Ti-6Al-4V and Osseointegration
- Definition: Titanium (Ti) and its alloys (most commonly Ti-6Al-4V) are biocompatible metals used for uncemented implants and fracture fixation
- Definition: They are known for excellent osseointegration and low modulus of elasticity
- Mechanism: Titanium (Base), Aluminium (Stabilises Alpha phase - Strength), Vanadium (Stabilises Beta phase - Ductility)
- Management: Surface treatments (Plasma spray, Acid etching, Grit blasting) enhance osseointegration
- “Young's Modulus: ~110 GPa (Closer to cortical bone at 20 GPa than SS/CoCr)
- “MRI Compatible (Low artifact)
- “Excellent biocompatibility (inert)
- “Poor wear resistance (Notch sensitivity - not a bearing surface)
Titanium Alloys
Titanium is the Most Biocompatible metal because osseointegration occurs directly onto the $TiO_2$ layer. However, it is soft and susceptible to Notch Sensitivity and Abrasive Wear (black debris). NEVER use a Titanium femoral head articulating with Polyethylene (creates massive wear/black synovitis). Ti is for anchoring to bone, not for sliding.
Ti-6Al-4V
The most common orthopaedic alloy ("Grade 5").
- Titanium (Ti): ~90%.
- Aluminium (Al): 6%. Alpha stabiliser. Increases strength and oxidation resistance.
- Vanadium (V): 4%. Beta stabiliser. Increases ductility.
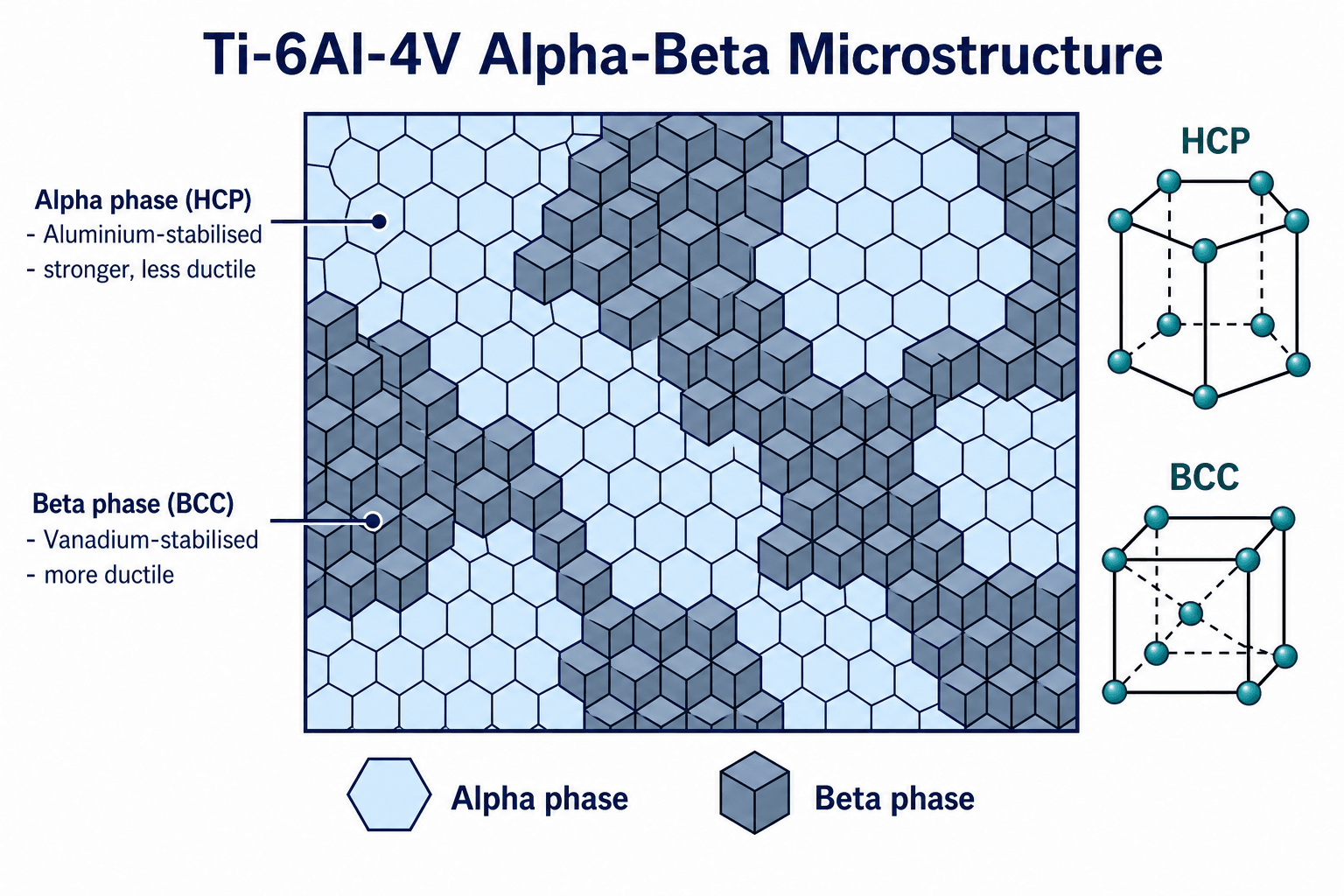
- Alpha: HCP (Hexagonal Close Packed). Stronger, brittle.
- Beta: BCC (Body Centred Cubic). Ductile.
- Ti-6Al-4V is an Alpha-Beta Alloy.
- Forms Titanium Dioxide ($TiO_2$) instantaneously upon exposure to oxygen.
- Extremely stable and protective against saline corrosion.
