Facet Joint Pathology | Cause of Radiculopathy | Indicator of Instability
- Synovial cysts are a marker of underlying FACET JOINT INSTABILITY.
- They most commonly occur at L4/5 (the most mobile segment).
- Spontaneous resolution is rare but possible (cyst rupture).
- Aspiration/Injection has a high failure rate (~30-40% need a repeat procedure or surgery).
- Surgical excision is curative, but may require FUSION if frank instability (spondylolisthesis) is present.
- “Pain is often postural (worse standing/walking) - mimicking Neurogenic Claudication.
- “Unilateral Radiculopathy is the most common presentation.
- “Look for 'Fluid Sign' on MRI (Hyperintense T2) - confirms fluid content.
- “Calcified cysts (Hypointense T2) are adherent and difficult to resect.
Overview and Epidemiology
Definition
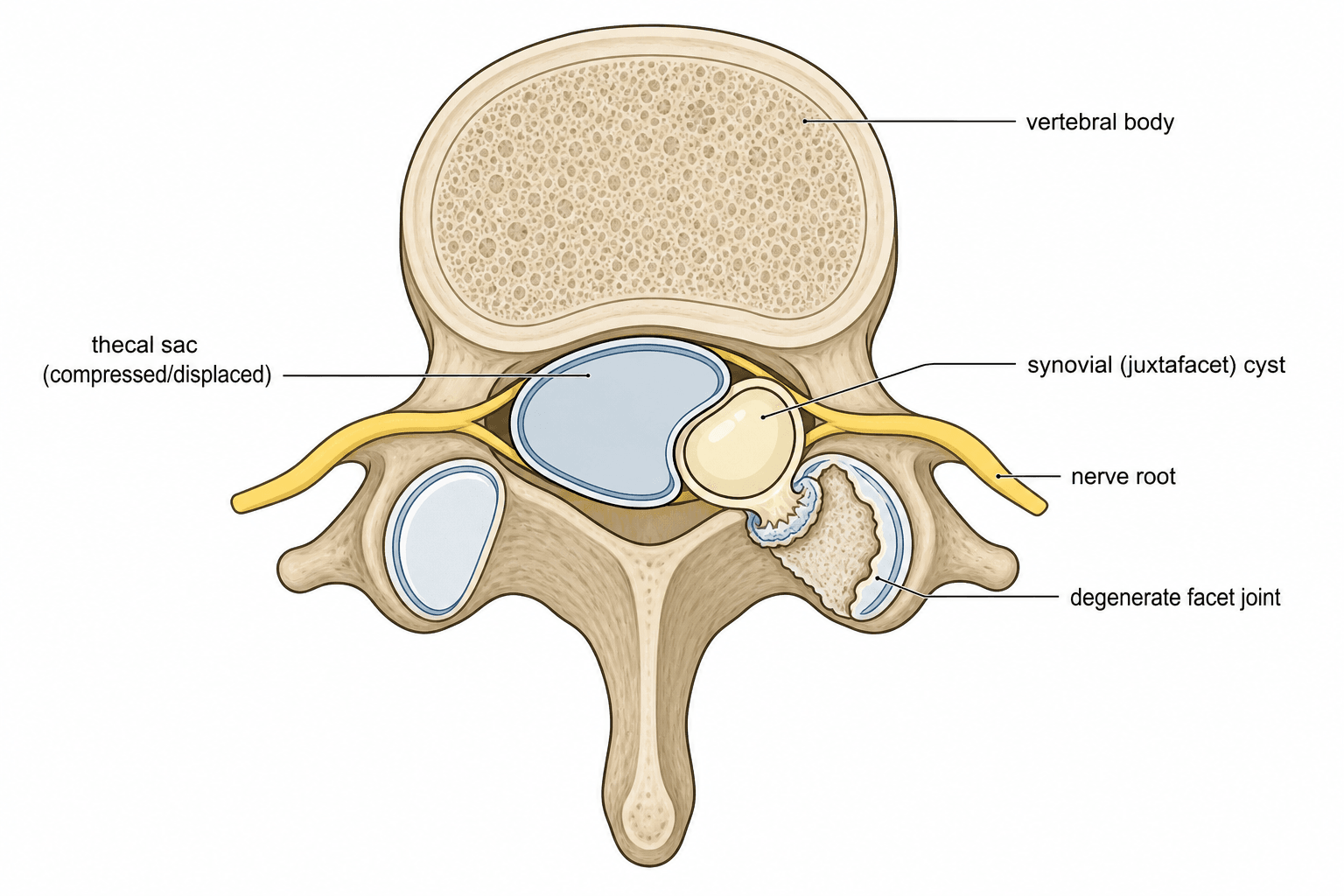
- A juxtafacet (synovial) cyst is a fluid-filled outpouching arising from a degenerate lumbar facet (zygapophyseal) joint that herniates into the epidural space and may compress the traversing or exiting nerve root.
