Hexapod System | Stewart Platform | 6-Axis Correction
- Hexapod = Stewart platform: 6 telescopic struts connecting 2 rings = 6 DOF
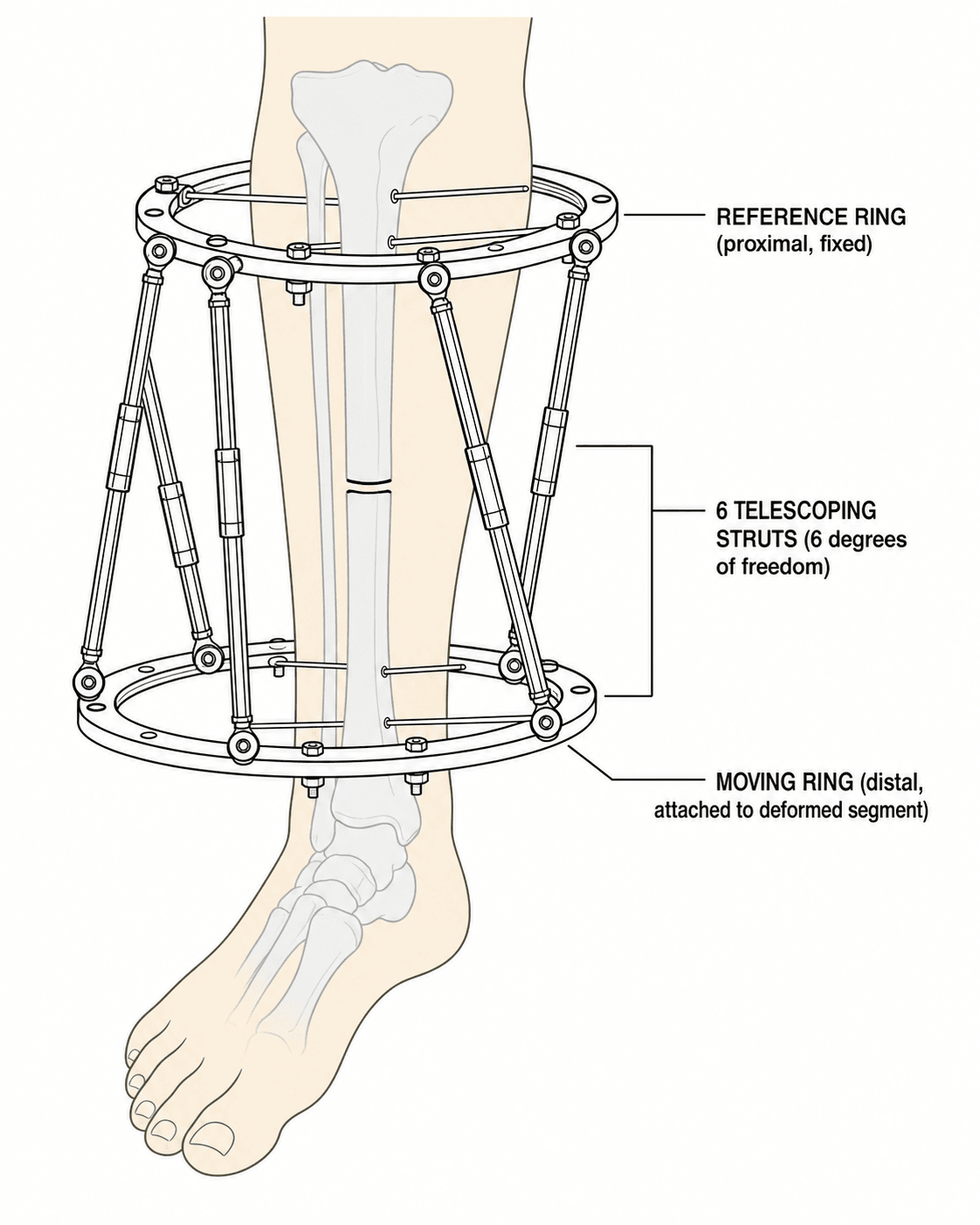
- Reference ring: Fixed ring (usually proximal) defines coordinate system
- Moving ring: Ring that moves relative to reference ring during correction
- Mounting parameters: 14 measurements (7 per ring) required for software
- Total residual: Combined measure of all deformity components - correction complete when approaches zero
- “Stewart platform originally designed for flight simulators (1965)
- “TSF can correct all 6 axes simultaneously - unlike Ilizarov
- “Virtual hinge at CORA minimizes unwanted translation during angular correction
- “Frame mounting errors cause residual deformity - precision critical
Stewart platform kinematic mechanism: 6 telescopic struts connect 2 rings with universal joints. This configuration provides 6 degrees of freedom (3 translations + 3 rotations), allowing simultaneous multiplanar correction. Unlike Ilizarov, no hinge placement or frame rebuilding required.