- The oxide layer is the surface bone deposits directly onto: osteoblasts adhere via integrin-mediated focal adhesions and lay down mineralised matrix in direct apposition (true osseointegration). Hemidesmosomes are the epithelial soft-tissue seal of transmucosal dental implants, not the bone-attachment mechanism (the cell biology is developed in the osseointegration topic).
Overview
- Uncemented femoral stems (THA)
- Acetabular shells and cups
- Locking plates (distal radius, proximal humerus)
- Spinal instrumentation (pedicle screws, rods)
Direct bone apposition (osseointegration) via TiO₂ layer
Ti for Anchoring, NOT Articulation:
- Titanium = Bone interface (stems, shells, plates)
- CoCr/Ceramic = Bearing surface (heads, liners)
Never use Ti femoral head against polyethylene - catastrophic wear
Concepts & Core Principles
Titanium is the orthopaedic metal of choice for anchoring to bone rather than for sliding bearings. Three properties dominate the exam discussion.
- Osseointegration. Titanium spontaneously forms a stable titanium-dioxide (TiO₂) passive layer onto which bone deposits directly, without an intervening fibrous membrane - the basis of cementless biological fixation.
- Low elastic modulus. At ~110 GPa, titanium is roughly half as stiff as cobalt-chrome or stainless steel and far closer to cortical bone (~15-20 GPa), transferring more load to the proximal femur and producing less stress shielding (Wolff's law).
- Poor tribology. Titanium is soft, notch-sensitive and a poor bearing surface; it must never articulate against polyethylene (abrasive wear, black metallosis). Cobalt-chrome or ceramic is used for the bearing couple.
One-line summary: Titanium for the bone interface (stems, shells, plates, screws, cages); cobalt-chrome or ceramic for the articulation.
