, serial casting if persistent, no tendon surgery
- Key Features
- Progressive foot deformity, bowel or bladder changes, back pain
- Discriminating Finding
- Deteriorating neurological signs, MRI spine abnormality
- Management Difference
- Neurosurgical decompression first, then orthopaedic correction
Always examine the spine in a child with progressive equinovarus. A tethered cord or syrinx can mimic or coexist with CP. Deteriorating gait, new bowel or bladder dysfunction, or asymmetric neurological findings warrant urgent MRI of the entire neuroaxis. Operating on a foot deformity caused by untreated spinal pathology is a critical error.
Investigations
Investigation Protocol
Clinical examination: Silfverskiold test, passive ROM, spasticity grading, observation of gait pattern
3-D instrumented gait analysis: The gold standard for surgical planning. Quantifies joint angles, moments, powers, and EMG timing of individual muscles through the gait cycle. Identifies which muscles are overactive and when, guiding the choice between SPLATT, TP lengthening, or both.
Video gait analysis: Useful when 3-D analysis is unavailable (common in limited-resource settings)
Views: Standing AP and lateral of the foot and ankle; saltarelli view (dorsiflexion lateral) if equinus severe
Look for: Talar flattening, navicular-medial malleular overlap (subtalar subluxation), calcaneal pitch, Meary angle (talar-first metatarsal angle), hindfoot alignment
Clinical correlation: Radiographs are most useful in fixed deformity to assess bony changes and plan osteotomies
Indication: Progressive deformity, bowel or bladder changes, asymmetric signs, absent CP diagnosis
Findings: Tethered cord, syrinx, diastematomyelia, lipoma
Critical: Neurosurgical intervention may halt progression and change orthopaedic management
3-D gait analysis has been shown to change the surgical plan in approximately 40 to 60 percent of cases compared with clinical examination alone. In the exam, mention it as the gold standard for surgical planning in ambulatory children (GMFCS I-III). It is not required for non-ambulatory children (GMFCS IV-V) where goals are positioning and comfort.
Management Algorithm
Conservative Management
Goal: Delay or prevent surgery, maintain ROM, optimise gait while the child grows
Conservative Protocol
Stretching programme: Daily gastrocnemius-soleus stretching, TP stretching, ankle ROM exercises
Strengthening: Peroneal strengthening (evertors), tibialis anterior strengthening for eccentric control
Functional training: Gait training, balance exercises, task-specific practice
Evidence: Therapy alone rarely corrects established equinovarus but maintains ROM and delays surgery
Mechanism: Botulinum toxin type A blocks acetylcholine release at the neuromuscular junction, reducing spasticity for approximately 3 to 4 months per injection
Targets: Gastrocnemius, tibialis posterior, tibialis anterior (guided by gait analysis)
Dose: Typically 4 to 6 units per kilogram per muscle (total dose up to 15 to 20 units per kilogram per session)
Evidence: Effective for dynamic deformity; delays surgery but does not prevent eventual need in most cases
Limitation: Repeated injections may cause antibody formation and reduced efficacy; does not address fixed contracture
Solid AFO: Controls equinus and partially controls varus in stance; best for fixed equinus
Hinged AFO: Allows some dorsiflexion while controlling equinus; preferred for ambulatory children to permit third rocker
Ground reaction AFO: Anterior tibial shell controls crouch gait and equinus simultaneously
Supramalleolar orthosis (SMO): Controls subtalar varus while allowing ankle movement; useful when varus is the primary problem
Key principle: Bracing compensates for deformity but does not correct it; most children require surgery as they grow
Indication: Short-term correction of dynamic equinus, often combined with BTX-A
Technique: Above-knee cast changed weekly, gradually correcting equinus and varus
Limitation: Short-lived benefit; deformity recurs once cast removed if underlying spasticity persists
Non-operative treatment is the first line for dynamic equinovarus in young children (typically under 6 years). However, it is a temporising strategy. Approximately 70 to 80 percent of children with spastic equinovarus will eventually require surgery. The goal of conservative care is to maintain ROM and optimise the timing of single-event multilevel surgery (SEMLS), typically performed between ages 6 and 10 years.
