Anterior Rotator Cuff | Internal Rotation | Lesser Tuberosity
FOX & ROMEO CLASSIFICATION
Critical Must-Knows
- Subscapularis = internal rotator, anterior cuff, inserts on lesser tuberosity
- Upper fibers tear most commonly (within biceps sheath)
- Comma sign = SGHL/coracoid ligament complex indicates superior edge
- Lift-off and bear-hug tests for clinical diagnosis
- Biceps pathology frequently associated
Clinical Pearls
- "Napoleon and lift-off tests assess subscapularis function
- "Fox & Romeo classification based on tear extent
- "Upper 50% needs repair, lower 50% may be debridement only
- "Biceps subluxation/dislocation common with subscapularis tears
Clinical Imaging
Imaging Gallery




Critical Subscapularis Exam Points
Comma Sign
The comma sign is the SGHL/coracoid ligament complex that runs with the superior edge of the subscapularis. In complete tears, this tissue becomes visible and indicates where repair should begin. It is a key arthroscopic landmark.
Upper Fibers First
Upper subscapularis fibers tear first because they are intra-articular (within the biceps sheath). Full-thickness tears extend from superior to inferior. Lower fibers are extra-articular and more protected.
Biceps Association
Subscapularis tears frequently involve the biceps pulley. Biceps may be subluxed, dislocated, or torn. Always evaluate biceps when assessing subscapularis and consider tenotomy/tenodesis.
Clinical Tests
Lift-off test: Hand behind back, patient lifts hand off back (tests intact subscapularis). Bear-hug test: Hand on opposite shoulder, resist IR. Napoleon test: Hand on abdomen, assess for wrist flexion (indicates weakness).
Subscapularis vs Other Rotator Cuff
| Feature | Subscapularis | Supraspinatus | Infraspinatus |
|---|---|---|---|
| Insertion | Lesser tuberosity | Greater tuberosity | Greater tuberosity |
| Function | Internal rotation | Abduction | External rotation |
| Position | Anterior | Superior | Posterior |
| Tear frequency | 10-25% | Most common | Common with SSP |
SITSSubscapularis - Key Features
| S | Subscapularis Anterior cuff, internal rotation |
| I | Infraspinatus Posterior cuff, external rotation |
| T | Teres minor Posterior cuff, external rotation |
| S | Supraspinatus Superior cuff, abduction |
| S | Subscapularis Anterior cuff, internal rotation | T | Teres minor Posterior cuff, external rotation |
| I | Infraspinatus Posterior cuff, external rotation | S | Supraspinatus Superior cuff, abduction |
Hook:SITS = rotator cuff muscles, Subscapularis is the ONLY internal rotator!
LBNSubscapularis Tests
| L | Lift-off Hand behind back, lift off (Gerber test) |
| B | Bear-hug Hand on opposite shoulder, resist IR |
| N | Napoleon Hand on abdomen, check wrist position |
| L | Lift-off Hand behind back, lift off (Gerber test) |
| B | Bear-hug Hand on opposite shoulder, resist IR |
| N | Napoleon Hand on abdomen, check wrist position |
Hook:LBN = Lift-off, Bear-hug, Napoleon - three tests for subscapularis!
1-2-3-4Fox and Romeo Classification
| 1 | Partial articular surface Debridement +/- repair |
| 2 | Upper 25% complete Arthroscopic repair |
| 3 | Upper 50% complete Arthroscopic repair |
| 4 | Entire tendon Repair +/- tendon transfer |
| 1 | Partial articular surface Debridement +/- repair | 3 | Upper 50% complete Arthroscopic repair |
| 2 | Upper 25% complete Arthroscopic repair | 4 | Entire tendon Repair +/- tendon transfer |
Hook:Fox and Romeo 1-2-3-4: Partial → 25% → 50% → Full!
Overview and Epidemiology
Why Subscapularis Matters
Subscapularis tears were historically underdiagnosed. They cause internal rotation weakness and anterior shoulder dysfunction. Associated biceps problems are common. Repair restores the anterior restraint and force couple balance. Recognition and appropriate treatment improve outcomes.