Microstructure
Hexagonal Close Packed Structure:
- Stronger, more resistant to creep
- Less ductile
- Aluminium (6%) stabilizes alpha phase
- Provides high-temperature strength
Body Centered Cubic Structure:
- More ductile
- Better fatigue resistance
- Vanadium (4%) stabilizes beta phase
- Provides formability
Ti-6Al-4V Combination:
- Dual-phase structure
- Balance of strength AND ductility
- Heat treatable for optimized properties
- Gold standard for orthopaedic use
TiO₂ Passivation Layer:
- Forms within nanoseconds of air exposure
- 2-10nm thick
- Self-healing if scratched
- Bone bonds directly via osteoblast integrin focal adhesions (NOT hemidesmosomes, which are the epithelial soft-tissue seal)
Classification
Titanium Grades for Orthopaedics
- Composition
- Pure titanium
- Properties
- Softer, excellent biocompatibility
- Applications
- Dental, porous coatings
- Composition
- 6% Al, 4% V
- Properties
- High strength, osseointegration
- Applications
- Stems, shells, plates
- Composition
- 6% Al, 7% Nb
- Properties
- No vanadium (less cytotoxic)
- Applications
- Alternative to Grade 5
- Composition
- Ti-Nb-Ta-Zr
- Properties
- Ultra-low modulus (~55 GPa)
- Applications
- Research/newer stems
Commercially Pure Titanium vs the Alloy: What the Grades Mean
The classification names "CP-Ti (1-4)" and "Ti-6Al-4V (Grade 5)" but never explains what separates them — a classic basic-science discriminator.
Commercially pure (CP) titanium is essentially unalloyed titanium, supplied in four grades (1-4) that differ chiefly by their interstitial oxygen (and iron) content: more oxygen raises strength but lowers ductility, so grade 1 is the softest and most ductile and grade 4 the strongest. CP-Ti is even more biocompatible and more ductile than the alloy but considerably weaker, so it is used where bone apposition and formability matter more than bulk strength — porous coatings, sintered beads, fibre-metal pads, mesh and dental implants (the original Brånemark/Albrektsson osseointegration work used unalloyed CP-Ti screws).
Ti-6Al-4V (Grade 5) is the alpha-beta alloy: adding aluminium and vanadium roughly doubles the strength and fatigue resistance, which is why it is the structural substrate for stems, plates and screws — at some cost in ductility, and with the (largely theoretical) ion-release concern that drove vanadium-free variants. The implant specification is the ELI (Extra-Low-Interstitial) grade — a low-oxygen variant with better fracture toughness and fatigue (ASTM F136).
- Strength / interstitials
- Strength rises 1→4 with oxygen content; all weaker but more ductile/biocompatible than the alloy
- Typical role
- Porous coatings, beads, mesh, dental
- Strength / interstitials
- Alpha-beta alloy; roughly double the strength and fatigue resistance
- Typical role
- Structural: stems, plates, screws, cages
They are often combined — a CP-Ti porous coating sintered or diffusion-bonded onto a Ti-6Al-4V substrate gives bone-friendly ingrowth on top of a load-bearing core.
Q: What is the difference between commercially pure titanium and Ti-6Al-4V, and where is each used? A: CP-Ti is unalloyed (grades 1-4 by oxygen content, strength rising 1→4) — softer, more ductile, maximally biocompatible, used for porous/coating and dental surfaces. Ti-6Al-4V is the alpha-beta alloy — roughly double the strength and fatigue resistance, the structural implant metal. They are commonly combined (CP-Ti coating on a Ti-6Al-4V substrate).
Hydroxyapatite Coating: A Bioactive Accelerant, Not a Substitute
The classification and an MCQ pearl both note that a hydroxyapatite (HA) coating "accelerates early osseointegration" and "may delaminate", but the concept deserves development because HA behaves very differently from a roughened metal surface.
- What it is: HA is a calcium-phosphate ceramic chemically similar to the mineral phase of bone, applied as a thin (~50-75 μm) plasma-sprayed layer onto the titanium substrate of cementless stems and cups.
- Why use it (osteoconduction): HA is bioactive and osteoconductive — bone bonds to it chemically and grows along it, so it speeds early bone apposition and can bridge small gaps (of the order of a millimetre or two) between implant and bone that a bare metal surface would not, giving faster, more forgiving early fixation.
- It is partly resorbable: over time the HA is remodelled and replaced, with bone bonding to the underlying roughened metal — so it acts as an early-fixation accelerant rather than a permanent layer. It is usually applied on top of a roughened or porous surface, not instead of one.