The foot is one segment of a child with a global tone problem, and examiners reward the candidate who places foot surgery within the spasticity-management ladder rather than treating the foot in isolation:
- Focal tone reduction: botulinum toxin A (covered) for a few overactive muscles - dynamic, temporary, buys time and predicts the effect of a future lengthening/transfer.
- Generalised tone reduction (medical): oral agents - baclofen, diazepam, dantrolene, tizanidine - help diffuse spasticity but are limited by sedation/systemic effects.
- Intrathecal baclofen (ITB) pump: for severe generalised spasticity/dystonia (often GMFCS IV-V), delivering baclofen to the cord with a far lower systemic dose - reduces tone but does not correct fixed deformity.
- Selective dorsal rhizotomy (SDR): a neurosurgical division of selected dorsal (sensory) rootlets that permanently reduces lower-limb spasticity in carefully selected ambulatory spastic diplegics (typically GMFCS II-III) with good underlying strength - it lowers tone but unmasks (does not fix) any fixed contracture, and many SDR children still need orthopaedic procedures.
The practical rule: address global tone first or concurrently - operating on a foot in a child whose generalised spasticity should be managed by ITB/SDR (or whose dynamic deformity would respond to BTX) risks early recurrence. Foot bony/tendon surgery is for fixed deformity, or dynamic deformity after tone has been optimised, ideally bundled into SEMLS.
Spastic equinovarus is also the classic foot deformity after an upper-motor-neuron insult in the adult (stroke, traumatic brain injury, incomplete spinal cord injury), and examiners use the contrast with the CP child:
- Timing: in the adult, wait for neurological recovery to plateau (commonly about 6 to 12 months) before any irreversible bony/tendon surgery, because spontaneous motor recovery and tone change continue; use BTX-A, serial casting and AFO bracing in the interim. (In CP the deformity is developmental and surgery is timed to growth/SEMLS instead.)
- Deformity is often more FIXED and the equinovarus is typically driven by an overactive tibialis posterior and tibialis anterior plus triceps surae, frequently with toe curling from long-flexor overactivity.
- The "confusion test": ask the patient to flex the hip against resistance - if the tibialis anterior fires inappropriately (the foot dorsiflexes/inverts) it confirms TA as a deforming swing-phase invertor and a SPLATT target; EMG-guided/dynamic assessment likewise identifies TP overactivity.
- Procedures mirror the CP foot but are tone-rebalancing in an adult: TAL/gastrocnemius lengthening, SPLATT, tibialis posterior lengthening or split transfer, and - distinctively - long-toe-flexor release/transfer or fractional lengthening for the curled toes, sometimes with selective motor-branch neurectomy of the deforming muscle. The goal is a plantigrade, braceable, shoeable foot, not normal gait.
Exam point: adult (post-stroke) spastic equinovarus is the same deformity but you wait for neurological plateau (~6-12 months), lean on BTX/casting/AFO first, use the confusion test to plan a SPLATT, and add long-toe-flexor surgery - the principles overlap CP but the timing and the recovery context differ.
Complications
- Incidence
- 10 to 30 percent over 5 to 10 years
- Risk Factors
- Younger age at surgery, higher GMFCS, growth remaining
- Management
- Revision SEMLS; consider repeat gait analysis
- Incidence
- 5 to 15 percent after TAL or TP transfer
- Risk Factors
- Over-lengthening Achilles, over-transfer of TP
- Management
- Avoided by careful intraoperative tensioning; bracing if mild
- Incidence
- 10 to 20 percent after TAL in diplegics
- Risk Factors
- Excessive Achilles lengthening, especially in GMFCS II-III
- Management
- Ground reaction AFO; revision with gastrocnemius advancement
- Incidence
- 2 to 5 percent
- Risk Factors
- Multiple incisions, poor nutrition, GMFCS IV-V
- Management
- Standard wound care; delayed rehabilitation
- Incidence
- Variable, more common with bony procedures
- Risk Factors
- Prolonged immobilisation, multiple simultaneous procedures
- Management
- Early mobilisation protocol, intensive post-op therapy
- Incidence
- 5 to 10 percent
- Risk Factors
- Poor tendon quality, inadequate fixation, early loading
- Management
- Revision transfer or alternative procedure
Over-lengthening the Achilles tendon is one of the most significant complications in CP foot surgery. It produces calcaneus gait (heel-strike with absence of push-off) and can progress to crouch gait in diplegic children. Prevention strategies include: using gastrocnemius recession (Baumann or Strayer) rather than TAL whenever the Silfverskiold test is positive; avoiding percutaneous TAL in ambulatory children; and meticulous intraoperative tensioning. Once established, calcaneus gait is difficult to salvage and may require gastrocnemius advancement or tendon transfer.