Demographics
- Males predominate (occupational factors)
- 5th-6th decade common age
- Trauma or degeneration etiology
- Heavy laborers at higher risk
- Often with other cuff tears (anterosuperior)
Etiology
- Traumatic: Hyperextension, forced ER
- Degenerative: Anterior impingement
- Iatrogenic: Shoulder surgery (arthroplasty)
- Associated with massive cuff tears
- Subcoracoid stenosis contributes
Pathophysiology and Mechanisms
Subscapularis Anatomy - Essential
The subscapularis is the ONLY internal rotator of the rotator cuff. It inserts on the lesser tuberosity via a broad tendon. The upper 60% is tendinous (can be repaired with anchors), the lower 40% is muscular (cannot hold sutures well). The biceps tendon runs in the groove between subscapularis and supraspinatus.
Subscapularis Fiber Properties
| Region | Tissue Type | Repair Considerations |
|---|---|---|
| Upper 60% | Tendinous | Can hold sutures, anchor repair |
| Lower 40% | Muscular | Poor suture holding, may need margin convergence |
Key Landmarks
- Lesser tuberosity insertion
- Biceps groove (lateral border)
- Comma sign (SGHL complex at superior edge)
- Coracoid process (anterior landmark)
- Biceps pulley at junction with SSP
Biomechanical Function
- Internal rotation - primary function
- Anterior stabilizer of humeral head
- Force couple with infraspinatus/teres minor
- Humeral head depressor (with other cuff)
- Loss disrupts force couple balance
Comma Sign
The comma sign is the Superior Glenohumeral Ligament (SGHL) and coracoid ligament complex. It runs adjacent to the superior edge of the subscapularis. In complete tears, this tissue hangs like a comma and indicates where the superior edge is located - critical for repair.
Classification Systems
Fox & Romeo Classification
| Type | Tear Extent | Treatment |
|---|---|---|
| Type 1 | Partial articular surface tear | Debridement +/- repair if over 50% thickness |
| Type 2 | Complete tear of upper 25% | Arthroscopic repair with anchors |
| Type 3 | Complete tear of upper 50% | Arthroscopic repair with anchors |
| Type 4 | Complete tear of entire tendon | Repair +/- tendon transfer (pec major) |
This classification guides surgical decision-making based on tear extent.
Clinical Assessment
History
- Anterior shoulder pain
- Internal rotation weakness (e.g., tucking shirt)
- Trauma (hyperextension, forced ER)
- Prior shoulder surgery (arthroplasty risk)
- Associated symptoms of biceps pathology
Examination
- Lift-off test (Gerber)
- Bear-hug test
- Napoleon test (belly-press)
- Internal rotation lag sign
- Biceps assessment (Speed's, Yergason's)
Clinical Tests Explained
Lift-off test: Patient places hand behind back, attempts to lift hand off back against resistance. Positive if unable (indicates subscapularis weakness).
Bear-hug test: Hand on opposite shoulder, resist examiner pushing arm into ER. Positive if weakness.
Napoleon/Belly-press: Hand on abdomen, press inward. If wrist flexes (rather than staying straight), indicates subscapularis weakness as patient compensates.
Investigations
Investigation Protocol
AP, axillary, outlet views. Limited value for soft tissue. May show lesser tuberosity changes or biceps groove abnormalities. Rule out arthritis or fracture.
Dynamic assessment of subscapularis. Operator-dependent but can visualize tears. Less reliable than MRI for subscapularis specifically.
Best imaging modality. Axial views show subscapularis and lesser tuberosity insertion. Sagittal views assess fatty infiltration. Assess for biceps subluxation/dislocation.
MRI Findings
On axial MRI, look for: tendon discontinuity at lesser tuberosity, biceps subluxation (medial to the groove), fatty infiltration on sagittal views (Goutallier classification), and associated supraspinatus pathology (anterosuperior cuff tears).