14 total parameters (7 per ring) must be measured accurately: ring diameter, ring-to-ring distance, frame offset (anterior, lateral), strut mounting positions (rotational orientation), and axial orientation. Errors in measurement cause residual deformity.
Reference ring = fixed ring (typically proximal) that defines the coordinate system. Moving ring = ring that moves during correction. Choice affects deformity prescription - be consistent. The reference ring is attached to the "stable" bone segment.
Total residual = composite measure of remaining deformity across all 6 axes. Calculated by software after inputting current deformity parameters. Correction progresses until total residual approaches zero. Used to monitor progress and endpoint.
- Taylor Spatial Frame (TSF)
- 6 telescopic struts (hexapod)
- Ilizarov Circular Fixator
- Rods, hinges, motors (modular)
- Taylor Spatial Frame (TSF)
- 6 DOF simultaneous correction
- Ilizarov Circular Fixator
- Sequential corrections required
- Taylor Spatial Frame (TSF)
- Computer software (web-based)
- Ilizarov Circular Fixator
- Mechanical/manual planning
- Taylor Spatial Frame (TSF)
- Virtual hinge (software)
- Ilizarov Circular Fixator
- Physical hinges required
- Taylor Spatial Frame (TSF)
- Not required during treatment
- Ilizarov Circular Fixator
- Often needed for direction changes
- Taylor Spatial Frame (TSF)
- Software-dependent (steep initially)
- Ilizarov Circular Fixator
- Traditional mechanics (steep)
- Taylor Spatial Frame (TSF)
- Higher (struts, software)
- Ilizarov Circular Fixator
- Lower (traditional components)
- Taylor Spatial Frame (TSF)
- Easy re-prescription via software
- Ilizarov Circular Fixator
- Frame reconfiguration needed
TAR-VAR6 Degrees of Freedom
Hook:TAR-VAR = 6 DOF: 3 Translations (AP, Axial, ML) + 3 Rotations (Varus/valgus, Axial rotation, Recurvatum)!
DR FLOSSMounting Parameters (7 per ring)
Hook:DR FLOSS your frame: Diameter, Ring distance, Frame offset (AP), Lateral offset, Orientation, Strut positions, Segment!
Overview and Principles
The Taylor Spatial Frame (TSF) is a hexapod external fixator based on the Stewart platform mechanism, originally developed by Dr. J. Charles Taylor in Memphis, Tennessee. It enables simultaneous six-axis deformity correction through computer-assisted planning and graduated strut adjustments.
Key Principles:
The TSF consists of two rings connected by six telescopic struts arranged in a specific geometric pattern. This hexapod configuration creates a Stewart-Gough platform - the same kinematic mechanism used in flight simulators, robotic surgery, and precision positioning systems.