- "Juxtafacet cyst" is the umbrella term (Kao, 1974) covering both true synovial cysts (synovial lining, joint communication) and ganglion cysts (no synovial lining).
Who and where
- Disease of the degenerate spine: peak in the 6th-7th decade, slight female predominance.
- Overwhelmingly lumbar; L4/5 accounts for roughly 75% (the most mobile lumbar segment), followed by L5/S1 and L3/4. Cervical and thoracic cysts are rare (each under 3%) (Bydon 2010).
- Degenerative spondylolisthesis coexists in up to 40-50% of cases — the cyst is regarded as a marker of segmental instability.
Why it matters
- Increasingly diagnosed with widespread MRI use.
- The central exam debate is decompression alone versus decompression plus fusion, driven by the cyst's link to instability.
Pathophysiology and Mechanisms
The Facet Joint
- Synovial joint heavily innervated by medial branch nerves.
- The cyst typically arises from the medial aspect of the joint.
- Occupies the Posterolateral epidural space.
Relationship to Nerve Root
- Compresses the nerve root from Posterior to Anterior.
- (Contrast with Disc Herniation which compresses Anterior to Posterior).
- Clinical Note: This makes the nerve root very superficial during surgery - Risk of injury mainly during initial exposure.
Instability Link
- L4/5 is the most mobile lumbar segment.
- Degenerative Spondylolisthesis is present in up to 40-50% of cases.
- The cyst is the body's attempt to stabilize the joint ("Hydraulic Splint").
Classification Systems
Pathological Classification There is no widely used clinical classification (e.g. AO Spine) specifically for synovial cysts. They are classified based on Pathology or Location.
-
True Synovial Cyst:
- Lined by synovium (cuboidal or pseudo-stratified epithelium).
- Clear communication with the joint space.
- Often reducible with positioning.
-
Ganglion / Pseudocyst:
- No synovial lining but fibrous connective tissue capsule.
- Contains mucinous fluid.
- Often due to myxoid degeneration of the collagen in the joint capsule or Ligamentum Flavum.
- Less likely to reduce.
Clinical Assessment
History
- Radiculopathy: Unilateral leg pain (Sciatica).
- Neurogenic Claudication: Pain worse with walking/standing (Stenosis).
- Postural: Often relieved by sitting (flexion opens the canal).
- Acuity: Can be acute (bleeding into cyst) or subacute/chronic.
Examination
- Lasegue's Sign: Straight leg raise may be positive.
- Motor/Sensory: Deficit corresponding to the level (e.g. L5 EHL weakness).
- Kemp's Test: Extension/Rotation often exacerbates facet pain.
The Acute Haemorrhagic Synovial Cyst
The clinical assessment notes a cyst can present acutely with "bleeding into the cyst," and the imaging section flags that "T1 high signal may indicate haemorrhage" — this distinct presentation is worth developing, because it overturns the usual gradual picture and changes management.
Presentation. Instead of the typical chronic, postural radiculopathy, haemorrhage into the cyst causes sudden, severe radicular pain or rapidly progressive neurological deficit — and, in the lumbar spine, occasionally an acute cauda equina syndrome (the acute CES picture itself is developed in the cauda-equina-syndrome topic). It may be spontaneous or precipitated by minor trauma or, importantly, by anticoagulant / antiplatelet therapy.
