Radial-sided wrist pain with gripping | STT degeneration at radial carpus | Watson grade directs surgery | CMC coexists 30-40%
- STT joint is distal scaphoid articulation with trapezium-trapezoid at radial carpus
- Tenderness located 1cm distal and radial to radial styloid; pain on resisted wrist extension
- Carpal tunnel (skyline) view is essential to profile STT joint space narrowing and osteophytes
- Watson Grade I-II (isolated): distal scaphoid excision or STT fusion; Grade III (pancarpal): PRC or arthrodesis
- Coexists with thumb CMC arthritis in 30-40% of cases - always assess both joints
- “Always obtain carpal tunnel view - STT joint frequently obscured on standard PA radiograph
- “Use diagnostic STT injection to confirm pain generator before surgery, especially with coexisting CMC arthritis
- “Preserve proximal scaphoid and scapholunate ligament attachment during distal excision to avoid instability
- “STT fusion for high-demand patients trades 10-15° motion loss for maintained grip strength
Triscaphe Arthritis (STT Arthritis)
Core Exam Knowledge
- Anatomic location: Articulation between distal scaphoid and trapezium-trapezoid (radial carpus)
- Classic presentation: Radial-sided wrist pain with gripping, tenderness over STT joint, pain with wrist extension and radial deviation
- Associated conditions: Often coexists with thumb CMC arthritis (30-40% of cases) and scapholunate dissociation
- Imaging hallmark: Joint space narrowing, subchondral sclerosis, and osteophytes on PA and carpal tunnel view radiographs
- Conservative first-line: Activity modification, NSAIDs, corticosteroid injection (50-60% achieve temporary relief)
- Surgical options: Distal scaphoid excision with tendon interposition (isolated STT), STT fusion (younger active patients), proximal row carpectomy (pancarpal involvement)
- Do not treat the STT joint in isolation when thumb CMC arthritis coexists (30-40%) - confirm the dominant pain generator with a diagnostic injection first, or persistent pain will follow.
- Always obtain a carpal tunnel or oblique view - the STT joint is frequently obscured on a standard PA radiograph, and missing the diagnosis is a classic error.
- Do not over-resect the distal scaphoid - excessive excision risks carpal instability; preserve the proximal scaphoid and its scapholunate attachment.
- Avoid isolated STT fusion when radiocarpal (radioscaphoid) arthritis is present - it will fail; this is Grade III disease requiring salvage (PRC or total wrist fusion).
Clinical Examination: Tenderness directly over STT joint (palpable 1cm distal and radial to radial styloid), pain with resisted wrist extension, scaphoid compression test positive
Imaging Views: PA radiograph shows joint narrowing, carpal tunnel view best demonstrates STT joint space, lateral shows scaphoid alignment
Watson Classification: Grades I-III based on radiographic severity and extent of involvement
Surgical Decision-Making: Isolated STT = excision arthroplasty; younger/higher demand = STT fusion; pancarpal disease = proximal row carpectomy
Epidemiology and Disease Burden
Incidence and Demographics
Triscaphe arthritis is less common than scapholunate advanced collapse (SLAC) but is the second most frequent pattern of degenerative wrist arthritis and a significant cause of radial-sided wrist pain. The condition affects both men and women, with a slight male predominance in post-traumatic cases and female predominance in primary osteoarthritis cases. Age of presentation is typically 45-65 years, though post-traumatic cases may present earlier.
Risk Factors and Etiology
STT arthritis may be primary (idiopathic osteoarthritis) or secondary to underlying pathology. Risk factors include previous wrist trauma (particularly scaphoid fractures or distal radius fractures involving the radiocarpal joint), scapholunate dissociation (altered carpal mechanics leading to abnormal STT loading), hypermobility of the STT joint, thumb CMC arthritis (often coexistent due to shared biomechanical forces), and generalized osteoarthritis affecting multiple joints.
Post-traumatic arthritis is particularly common following scaphoid malunion with humpback deformity, where the abnormal scaphoid position concentrates load on the distal scaphoid-trapezium articulation. Chronic scapholunate dissociation alters carpal kinematics, increasing STT joint reactive forces and accelerating degenerative changes.
Associated Conditions
High Yield: STT arthritis commonly coexists with thumb CMC arthritis (30-40% of cases).