- Three translational: Anterior-posterior, medial-lateral, axial (shortening/lengthening)
- Three rotational: Varus/valgus (coronal angulation), flexion/extension (sagittal angulation), axial rotation (torsion)
- Simultaneous multiplanar correction - no need for sequential corrections
- No physical hinges required - virtual hinge calculated by software
- No frame rebuilding - same construct throughout treatment
- Residual correction capability - easily re-prescribe if deformity persists
- Computer-assisted planning - reduces human calculation errors
The Stewart platform was described by D. Stewart in 1965 for use in flight simulation. It provides 6 degrees of freedom through 6 linear actuators connecting two platforms. Taylor applied this mechanism to orthopaedic external fixation in the 1990s, revolutionizing deformity correction.
Indications and Contraindications
Indications
- Complex multiplanar deformities (congenital, developmental, post-traumatic)
- Tibial and femoral malunion
- Metabolic bone disease deformities (rickets, Blount disease)
- Angular deformities with rotational and translational components
- Limb length discrepancy requiring distraction osteogenesis
- Combined lengthening with deformity correction
- Congenital short femur, fibular hemimelia
- Acute fracture reduction with gradual correction
- Malunion correction with osteotomy
- Nonunion with deformity
- Bone transport for segmental defects
- Infected nonunion management
- Combined with Masquelet technique
Contraindications
- Active sepsis (systemic)
- Severe soft tissue compromise precluding pin/wire placement
- Non-compliant patient (unable to perform daily adjustments)
- Inadequate bone stock for wire/pin fixation
- Severe peripheral vascular disease
- Uncontrolled diabetes mellitus
- Osteoporosis (may require modified technique)
- Morbid obesity (frame stability concerns)
- Psychological unsuitability
Technical Principles
The Hexapod Mechanism
Stewart Platform Kinematics:
The TSF utilizes inverse kinematics - given a desired end position/orientation, the software calculates the required strut lengths. This is the opposite of forward kinematics (calculating position from joint angles).
Key Components:
- Two rings: Reference ring and moving ring
- Six struts: Telescopic struts with universal joints at each end
- Universal joints: Allow multi-axis rotation at strut-ring connections
- Strut mechanism: Threaded telescoping design for length adjustment
Why 6 Struts?
Six struts provide exactly 6 degrees of freedom - the minimum required for full spatial positioning. This is mathematically analogous to 6 linear equations with 6 unknowns, creating a fully determined (not over- or under-constrained) system.
Reference and Moving Rings
- The "fixed" ring that defines the coordinate system
- Usually placed on the proximal (stable) segment
- All deformity parameters measured relative to this ring
- Convention: Typically the ring closest to the trunk
- The ring that moves during correction
- Attached to the distal (deformed) segment
- Moves to the corrected position as struts adjust
The choice of reference ring affects how deformity is prescribed to the software. If you select the proximal ring as reference, describe the deformity of the distal segment. Be consistent - errors in reference ring selection lead to correction in the wrong direction.
Virtual Hinge Concept
In traditional Ilizarov correction, physical hinges are placed at the Center of Rotation of Angulation (CORA) to achieve pure angular correction without translation.
The TSF creates a virtual hinge through software calculation:
- The software calculates strut adjustments that simulate rotation about a hinge at any specified point
- No physical hinge needed
- Virtual hinge placed at CORA minimizes secondary translation
- Can be adjusted/repositioned during treatment if needed
CORA (Center of Rotation of Angulation):
- The intersection of the proximal and distal mechanical axes
- Ideal pivot point for angular correction
- Correction about CORA produces pure angulation without translation
- Correction about a point away from CORA produces combined angulation and translation
Total Residual
Definition:
The total residual is a composite measure representing the magnitude of remaining deformity across all 6 axes after software calculation.
- Software combines angular deformities (degrees) and translational deformities (mm)
- Weighted combination into single value
- Approaches zero as correction completes
- Monitor correction progress
- Endpoint determination (typically less than 5mm equivalent)
- Identify incomplete corrections requiring adjustment
Frame Offset: the Dominant Source of Residual Deformity
The topic states that mounting-parameter errors cause residual deformity — the specific culprit is the frame (ring) offset, and it is worth knowing how to get it right.
