Failure of Digital Separation
- Simple: Skin only connection between digits.
- Complex: Bone, joint, or nail involvement.
- Complete: Web extends to fingertip.
- Incomplete: Partial webbing (proximal only).
- Border Digits (thumb-index, ring-small): Operate earlier (6-12 months) due to length inequality causing angular deformity.
- “3rd web space most commonly affected
- “Border digits need EARLIER surgery (6-12mo)
- “NEVER release both sides of digit at once
- “Full-thickness skin graft (usually groin)
- “Web creep is most common complication
Border digit syndactyly (thumb-index, ring-small) requires EARLIER surgery at 6-12 months.
- Reason: Length inequality between adjacent digits
- The shorter digit tethers and angulates toward the longer one
- Delayed surgery causes permanent angular deformity
- First web space (thumb-index) is functionally critical
Skin Only Connection
- Soft tissue bridge
- No bony involvement
- Separate nail folds
- Straightforward surgery
Bone/Joint Involvement
- Shared bony elements
- Abnormal joints
- May share nails
- Osteotomy required
Complex + Accessory
- Complex features PLUS
- Accessory phalanges
- Multiple deformities
- Syndromic association
- Simple
- Skin/soft tissue only
- Complex
- Bone, joint, nail involved
- Simple
- Normal bony anatomy
- Complex
- Shared/abnormal bones
- Simple
- Straightforward separation
- Complex
- Osteotomy, nail reconstruction
- Simple
- Excellent function
- Complex
- Good but may need revision
BORDERBORDER Digit Early Surgery
Hook:BORDER digits need early surgery (6-12mo) to prevent angular deformity from length inequality
Overview and Epidemiology
Syndactyly is failure of digital separation during embryological development, representing the most common congenital hand anomaly.
Epidemiology
- Incidence: 1 in 2,000 live births
- Most Common Location: 3rd web space (long-ring fingers)
- Bilaterality: 50% are bilateral
- Male:Female: 2:1 male predominance
- Inheritance: Can be sporadic or autosomal dominant
Embryology
- Digital rays form at 4-5 weeks gestation
- Interdigital separation (apoptosis) occurs at 7-8 weeks
- Syndactyly results from failure of programmed cell death
- Sonic Hedgehog and WNT signalling pathways involved
Associated Syndromes
- Syndactyly Pattern
- Complex, complete - 'mitten hand'
- Other Key Features
- Craniosynostosis, midface hypoplasia
- Syndactyly Pattern
- Simple, often symbrachydactyly
- Other Key Features
- Absent pec major, chest wall anomaly
- Syndactyly Pattern
- Variable syndactyly
- Other Key Features
- Craniosynostosis, polydactyly
- Syndactyly Pattern
- Hands and feet
- Other Key Features
- Craniosynostosis, broad thumbs/toes
Neurovascular Anatomy and Its Surgical Limits
The single most important operative-anatomy point (and a stock viva follow-up) is that the neurovascular bifurcation in a syndactylised web sits more DISTALLY than normal, and this dictates how deep a commissure you can safely create.
- Pattern in syndactyly
- Bifurcates into the two proper digital arteries more distally than normal - sometimes distal to the level of the desired web commissure
- Surgical consequence
- May be unable to deepen the web to the normal level without dividing one proper digital artery; if so, ligate ONE branch (the digit survives on its other proper artery) or stage the release
- Pattern in syndactyly
- Also bifurcates distally, usually a little distal to the artery
- Surgical consequence
- Can be split more proximally by interfascicular microdissection, so the NERVE is rarely the limiting structure - the ARTERY is
- Pattern in syndactyly
- Each separated digit ends up perfused by a single proper digital artery on its newly raw side
- Surgical consequence
- This is the anatomical reason you must NEVER release both borders of one digit in the same stage
In complete syndactyly always assume the supply is aberrant: identify the bifurcation early, and if it is too distal, choose between accepting a slightly shallower commissure, ligating one branch, or staging - never blindly dissect proximally through the artery.