Outcomes and Prognosis
- Typical Procedure
- SEMLS (GR + SPLATT ± TP lengthening)
- Expected Outcome
- Near-normal gait, excellent satisfaction
- Long-term Function
- Community ambulation, sport participation possible
- Typical Procedure
- SEMLS (GR + SPLATT + TP procedure)
- Expected Outcome
- Significant gait improvement, reduced tripping
- Long-term Function
- Independent community ambulation maintained
- Typical Procedure
- SEMLS (comprehensive, may include bony)
- Expected Outcome
- Improved gait efficiency, reduced assistive device need
- Long-term Function
- Maintained household to community ambulation
- Typical Procedure
- Positioning procedures, talectomy or fusion
- Expected Outcome
- Improved comfort and bracing tolerance
- Long-term Function
- Comfortable sitting, standing transfers
- Typical Procedure
- Palliative (release, talectomy for positioning)
- Expected Outcome
- Comfort, hygiene, skin breakdown prevention
- Long-term Function
- Pain-free positioning
Best prognosis: GMFCS I-II, dynamic deformity, ambulatory, good selective motor control, good balance, age 7 to 10 at surgery, compliant with post-operative therapy
Poor prognosis: GMFCS IV-V, fixed bony deformity, poor selective motor control, absent balance reactions, age under 5 at surgery (high recurrence), poor compliance with rehabilitation
Key message: SEMLS produces durable results in GMFCS I-III, with approximately 80 to 90 percent maintaining improved gait at 5-year follow-up. Recurrence is the main concern in younger children and higher GMFCS levels.
Guidelines, Registries & Global Practice
- Cerebral palsy affects approximately 2 to 3 per 1000 live births worldwide, with higher rates in preterm and low-birth-weight infants
- Equinovarus is the most common foot deformity in CP, affecting approximately 15 to 30 percent of children with spastic subtypes
- Spastic diplegia has the highest association with bilateral equinovarus; hemiplegia typically produces unilateral deformity
- Global variation: Higher CP prevalence in low-resource settings due to higher preterm birth rates and limited perinatal care; however, access to gait analysis and SEMLS is concentrated in high-resource centres
- High-resource centres: 3-D gait analysis before SEMLS, custom AFOs, BTX-A programmes, specialist CP gait laboratories
- Middle-resource: Clinical gait analysis, BTX-A available, surgical SEMLS performed but with limited gait lab guidance
- Low-resource: Limited BTX-A access, clinical examination-based surgical decisions, limited post-operative rehabilitation, higher recurrence rates
- Universal principle: The surgical principles (dynamic vs fixed, TA vs TP driven, avoid over-lengthening) apply regardless of resource setting
- Assessment Emphasis
- 3-D gait analysis gold standard for surgical planning; GMFCS-based goals
- Surgical Approach
- SEMLS preferred over staged procedures; gastrocnemius recession over TAL when possible
- Key Recommendation
- Evidence-based care pathway: conservative first, then SEMLS at age 6 to 10
- Assessment Emphasis
- Gait analysis before SEMLS in GMFCS I-III; careful dynamic vs fixed assessment
- Surgical Approach
- Gastrocnemius recession preferred; TAL reserved for fixed equinus; SEMLS model standard
- Key Recommendation
- Multidisciplinary team: orthopaedic surgeon, physiatrist, physiotherapist, orthotist
- Assessment Emphasis
- Gait analysis changes surgical plan in 40 to 60 percent of cases
- Surgical Approach
- SPLATT for TA-driven, TP procedures for TP-driven; address all levels simultaneously
- Key Recommendation
- Post-operative intensive rehabilitation is mandatory for outcome
- Assessment Emphasis
- Standardised follow-up with GMFCS, gait classification, and repeated assessment
- Surgical Approach
- Conservative until age 6 to 7, then SEMLS if progressive despite BTX-A and bracing
- Key Recommendation
- Population-based registry tracking outcomes across Scandinavia
The CPUP (Cerebral Palsy Follow-Up Programme) in Sweden and Scandinavia is the most comprehensive CP surveillance registry, tracking GMFCS, gait classification, interventions, and outcomes from diagnosis through adulthood. It has demonstrated that early and standardised intervention reduces the proportion of children requiring major orthopaedic surgery. The evidence base for CP foot surgery is predominantly Level III-IV (retrospective and prospective cohort studies), with few randomised trials. The SEMLS concept, while widely adopted, is supported by consistent observational evidence rather than RCT data.