- What the offset is. The frame/ring offset is the perpendicular distance from the bone (reference) axis to the centre of the reference ring in the AP and lateral planes; together with ring diameter and ring-to-ring distance it locates the ring in space relative to the bone, so the software knows where the frame is.
- Why it dominates the error budget. Offset is the hardest parameter to measure and the most error-prone, and a small offset error translates almost directly into residual deformity — roughly a millimetre of offset error per degree of residual angulation in typical constructs; the error grows with the distance between the origin and the reference ring.
- How to measure it accurately. Use calibrated radiographs (a calibration marker of known size) or a calibrated image intensifier, with the bone axis drawn on true AP and lateral films and the perpendicular distance to the ring centre measured — non-calibrated films are the least accurate.
- The CT alternative. Basing the correction on the actual 3D frame-to-bone position on CT compensates for mounting error more completely (sub-degree and sub-millimetre in phantoms) but is reserved for complex cases because of cost and radiation.
Q: Why is residual deformity after a hexapod correction usually a mounting-parameter problem, and which parameter? A: The frame (ring) offset - the perpendicular distance from the bone axis to the ring centre - is the hardest parameter to measure and the dominant error source, with roughly 1 mm of offset error per degree of residual angulation (error grows with origin-to-ring distance). Measure it on calibrated radiographs/image intensifier (or plan from 3D CT), not uncalibrated films.
MAD CORADeformity Parameters (CORA Analysis)
Hook:MAD CORA analysis: Mechanical axis, Angulation, Displacement + CORA, Orientation, Rotation, Axial length!
Surgical Technique
Preoperative Planning
- Long-leg standing radiographs (AP and lateral)
- CT scan for rotational deformity assessment
- EOS imaging if available (low radiation, full-length)
- Mechanical axis deviation (MAD)
- Identify CORA(s) - may be single or multiple
- Measure angular deformity (magnitude and direction)
- Assess translational deformity
- Evaluate rotational deformity (CT required)
- Measure limb length discrepancy
- Level of osteotomy (ideally at CORA)
- If CORA outside bone, plan for secondary correction
- Corticotomy technique for lengthening
Ring Selection and Sizing
- Allow 2-3 finger breadths clearance circumferentially
- Consider soft tissue swelling
- Larger rings allow better access but reduce stability
- Full rings vs 5/8 rings vs foot plates
- Proximal tibial: Consider knee ROM
- Distal tibial: Consider ankle clearance
- Femoral: May need half-rings for sitting
Frame Assembly
Steps:
- Assemble rings with appropriate connectors
- Attach 6 struts to designated mounting positions
- Ensure universal joints move freely
- Check strut length range adequate for planned correction
- Record strut positions on mounting worksheet
Wire and Pin Placement
- Minimum 2 fixation elements per ring (wires and/or pins)
- Tensioned wires (1.5-1.8mm) for ring stability
- Half-pins (5-6mm) for added stability
- Safe corridors to avoid neurovascular structures
- Proximal ring: Safe wire from fibular head to posteromedial tibia
- Reference wire perpendicular to tibial axis
- Avoid peroneal nerve
- Distal ring: Safe zone anterior to posterior
- Protect anterior tibial vessels
- Olive wires: 130-150 kg tension
- Smooth wires: 110-130 kg tension
- Re-tension after 48 hours (settling)
This section covers frame application technique.