Pathophysiology and Anatomy
STT Joint Anatomy
The scaphotrapeziotrapezoid (STT) joint is a complex three-bone articulation at the radial carpus. The distal pole of the scaphoid articulates with the trapezium and trapezoid in a reciprocally curved saddle-type configuration. The joint surfaces are covered with hyaline articular cartilage and are supported by a fibrous joint capsule reinforced by intrinsic ligaments including the scaphotrapezial ligament and scaphotrapezoid ligament.
The STT joint is distinct from the scaphocapitate articulation medially and the trapezium-first metacarpal (thumb CMC) joint distally, though biomechanically these articulations are interdependent. The STT joint functions as a transitional zone between the mobile distal carpal row (trapezium and trapezoid) and the relatively fixed scaphoid, which serves as a mechanical link between the proximal and distal rows.
Biomechanics and Load Transmission
- stt_position
- Scaphoid extends, STT compressed
- load
- High compressive load
- stt_position
- Scaphoid flexes, STT decompressed
- load
- Low load
- stt_position
- Maximum STT compression
- load
- Highest load across joint
- stt_position
- STT relatively decompressed
- load
- Lower load
- stt_position
- Wrist extends, STT loads
- load
- High repetitive load
NOP - Narrowing, Osteophytes, PancarpalWatson STT Arthritis Classification
Hook:As arthritis progresses from Grade I to III, think NOP - it gets progressively worse
Watson's classification for STT arthritis parallels his classification for SLAC wrist. Grade I shows joint space narrowing at the STT articulation with minimal subchondral changes and no osteophytes. Grade II demonstrates advanced STT arthritis with subchondral sclerosis, cyst formation, and osteophyte formation, but the radiocarpal joint (particularly radiolunate articulation) and midcarpal joint are preserved. Grade III includes involvement of adjacent joints, particularly the radioscaphoid or capitolunate articulations, indicating pancarpal degenerative disease.
This classification has important treatment implications. Grade I-II STT arthritis with preserved adjacent joints is amenable to joint-preserving surgery (distal scaphoid excision) or STT fusion. Grade III arthritis typically requires proximal row carpectomy or total wrist arthrodesis.
Advanced Imaging
Computed tomography (CT) provides detailed assessment of bone architecture, osteophyte location and size, subchondral cyst formation, and the extent of cartilage loss (inferred from joint space narrowing). CT is particularly valuable for preoperative planning when STT fusion is contemplated, as it defines the quality of bone stock and optimal fusion position. Three-dimensional reconstructions help visualize complex deformity.
Magnetic resonance imaging (MRI) directly visualizes articular cartilage (on high-resolution sequences), bone marrow edema (suggesting active degenerative process), synovitis, and associated soft tissue pathology including ganglion cysts. MRI also assesses the scapholunate ligament (looking for occult dissociation) and the remainder of the carpus for additional pathology. However, plain radiographs and CT are usually sufficient for diagnosis and treatment planning.
Diagnostic Injection
Fluoroscopically guided corticosteroid injection into the STT joint serves both diagnostic and therapeutic purposes. Temporary pain relief following injection confirms the STT joint as the primary pain generator, which is particularly valuable when multiple potential sources exist (thumb CMC arthritis, de Quervain tenosynovitis, radiocarpal arthritis). The injection typically combines a corticosteroid (triamcinolone 40mg or methylprednisolone 40mg) with local anesthetic (lidocaine or bupivacaine).
Response to injection is assessed based on pain relief duration and degree. Complete relief lasting several hours (during local anesthetic effect) followed by gradual return of symptoms over days to weeks confirms STT arthritis. Lack of relief or minimal improvement suggests alternative or additional pain sources requiring further investigation.
Conservative Options
Non-Operative Treatment
Patient Presentation
History
Patients typically present with radial-sided wrist pain that is insidious in onset and progressive over months to years. The pain is activity-related and worse with gripping, pushing, wrist extension, and radial deviation. Specific aggravating activities include push-ups, yoga (downward dog position), lifting heavy objects, using tools (screwdrivers, hammers), and keyboard use with wrist extension. Pain may radiate proximally along the radial forearm or distally into the thenar eminence, particularly when thumb CMC arthritis coexists.
Rest typically provides partial relief, though night pain may occur in advanced cases. Morning stiffness lasting 10-30 minutes is common. Mechanical symptoms such as clicking or catching may be reported, particularly if loose bodies are present. Weakness is often described but typically reflects pain inhibition rather than true motor deficit.