Imaging — don't be caught out. Blood changes the expected signal: the cyst becomes T1-hyperintense (methaemoglobin) rather than the usual T1-hypointense fluid, often heterogeneous with fluid-fluid levels, with blooming on gradient-echo / blood-sensitive sequences, and the cyst is typically enlarged and tense. A facet cyst that is bright on T1 should prompt thoughts of haemorrhage, not just proteinaceous fluid.
Management. A haemorrhagic cyst with acute severe pain or a new deficit shifts management away from a conservative or injection trial and toward urgent surgical decompression; review and correct any anticoagulation/coagulopathy as part of the work-up.
Sudden, severe radiculopathy (or acute cauda equina) from a facet cyst suggests intracystic haemorrhage — often spontaneous or anticoagulant-related. The cyst turns T1-hyperintense (methaemoglobin) with fluid-fluid levels/blooming, not the usual T1-dark fluid. Treat it as urgent: prompt imaging, check anticoagulation, and a low threshold for surgical decompression rather than injection.
Imaging and Investigations
Diagnostic Protocol
- AP/Lateral.
- Flexion/Extension Views: CRITICAL to rule out dynamic instability (Spondylolisthesis).
- Look for: Facet hypertrophy, vacuum phenomenon.
- T2 Weighted: Hyperintense (Bright) = Fluid.
- T1 Weighted: Hypointense. High signal may indicate hemorrhage (subacute).
- Gadolinium: Rim enhancement is typical (inflammation).
- Used if MRI contraindicated.
- Shows "filling defect" in the dye column.
- Good for visualizing calcification of the cyst wall.
Management Algorithm
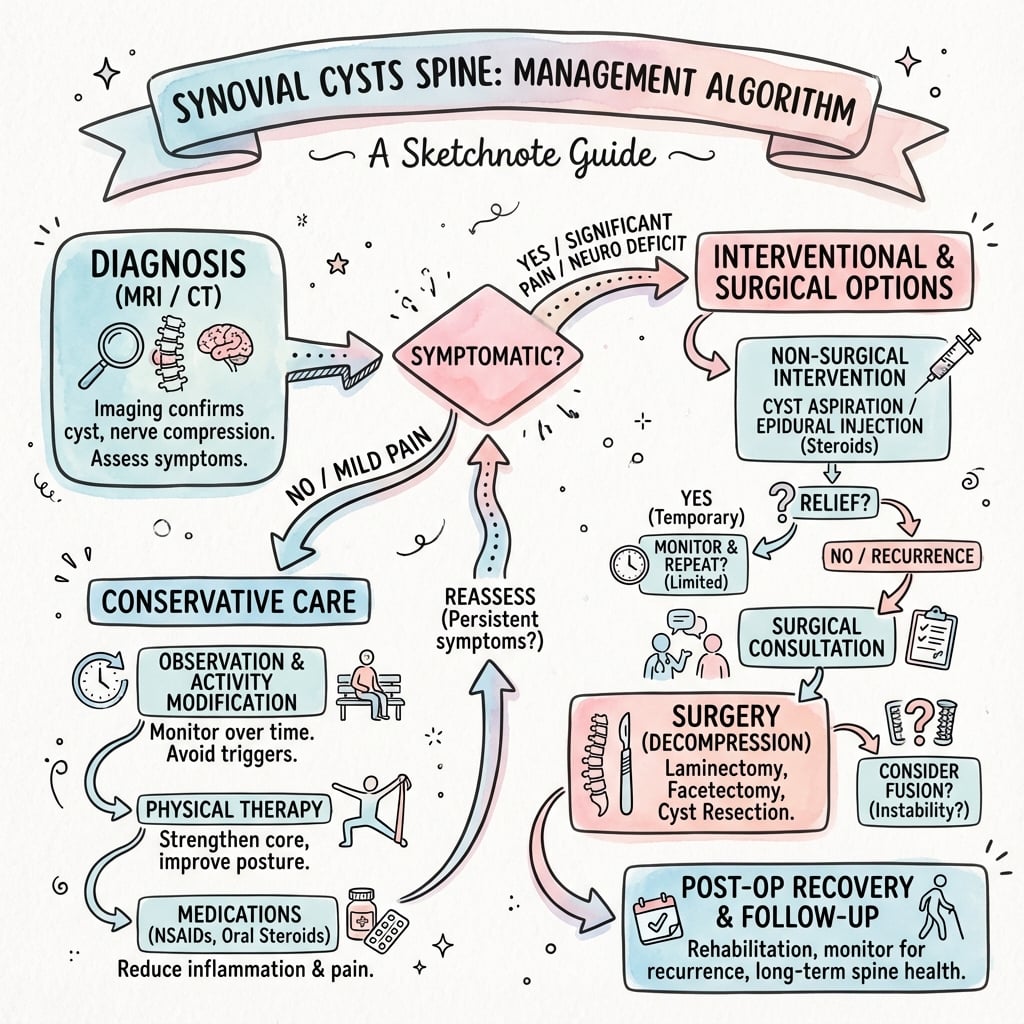
- 1
Symptomatic Cyst
- 2
Pain Persists
- 3
Recurrence / Failure
Percutaneous Cyst Rupture & Aspiration — How It Is Done
The treatment hierarchy, the outcomes and three evidence cards all turn on "percutaneous rupture / aspiration," but the actual procedure is never described — so it is worth setting out, because the technique explains both its appeal and its limited durability.