Record in every pre-operative CP foot assessment:
- GMFCS level and topographic CP classification (hemiplegia, diplegia, quadriplegia)
- Dynamic vs fixed deformity at each level (equinus, hindfoot, forefoot)
- Silfverskiold test result (positive or negative)
- 3-D gait analysis findings (if available) - which muscles are overactive and when
- Prior treatments: BTX-A (number, timing, response), AFO type and compliance, physiotherapy
- Patient and family goals with realistic expectations documented
Missed TP overactivity (addressing only TA-driven varus with SPLATT without managing the TP) is a common cause of persistent varus and reoperation. Always evaluate both muscles.
Controversies & Areas of Uncertainty
The optimal age for SEMLS is debated. Most surgeons operate between ages 6 and 10 years. Earlier surgery (under 6) has higher recurrence rates due to continued growth and spasticity. Later surgery (over 12) risks fixed bony changes. The trend is toward operating when gait deterioration is documented rather than at a fixed age.
Gastrocnemius recession is preferred when the Silfverskiold test is positive, as it preserves soleus push-off power and reduces calcaneus gait risk. However, some surgeons argue that the distinction is less important than meticulous intraoperative tensioning. The consensus in high-resource practice favours recession for dynamic equinus.
Split transfers (SPLATT, SPOTT) are generally preferred over full transfers because they preserve some native function. However, in severe deformity, full TP transfer may provide greater corrective power. No head-to-head trials exist; choice is guided by severity and surgeon preference.
BTX-A is effective for dynamic deformity but does not prevent eventual surgery in most children. The controversy centres on whether repeated BTX-A cycles delay surgery unnecessarily or provide genuine benefit during growth. Current consensus: BTX-A is a bridge to surgery, not a substitute.
MCQ Practice Points
Q: Which muscle is the primary driver of hindfoot varus in spastic CP equinovarus? A: Tibialis posterior. The TP inverts the subtalar joint and is normally silent during midstance. In spastic CP, TP overactivity during stance produces hindfoot varus. The TA primarily drives forefoot supination and first ray plantarflexion. Distinguishing which muscle dominates the varus is essential for surgical planning.
Q: What is the significance of the Silfverskiold test in equinovarus surgery? A: The Silfverskiold test distinguishes isolated gastrocnemius tightness (dorsiflexion improves by more than 10 degrees with knee flexion) from combined gastrocnemius-soleus tightness (no improvement with knee flexion). A positive test supports gastrocnemius recession rather than TAL, which reduces the risk of over-lengthening and calcaneus gait in ambulatory children.
Q: What is the most important prognostic factor for outcome after SEMLS in CP? A: GMFCS level. GMFCS I-II children have excellent outcomes with durable gait improvement. GMFCS III children have good but more variable outcomes. GMFCS IV-V children have limited ambulatory goals, and surgery focuses on comfort and positioning. Always state the GMFCS level when discussing treatment plans.
Q: Describe the SPLATT procedure and its key anatomical steps. A: SPLATT (split tibialis anterior tendon transfer) splits the TA tendon longitudinally. The medial half remains in situ, preserving dorsiflexion power. The lateral half is passed through the interosseous membrane from anterior to posterior, then routed subcutaneously to insert on the lateral cuneiform or cuboid using a suture anchor or bone tunnel. This converts the lateral half from an invertor to an evertor, correcting dynamic forefoot supination.
