Bennett's vs Rolando | CMC Joint Involvement | Deforming Forces | Articular Reduction
- Bennett's: 2-part intra-articular fracture-subluxation with small volar-ulnar fragment held by the deep anterior oblique (beak) ligament
- Deforming forces: APL pulls shaft proximally and radially, adductor pollicis pulls the head into adduction, so the shaft subluxates dorsally and supinates
- Rolando: 3-or-more-part comminuted intra-articular (Y or T pattern) - worse prognosis than Bennett's
- Robert's view (hyperpronated thumb AP) is the key view to assess volar fragment size and step-off
- Threshold for surgery: greater than 1-2mm articular step-off or CMC subluxation that cannot be maintained
- “Know the Green/O'Brien classification: Type I (Bennett's), Type II (Rolando), Type IIIA (transverse extra-articular), Type IIIB (oblique extra-articular)
- “Bennett's reduction manoeuvre: Traction + Extension + Pronation + Abduction (TEPA) - reverse the deformity
- “Rolando 'bag of bones' comminution favours distraction external fixation (ligamentotaxis) over ORIF
- “Radiographic CMC OA does NOT always correlate with symptoms (Cannon 1986, Livesley 1990)
Thumb Base Fractures
You must know the deforming forces in a Bennett's fracture. The small volar-ulnar fragment stays in place (anchor). The main metacarpal shaft fragment is pulled proximally, dorsally, and radially. Know which tendon pulls where: APL pulls the shaft proximally and radially; adductor pollicis pulls the head into adduction (supination). The deep anterior oblique (beak) ligament holds the volar fragment.
Overview
Thumb Base Fracture Overview
Definition:
- Fractures involving the base of the first metacarpal
- May be extra-articular or intra-articular (1st CMC joint)
- Bennett's and Rolando patterns are the intra-articular subtypes
- Description
- 2-part fracture-dislocation with volar-ulnar fragment
- Articular Involvement
- Intra-articular
- Description
- Comminuted Y or T pattern (3+ fragments)
- Articular Involvement
- Intra-articular
- Description
- Extra-articular transverse or oblique fracture
- Articular Involvement
- Extra-articular
Anatomy
CMC Joint Anatomy
- Biconcave saddle joint with 2 degrees of freedom
- Allows flexion/extension, abduction/adduction, and circumduction (with screw-home rotation)
- Critical for opposition and pinch function
- Deep anterior oblique ligament (dAOL / beak ligament) - intra-articular pivot, attaches to volar-ulnar beak
- Superficial anterior oblique ligament (sAOL)
- Dorsoradial ligament (DRL) - increasingly recognised as a key dorsal restraint
- Posterior oblique ligament
- Intermetacarpal ligament (1st to 2nd MC)
- Location
- Volar-ulnar beak of MC base to trapezium
- Function
- Pivot for pronation, restrains subluxation
- Location
- Dorsal trapezium to MC base
- Function
- Major restraint to dorsal subluxation
- Location
- 1st to 2nd MC base
- Function
- Limits radial deviation / tension band
Deforming Forces in Bennett's (summary):
- Volar-ulnar (beak) fragment stays reduced, anchored by the deep anterior oblique ligament
- APL pulls the shaft proximally and radially
- Adductor pollicis pulls the head into adduction, pivoting the base dorsally and into supination
- Net result: dorsoradial subluxation of the 1st CMC joint
Classification
Green & O'Brien Classification (first metacarpal base)
- Pattern
- Bennett's - 2-part intra-articular fracture-subluxation
- Stability
- Unstable
- Pattern
- Rolando - comminuted intra-articular (Y / T)
- Stability
- Unstable
- Pattern
- Extra-articular transverse
- Stability
- Usually stable
- Pattern
- Extra-articular oblique
- Stability
- Can be unstable
- Pattern
- Paediatric epiphyseal (Salter-Harris) base injury
- Stability
- Variable
Key points:
- Types I and II are intra-articular and threaten the CMC joint surface
- Type III (extra-articular) tolerates more angulation because remodelling and CMC mobility compensate
Paediatric Thumb Metacarpal Base Fractures (Type IV)
The Green & O'Brien classification lists a Type IV paediatric epiphyseal (physeal) base injury, but it behaves differently enough to deserve its own answer in a viva. The key anatomical fact is that, unlike the finger metacarpals, the thumb metacarpal has its physis at the PROXIMAL end (the base) - exactly where these fractures occur. So a "thumb base fracture" in a child is usually a physeal injury, and it must be described in Salter-Harris terms.