- The controversies (the "may delaminate" point): a delaminating coating sheds HA particles that act as third-body wear, accelerating polyethylene wear and osteolysis; coating durability depends on crystallinity and dissolution rate; and crucially, while HA improves early fixation, most long-term studies show little durable advantage over a well-made grit-blasted or porous titanium surface — so its routine use is debated and many modern stems rely on surface roughening or porous titanium alone.
Q: What does a hydroxyapatite coating add to a titanium implant, and what is the catch? A: HA is an osteoconductive calcium-phosphate layer that accelerates early bone bonding and bridges small gaps, then is partly resorbed and replaced by bone on the underlying metal. The catches are delamination → third-body wear/osteolysis and the evidence that it confers little long-term advantage over a good grit-blasted or porous titanium surface — so it is an early accelerant, not a substitute for a sound surface.
Patient-Specific Selection
- Metal hypersensitivity. Titanium very rarely causes hypersensitivity, making it the implant of choice in patients with documented nickel or cobalt-chrome allergy; pre-operative patch testing can be considered in suspected cases.
- Imaging needs. Titanium produces far less artifact than cobalt-chrome or stainless steel and is MRI-safe at 1.5T and 3T - the preferred metal where surveillance imaging matters (spine, tumour, revision).
Testing and Imaging
Imaging with Titanium Implants
- Titanium is radiopaque
- Less dense than CoCr (thinner lines on XR)
- Low artifact compared to other metals
- Safe at 1.5T and 3T
- Metal reduction sequences (MARS) available
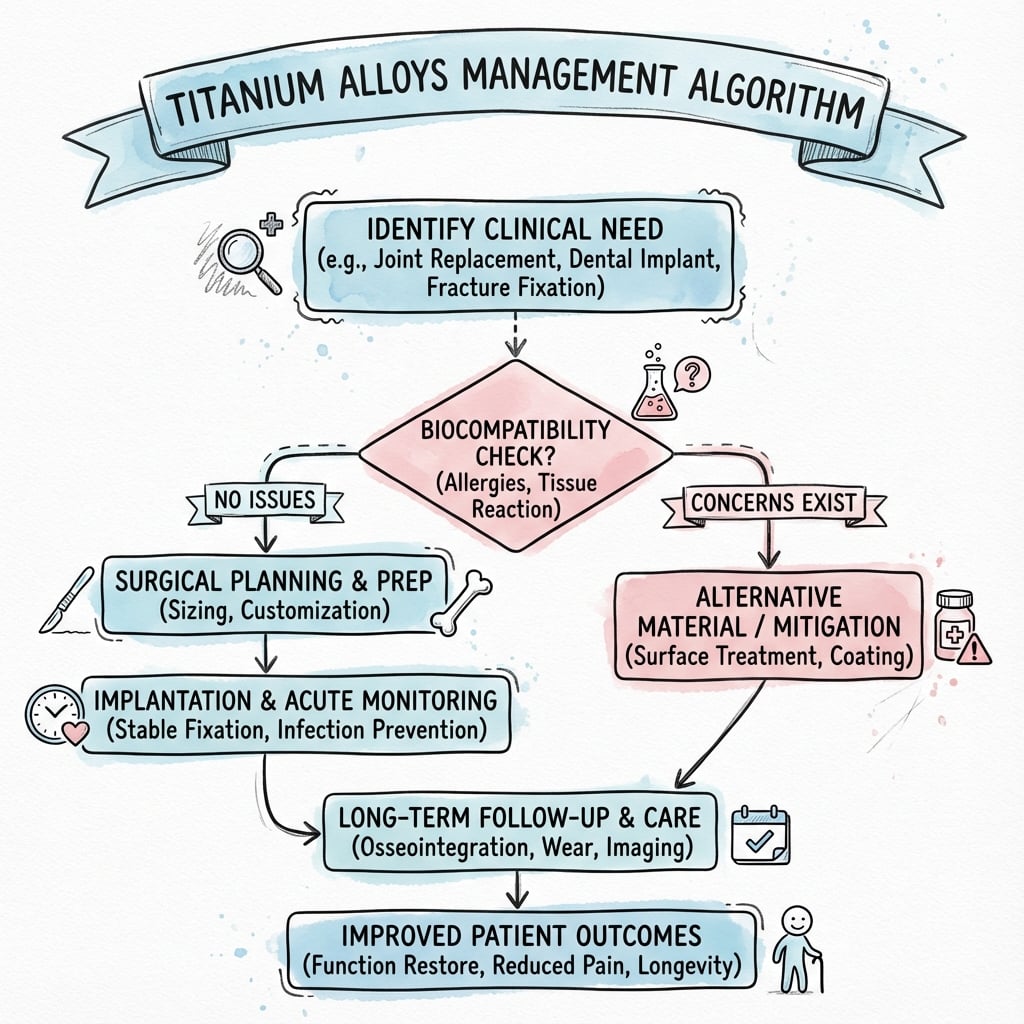
Management Algorithm
Complications
Titanium-Specific Complications
- Screw fuses to plate, cannot remove
- Oxide layers disrupted, raw metal surfaces bond
- Prevention: Anodisation, correct technique
- Cracks propagate from surface defects