Physical Examination
Inspection: Look for thenar atrophy (suggests median nerve involvement or severe thumb CMC arthritis), swelling over radial wrist (usually mild), and deformity (rare unless severe)
Palpation: Direct tenderness over STT joint (1cm distal and radial to radial styloid, just proximal to thumb CMC joint); compare to CMC joint and radial styloid
Range of Motion: Usually preserved or mildly reduced; document flexion, extension, radial deviation, ulnar deviation; pain typically at extremes of extension and radial deviation
Provocative Tests: STT compression test (axial load on thumb while moving wrist in radial/ulnar deviation), resisted wrist extension (reproduces pain), grind test (if CMC also involved)
Strength: Grip strength often reduced 20-40% compared to contralateral side; pinch strength may be reduced if CMC involved
Neurovascular: Assess median and radial nerve function; superficial radial nerve may be tender if compressed by osteophytes
The STT compression test is performed by applying axial compression through the thumb metacarpal while passively moving the wrist from ulnar to radial deviation. Pain with this maneuver, particularly localized to the STT joint, is highly suggestive of STT arthritis. Comparison with the contralateral asymptomatic wrist helps differentiate pathologic findings from normal joint crepitus.
Functional Impact
Functional limitations correlate with pain severity and arthritic stage. Common difficulties include reduced grip strength affecting jar opening, lifting, and tool use, inability to bear weight on extended wrist (affecting push-ups, yoga, transfers), keyboard and mouse use (particularly if wrist extension is required), and steering wheel manipulation. Patients may develop compensatory strategies such as avoiding wrist extension or shifting tasks to the opposite hand.
Anatomy
STT Joint Anatomy
- Distal scaphoid pole: Saddle-shaped articular surface
- Trapezium: Radial component, also articulates with thumb CMC
- Trapezoid: Ulnar component, smallest carpal bone
- Complex three-bone articulation at radial carpus
- Functionally linked to thumb CMC joint distally
- Scaphocapitate joint medially
- Scaphotrapezial ligament
- Scaphotrapezoid ligament
- Joint capsule reinforced by intrinsic ligaments
- STT joint palpable 1cm distal and radial to radial styloid
- Distinct from thumb CMC (more distal) and scaphoid tubercle (more proximal)
Classification
Watson Classification for STT Arthritis
- Radiographic Findings
- Joint space narrowing, minimal changes
- Adjacent Joints
- Preserved radiocarpal/midcarpal
- Treatment Options
- Conservative, excision arthroplasty
- Radiographic Findings
- Sclerosis, cysts, osteophytes
- Adjacent Joints
- Preserved radiocarpal/midcarpal
- Treatment Options
- Excision arthroplasty, STT fusion
- Radiographic Findings
- Advanced STT degeneration
- Adjacent Joints
- Radiocarpal or midcarpal involved
- Treatment Options
- PRC or total wrist arthrodesis
Key Principle:
- Grade I-II: Joint-preserving surgery possible
- Grade III: Salvage procedures required
Clinical Assessment
Clinical Examination for STT Arthritis
- Radial-sided wrist pain (insidious onset, progressive)
- Worse with gripping, pushing, wrist extension
- Aggravating activities: push-ups, lifting, keyboard use
- Morning stiffness 10-30 minutes
- Mild swelling over radial wrist (if present)
- Thenar atrophy suggests concurrent thumb CMC arthritis or median nerve involvement
- STT joint tenderness: 1cm distal and radial to radial styloid
- Compare to CMC joint (more distal) and radial styloid (more proximal)
- STT compression test: Axial load through thumb + wrist radial/ulnar deviation
- Resisted wrist extension: Reproduces STT pain
- Grind test: Positive if concurrent CMC arthritis
Investigations
Imaging for STT Arthritis
- PA view: Joint space narrowing, subchondral sclerosis, osteophytes
- Lateral view: Scaphoid position, radiocarpal alignment
- Oblique view: Additional joint visualization
- Carpal tunnel (skyline) view: Best profiles STT joint
- Wrist in maximum dorsiflexion, beam directed proximally from palm
- Clearly demonstrates joint space and subchondral changes
- Joint space narrowing at STT articulation
- Subchondral sclerosis
- Marginal osteophytes (often dorsal)
- Subchondral cysts (advanced disease)
Radiological Assessment
Radiographic Evaluation
Standard wrist radiographs including posteroanterior (PA), lateral, and oblique views form the foundation of imaging assessment. The PA view demonstrates joint space narrowing at the STT articulation, subchondral sclerosis, and marginal osteophytes. However, the STT joint is often better visualized on specialized views.