- Most common patterns are extra-articular - a metaphyseal base fracture or a Salter-Harris II (a metaphyseal Thurston-Holland fragment with the physis). These are usually managed by closed reduction and a thumb spica cast, and they remodel well because the physis is adjacent to the deformity and the mobile CMC joint compensates. Considerably more angulation is accepted than in an adult because of this remodelling potential.
- Salter-Harris III / IV fractures cross the physis into the CMC joint - the true intra-articular "paediatric Bennett equivalent." Because they are both intra-articular and physeal, displacement threatens the joint surface AND the growth plate; if displaced they need anatomic reduction and stabilisation (usually CRPP), with smooth wires avoiding repeated physeal crossing.
- The principle mirrors adults: extra-articular tolerates angulation; intra-articular demands congruity - but in a child you add the extra goal of protecting the physis from growth arrest (a malreduced SH-III/IV can form a physeal bar and cause angular deformity or shortening).
Why the thumb is different from the fingers:
- Thumb (and, by convention, first) metacarpal physis is proximal; the finger metacarpal physes are distal. A "base" injury in a child's thumb is therefore a physeal injury by default.
- Describe it in Salter-Harris terms first, then say intra- vs extra-articular - this drives management exactly as it does in adults.
- Remodelling is greatest for extra-articular metaphyseal / SH-II patterns near the proximal physis; do NOT rely on it for intra-articular (SH-III/IV) displacement - that must be reduced anatomically.
- Beware the growth-arrest risk of a malreduced SH-III/IV: warn the family and follow radiographs for a physeal bar / progressive deformity.
Clinical Assessment
History and Examination
- Axial load on a flexed thumb (punch, fall onto thumb)
- Direct blow to the thumb base
- High-energy (motor vehicle) or low-energy (sport, fall)
- Hand dominance and occupation
- Time since injury
- Previous thumb injuries
- Smoking status (affects healing)
- Swelling and tenderness at thumb base / thenar eminence
- Deformity - shortened, adducted thumb
- Assess neurovascular status (radial sensory nerve)
- Check IP and MCP joint motion
- Look for associated injuries (scaphoid, distal radius)
- Key Findings
- CMC swelling, tenderness, instability
- Deformity
- Adducted, shortened thumb
- Key Findings
- More swelling, crepitus
- Deformity
- Similar but more severe
- Key Findings
- Shaft tenderness, apex dorsal
- Deformity
- Less CMC involvement
Investigations


Imaging Assessment
- AP of thumb (Robert's view - true AP with hyperpronation)
- Lateral of thumb
- PA and lateral of hand
- Assess articular involvement, displacement, comminution
- Hand maximally pronated (thumb facing down onto the plate)
- Gives a true AP of the 1st CMC joint
- Best view to assess the Bennett's volar fragment and step-off
- When to Use
- All cases
- Key Information
- Fracture pattern, displacement
- When to Use
- Suspected intra-articular
- Key Information
- Volar fragment size, step-off
- When to Use
- Rolando / comminuted patterns
- Key Information
- Fragment size, surgical planning
The Bett's View: Seeing the Dorsal Subluxation
The topic rightly makes the Robert's view (true AP with the forearm hyperpronated, thumb dorsum on the plate) the key film for the volar-ulnar fragment and articular step-off. But the Robert's view is an AP, and the defining instability of a Bennett's fracture is dorsoradial - the dorsal component is exactly what an AP projection cannot show. The named companion film is the Bett's view (a dedicated true lateral of the first CMC joint), obtained with the hand pronated roughly 20-30 degrees from the fully pronated position with the beam angled, so the joint is profiled in the sagittal plane.