Complications
Frame-Related Complications
- Most common complication (30-100% incidence)
- Superficial: Local care, oral antibiotics
- Deep: May require pin removal, IV antibiotics
- Prevention: Regular pin care, good technique
- Presents as pain, instability, increased discharge
- May require pin replacement
- More common with half-pins in poor bone
- Due to pin failure, ring breakage, strut malfunction
- Requires urgent assessment and revision
Correction-Related Complications
- Due to mounting parameter errors
- Incorrect deformity prescription
- Patient non-compliance with schedule
- Management: Re-measure, re-prescribe
- Deformity corrected beyond neutral
- May be intentional (planned over-correction for rebound)
- Unintentional: Revise prescription
- Stretch neuropathy with lengthening
- Vascular compromise (rare)
- Slow or stop distraction if symptoms develop
Bone-Related Complications
- Regenerate consolidates before target length
- Management: Speed up distraction, consider re-osteotomy
- At osteotomy site or regenerate
- Risk factors: Smoking, diabetes, poor technique
- Management: Bone graft, optimize biology
- After frame removal
- Protect with cast/brace until remodeling complete
Soft Tissue Complications
- Adjacent joints stiffen during prolonged treatment
- Prevention: Aggressive physiotherapy
- May require manipulation, release
- Gastrocnemius (equinus) in tibial lengthening
- Quadriceps in femoral lengthening
- Consider prophylactic releases for large lengthenings
The most significant functional complications are joint stiffness and contracture. Physiotherapy from day one is essential. Monitor ROM at every visit. Consider prophylactic soft tissue releases (gastrocnemius slide, quadricepsplasty) for lengthenings greater than 4-5cm.
The Origin and Corresponding Point: How a TSF Prescription Actually Works
The software section refers to an "origin" without defining it — the origin/corresponding-point framework is the conceptual core of how a hexapod deformity is prescribed.
- Origin and corresponding point. The surgeon chooses an origin — a defined reference point on the reference (fixed) fragment, conventionally at the osteotomy level on the reference-ring side — and a corresponding point, the matching point on the moving fragment that should end up superimposed on the origin once the deformity is corrected. The deformity is described as the translations and angulations needed to move the corresponding point onto the origin.
- Structure at rest vs deformity parameters. The software needs two things: the mounting parameters (where the frame sits — the "frame at rest") and the deformity parameters (AP and lateral angulation, AP/lateral/axial translation, and axial rotation of the corresponding point relative to the origin). From these it computes the six daily strut lengths.
- Choosing the origin sensibly. Placing the origin at the CORA makes the correction a pure angulation (a virtual hinge there), minimising secondary translation; an origin away from the CORA produces combined angulation and translation that the software still resolves but which must be intended.
- Why this makes residual correction easy. If a residual deformity remains, the surgeon simply re-defines the current corresponding-point offset (the residual program) and the software issues a fresh strut schedule — with no frame rebuild, unlike an Ilizarov.
Q: In TSF software, what are the origin and the corresponding point? A: The origin is a chosen reference point on the fixed (reference) fragment (usually at the osteotomy on the reference-ring side); the corresponding point is the matching point on the moving fragment. The deformity is prescribed as the translations/angulations that bring the corresponding point onto the origin. Put the origin at the CORA for a pure-angular (virtual-hinge) correction; any residual is fixed by re-entering the offset (residual program) with no frame rebuild.
Choosing the Correction Method (Decision Table)
When a multiplanar deformity is identified, the exam question is usually "which device/technique?" Use the clinical features below to justify your choice rather than reflexively reaching for a hexapod.
- Preferred strategy
- Acute osteotomy + plate/monolateral fixator
- Why
- Single plane corrects accurately in one stage; avoids prolonged frame
- Preferred strategy
- Hexapod (TSF) gradual six-axis correction
- Why
- Simultaneous correction of all axes; virtual hinge; software residual mode
- Preferred strategy
- Hexapod or Ilizarov with distraction osteogenesis
- Why
- Gradual distraction needed; hexapod adds 3D angular control
- Preferred strategy
- Osteotomy at CORA (acute or gradual)
- Why
- Pure angular correction without secondary translation
- Preferred strategy
- Ilizarov or hexapod bone transport +/- Masquelet
- Why
- Manages infection, dead space and length together
- Preferred strategy
- Hexapod gradual correction
- Why
- Avoids acute open surgery through poor envelope
- Preferred strategy
- Traditional Ilizarov
- Why
- No per-case software/strut cost; equivalent biology
- Preferred strategy
- Internal/acute correction (avoid gradual frame)
- Why
- Gradual correction fails without reliable strut adjustment
Guidelines, Registries & Global Practice
The TSF (Smith & Nephew) is one of several hexapod systems worldwide; equivalent platforms include the TrueLok-Hex (Orthofix), the Ortho-SUV frame, and the MAXFRAME (Zimmer Biomet). All share Stewart-platform kinematics and web/desktop planning software, so the principles below are device-agnostic.