In syndactyly the common digital artery bifurcates abnormally distally. If it divides distal to the planned commissure you cannot deepen the web normally without sacrificing a proper digital artery - so you ligate one branch (relying on the digit's other artery) or stage. The nerve can be separated proximally by interfascicular dissection, so it is the artery that sets the limit. This shared-supply anatomy is exactly why both sides of one digit are never released at once.
CRITICAL: When releasing syndactyly in multiple adjacent web spaces, NEVER release both sides of a digit at the same time. This compromises blood supply and can cause digital necrosis. Stage surgery 3-6 months apart.
GRAFTGRAFT for Web Reconstruction
Hook:GRAFT: Groin donor, Rectangular dorsal flap, Acute zigzag angles, Full-thickness graft, Tension-free closure
Pathophysiology
Embryological Development
Digital separation occurs through programmed cell death (apoptosis) of interdigital tissue between weeks 6-8 of gestation. Syndactyly results from failure of this normal apoptotic process.
- Week 4-5: Limb buds appear as paddle-shaped structures
- Week 6: Digital rays become visible within hand plate
- Week 6-8: Interdigital mesenchyme undergoes apoptosis
- Week 8: Digits fully separated with distinct web spaces
- Sonic Hedgehog (SHH) signaling: Regulates anterior-posterior patterning
- WNT signaling pathway: Controls apoptosis of interdigital tissue
- Bone Morphogenetic Proteins (BMPs): Trigger interdigital cell death
- FGFR mutations: Associated with syndromic syndactyly (Apert)
Pathophysiology by Type
- Failure of soft tissue apoptosis only
- Skin and subcutaneous tissue remain connected
- Normal skeletal development
- Often familial with autosomal dominant inheritance
- Abnormal skeletal patterning in addition to soft tissue
- May involve delta phalanges, shared joints
- Associated with FGFR2 mutations in syndromic cases
- More severe embryological disruption
- Isolated syndactyly: Often autosomal dominant with variable penetrance
- Syndromic syndactyly: FGFR2 (Apert), TWIST1 (Saethre-Chotzen)
- Environmental factors rarely implicated
Third Web Space Predilection
The 3rd web space (long-ring) is most commonly affected because these digital rays separate latest in embryological development (week 7-8), providing longer window for developmental disruption.
SCCCSCCC Classification
Hook:SCCC: Simple/Complex describes tissue involvement, Complete/Incomplete describes extent