- Robert's (AP) answers "how big is the volar fragment and how much articular step-off?" The Bett's (lateral) answers "how much dorsal subluxation is there?" - you need both to characterise a Bennett's fracture, and a subluxation can be under-called on the AP alone.
- Always compare with the contralateral (uninjured) thumb, and read the post-reduction lateral to confirm the shaft has been brought back down onto the anchored volar fragment (dorsal translation eliminated), not just aligned on the AP.
- A true lateral is also the view that unmasks residual subluxation after casting or pinning - loss of reduction in a "healing" Bennett's is most often a recurrence of dorsal shift seen on the lateral while the AP still looks acceptable.
Why two dedicated views, not one:
- Robert's view = true AP (forearm hyperpronated) - volar-ulnar fragment size, articular step-off, radial subluxation.
- Bett's view = true lateral of the 1st CMC (hand partially pronated, beam angled) - dorsal subluxation, which the AP cannot display.
- The instability vector in Bennett's is dorsoradial: an AP shows the radial half, the lateral shows the dorsal half. Assess reduction and follow-up on both, and compare with the normal side.
- If either view or plain films are equivocal about the joint surface, CT resolves fragment size and step-off for the ORIF-versus-CRPP-versus-ex-fix decision.
Differential Diagnosis
A swollen, painful thumb base after trauma is not always a Bennett's fracture. The differentials below are the ones examiners expect you to actively exclude.
- Distinguishing Feature
- 2-part intra-articular base #, dorsoradial subluxation
- Key Test / Clue
- Robert's view shows volar-ulnar fragment
- Distinguishing Feature
- Comminuted Y/T intra-articular base #
- Key Test / Clue
- CT shows 3+ fragments
- Distinguishing Feature
- Joint surface intact, apex-dorsal angulation
- Key Test / Clue
- Congruent CMC on Robert's view
- Distinguishing Feature
- Pure ligamentous dislocation, no bony fragment
- Key Test / Clue
- Reduces but re-subluxes; beak ligament tear
- Distinguishing Feature
- Pain at MCP not CMC; valgus laxity
- Key Test / Clue
- Stress MCP in extension and 30 deg flexion
- Distinguishing Feature
- Anatomical snuffbox tenderness
- Key Test / Clue
- Scaphoid views; MRI if occult
- Distinguishing Feature
- Older patient, insidious pain, grind test positive
- Key Test / Clue
- X-ray osteophytes; no acute trauma
Management
Surgical Technique
CRPP Technique (Bennett's)
- Supine, arm on a hand table
- Regional or general anaesthesia
- Image intensifier (mini C-arm preferred)
- Tourniquet optional
- Longitudinal traction on the thumb
- Extend the MCP joint
- Pronate the thumb
- Abduct the thumb (radial pressure on the base)
- Direct dorsal pressure on the MC base
- 1.4-1.6mm K-wires (usually 2 wires)
- 1st MC to trapezium (trans-articular) OR 1st MC to 2nd MC base
- Confirm reduction on fluoroscopy (AP, lateral, Robert's)
- Protect wire ends, bend and cut short (or bury)
- Thumb spica splint / cast
- CRPP
- Adequate closed reduction
- ORIF
- Irreducible or inadequate
- CRPP
- Any size (pins bypass fragment)
- ORIF
- Large enough for a screw
- CRPP
- Maintained with pins
- ORIF
- Needs absolute stability
Complications
Potential Complications
- Pin site infection (superficial or deep)
- Radial sensory nerve injury (numbness, neuroma)
- Loss of reduction / fixation failure
- Wound complications
- Post-traumatic CMC arthritis (most significant)
- Malunion with dorsal prominence and varus base angulation
- Stiffness (CMC, MCP)
- Chronic instability
- Complex regional pain syndrome (rare)
- Risk Factor
- Articular step-off greater than 2mm
- Prevention/Treatment
- Anatomic reduction
- Risk Factor
- Pin placement, surgical incision
- Prevention/Treatment
- Careful technique, protect nerve
- Risk Factor
- Inadequate reduction
- Prevention/Treatment
- Intraoperative fluoroscopy check
- Risk Factor
- Prolonged immobilisation