Q: What is the most significant preventable complication of Achilles tendon lengthening in CP? A: Over-lengthening causing calcaneus gait. This occurs when TAL is performed instead of gastrocnemius recession in a child with isolated gastrocnemius tightness (positive Silfverskiold). The calcaneus gait results in loss of push-off power and can progress to crouch gait in diplegics. Prevention requires using the Silfverskiold test to select the appropriate procedure and meticulous intraoperative tensioning.
Clinical Imaging
Spastic Equinovarus Foot Deformity in Cerebral Palsy
Images for this topic are sourced separately via the dedicated image pipeline.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old girl with spastic diplegia, GMFCS II, presents with progressive toe-walking and tripping. On examination, she has bilateral equinovarus with hindfoot varus worse on the right. Passive correction is possible but deformity recurs immediately with activity. Silfverskiold test is positive. She has been using hinged AFOs and had BTX-A injections to the gastrocnemius twice with temporary benefit. 3-D gait analysis shows premature heel rise, tibialis posterior active in midstance, and tibialis anterior overactivity in swing. How would you manage this?”
“A 14-year-old boy with spastic hemiplegia, GMFCS I, presents with a progressive right equinovarus foot deformity. He has had no prior surgical treatment. On examination, he has a fixed hindfoot varus with equinus that does not correct under examination. Weight-bearing lateral X-ray shows talar flattening and decreased calcaneal pitch. He walks on the lateral border of his right foot with pain over the base of the fifth metatarsal. How would you investigate and manage this?”
Key Anatomy & Pathophysiology
- Gastrocnemius-soleus spasticity drives equinus; TP drives hindfoot varus; TA drives forefoot supination
- Peroneals (evertors) are weak antagonists that cannot oppose inversion
- Dynamic deformity corrects under GA (spasticity alone); fixed deformity persists (contracture and bone)
- Untreated dynamic deformity progresses to fixed contracture with secondary bony deformation
Assessment
- Silfverskiold test: positive = isolated gastrocnemius tightness (do recession, not TAL)
- Examine under GA: confirms dynamic vs fixed at each level
- 3-D gait analysis: gold standard; changes surgical plan in 40 to 60 percent of cases
- GMFCS level: single most important prognostic factor - always state it
Surgical Algorithm (SEMLS)
- Equinus: Gastrocnemius recession (dynamic) or TAL (fixed); avoid over-lengthening
- Hindfoot varus (TP-driven): TP intramuscular lengthening (dynamic) or Z-lengthening / split transfer (fixed)
- Forefoot supination (TA-driven): SPLATT - split TA, lateral half through interosseous membrane to cuboid
- Timing: SEMLS at age 6 to 10 years; all levels in one sitting; 6 to 12 months post-op rehabilitation
Complications to Avoid
- Over-lengthening Achilles = calcaneus gait (use Silfverskiold to choose recession over TAL)
- Recurrent deformity = 10 to 30 percent over 5 to 10 years, higher in younger children and higher GMFCS
- Missed TP overactivity = persistent varus after SPLATT alone
- Crouch gait = over-lengthened Achilles in diplegics, requires ground reaction AFO or revision
Evidence Base
The split anterior tibialis tendon transfer procedure for spastic equinovarus foot in children with cerebral palsy: results and factors associated with a failed outcome
- SPLATT achieved correction in most children but younger age at surgery and severe spasticity predicted poorer outcomes and recurrence
Split tibialis posterior tendon transfer for correction of spastic equinovarus hindfoot deformity
- Split TP transfer reliably corrected spastic equinovarus hindfoot deformity with good maintenance of correction at follow-up
Modified split tendon transfer of posterior tibialis muscle in the treatment of spastic equinovarus foot deformity: long-term results and comparison with the standard procedure
- Modified split TP transfer demonstrated durable long-term correction comparable to standard split transfer with low recurrence rates
Correction of severe crouch gait in patients with spastic diplegia with use of multilevel orthopaedic surgery
- Multilevel orthopaedic surgery including foot procedures produced significant and sustained improvements in gait parameters at mean 3-year follow-up in spastic diplegia