The carpal tunnel (skyline) view, the semi-supinated oblique, and a PA view in slight ulnar deviation are the most useful projections for profiling the STT joint, which is frequently obscured by bony overlap on a standard PA radiograph. The carpal tunnel view is obtained with the wrist in maximum dorsiflexion, with the X-ray beam directed proximally from the palm. This view profiles the STT joint and clearly demonstrates joint space narrowing, subchondral changes, and the relationship between the distal scaphoid and the trapezium-trapezoid. This view should be standard in the assessment of radial wrist pain when STT arthritis is suspected.
The lateral radiograph assesses overall carpal alignment, scaphoid position (looking for flexion deformity from SL dissociation or extension from malunion), and the radiocarpal joint. Scaphoid-specific views (PA with ulnar deviation and slight extension) may reveal scaphoid pathology such as malunion or nonunion that predisposes to STT arthritis.
Radiographic Classification
Initial management of STT arthritis is conservative, particularly for Grade I disease and mild Grade II. Activity modification involves avoiding or limiting provocative positions and activities, particularly wrist extension with loading, forceful gripping, and repetitive radial deviation. Patients are educated to modify technique (using neutral wrist position for lifting, avoiding push-up exercises, adjusting keyboard ergonomics).
Non-steroidal anti-inflammatory drugs (NSAIDs) provide symptomatic relief and may reduce synovitis. Topical NSAIDs (diclofenac gel) may be preferred for patients with gastrointestinal concerns or those on anticoagulation. Acetaminophen is an alternative for pain control without anti-inflammatory effects.
Splinting with a wrist extension restriction orthosis (limiting wrist extension to 20-30 degrees) reduces STT joint loading and may provide symptom relief during activities. Custom thermoplastic splints fabricated by hand therapists or off-the-shelf wrist braces may be used. Splints are typically worn during aggravating activities rather than continuously to avoid stiffness and muscle deconditioning.
Corticosteroid injection provides temporary relief in 60-80% of patients, with duration of benefit ranging from weeks to months. Repeat injections may be performed, though prolonged corticosteroid use risks cartilage damage and is generally limited to 2-3 injections per year. Hyaluronic acid (viscosupplementation) has been described for STT arthritis but lacks robust evidence supporting its efficacy.
Indications for Surgery
Surgical treatment is considered when conservative measures fail to provide adequate symptom control, pain significantly limits function or quality of life, patients wish to return to activities incompatible with conservative management, or there is documented radiographic progression despite conservative treatment. The duration of conservative treatment varies but typically 3-6 months of appropriate therapy is recommended before proceeding to surgery.
Distal Scaphoid Excision
- indication
- Grade I-II isolated STT arthritis
- technique
- Excise distal 2-4mm scaphoid, interposition arthroplasty
- outcomes
- 80-85% satisfaction, preserves wrist motion
- indication
- Young, high-demand patients, Grade II
- technique
- Fuse scaphoid-trapezium-trapezoid in situ
- outcomes
- Reliable pain relief, some motion loss (10-15 degrees)
- indication
- Grade III with pancarpal arthritis, intact capitate-lunate fossa
- technique
- Excise scaphoid, lunate, triquetrum
- outcomes
- Good pain relief, 50% motion, reliable salvage
- indication
- Grade III, failed prior surgery, severe arthritis
- technique
- Fuse radius to metacarpals
- outcomes
- Complete pain relief, no wrist motion, stable support
Distal scaphoid excision with tendon interposition arthroplasty is the most common procedure for isolated STT arthritis (Grade I-II). The technique involves a radial-sided approach between the first and second dorsal compartments or a volar-radial approach. The distal 2-4mm of the scaphoid is excised using an osteotome or oscillating saw, removing all arthritic bone and osteophytes while preserving the scapholunate ligament attachment proximally.
Interposition arthroplasty using a rolled portion of flexor carpi radialis (FCR) tendon, capsule, or allograft is performed to prevent bone-to-bone contact between the proximal scaphoid and trapezium. The interposition material is secured with suture or anchor. Some surgeons perform simple excision without interposition with comparable results.