- Prevention/Treatment
- Early ROM after 4-6 weeks
Postoperative Care
Rehabilitation Protocol
- Thumb spica cast or splint
- Elevate the hand to reduce swelling
- Active finger ROM to prevent stiffness
- Check X-ray at 2 and 6 weeks
- Office procedure under local anaesthesia
- After radiographic evidence of healing
- Transition to a removable splint
- Wean from the splint over 2-4 weeks
- Active and passive ROM exercises
- Hand therapy referral
- Avoid heavy loading initially
- Activity
- Thumb spica cast, finger ROM
- Goal
- Fracture healing
- Activity
- K-wire removal, X-ray check
- Goal
- Union confirmed
- Activity
- Active ROM, hand therapy
- Goal
- Restore motion
- Activity
- Progressive strengthening
- Goal
- Return to function
Outcomes
Functional Outcomes
- Good to excellent results in roughly 85-90% with adequate reduction
- Residual step-off correlates with radiographic OA (Kjaer-Petersen 1990)
- Radiographic OA does not always correlate with symptoms (Cannon 1986)
- Conservative management of displaced patterns gives poor long-term joints (Livesley 1990)
- Worse outcomes than Bennett's
- Higher rate of post-traumatic arthritis
- Comminuted patterns have the poorest prognosis, though modern ligamentotaxis series report grip/pinch around 90% of the contralateral side (Houshian 2013, Marsland 2012)
- Generally excellent outcomes
- Tolerates 20-30 degrees malunion without a functional deficit
- Good/Excellent Outcome
- Greater than 95%
- OA Rate
- Less than 5%
- Good/Excellent Outcome
- 85-90%
- OA Rate
- 10-20% (often asymptomatic)
- Good/Excellent Outcome
- 60-75%
- OA Rate
- 30-50%
Guidelines, Registries & Global Practice
Global Epidemiology
- Thumb metacarpal base fractures account for roughly a quarter of all metacarpal fractures and around 1-2% of all fractures.
- Bennett's is the most common intra-articular thumb base fracture; Rolando is considerably less common.
- Typical demographic: young to middle-aged men, dominant hand, from axial loading of a flexed thumb (punch, fall, sport).
Side-by-Side Guideline / Reference Comparison
- Emphasis
- Pattern-based decision making
- Practical Recommendation
- Anatomic articular reduction; CRPP for Bennett's, ex-fix or ORIF for Rolando
- Emphasis
- Hand trauma pathways, timely hand-surgery review
- Practical Recommendation
- Reduce and stabilise unstable intra-articular base fractures; restore congruity
- Emphasis
- Restore articular surface and CMC stability
- Practical Recommendation
- Surgery for step-off greater than 1-2mm or maintained subluxation
- Emphasis
- Function over radiographic perfection
- Practical Recommendation
- Aim for congruity but counsel that radiographic OA may be asymptomatic
Registry note: Unlike arthroplasty, isolated thumb base fractures are not tracked by national joint registries (NJR, AJRR, AOANJRR, SHAR). Evidence therefore rests on case series and small comparative studies rather than registry data - reflected in the predominantly Level IV evidence base.
Controversies & Areas of Uncertainty
- Does anatomic reduction prevent symptomatic arthritis? Kjaer-Petersen (1990) found residual displacement correlated with radiographic arthritis, yet Cannon (1986) found no reliable correlation between reduction accuracy and symptoms at a mean of 9.6 years. Cartilage injury at the moment of impact may matter as much as the residual step-off.
- CRPP vs ORIF for Bennett's. There is no randomised evidence. Most surgeons reserve ORIF for large, irreducible fragments and use CRPP first-line; the quality of articular reduction matters more than the implant chosen.
- Acceptable articular step-off. The widely quoted "1-2mm" threshold is derived from small retrospective series, not high-level evidence; some authors accept up to 1mm only, others tolerate 2mm.
- Trans-articular vs extra-articular pinning. Pinning the 1st MC to the trapezium crosses the joint; pinning to the 2nd MC base spares it. Both are used; no clear superiority.