fluoroscopy or CT.
- Facet injection with forced distension (indirect rupture). A needle is placed into the affected facet joint; contrast confirms intra-articular position and frequently opacifies the cyst — confirming joint communication. Fluid (contrast, local anaesthetic, corticosteroid and/or saline) is then injected under increasing pressure to distend the joint and burst the cyst into the epidural space, decompressing the nerve root, with steroid left behind for its anti-inflammatory effect.
- Direct percutaneous cyst puncture / aspiration. The cyst itself is punctured and aspirated, with or without intracystic steroid — often combined with the distension-rupture above.
Why it works — and why it often does not last. Over-pressurising the joint ruptures the cyst wall, giving immediate root decompression plus a steroid effect. But it does not address the underlying unstable, fluid-pumping facet joint, so the cyst frequently reforms — which is exactly why durability is limited (resolution around 58 percent, roughly 30 to 40 percent needing a repeat procedure and about one-third still proceeding to surgery, per the cited Campbell and Lutz data).
Candidate selection. Best suited to a small, non-calcified cyst that communicates with the joint (allowing indirect distension rupture), and to poor surgical candidates or patients wishing to defer surgery — with explicit counselling that about a third still come to operation. A calcified cyst wall resists rupture and predicts failure. (Detailed facet/epidural injection technique sits within interventional spine practice.)
Percutaneous treatment is image-guided (fluoroscopy/CT): inject the facet joint under pressure to burst the cyst into the epidural space (indirect rupture) with or without direct cyst aspiration, leaving steroid behind. It decompresses the root immediately, but the unstable joint keeps pumping fluid, so durability is limited (~58 percent resolution; about one-third still need surgery). Reserve it for small, non-calcified, joint-communicating cysts or poor surgical candidates.
Surgical Technique
Micro-decompression / Cyst Resection
- Indication: Stable joint (No slip), Leg pain dominant.
- Technique:
- Midline approach or Tubular.
- Laminectomy / Medial Facetectomy.
- Identify cyst (often purple/blue color).
- Dissect plane between Dura and Cyst. CAUTION: Often very adherent.
- Excision.
- Cons: Risk of recurrence or iatrogenic instability.
Complications
- Risk
- High (~8%)
- Note
- Higher than disc herniation due to inflammatory adhesions (MIS series, Garg 2021).
- Risk
- Under 5%
- Note
- 1.8% after decompression alone, 0% after fusion (Bydon 2010).
- Risk
- Variable
- Note
- Post-facetectomy slip progression.
- Risk
- 5%
- Note
- Especially if calcified cyst wall left behind.
Postoperative Rehab
Hospital Stay
- Decompression: Day Case or Overnight (23hr stay).
- Fusion: 2-3 Days.
Restrictions
- Decompression: No heavy lifting (over 10kg) for 6 weeks (Risk of recurrent herniation/cyst through annulotomy if done).
- Fusion: Brace optional (surgeon preference). No bending/twisting/lifting (BLT) for 6-12 weeks until fusion mass forms.
Red Flags in Recovery
- Positional Headache: Potential CSF leak/pseudomeningocele.