Management Algorithm
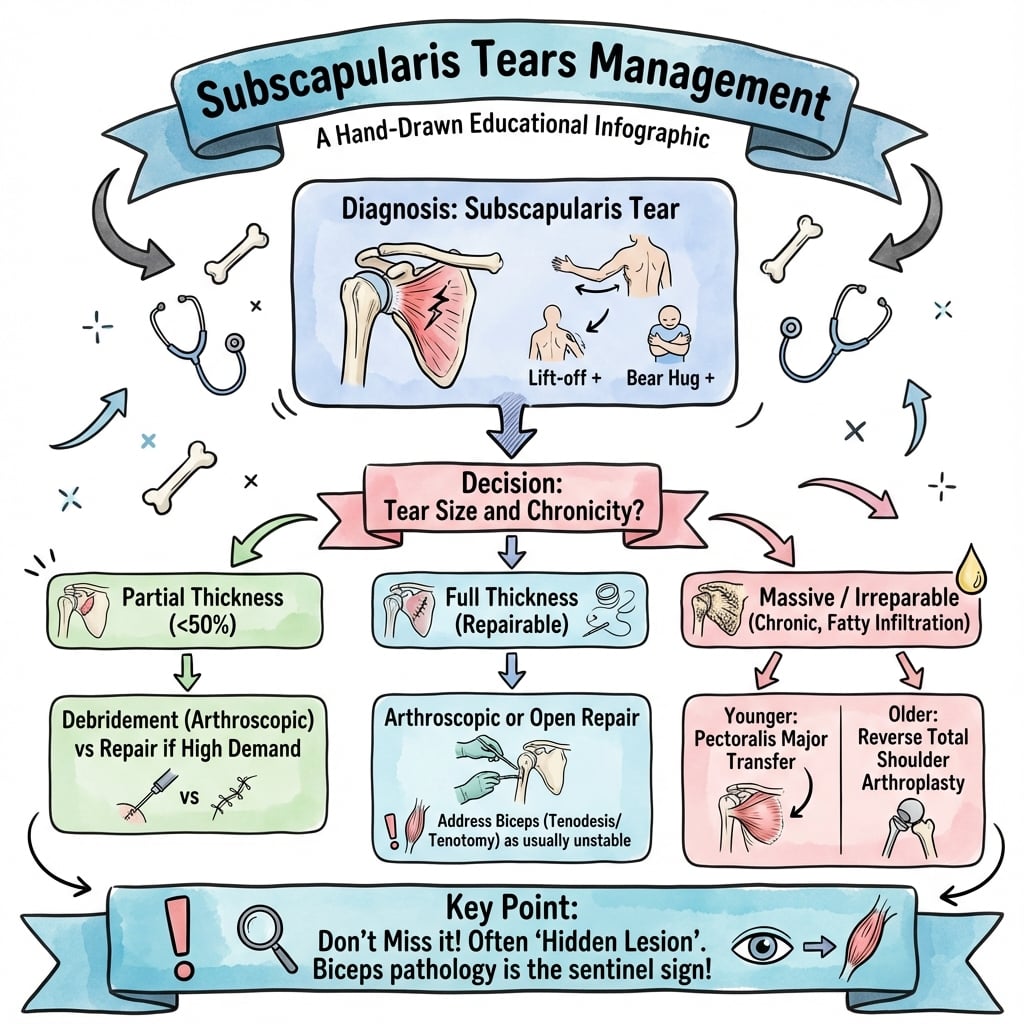
Treatment by Classification
Type 1 (Partial tears):
- Debridement if under 50% thickness
- Repair if over 50% thickness or painful
- Address biceps pathology
Type 2-3 (Upper 25-50%):
- Arthroscopic repair with suture anchors
- Lesser tuberosity anchor placement
- Biceps tenotomy/tenodesis commonly needed
Type 4 (Complete):
- Attempt primary repair if tissue quality adequate
- Consider pectoralis major transfer if irreparable
- Fatty infiltration affects reparability
Surgical management guided by tear extent, tissue quality, and patient factors.