- Rolando: ex-fix vs ORIF. Distraction external fixation (ligamentotaxis) gives reproducibly good function for comminuted patterns (Houshian 2013, Marsland 2012), challenging the older default of attempting plate ORIF on small fragments.
- Beak ligament dogma. Anatomic work (Bettinger 1999; Ladd/Hagert group) shows the dorsoradial ligament is also a major restraint, so the classic teaching that the AOL is the sole stabiliser is an oversimplification.
MCQ Practice Points
Q: What is a Bennett fracture and what deforming forces cause subluxation?
A: A Bennett fracture is an intra-articular fracture-subluxation at the thumb CMC joint with a volar-ulnar fragment held reduced by the deep anterior oblique (beak) ligament while the metacarpal shaft displaces radially, proximally, and supinates. Deforming forces: abductor pollicis longus (APL) pulls the metacarpal base proximally and radially; adductor pollicis adducts the thumb; the thumb extensors hyperextend the MCP. The beak ligament keeps the volar fragment reduced while the shaft subluxates away from it.
Q: What is the difference between a Bennett fracture and a Rolando fracture?
A: Bennett fracture: two-part intra-articular fracture-subluxation with a single volar-ulnar fragment. Rolando fracture: comminuted intra-articular fracture with a T or Y pattern (minimum three fragments - volar, dorsal, and metacarpal shaft). The Rolando pattern is less common but has a worse prognosis due to comminution and articular damage. Treatment: Bennett's - closed reduction and K-wire fixation, or a single lag screw if the fragment is adequate; Rolando's - plate fixation for large fragments, or distraction external fixation with ligamentotaxis for severe comminution.
Q: What are the indications for surgical fixation of thumb metacarpal base fractures?
A: Surgical indications: 1) articular step-off greater than 1-2mm after closed reduction; 2) CMC subluxation that cannot be maintained; 3) any displaced Bennett fracture (inherently unstable); 4) Rolando fracture with reducible fragments; 5) unstable extra-articular fractures. The goals are anatomic articular reduction and a stable CMC joint. Options include closed reduction and percutaneous K-wires, ORIF with a lag screw (Bennett's with an adequate fragment), or plate / external fixation (Rolando or comminuted patterns).
Q: How do you differentiate an extra-articular thumb metacarpal base fracture from a Bennett fracture clinically and radiographically?
A: An extra-articular fracture (Winterstein): the fracture line does not involve the CMC joint surface, the joint remains congruent, and deformity is apex-dorsal angulation at the fracture site. A Bennett fracture: the fracture line enters the CMC joint, an intra-articular fragment is visible on the Robert's view (true AP of the thumb with the hand hyperpronated), and the CMC joint shows subluxation with widening. Extra-articular fractures tolerate more angulation (20-30 degrees) than intra-articular fractures because CMC mobility compensates.
Q: What is the significance of the anterior oblique ligament (AOL) in Bennett fractures?
A: The deep anterior oblique (beak) ligament runs from the volar-ulnar beak of the metacarpal base to the trapezium and is a key stabiliser of the thumb CMC joint. In a Bennett fracture the volar-ulnar fragment remains attached to the beak ligament, keeping it reduced to the trapezium while the metacarpal shaft subluxates - producing the classic fracture-subluxation. Surgical reduction must bring the shaft back to the volar fragment (and thus to the trapezium). Anatomic studies (Bettinger 1999) show the dorsoradial ligament is also a substantial restraint, so the beak ligament is not the only stabiliser.