- Return of Radiculopathy: Early recurrence or hematoma.
- Fever/Wound Ooze: Infection (Discitis).
Outcomes and Prognosis
- Conservative: Spontaneous regression is documented but rare (Houten 2003).
- Percutaneous (aspiration/rupture): Cyst resolution ~58% vs ~90% for surgery (Campbell 2016); ~30-40% need a repeat procedure and roughly one-third proceed to surgery (Lutz 2017). Useful for temporary control or poor surgical candidates.
- Surgery:
- Back and leg pain relief in ~91-92% (Bydon 2010, Xu 2010).
- Cyst recurrence under 5% after decompression alone (1.8%) and 0% after concomitant fusion (Bydon 2010); fusion also reduces recurrent mechanical back pain (Xu 2010).
Guidelines, Registries & Global Practice
Global epidemiology
- A degenerative condition of the ageing spine; incidence is rising with broader MRI access worldwide. L4/5 predominance (~75%) and the 40-50% association with degenerative spondylolisthesis are consistent across international series (Bydon 2010, Campbell 2016).
Guidelines — note the gap
- There is no dedicated society guideline (AAOS, BOA, AO Spine, EFORT, NASS) specific to lumbar synovial cysts; management is extrapolated from degenerative lumbar stenosis and spondylolisthesis pathways.
- NASS / NICE (degenerative stenosis): trial of conservative care first in the neurologically intact patient; surgery for persistent radiculopathy/claudication or progressive deficit.
- AO Spine / spondylolisthesis principles: where a cyst coexists with documented instability (dynamic slip), decompression plus instrumented fusion is favoured — consistent with the cyst literature.
- Common consensus across societies: micro-decompression with cyst excision is the workhorse for the stable spine; add fusion for instability or recurrence.
Registry note
- Synovial cysts are not separately tracked by arthroplasty registries; where fusion is performed, implant and revision data fall within national spine fusion registries rather than a cyst-specific dataset.
High- vs limited-resource practice
- Well-resourced settings: ready MRI, dynamic radiographs, image-guided percutaneous rupture, and MIS tubular/endoscopic resection are all available, supporting individualised escalation.
- Limited-resource settings: reliance on a single MRI and standing radiographs; open micro-decompression remains the mainstay, with percutaneous and endoscopic options less accessible. Definitive surgery is often favoured over repeated injections to avoid multiple visits.
Controversies & Areas of Uncertainty
- Fusion versus decompression alone: The central debate. Cyst recurrence is rare after decompression alone (1.8%) and never reported after fusion, and fusion reduces recurrent mechanical back pain (Bydon 2010, Xu 2010). However, no randomised trial exists; systematic reviews explicitly state there is insufficient evidence to define WHEN fusion should be added (Campbell 2016). Most surgeons reserve fusion for an established slip, dynamic instability, or recurrent cyst/back pain.
- Does removing the medial facet cause instability? Resection requires medial facetectomy. The threshold (often quoted as over 50% of the facet, or bilateral facet violation) at which iatrogenic instability mandates fusion is not precisely defined by high-level evidence.
- Role of percutaneous treatment: Clearly less durable than surgery, but the ideal candidate (small cyst, high surgical risk, patient preference) is not well characterised.
- MIS versus open: Tubular microscopic and endoscopic resection give comparable outcomes to open surgery with no microscopic-vs-endoscopic difference (Garg 2021), but comparative trials against open surgery are limited and largely retrospective.
- Calcified cysts: Dense calcification of the cyst wall predicts dense dural adhesion, higher durotomy risk, and incomplete resection — but evidence is observational.
Mnemonics
CYSTCyst Characteristics
Hook:Key imaging features.
SIPTreatment Hierarchy
Hook:Stepwise management.
FACETSynovial Features
Hook:Pathological features.
MCQ Practice Points
Q: What MRI finding distinguishes a synovial cyst from a ganglion cyst? A: Communication with the facet joint. (Though clinically managed similarly).
Q: Which spinal level accounts for over 75% of synovial cysts? A: L4/5. It is the level of maximal mobility/instability.
Q: Where are these cysts typically located relative to the thecal sac? A: Posterolateral. Compressing the traversing nerve root in the lateral recess.