Pre-operative Planning
Imaging Review
- Confirm tear extent on MRI
- Assess fatty infiltration (Goutallier)
- Evaluate biceps position
- Look for associated supraspinatus tear
- Coracoid morphology assessment
Surgical Planning
- Beach chair or lateral position
- Prepare for biceps procedure
- Plan anchor number and placement
- Consider subcoracoid decompression if stenosis
- Pec major transfer backup if irreparable
Surgical Technique
Visualization
Standard posterior portal viewing:
- Rotate arm into external rotation to see subscapularis insertion
- Identify lesser tuberosity
- Assess biceps tendon and pulley
- Look for comma sign if complete tear
Key landmarks:
- Biceps groove (lateral border of subscapularis)
- Lesser tuberosity (insertion site)
- Comma sign (superior edge in complete tears)
- Coracoid process (anterior)
Complete subscapularis visualization requires external rotation of the arm.
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Re-tear | 10-30% | Large tears, fatty infiltration | Careful patient selection, good technique |
| Stiffness | 5-15% | Prolonged immobilization | Appropriate rehab protocol |
| Nerve injury | Rare | Anterior instrumentation | Anatomic awareness |
| Persistent pain | Variable | Associated pathology, CRPS | Address all pathology |
Nerve at Risk
The axillary nerve runs anteroinferiorly. The musculocutaneous nerve enters coracobrachialis near the coracoid. Anterior instrumentation should be cautious. Subcoracoid decompression must avoid overly aggressive bone removal near the coracoid tip.
Postoperative Care and Rehabilitation
Rehabilitation Phases
Recovery Timeline
Sling immobilization in neutral rotation. Avoid internal rotation. Passive external rotation only. Elbow and hand exercises.
Active-assisted ROM. Begin internal rotation. Avoid resisted IR until 10-12 weeks.
Progress active ROM. Begin isotonic strengthening. Internal rotation strengthening begins.
Progressive strengthening. Sport-specific activities. Return to full activity 4-6 months.
Protocol protects subscapularis repair from early internal rotation loading.
Outcomes and Prognosis
Outcomes by Tear Type
| Tear Type | Repair Success | Prognosis |
|---|---|---|
| Partial (Type 1) | Excellent | Best outcomes |
| Upper 25-50% (Type 2-3) | Good | Favorable with repair |
| Complete (Type 4) | Variable | Depends on tissue quality |
| Fatty infiltration | Reduced | Consider transfer |
Prognostic Factors
Favorable: Smaller tears (Type 1-2), acute tears, minimal fatty infiltration, younger patients, isolated subscapularis tear.
Unfavorable: Larger tears (Type 4), chronic tears, significant fatty infiltration (Goutallier 3-4), older patients, combined anterosuperior tears.
Evidence Base and Key Trials
Arthroscopic Repair of Isolated Subscapularis Tears (Lafosse)
- Prospective series of 17 all-arthroscopic isolated subscapularis repairs
- Relative Constant score improved 58% to 96% (p under 0.05)
- UCLA score improved 16 to 32 points; repair intact on CT arthrography in 15 of 17
- No progression of fatty infiltration after durable repair
Fox and Romeo Classification of Subscapularis Tears
- Four-grade scheme: partial articular, upper 25%, upper 50%, complete
- Tear extent guides debridement vs anchor repair vs transfer
- Most widely cited subscapularis classification in exams
The Comma Sign: Arthroscopic Guide to the Torn Subscapularis
- Defined the comma sign as an arc of the SGHL/coracohumeral ligament complex
- Marks the superolateral corner of a retracted subscapularis stump
- Aids identification in chronic tears scarred to deltoid fascia
The Bear-Hug Test for Subscapularis Tears
- 68 consecutive patients, arthroscopy as reference standard (Level I diagnostic)
- Bear-hug most sensitive (60%) vs belly-press 40%, Napoleon 25%, lift-off 18%
- All tests highly specific (lift-off 100%, bear-hug 92%)
- Lift-off only becomes positive once over 75% of tendon is torn
Pectoralis Major Transfer for Irreparable Subscapularis Rupture
- 12 patients with irreparable subscapularis tears; superior pectoralis major routed behind conjoint tendon
- 9 of 12 rated excellent or good at mean 28 months
- Constant-Murley improved from 27% to 67% of normal
- All 4 preoperatively unstable shoulders became stable
Lift-Off Test and Isolated Subscapularis Rupture (Gerber)
- 16 men with isolated subscapularis rupture from forced hyperextension/external rotation
- Introduced the lift-off test, which reliably diagnosed or excluded relevant tears
- Injured shoulders showed increased external rotation and reduced internal-rotation strength
- Axillary nerve must be protected during open repair
Goutallier Grading of Fatty Muscle Degeneration
- Five-stage CT grading of cuff muscle fatty degeneration in 63 patients
- Advanced fatty degeneration does not reverse after repair and worsens with time
- High-grade infiltration strongly predicts poorer surgical outcome
- Supports operating before irreversible muscle change occurs
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Subscapularis Assessment (~2-3 min)
"A 55-year-old man has anterior shoulder pain and weakness with internal rotation after a fall. How do you assess for subscapularis tear?"