At a Glance
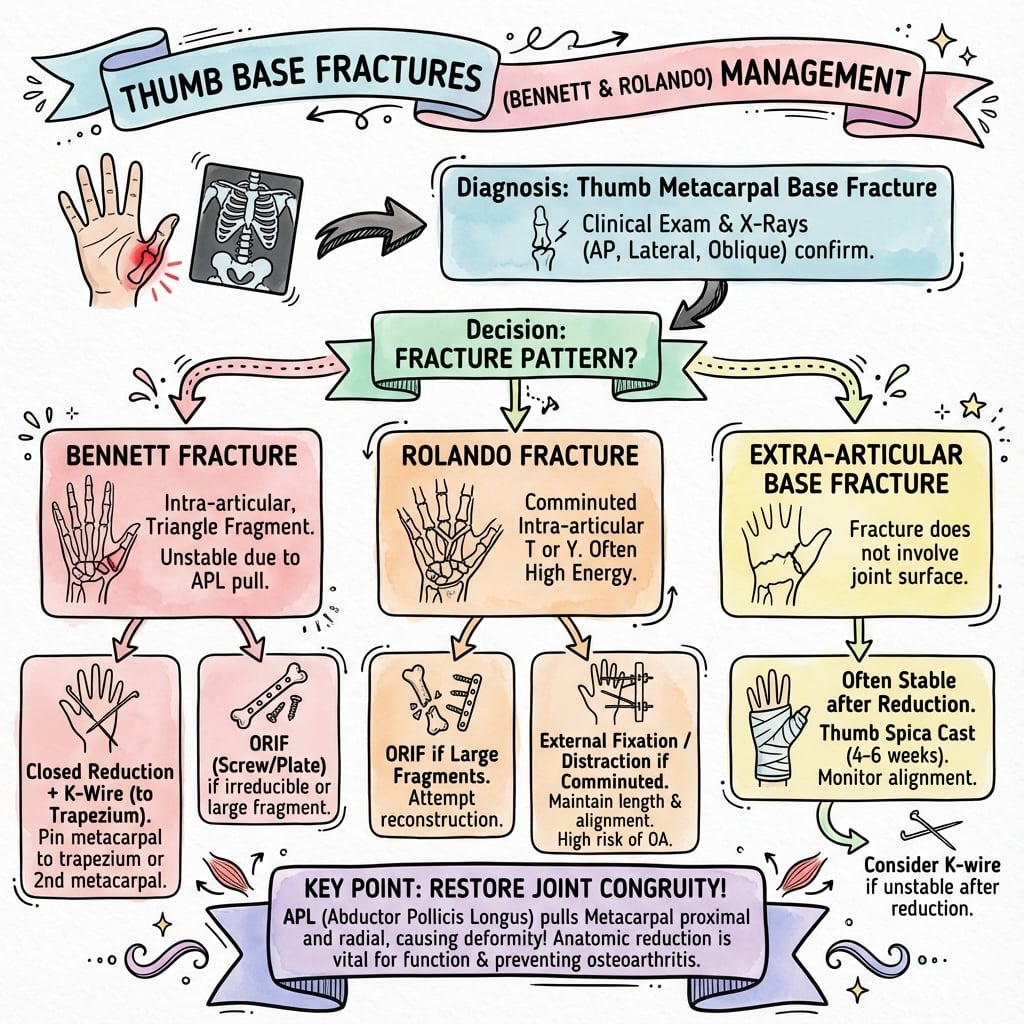
Thumb base fractures include Bennett's (2-part intra-articular), Rolando (3-part or comminuted intra-articular), and extra-articular patterns. Bennett's fracture is characterised by a small volar-ulnar fragment held by the deep anterior oblique (beak) ligament while the shaft displaces proximally, dorsally, and radially under APL and adductor pollicis pull. Treatment aims to restore articular congruity (under 1-2mm step-off) to limit CMC arthritis: CRPP is standard for Bennett's (traction + extension + pronation + abduction reduction), while Rolando fractures require ORIF for large fragments or distraction external fixation for comminuted "bag of bones" injuries. Extra-articular fractures are generally stable and managed with casting.
PADBennett's Deforming Forces
Hook:The shaft moves on a PAD - away from the anchored volar fragment
TEPABennett's Reduction Manoeuvre
Hook:TEPA reverses the deformity - Think 'TEPA the thumb back into place'
BREThumb Base Fracture Types
Hook:BRE - like 'break' - the 3 ways to break the thumb base
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old boxer presents with pain at the base of his right thumb. X-ray shows a 2-part intra-articular fracture with a small volar-ulnar fragment. The shaft is subluxed dorsally. How do you manage this?”