- Avoid scratching during surgery
- Thread roots are stress risers
- Black debris if used as bearing surface
- Adverse tissue reaction (metallosis)
- NEVER use Ti head on polyethylene
Postoperative Considerations
Follow-up for Ti Implants
- Bone ingrowth: 6-12 weeks
- Protected weightbearing initially
- Monitor for subsidence on radiographs
- Hardware removal possible but cold welding risk
- Consider leaving asymptomatic hardware
- Document implant details for future surgery
Clinical Relevance
Why Ti for Stems, CoCr for Heads?
Comparing Orthopaedic Metals
The exam "differential" for a biomaterials viva is choosing between the three structural metals. Match the property to the clinical job.
- Titanium (Ti-6Al-4V)
- ~110 GPa (closest to bone)
- Cobalt-Chrome (Co-Cr-Mo)
- ~210-240 GPa
- Stainless Steel (316L)
- ~190-200 GPa
- Titanium (Ti-6Al-4V)
- Excellent (TiO2, osseointegrates)
- Cobalt-Chrome (Co-Cr-Mo)
- Good (releases Co/Cr ions)
- Stainless Steel (316L)
- Moderate (Ni sensitivity)
- Titanium (Ti-6Al-4V)
- Poor - never a bearing surface
- Cobalt-Chrome (Co-Cr-Mo)
- Excellent - heads, MoM, knees
- Stainless Steel (316L)
- Poor - not a bearing surface
- Titanium (Ti-6Al-4V)
- Outstanding (self-healing oxide)
- Cobalt-Chrome (Co-Cr-Mo)
- Excellent
- Stainless Steel (316L)
- Liable to crevice/pitting corrosion
- Titanium (Ti-6Al-4V)
- Low (preferred for spine/tumour)
- Cobalt-Chrome (Co-Cr-Mo)
- High
- Stainless Steel (316L)
- High
- Titanium (Ti-6Al-4V)
- Stems, shells, plates, screws, cages
- Cobalt-Chrome (Co-Cr-Mo)
- Femoral heads, bearings, modular junctions
- Stainless Steel (316L)
- Temporary fixation, low-cost trauma implants
Discriminator: If the question stresses bone fixation, low stiffness or MRI the answer is titanium. If it stresses a hard, smooth, wear-resistant articulating surface the answer is cobalt-chrome (or ceramic). Stainless steel is the cheap, ductile, easily-contoured choice for temporary or resource-limited trauma fixation.