Postoperative immobilization in a thumb spica splint for 2 weeks is followed by progressive range of motion exercises. Full activity is typically allowed at 6-8 weeks. Outcomes are generally good with 80-85% patient satisfaction and relief of pain. Complications include persistent pain (10-15%), scaphoid instability (rare), and progressive radiocarpal arthritis (long-term concern).
STT Arthrodesis
STT fusion is preferred for younger, higher-demand patients who wish to maintain grip strength and are willing to accept some motion loss. The procedure involves exposure of the STT joint, removal of articular cartilage from all three surfaces (scaphoid, trapezium, trapezoid), positioning the bones in optimal alignment (slight scaphoid extension to prevent flexion collapse), and fixation with headless compression screws, plates, or K-wires.
Bone graft (usually iliac crest autograft or allograft) is placed in the fusion site to promote union. Immobilization in a thumb spica cast for 6-8 weeks is required, followed by protected motion until fusion is confirmed radiographically (typically 10-14 weeks). Fusion rates are 85-95% with modern techniques and rigid fixation.
Outcomes after STT fusion include excellent pain relief in 85-90% of patients, maintenance of grip strength close to pre-disease levels, and wrist motion loss of approximately 10-15 degrees in flexion-extension arc and 10 degrees in radial-ulnar deviation. Complications include nonunion (5-15%), hardware prominence or irritation, and progression to radiocarpal arthritis (long-term concern due to altered carpal kinematics).
Proximal Row Carpectomy
Proximal row carpectomy (PRC) is indicated for Grade III STT arthritis with pancarpal involvement, provided the lunate fossa of the radius and the head of the capitate have preserved articular cartilage. The procedure involves complete excision of the scaphoid, lunate, and triquetrum through a dorsal approach. The capitate articulates directly with the lunate fossa, creating a new radiocarpal articulation.
PRC provides reliable pain relief (80-85% satisfaction) and preserves functional wrist motion (typically 50-60% of normal flexion-extension arc). Grip strength recovers to 70-80% of the contralateral side. The procedure is advantageous as a salvage option because it does not burn bridges for future reconstruction (total wrist arthrodesis remains possible if PRC fails). Long-term concerns include progressive capitate-lunate fossa arthritis, though this is typically slow in onset.
Total Wrist Arthrodesis
Total wrist arthrodesis is reserved for Grade III arthritis with extensive cartilage loss that precludes PRC, failed prior motion-preserving surgery, or patients with low functional demands who prioritize pain relief and stable support over motion. The procedure fuses the radius to the second and third metacarpals in neutral to slight extension (10-15 degrees) and neutral radial-ulnar deviation.
Fixation options include dorsal plates (most common), intramedullary rods, or combinations. Bone graft promotes fusion, which is achieved in greater than 95% of cases. Pain relief is excellent and predictable. The primary disadvantage is complete loss of wrist motion, which impacts activities of daily living. However, most patients adapt well, particularly if unilateral involvement allows the opposite hand to perform two-handed tasks.
Surgical Risks
Surgical Considerations
Persistent Pain after Excision: May indicate incomplete excision, scaphoid instability, or unrecognized radiocarpal arthritis; reassess with CT and consider revision or salvage
Nonunion after STT Fusion: Occurs in 5-15%; may be asymptomatic or painful; symptomatic nonunion requires revision with bone graft and rigid fixation
Hardware Prominence: Common with dorsal plates and screws; remove hardware if symptomatic after fusion consolidation
Progressive Radiocarpal Arthritis: Long-term concern after both excision and fusion; monitor with serial radiographs; PRC or arthrodesis if develops
Superficial Radial Nerve Injury: Risk with radial approaches; protect nerve branches, avoid retractor pressure; dysesthesias usually temporary
Early complications include wound healing problems (infection, dehiscence), hematoma formation, and superficial radial nerve injury (numbness or painful neuroma over radial thumb and dorsal hand). Hardware-related complications include screw prominence, plate irritation, and hardware failure. Complex regional pain syndrome (CRPS) is rare but devastating when it occurs (less than 2% incidence).
Late complications include persistent pain despite surgery (10-15% after excision, 5-10% after fusion), nonunion after STT fusion (5-15%), scaphoid instability after excessive distal scaphoid excision, and progressive radiocarpal or midcarpal arthritis (long-term concern after both excision and fusion due to altered kinematics). Thumb CMC arthritis may become symptomatic or progress after STT surgery if not addressed concurrently.