“A 35-year-old carpenter presents with a thumb base injury. X-rays show a comminuted intra-articular fracture of the first metacarpal base with a Y-shaped pattern - there are volar, dorsal, and shaft fragments visible. CT confirms three main fragments with the volar and dorsal pieces each approximately 5mm in size. He is concerned about returning to carpentry work which requires strong pinch grip. What are your treatment options and what would you recommend?”
“A 42-year-old presents with chronic thumb base pain 5 years after a Bennett's fracture that was treated with closed reduction and casting. He was told at the time surgery was not needed. X-rays show a well-healed fracture with 3mm articular step-off at the CMC joint and moderate osteoarthritis with joint space narrowing and osteophytes. He has pain with pinch and gripping affecting his work as a mechanic. What would you discuss regarding management?”
Classification
- Bennett's: 2-part intra-articular (oblique)
- Rolando: 3-part or comminuted intra-articular (Y/T)
- Extra-articular: transverse/oblique shaft (Winterstein)
Deforming Forces (Bennett's)
- Shaft: proximally/radially (APL), into adduction (adductor pollicis)
- Volar fragment: stays reduced (deep anterior oblique / beak ligament)
Treatment Thresholds
- Articular step-off over 1-2mm: surgery
- Bennett's: almost always CRPP or ORIF
- Rolando: distraction ex-fix if comminuted, ORIF if large fragments
Evidence Base
The evidence base for thumb base fractures is predominantly Level IV (case series and retrospective reviews); there are no randomised trials comparing CRPP with ORIF. The cards below summarise the landmark anatomical, long-term outcome, and reconstructive studies.
Original Description of Bennett's Fracture
- First description of a 'fracture of the metacarpal bone of the thumb'
- Described the oblique fracture line entering the CMC joint
- Recognised the characteristic subluxation of the shaft
- Distinguished it from extra-articular base fractures
Anatomy of the Trapeziometacarpal Stabilising Ligaments
- Cadaveric study identifying 16 ligaments stabilising the trapezium and TMC joint
- The deep anterior oblique (beak) ligament acts as a pivot for the metacarpal during palmar abduction and pronation
- The dorsoradial and deep anterior oblique ligaments play a substantial role in TMC stability
- Trapezio-2nd/3rd metacarpal ligaments act as tension bands resisting cantilever bending
Quality of Reduction and Outcome in Bennett's Fracture
- 41 Bennett's fractures treated by closed reduction, percutaneous K-wire, or open reduction
- Median 7.3-year follow-up of reviewed patients
- 15 of 18 with excellent reduction were symptom-free vs only 6 of 13 with residual displacement
- Radiographic arthritis in 3 of 14 anatomically reduced vs 7 of 10 with residual displacement
Long-term Outcome of Conservatively Treated Bennett's
- 25 Bennett's fractures reviewed at mean 9.6 years (5-16 years); 22 treated conservatively
- Only 2 patients had significant symptoms despite frequent loss of TMC motion
- Symptoms could NOT be reliably correlated with the accuracy of reduction
- Little evidence that imperfect reduction led to symptomatic arthritis long-term
26-year Follow-up of Conservatively Managed Bennett's
- 17 conservatively treated Bennett's fracture-dislocations reviewed at a mean of 26 years
- All had decreased range of movement and grip strength; 12 had a characteristic deformity
- Radiographs showed persistent CMC subluxation and marked degenerative change
- Authors recommend that this injury should NOT be managed conservatively
Distraction External Fixation for Rolando Fractures
- 16 comminuted Rolando fractures treated by capsuloligamentotaxis with a Pennig mini external fixator
- Supplementary K-wires used to maintain reduction; mean follow-up 20 months
- Excellent union in all cases; all but 2 patients pain-free at final review
- Mean grip 96% and pinch 93% of the unaffected thumb
Spanning External Fixation for the Rolando Fracture
- 8 Rolando fractures treated with a static two-pin trapeziometacarpal-spanning external fixator (ligamentotaxis)
- Mean time to frame removal 28 days
- Mean QuickDASH 7.95 at mean 2.7-year follow-up; all returned to previous activity
- Three superficial pin-site infections, no significant joint incongruity or malunion at 4 months