Clinical Applications
Orthopaedic Applications
- Uncemented femoral stems (standard)
- Acetabular shells (porous coated)
- NOT for femoral heads (use CoCr or ceramic)
- Locking plates (distal radius, proximal humerus)
- Intramedullary nails
- Screws (beware cold welding)
- Pedicle screws
- Rods (may be preferred over CoCr for MRI)
- Interbody cages (Ti or PEEK)
Surgical Handling
Handling Titanium Implants
- Use correct screwdriver (Star/Torx preferred over Hex)
- Maintain axial pressure
- Avoid cross-threading (soft metal)
- Single insertion preferred (reduces cold welding)
- Contour carefully (notch sensitivity)
- Avoid scratching surface
- Use anodised screws with plates
Guidelines, Registries & Global Practice
OrthoVellum is a global resource. Titanium implant selection is governed by international material standards and supported by convergent registry evidence worldwide.
Recognised internationally:
- ASTM F136 / ISO 5832-3 — wrought Ti-6Al-4V ELI for surgical implants
- ASTM F1472 / F67 — Ti-6Al-4V and CP-titanium
- ISO 5832-11 — Ti-6Al-7Nb (vanadium-free)
- ISO 13485 — manufacturer quality management
Standards are referenced by AAOS, BOA, AO and EFORT alike.
Convergent registry signal (NJR, AJRR, AOANJRR, SHAR, NZJR):
- Cementless titanium stems achieve high long-term survival across registries
- Stem material is rarely the failure driver; bearing wear and instability dominate revisions
- Cementing is favoured in older/osteoporotic patients in several registries (periprosthetic fracture risk with cementless)
Where guidance differs:
- NICE / BOA (UK) and several registries: cemented or hybrid fixation preferred in elderly hip-fracture patients
- AAOS (US) and many high-volume centres: cementless titanium fixation common across age groups
- AO Foundation: titanium locking plates standard for periarticular and osteoporotic fractures (angular stability, low artifact)
High vs limited resource:
- High-resource: titanium stems, ceramic bearings, 3D-printed augments, MRI-driven titanium spinal constructs
- Limited-resource: stainless steel remains common for trauma fixation (lower cost, ductile, easily contoured); titanium reserved for selected reconstructions
Global exam point: Across the major registries, cementless titanium stems osseointegrate reliably and survive into the third decade; revisions are driven by the bearing/acetabular side, not the stem. The live debate is fixation method in the elderly (cemented vs cementless), not the material — titanium remains the dominant cementless metal worldwide.
Controversies & Areas of Uncertainty
- Beta-titanium and "modulus matching". Low-modulus beta alloys (Ti-Nb-Ta-Zr, ~55-80 GPa) promise less stress shielding, but reducing stiffness too far risks higher implant strain, fatigue and micromotion. The optimum stem stiffness remains undefined and clinical superiority over Ti-6Al-4V is unproven.
- Vanadium and aluminium toxicity. Concern over vanadium and aluminium ion release drove vanadium-free alternatives (Ti-6Al-7Nb, Ti-5Al-2.5Fe). Clinical evidence of harm from Ti-6Al-4V in vivo is weak, so Grade 5 remains the workhorse alloy; the issue is largely theoretical.
- Titanium particle debris and "metallosis". Abrasive titanium wear (from a Ti bearing, fretting at modular junctions, or impingement) can cause black staining and an adverse local tissue reaction. The threshold for revising a stained but asymptomatic joint is debated.
- Trunnionosis / mixed-metal junctions. Fretting-crevice corrosion at the titanium-stem/cobalt-chrome-head taper can release metal debris. Whether to avoid mixed-metal couples or accept them with good taper engineering is unresolved.
- 3D-printed porous titanium. Additively manufactured trabecular structures reproduce ideal pore geometry, but long-term registry data, fatigue behaviour of as-printed lattices, and powder-residue effects are still maturing.
MCQ Practice Points
Q: What is the composition and key mechanical property of Ti-6Al-4V alloy used in orthopaedic implants?