Q: How durable is percutaneous aspiration/rupture? A: Poor — roughly 30-40% require a repeat procedure and about one-third ultimately proceed to surgery.
Q: What does the presence of a synovial cyst imply about the facet joint? A: Instability. It is a marker of hypermobility.
At a Glance
- Synovial Cyst
- Posterolateral (Dorsal to nerve)
- Disc Herniation
- Anterior (Ventral to nerve)
- Synovial Cyst
- Facet Joint
- Disc Herniation
- Intervertebral Disc
- Synovial Cyst
- Bright (Fluid) or Dark (Calcified)
- Disc Herniation
- Dark (Dessicated nucleus)
- Synovial Cyst
- Spondylolisthesis (Instability)
- Disc Herniation
- Degenerative Disc Disease
Exam Day Cheat Sheet
Key Facts
- L4/5 Most Common
- Marker of Instability
- Adherent to Dura
- High recurrence with aspiration
Imaging
- T2 Hyperintense (Fluid)
- T1 Hypointense
- Posterolateral location
- Facet OA
Treatment
- Conservative (rarely works)
- Injection (Temorizing)
- Decompression (Stable)
- Fusion (Unstable)
Risks
- Dural Tear (High)
- Recurrence (10%)
- Iatrogenic Instability
- Infection (Discitis)
Image Manifest
- [4-magnetic-resonance-imaging-revealed-a-15-cm-intras.png]: Intrasacral Cyst showing compression
- [5-sagittal-t2-weighted-mri-images-showing-sequential.png]: Axial T2 MRI showing lateral recess compression
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“65M, L4/5 Synovial Cyst causing L5 radiculopathy. Flexion/Extension X-rays show NO slip. What surgery do you offer?”
“During resection of an L4/5 cyst, you encounter a dural tear. The cyst wall was adherent. What is your management algorithm?”
“A 58F with an L4/5 synovial cyst and a 3-month history of L5 radiculopathy asks whether she can avoid surgery with an injection. There is no spondylolisthesis and she is neurologically intact. How do you counsel her?”
Evidence Base
To Fuse or Not — Systematic Review of Outcomes
- 82 studies, 966 patients with spinal synovial cysts.
- L4/5 was the dominant level (75.4%); radicular pain in 69.6%, back pain in 48.3%.
- Back and leg pain resolved in 92.5% and 91.1% after surgery.
- Same-level cyst recurrence 1.8% after decompression ALONE versus 0% after decompression plus fusion.
Recurrence After Resection — Laminectomy vs Instrumented Fusion
- 167 consecutive patients, 195 synovial cysts, single institution over 19 years.
- Back and radicular pain improved in 91.6% and 91.9% after surgery.
- Laminectomy alone carried significantly higher cyst recurrence and recurrent back pain than fusion (log-rank p=0.042 and p=0.018).
- Decompression with instrumented fusion had the lowest incidence of both cyst recurrence and recurrent back pain.
Percutaneous vs Surgical — Comparative Meta-Analysis
- 50 studies, 870 patients with lumbar facet joint cysts.
- Cyst resolution 90% for decompression (with or without fusion) versus 58% for percutaneous procedures.
- Repeat procedures required in 29% after percutaneous treatment versus under 1% after decompression.
- Insufficient data to define when fusion should be added.
Percutaneous Rupture — Prospective Cohort
- 35 patients, fluoroscopy-guided percutaneous cyst rupture, 1-year follow-up.
- Significant improvements in pain and Oswestry Disability Index; satisfaction near 70%.
- 40% (14/35) required repeat rupture.
- 31% (11/35) progressed to surgery.
Minimally Invasive Excision — Systematic Review
- 20 studies, 388 patients, tubular microscopic or endoscopic resection.
- Favourable Macnab outcome in 86%.
- Incidental durotomy 8%, cyst recurrence 4%, reoperation 5%.
- No significant difference between microscopic and endoscopic approaches.
Spontaneous Regression — Case Series
- Three patients with symptomatic lumbar synovial cysts that resolved without surgery.
- Spontaneous regression is documented but rare in the literature.
- Nonoperative management can be appropriate when neurological deficit is absent.
- Supports a trial of conservative care before intervention in selected patients.