Classification
By Tissue Involvement
Simple Syndactyly
- Only soft tissue (skin, subcutaneous) connection
- No bony involvement
- Separate nail folds
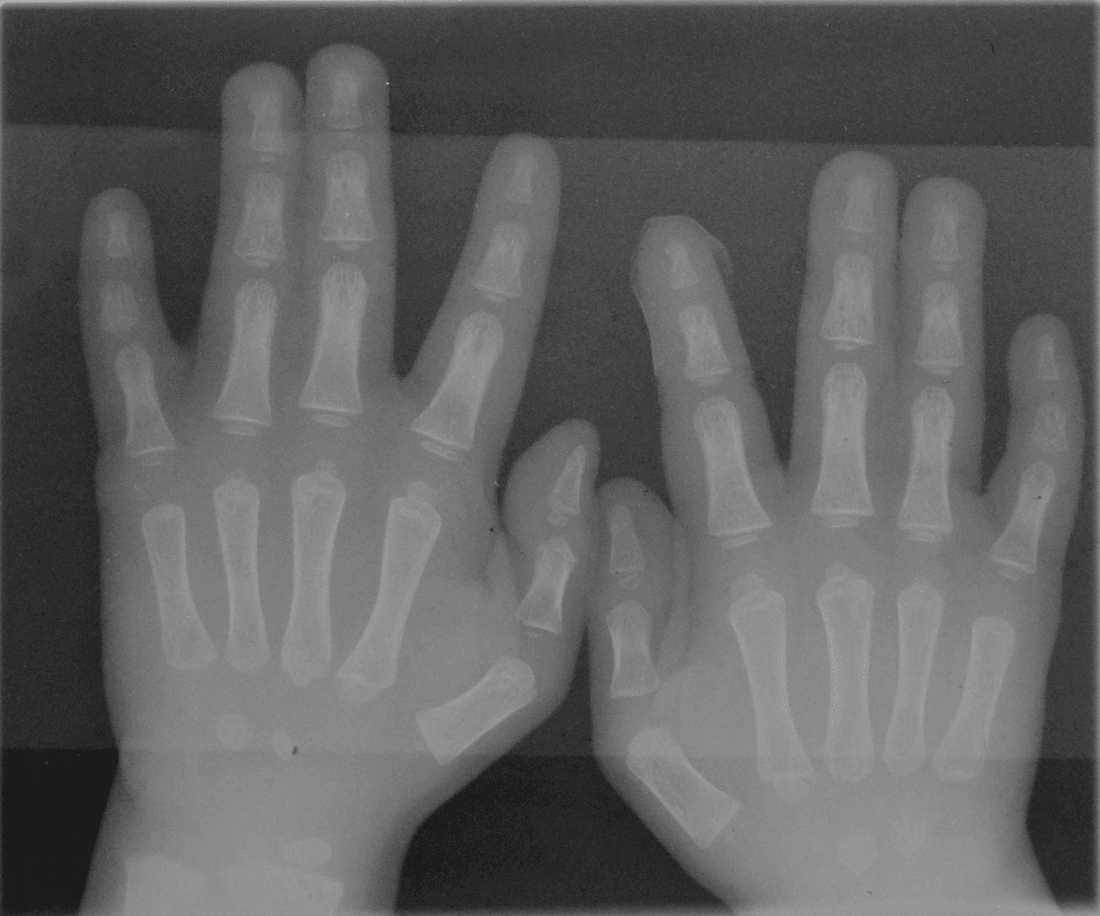
- X-ray shows normal skeletal anatomy
- Most common type (70-80%)
Complex Syndactyly
- Bony connection between digits
- Shared joints or abnormal skeletal elements
- May have shared or abnormal nails
- X-ray shows bone fusion, delta phalanges
- Requires osteotomy during surgery
Complicated Syndactyly
- Complex features PLUS accessory phalanges
- Multiple abnormalities
- Often associated with syndromes
- Most challenging surgical reconstruction
The 3rd web space (between long and ring fingers) is most commonly affected in syndactyly. This relates to embryological timing - the 3rd and 4th digital rays separate last. The 1st web space (thumb-index) is least commonly affected as it separates earliest.
Clinical Assessment
History
- Family history: Autosomal dominant inheritance in some forms
- Pregnancy history: Teratogen exposure, maternal diabetes
- Syndromic features: Head shape, chest wall, other anomalies
- Functional concerns: Grip, fine motor development
Physical Examination
- Extent: Complete vs incomplete
- Which web spaces affected
- Skin quality/scars
- Associated anomalies
- Length discrepancy
- Angular deformity
- Rotation
- Nail appearance (shared?)
- Active movement
- Independent flexion/extension
- Grip patterns
- Opposition (if thumb involved)
Key Examination Points
- Complete vs Incomplete: Does web reach fingertip?
- Simple vs Complex: Palpate for bony connection
- Nail Assessment: Shared nail suggests complex type
- Border Digit Involvement: Assess for angular deformity
- Other Hand Anomalies: Polydactyly, camptodactyly
- Syndromic Features: Head, chest, feet

Investigations
Imaging
- X-ray: Essential for surgical planning
- Assess bony anatomy
- Identify shared/fused bones
- Evaluate joint anatomy
- Detect accessory phalanges
When to Consider Further Investigation
- Genetic Testing: If syndromic features (Apert, Poland)
- Cardiac Echo: Associated cardiac anomalies in syndromes
- CT/MRI: Rarely needed, complex cases only
X-ray Findings by Type
- X-ray Appearance
- Normal bony anatomy
- X-ray Appearance
- Shared phalanges, delta phalanx
- X-ray Appearance
- Accessory bones, abnormal joints
Differential Diagnosis
Not every pair of digits held together is true syndactyly. Distinguish these on examination and radiograph.