A: Ti-6Al-4V contains 90% titanium, 6% aluminium (alpha stabilizer), 4% vanadium (beta stabilizer). Key properties: Elastic modulus 110 GPa (closest to cortical bone at 18-20 GPa of any metal), excellent corrosion resistance, excellent biocompatibility. Lower modulus reduces stress shielding compared to CoCr (210 GPa) or stainless steel (200 GPa).
Q: Why is titanium NOT used for articulating bearing surfaces in joint replacement?
A: Titanium has poor wear resistance and high coefficient of friction. Titanium oxide layer (provides corrosion resistance) is easily disrupted by articulation, causing abrasive wear, metal debris, and adverse tissue reactions. Titanium is used for: stems, shells, plates, screws - NOT for femoral heads or tibial trays articulating with polyethylene. CoCr or ceramic used for bearing surfaces.
Q: What is the mechanism of titanium's corrosion resistance?
A: Spontaneous formation of a passive titanium oxide (TiO2) layer 2-10nm thick. This layer reforms within milliseconds if damaged. The oxide layer prevents further oxidation and ion release. Titanium is "bioinert" due to this stable oxide. Contrast with CoCr which releases metal ions (cobalt, chromium) and stainless steel which may corrode in vivo.
Q: What is "notch sensitivity" in the context of titanium implants?
A: Tendency for crack initiation and propagation from surface defects (scratches, notches, thread roots). Titanium is more notch-sensitive than stainless steel. Implications: careful handling during surgery (avoid scratching), smooth surface finish, avoidance of sharp corners in implant design. Screw threads are stress risers - titanium screws can fail at thread root.
Q: What is the advantage of porous titanium coatings on cementless implants?
A: Allows bone ingrowth for biological fixation. Pore size 100-400 μm optimal for bone ingrowth. Surface treatments include: plasma spray, sintered beads, electron beam melting (EBM), 3D printing (trabecular metal-like structures). Titanium's biocompatibility and ability to osseointegrate makes it ideal for cementless fixation. Hydroxyapatite coating may accelerate early osseointegration.
At a Glance
Titanium (Ti-6Al-4V) is the most biocompatible orthopaedic metal due to its spontaneous TiO₂ passivation layer that permits direct bone apposition—the basis of osseointegration. It has lower elastic modulus (~110 GPa) compared to stainless steel/CoCr (~200 GPa), reducing stress shielding and making it ideal for uncemented femoral stems. The alpha-beta alloy structure provides strength (aluminium) and ductility (vanadium). However, titanium is soft with poor wear resistance and notch sensitivity, making it unsuitable for bearing surfaces—never use titanium femoral heads against polyethylene. Cold welding between titanium screws and plates is prevented by Type II anodisation. Applications include uncemented arthroplasty components, locking plates, and spinal instrumentation.
B-O-N-E vs W-E-A-RTitanium Pros and Cons
Hook:Ti is for BONE, not for WEAR
6 A's, 4 V'sTi-6Al-4V Composition
Hook:Aluminium stabilises Alpha (both start with A); Vanadium leaves a Void of brittleness by stabilising the ductile beta phase
Modulus of Elasticity
- Titanium: ~110 GPa.
- Stainless Steel/CoCr: ~200-240 GPa.
- Cortical Bone: ~20 GPa.
Significance:
- Titanium has a modulus much closer to bone than Steel/CoCr.
- This creates Less Stress Shielding.
- Ideal for femoral stems where load transfer to proximal bone prevents resorption (Wolff's Law).
Cold Welding
- When a Ti screw is tightened into a Ti plate, the oxide layers can scrape off.
- The two raw metal surfaces fuse under pressure ("Gall").
- Result: Screw cannot be removed.
- Anodisation (Type II): Electrochemical thickening of the oxide layer (makes it harder/grey).
- Using different alloys for screw vs plate (less common).