Scenario 2: Subscapularis Repair (~2-3 min)
"During shoulder arthroscopy, you identify a complete tear of the upper 50% of subscapularis with biceps subluxation. Describe your management."
Scenario 3: Irreparable Subscapularis (~2 min)
"A 60-year-old man has complete subscapularis tear with Goutallier grade 4 fatty infiltration. MRI shows significant muscle atrophy. What are your options?"
MCQ Practice Points
Insertion Question
Q: Where does the subscapularis insert? A: Lesser tuberosity - The subscapularis is the only rotator cuff muscle to insert on the lesser tuberosity. The other three cuff muscles (supraspinatus, infraspinatus, teres minor) insert on the greater tuberosity.
Function Question
Q: What is the primary function of the subscapularis? A: Internal rotation - The subscapularis is the ONLY internal rotator of the rotator cuff. It also provides anterior stability and contributes to the humeral head depressor function as part of the force couple.
Comma Sign Question
Q: What is the comma sign? A: The Superior Glenohumeral Ligament (SGHL) and coracoid ligament complex - This tissue runs adjacent to the superior edge of the subscapularis and becomes visible as a "comma" in complete tears. It marks where repair should begin.
Classification Question
Q: In Fox & Romeo classification, what is a Type 3 subscapularis tear? A: Complete tear of the upper 50% of the tendon - Type 1 = partial articular, Type 2 = upper 25%, Type 3 = upper 50%, Type 4 = entire tendon.
Clinical Test Question
Q: What clinical tests assess subscapularis function? A: Lift-off test (Gerber), Bear-hug test, Napoleon (belly-press) test - Lift-off tests ability to internally rotate against resistance with hand behind back. Bear-hug resists ER with hand on opposite shoulder. Napoleon assesses wrist position during belly-press.
Associated Pathology Question
Q: What pathology is commonly associated with subscapularis tears? A: Biceps pathology (subluxation, dislocation, tears) - The biceps pulley is at the junction of subscapularis and supraspinatus. Subscapularis tears often disrupt the pulley, causing biceps instability. Always address biceps at surgery.
Guidelines, Registries & Global Practice
Global epidemiology. Subscapularis involvement is found in roughly 10-25% of surgically treated rotator cuff tears, but arthroscopic series report a far higher rate of upper-fibre lesions (up to 27-30% of all shoulder arthroscopies in some cohorts) once surgeons actively look for them. The classic isolated traumatic tear (forced hyperextension/external rotation) affects predominantly middle-aged men; degenerative anterosuperior tears affect both sexes in the 6th-7th decades.