Global epidemiology and case mix:
- Hexapod frames are concentrated in tertiary limb-reconstruction units because of the planning, monitoring and patient-compliance demands.
- Commonest indications globally: post-traumatic tibial malunion/nonunion, congenital and developmental deformity (Blount disease, rickets, fibular hemimelia, congenital short femur), and limb-length discrepancy.
- In high-burden, limited-resource regions, neglected fractures and infected nonunions (often post-bonesetter) form a disproportionate share of the workload.
Societies, training and standards (side-by-side):
- Role relevant to hexapod frames
- Limb reconstruction courses, deformity-analysis curriculum, outcome reporting standards
- Role relevant to hexapod frames
- Deformity-correction and external-fixation education; CORA / mechanical-axis planning
- Role relevant to hexapod frames
- Open-fracture and external-fixation pin-site care standards applicable to ring/hexapod frames
- Role relevant to hexapod frames
- External fixation and limb-reconstruction educational resources
- Role relevant to hexapod frames
- Fellowship-level deformity-correction training and consensus
There is no single high-level guideline mandating hexapod over Ilizarov; selection is guided by deformity complexity, surgeon experience, software access and cost.
No dedicated hexapod-frame registry equivalent to arthroplasty registries (NJR, AJRR, AOANJRR) exists. Evidence is dominated by single-centre series and systematic reviews; this is a recognised limitation when quoting union and complication rates.
- High-resource: hexapod frame with software planning, CT-based deformity analysis, calibrated imaging for mounting parameters, dedicated physiotherapy and pin-site clinics.
- Limited-resource: traditional Ilizarov constructs remain first-line because of lower cost and no per-case software/strut expense; hexapods reserved for the most complex multiplanar cases.
- Across all settings, success depends on daily strut adjustment compliance and pin-site care over a typical 3-6 month treatment; multidisciplinary input (surgeon, physiotherapist, orthotist) is essential.
Controversies & Areas of Uncertainty
- Hexapod vs Ilizarov accuracy: Hexapods give superior 3D control and easier residual re-prescription, but comparative data are largely level III-IV single-centre series. Systematic review evidence suggests a potentially higher healing index with hexapods, and no high-level trial proves a union-rate advantage.
- Radiograph- vs CT-based mounting parameters: Frame-offset measurement is the dominant error source. Calibrated radiographs perform well, but CT/3D planning compensates for mounting error more completely. Routine CT planning is not universally adopted because of cost and radiation.
- Acute vs gradual correction: Gradual six-axis correction is more accurate for complex deformity, yet for simple uniplanar deformity acute one-stage correction avoids months in a frame; the threshold (often cited around 10 degrees of uniplanar varus) is convention, not high-level evidence.
- Latency, rate and rhythm of distraction: The classic 5-7 day latency and 1 mm/day in four divided increments derive from distraction-osteogenesis biology, but optimal rate varies with age, site and regenerate quality and is individualised, not protocolised.
- Pin-site care: Reported pin-site infection rates range widely (commonly 30 percent or more, mostly superficial). No single cleaning regimen is proven superior, which is why incidence figures must be quoted with caution.
- Registry gap: Absence of a dedicated hexapod registry means complication and survival figures rest on heterogeneous series, limiting generalisability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Explain the Taylor Spatial Frame to me. How does it work and what advantages does it offer over traditional Ilizarov frames?”
“A 25-year-old man presents with a tibial malunion following conservative treatment of a fracture 2 years ago. Radiographs show 20 degrees varus angulation, 15 degrees procurvatum, and 2cm shortening. How would you plan correction using a TSF?”