- 2895 unalloyed titanium screws placed in jaw and 124 in tibial/temporal/iliac bone without cement, achieving direct bone-to-implant contact (osseointegration)
- SEM and TEM of 38 retrieved integrated screws showed a direct bone-titanium interface with no intervening fibrous tissue
- No wear products were seen in bone or soft tissue despite loading times up to 90 months
- Soft tissue formed a biological seal preventing microorganism infiltration along trans-mucosal implants
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
Composition (Grade 5)
- Titanium (Base)
- Aluminium (Alpha)
- Vanadium (Beta)
Key Features
- Low Modulus (110 GPa)
- Biocompatible (TiO2)
- Cold Welding risk
Evidence Base
- Titanium alloys offer lower elastic modulus, superior biocompatibility and enhanced corrosion resistance compared with stainless steels and cobalt-based alloys
- Charts the progression from alpha (CP-Ti) and alpha-beta (Ti-6Al-4V) alloys to metastable beta titanium alloys with reduced modulus and superior notch-fatigue resistance
- Poor shear strength and poor wear resistance remain the principal limitations of titanium as a load-bearing/wear component
- Long-term performance is governed by fatigue and wear behaviour rather than static strength
- Smooth (Sa under 0.5 μm) and minimally rough (Sa 0.5-1 μm) surfaces produced weaker bone responses than rougher surfaces
- Moderately rough surfaces (Sa over 1-2 μm) gave the strongest bone-to-implant contact and removal-torque values
- Bone response is influenced at the micrometre and possibly nanometre scale, supporting controlled surface roughening
- Most published studies were limited by inadequate, non-standardised surface characterisation
- Porous-surfaced implants placed in canine femora for 4, 8 and 12 weeks with four distinct pore-size ranges
- A pore size of approximately 50 to 400 μm gave the maximum shear fixation strength (17 MPa) in the shortest time (8 weeks)
- Pore sizes outside this window achieved weaker or slower fixation
- Study used cobalt-base alloy beads but the pore-size principle was generalised to all porous metal coatings including titanium
- 354 grit-blasted tapered titanium stems followed for a mean of 22 years (minimum 20)
- Survivorship for femoral revision for aseptic loosening was 93% at 22 years (95% CI 90-96%)
- Undersized stems (canal fill under 80%) carried a 4.2-fold higher risk of aseptic loosening
- Patient age, male sex and diagnosis were not associated with higher loosening risk
- Proximally porous-coated, plasma-sprayed titanium-alloy straight stem followed at a mean of 20 years
- Mean Harris hip score improved from 46 to 87 points
- All hips showed proximal remodelling consistent with osseous ingrowth; no stem was revised for loosening
- Femoral osteolysis occurred in 20% but the acetabular component was the main failure mode (30% revised)
References
- Albrektsson T, Brånemark PI, Hansson HA, Lindström J. Osseointegrated titanium implants. Acta Orthop Scand. 1981;52(2):155-170. PMID 7246093. doi:10.3109/17453678108991776
- Long M, Rack HJ. Titanium alloys in total joint replacement--a materials science perspective. Biomaterials. 1998;19(18):1621-1639. PMID 9839998. doi:10.1016/s0142-9612(97)00146-4
- Wennerberg A, Albrektsson T. Effects of titanium surface topography on bone integration: a systematic review. Clin Oral Implants Res. 2009;20(Suppl 4):172-184. PMID 19663964. doi:10.1111/j.1600-0501.2009.01775.x
- Bobyn JD, Pilliar RM, Cameron HU, Weatherly GC. The optimum pore size for the fixation of porous-surfaced metal implants by the ingrowth of bone. Clin Orthop Relat Res. 1980;(150):263-270. PMID 7428231.
- Streit MR, Innmann MM, Merle C, et al. Long-term (20- to 25-year) results of an uncemented tapered titanium femoral component. Clin Orthop Relat Res. 2013;471(10):3262-3269. PMID 23670671. doi:10.1007/s11999-013-3033-4
- Meding JB, Ritter MA, Keating EM, Berend ME. Twenty-year followup of an uncemented stem in primary THA. Clin Orthop Relat Res. 2015;473(2):543-548. PMID 24993142. doi:10.1007/s11999-014-3763-y