- Key Distinguishing Feature
- Failure of separation, digits otherwise formed
- Web / Skeletal Pattern
- Soft-tissue or bony web; digits of near-normal length
- Key Distinguishing Feature
- Short, hypoplastic or absent digits with nail nubbins
- Web / Skeletal Pattern
- Webbing PLUS deficiency; often unilateral, Poland-associated
- Key Distinguishing Feature
- Syndactyly WITH an extra (often central) digit
- Web / Skeletal Pattern
- Web plus duplicated ray, 3rd/4th web region
- Key Distinguishing Feature
- Distal fusion with proximal sinus/fenestration, amniotic bands
- Web / Skeletal Pattern
- Fenestrated web, near-normal proximal commissure, tip fusion
- Key Distinguishing Feature
- Central ray deficiency creating a cleft
- Web / Skeletal Pattern
- Transverse web of border digits flanking a central defect
- Key Distinguishing Feature
- Fixed PIP flexion of a SINGLE digit, no fusion
- Web / Skeletal Pattern
- No web abnormality

Management

Surgical Timing
Border Digits (Thumb-Index, Ring-Small)
- 6-12 months - Earlier surgery
- Reason: Length inequality causes angular deformity
- Shorter digit tethered by longer, bends toward it
- Early release prevents permanent deformity
- First web space critical for thumb function
Central Digits (Index-Long, Long-Ring)
- 12-18 months - Standard timing
- Digits similar length, less deformity risk
- Larger digits easier to operate
- Before fine motor development critical period
Multiple Web Spaces
- Stage surgery - 3-6 months apart
- Never release both sides of same digit at once
- Vascular compromise risk if both sides released
Complex/Syndromic
- May require earlier intervention
- Often staged multiple procedures
- Coordinate with craniofacial team (Apert)
The Skin Deficit: Why a Graft Is Needed