Guideline & Society Positions (Side by Side)
| Body | Imaging / Diagnosis | Surgical Stance |
|---|---|---|
| AAOS (US) | MRI/MR-arthrogram for cuff integrity; clinical tests emphasised | Repair symptomatic full-thickness tears; address biceps pulley |
| BOA / BESS (UK) | Ultrasound or MRI per local access; structured shoulder pathway | Repair in active patients; conservative trial for low-demand/degenerate |
| AO Foundation | Define tear extent and reparability pre-op | Anchor repair of upper fibres; transfer if irreparable |
| EFORT / European consensus | Goutallier (CT) or Fuchs (MRI) fatty grading routine | Grade 3 to 4 infiltration shifts decision toward transfer/reverse |
Registry & Outcome Signal
- No dedicated cuff registry; evidence is from cohort series and reverse-arthroplasty registries (NJR, AOANJRR, AJRR)
- Reverse total shoulder registries show subscapularis status influences stability and internal-rotation outcome
- Re-tear rates after subscapularis repair reported 10-30%, higher with fatty infiltration
Resource-Setting Variation
- High-resource: MRI/MR-arthrogram, arthroscopic anchor repair, intra-op biceps tenodesis
- Limited-resource: ultrasound-led diagnosis, open repair, biceps tenotomy preferred (cheaper, no implant)
- Tendon transfer and reverse arthroplasty availability drives salvage choice globally
Differential Diagnosis
Anterior Shoulder Pain / Internal-Rotation Weakness - Differential
| Diagnosis | Distinguishing Feature | Key Test / Imaging |
|---|---|---|
| Subscapularis tear | IR weakness, increased passive ER, anterior pain | Positive bear-hug/lift-off; axial MRI tendon gap |
| Isolated biceps pulley lesion / LHB instability | Bicipital groove pain, painful arc, often normal IR strength | Speed/Yergason positive; MRI medial biceps subluxation, intact subscap |
| Anterosuperior (subscap + supraspinatus) tear | Combined IR and abduction weakness, pseudoparalysis if massive | MRI both tendons; sagittal fatty grading |
| Subcoracoid impingement | Pain on flexion/IR/adduction, no true weakness | Coracohumeral interval under 6 mm on axial MRI |
| Anterior glenohumeral instability | Apprehension, history of dislocation, age under 30 | Apprehension/relocation; MR-arthrogram labral lesion |
| Adhesive capsulitis | Global loss of passive ROM (esp. ER), stiffness over weakness | Restricted passive ER; MRI capsular/rotator-interval thickening |
Controversies & Areas of Uncertainty
Biceps: tenotomy vs tenodesis
No clear superiority for function or pain; tenotomy is faster and cheaper but risks Popeye deformity and cramping in younger/active patients. Choice remains age- and demand-driven, not evidence-mandated.
Partial / low-grade tears
Threshold for repairing partial upper-fibre tears (debride vs anchor) is unsettled; many Fox-Romeo Type 1 lesions are treated by addressing the biceps pulley alone with good results.
Single-row vs double-row
Lesser-tuberosity footprint is small; whether double-row/anchor density improves subscapularis healing over single-row is not established and extrapolated from posterosuperior cuff data.
Salvage for irreparable tears
Pectoralis major (subcoracoid vs supracoracoid) vs latissimus/lower-trapezius transfer vs reverse arthroplasty: no head-to-head trials; selection is guided by age, arthritis and remaining cuff.
SUBSCAPULARIS TEARS
Clinical summary
Definition
- •Tear of subscapularis tendon
- •Inserts on lesser tuberosity
- •Only internal rotator of rotator cuff
- •Upper fibers (intra-articular) tear first
Fox & Romeo Classification
- •Type 1: Partial articular surface
- •Type 2: Upper 25% complete
- •Type 3: Upper 50% complete
- •Type 4: Entire tendon complete
Clinical Tests
- •Lift-off test (Gerber) - hand behind back
- •Bear-hug - hand on opposite shoulder
- •Napoleon (belly-press) - hand on abdomen
- •Positive = weakness/compensation
Key Anatomy
- •Lesser tuberosity insertion
- •Comma sign = SGHL complex (superior edge)
- •Upper 60% tendinous (repairable)
- •Lower 40% muscular (poor suture holding)
Associated Pathology
- •Biceps subluxation/dislocation common
- •Anterosuperior cuff tears
- •Biceps pulley disruption
- •Always address biceps at surgery
Outcomes
- •70-90% good/excellent if repairable
- •Fatty infiltration reduces success
- •Pec major transfer if irreparable
- •Return to activity 4-6 months