“You applied a TSF for correction of a tibial deformity. At the end of the planned correction schedule, radiographs show a 10-degree residual varus deformity. What went wrong and how would you manage this?”
Hexapod Principles
- Stewart platform: 6 struts, 2 rings, 6 DOF
- 3 translational: AP, ML, axial
- 3 rotational: varus/valgus, flexion/extension, rotation
- Virtual hinge at CORA (no physical hinge)
Mounting Parameters (14 total)
- 7 per ring: diameter, ring distance, AP offset, lateral offset
- Master tab position, strut positions, segment/side
- Errors cause residual deformity
- Standardized measurement protocol essential
Reference vs Moving Ring
- Reference ring: stable segment (usually proximal)
- Moving ring: deformed segment (moves during correction)
- Defines coordinate system for software
- Be consistent with ring selection
Software Planning
- Input 14 mounting parameters
- Prescribe deformity in all 6 axes
- Software calculates daily strut changes
- Residual mode for mid-treatment adjustment
TSF vs Ilizarov Advantages
- Simultaneous multiplanar correction
- No hinge placement or frame rebuilding
- Computer-assisted (reduces errors)
- Easy residual correction via software
Distraction Protocol
- Latency: 5-7 days before starting
- Rate: 1mm/day in 4 divided doses
- Angular correction: 1-2 degrees/day
- Total residual approaches zero when complete
Evidence Base
Gradual (six-axis) versus acute correction of tibia vara
- Retrospective comparative study: 18 tibiae gradual TSF correction vs 14 tibiae acute correction
- Accurate angulation correction in 17/18 gradual vs 7/14 acute limbs
- Accurate translation (within 5 mm) in 18/18 gradual vs 7/14 acute
- Residual mechanical axis deviation 3.1 mm (gradual) vs 17.1 mm (acute)
Accuracy of radiographic measurement of TSF mounting parameters
- Sawbone tibia study comparing 150 radiographic mounting-parameter measurements to direct caliper reference
- Non-calibrated radiographs (method A) showed the highest variance vs reference
- Error increased with greater origin-to-reference-ring distance
- Calibrated radiographs and calibrated image-intensifier images were accurate and intercomparable (p=0.226)
Femoral deformity correction with the TSF in children and young adults
- 20 patients (22 limbs), age 5.9-24.6 years; mean time in frame 6.2 months
- Frontal and sagittal plane deformities corrected to within normal values
- Mean lengthening 4.9 cm (range 1.5-9 cm); external fixation index 2.2 months/cm
- 15 complications in 13 limbs (pin-tract infection, knee stiffness, delayed union, posterior knee subluxation)
Supramalleolar osteotomy with six-axis correction for distal tibial deformity
- 52 adults (mean age 44 years); 22 had oblique-plane deformities; mean time in frame 4 months
- All postoperative distal tibial joint-orientation angles within 0-4 degrees of normal
- Mean AOFAS improved from 40 to 71 (p less than 0.001)
- Complications: two osteotomy nonunions; three later required ankle fusion
Computer-assisted distraction osteogenesis: 3D-CT vs radiographic frame mounting
- Method computes correction from the actual frame-to-bone position on 3D CT, immediately compensating for mounting errors
- 20 tibial phantom experiments: mean residual error less than 2 degrees rotation and less than 0.5 mm length
- Pilot clinical study of 5 patients showed clinically acceptable corrections with no complications
- Supports CT-based planning as more accurate than radiograph-derived mounting parameters
Hexapod fixation for lengthening in disproportionate short stature (systematic review)
- 20-year systematic review (2004-2024) of hexapod limb lengthening in short stature
- Mean lengthening 3-5.9 cm; healing index 37-68.6 days/cm
- Most frequent complications: pin-site infection, compartment syndrome, delayed union
- TSF allowed more accurate corrections but often a higher healing index than other external fixators