A favourite "explain the principle" question: why can a conjoined web almost never simply be sewn back as two digits?
- The geometry: two separated digits present a far greater combined skin circumference than the flat, fused mass they came from. Separating them therefore creates an obligatory skin shortfall - there is simply not enough skin to wrap both digits and line the new commissure.
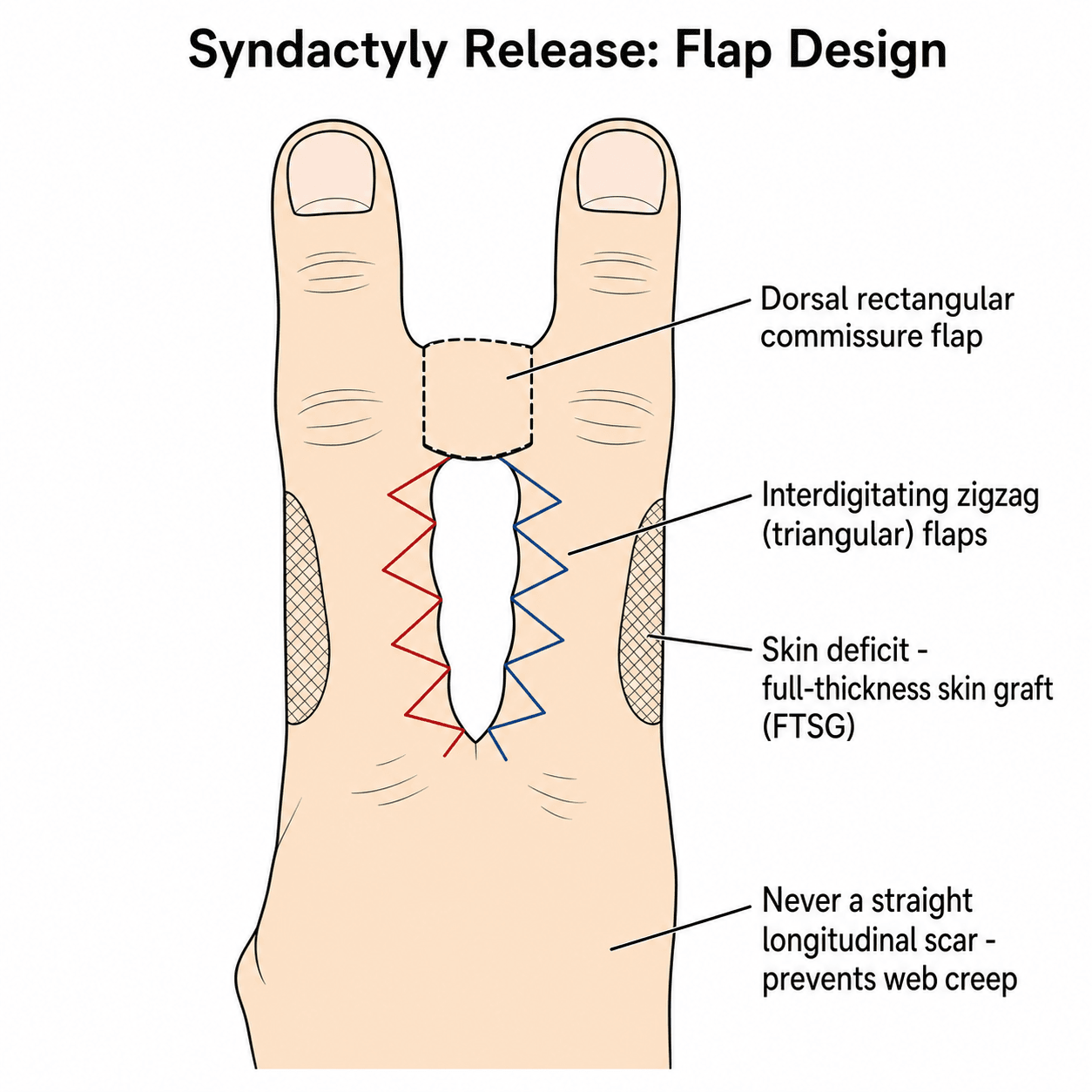
- What the flaps do: the dorsal commissure (rectangular or hourglass) flap resurfaces the new web at the correct level, and the interdigitating zigzag flaps resurface part of each digit while breaking up the scar line.
- What is left over: the residual raw areas - typically on the mid-lateral sides of the digits - are covered with full-thickness skin graft.
This is also why the graft-free debate hinges on web extent: a narrow incomplete web has a small deficit that local and dorsal flaps can cover alone, whereas a complete (and especially complex) web has a large deficit that still generally needs FTSG for tension-free closure.
Two cylinders have a bigger combined surface than the single flat web they were joined as - so syndactyly release creates an unavoidable skin deficit. Flaps recreate the commissure and resurface part of each digit; the leftover mid-lateral raw areas need full-thickness skin graft. The narrower (incomplete) the web, the smaller the deficit - which is why graft-free flap-only closure is realistic only for simple incomplete webs.
Apert syndrome has complex, complete syndactyly often described as "mitten hand" or "spade hand". Surgery is challenging due to shared bony structures and multiple digits involved. Requires staged procedures, often 4-5 operations. Coordinate with craniofacial team for concurrent craniosynostosis management.
CREEPCREEP - Web Creep Prevention
Hook:CREEP prevention: Correct flap, Rectangular commissure, Enough graft, Easy tension, Protect with spacer
Complications
Early Complications
- Vascular compromise: From releasing both sides of digit
- Flap necrosis: Tension, poor design
- Graft failure: Infection, haematoma, poor bed
- Infection: Standard surgical risk
Late Complications
Most Common (10-20%)
- Distal migration of commissure
- Develops over months-years
- Due to inadequate flap/graft
- May need revision surgery
- Linear scars contract
- Zigzag design prevents this
- May need Z-plasty revision
- Hand therapy important
- From delayed surgery in border digits
- May need corrective osteotomy
- Prevention: early surgery
Revision Surgery Indications
- Significant web creep
- Scar contracture limiting function
- Angular deformity
- Nail deformity
- Growth-related changes
Guidelines, Registries & Global Practice
Global Epidemiology
- Syndactyly is among the most common congenital hand anomalies worldwide, with widely quoted figures around 1 in 2,000-3,000 live births (population estimates vary with ascertainment).
- Registry data place overall congenital hand/upper-limb malformation incidence at roughly 1-3 per 10,000 live births, with simple syndactyly consistently among the top anomalies after radial polydactyly.
- Male predominance and a slight right-side preponderance are reported across populations.
- Around 10-20% of hand-anomaly cohorts carry a syndromic association, so every case warrants a screen for dysmorphic, craniofacial, chest-wall and lower-limb features.
Society Guidance Compared
Syndactyly is managed by surgical principle rather than by a single binding national guideline; the table below summarises how the major bodies frame care.
- Emphasis
- Function-led timing and staged release
- Practical Position
- Border digits earlier; never release both sides of one digit in a single stage
- Emphasis
- Paediatric hand MDT pathways
- Practical Position
- Referral to specialist paediatric hand units; FTSG remains standard for complete webs
- Emphasis
- Technique variation and graft-sparing flaps
- Practical Position
- Increasing use of dorsal commissure flaps to reduce or avoid grafting in simple cases
- Emphasis
- Standardised nomenclature
- Practical Position
- Oberg-Manske-Tonkin (OMT) classification adopted to harmonise reporting of malformations
Registry & Classification Notes
- Modern reporting uses the IFSSH-endorsed Oberg-Manske-Tonkin (OMT) classification, which frames syndactyly within malformations of hand-plate formation/differentiation, replacing purely descriptive systems for research and audit.
- The Withey score is the most widely used outcome instrument for grading post-release web creep, scar and digital deformity, allowing cross-centre comparison.
- No implant is involved, so there is no arthroplasty-style registry; epidemiology relies on birth-defect surveillance programmes (e.g. EUROCAT in Europe) and national hand-surgery audits.
High- vs Limited-Resource Practice Variation
- High-resource settings: elective staged release at specialist paediatric hand units, full-thickness grafting or graft-sparing dorsal flaps, formal hand therapy, silicone and night web-spacers, and longitudinal follow-up to skeletal maturity.
- Limited-resource settings: later presentation is common, raising rates of fixed angular deformity in border digits and reducing the window for graft-free techniques; single-stage, graft-minimising approaches and visiting/charitable surgical teams play a larger role.
- Universal principles (resource-independent): zigzag interdigitating incisions, a dorsal flap to recreate the commissure at the correct level, never releasing both borders of one digit simultaneously, and tension-free coverage to limit web creep.
Controversies & Areas of Uncertainty
The traditional teaching is well established, but several points remain genuinely debated and are favourite viva discriminators.
How early is too early?
- Tradition: central digits at 12-18 months
- Some advocate earlier release for psychosocial/parental reasons
- Comparative data suggest releasing central webs under 1 year may WORSEN cosmetic (Withey) scores
- Consensus: border digits early, central digits not rushed below 12 months
Is FTSG always needed?
- Dorsal commissure/V-Y flaps can avoid grafting in simple incomplete webs
- Avoids donor morbidity and graft-related creep
- Complete and complex webs still generally need FTSG for tension-free closure
- Skin substitutes (e.g. dermal matrices) are an evolving option, not standard
Operate at all?
- Largely cosmetic, often a normal familial variant
- High recurrence (up to ~28%) and modest satisfaction
- Recurrence rises if operated after age 2
- Many units counsel against routine surgery
Self-Assessment Quiz
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“6-month-old infant presents with complete simple syndactyly between thumb and index finger. What is your management?”
“10-month-old with complete simple syndactyly involving 2nd, 3rd, and 4th web spaces bilaterally. Parents want all corrected. How do you approach this?”
“Infant with Apert syndrome presents with complex complete syndactyly of all digits ('mitten hand'). Parents ask about treatment options and prognosis. How do you counsel them?”
CLASSIFICATION
- Simple: Skin only connection
- Complex: Bone/joint/nail involved
- Complete: Web to fingertip
- Incomplete: Partial proximal web
- 3rd web space most common
TIMING
- BORDER (thumb-index, ring-small): 6-12 months
- CENTRAL (index-long, long-ring): 12-18 months
- NEVER release both sides of digit at once
- Stage multiple webs 3-6 months apart
SURGICAL TECHNIQUE
- Zigzag interdigitating incisions
- Dorsal rectangular flap for commissure
- Full-thickness skin graft (groin)
- Complex: osteotomy + nail reconstruction
COMPLICATIONS
- WEB CREEP: Most common (10-20%)
- Scar contracture
- Vascular compromise (both sides released)
- Angular deformity (delayed border surgery)
- Nail deformity (complex type)
ASSOCIATED SYNDROMES
- APERT: Mitten hand + craniosynostosis
- POLAND: Symbrachydactyly + absent pec major
- CARPENTER: Craniosynostosis + polydactyly
- PFEIFFER: Broad thumbs/toes + craniosynostosis
Evidence Base
- 34 patients (51 commissures) graded blindly by 3 surgeons using the Withey score
- Children operated under 1 year had a WORSE mean Withey score (5.83) than those over 1 year (3.94), p=0.011
- Higher Withey score reflects more web creep and scar/rotational deformity
- Suggests very early release (under 12 months) of central webs may not improve cosmesis
- 26 children, 39 web reconstructions (median age 20 months) using a hexagonal dorsal flap with midline straight incisions
- Skin grafts needed in only 2 children (reserved for complex/complicated cases)
- Web creep occurred in 1 child (driven by postoperative infection); 2 developed hypertrophic scar
- Mean parental cosmetic VAS 87 and functional VAS 92 at mean 1.3 years
- 28 syndactylies (25 simple incomplete, 3 simple complete) released with a modified V-Y dorsal metacarpal flap WITHOUT skin graft
- Mean follow-up 4.2 years; only 2 patients (7.1%) had complications, both corrected by revision
- Eliminates donor-site morbidity and graft-related web creep in selected cases
- Authors restrict the graftless technique primarily to simple incomplete syndactyly
- 68 toe syndactylies (38 patients), mean follow-up 6.9 years
- Recurrence in 28.1%; surgery after age 2 years was the only independent risk factor for recurrence
- Complication rate 11.7% (mostly keloid); African ethnicity was a risk factor for keloid
- Only ~half of simple toe syndactylies were satisfied, questioning purely cosmetic release
- Multicentre Italian registry: 765 children with hand/upper-limb malformations among 3,100,421 live births
- Overall malformation incidence 2.5 per 10,000 live births, male and right-side predominance
- Simple syndactyly was one of the most frequent anomalies (after radial polydactyly), with complex syndactyly also common
- 84 children had syndromic associations
- 16 Apert hands treated with early staged surgery (mean 6 operations per child)
- First-web opening, digital separation, thumb realignment and clinodactyly correction performed
- Upton classification used to select first-web technique (dorsal hand flap in severe stages)
- Web revision required in 16%; all children achieved a rudimentary functional pinch
- Defined the widely used Upton classification of Apert hand anomalies (types I-III)
- Detailed pathologic anatomy of upper-limb anomalies in Apert syndrome
- Links severity of complex syndactyly to thumb and metacarpal involvement
- Guides the sequence and technique of staged reconstruction
- Classic reference text on congenital hand surgery
- Codified simple/complex and complete/incomplete descriptive terminology
- Established core surgical principles: zigzag flaps, dorsal commissure flap, FTSG
- Foundation for the modern staged approach to syndactyly