Outcomes and Prognosis
Patient satisfaction after surgical treatment for STT arthritis is generally good, with 75-85% reporting significant improvement. Pain relief is achieved in 80-90% of patients, though complete pain resolution is uncommon. Functional outcomes include return to work in 85-90% of patients (3-4 months for excision, 4-6 months for fusion), return to recreational activities in 70-80%, and grip strength recovery to 75-90% of contralateral side.
Factors predicting better outcomes include isolated STT arthritis without pancarpal involvement (Grade I-II), absence of workers' compensation or litigation, realistic patient expectations, and good compliance with postoperative rehabilitation. Factors predicting poorer outcomes include Grade III arthritis with radiocarpal involvement, concurrent thumb CMC arthritis not addressed, smoking (affects fusion healing), and secondary gain issues.
Key Concepts
STT Arthritis Fundamentals
- Degenerative arthritis affecting the scaphotrapeziotrapezoid (STT) joint
- Also known as triscaphe arthritis
- Accounts for 10-15% of degenerative wrist arthritis
- Radial-sided wrist pain with gripping and extension
- Tenderness 1cm distal and radial to radial styloid
- Peak incidence 45-65 years
- Often coexists with thumb CMC arthritis (30-40%)
- Details
- Distal scaphoid articulates with trapezium and trapezoid
- Details
- 10-15% of wrist arthritis cases
- Details
- Thumb CMC arthritis (30-40%), scapholunate dissociation
- Details
- Carpal tunnel (skyline) view profiles STT joint best
Differential Diagnosis of Radial Wrist Pain
- Key Site of Tenderness
- STT joint, ~1cm distal-radial to radial styloid
- Provocative Test
- STT compression / resisted wrist extension
- Imaging / Distinguishing Feature
- STT joint narrowing on carpal tunnel view; scaphoid often dorsiflexed (SL angle reduced)
- Key Site of Tenderness
- Base of thumb metacarpal
- Provocative Test
- Grind and traction-shift test positive
- Imaging / Distinguishing Feature
- Trapeziometacarpal narrowing; coexists with STT in 30-40%
- Key Site of Tenderness
- First dorsal compartment over radial styloid
- Provocative Test
- Finkelstein / Eichhoff positive
- Imaging / Distinguishing Feature
- Normal radiographs; ultrasound shows tendon sheath thickening
- Key Site of Tenderness
- Anatomic snuffbox and scaphoid tubercle
- Provocative Test
- Axial thumb compression, snuffbox pain
- Imaging / Distinguishing Feature
- Scaphoid lucency/sclerosis; humpback deformity
- Key Site of Tenderness
- Radial styloid / radioscaphoid joint
- Provocative Test
- Watson scaphoid shift positive
- Imaging / Distinguishing Feature
- Radial styloid beaking, SL widening over 3mm
- Key Site of Tenderness
- ~4cm proximal to wrist, dorsoradial forearm
- Provocative Test
- Pain/crepitus with resisted extension
- Imaging / Distinguishing Feature
- Soft-tissue swelling at first-second compartment crossover; normal joints
STT and thumb CMC arthritis frequently coexist and both cause radial-sided pain. A diagnostic intra-articular injection that localises the dominant pain generator is invaluable before committing to surgery, because treating only one joint is a common cause of persistent postoperative pain.
Management Algorithm
Surgical Technique
Distal Scaphoid Excision Technique
- Dorsal radial approach between first and second dorsal compartments
- Or volar-radial approach (FCR sheath)
- Protect superficial radial nerve branches
- Expose STT joint through capsulotomy
- Identify distal scaphoid articular surface
- Excise distal 2-4mm with oscillating saw or osteotome
- Remove all osteophytes
- Preserve scapholunate ligament attachment proximally
- Interposition arthroplasty with FCR tendon slip or capsule
- Capsule and skin closure
- Do not over-resect (scaphoid instability risk)
- Remove all arthritic bone to prevent impingement
- Interposition prevents bone-to-bone contact
Radial Styloid Impingement After STT Fusion
STT fusion reliably relieves pain and preserves grip, but it fixes the scaphoid in slight extension - and the surgical and complications sections describe altered radiocarpal loading without naming the specific mechanism that produces radial-sided pain after an otherwise-united fusion.
- The mechanism. Once the scaphoid is fused to the trapezium-trapezoid in extension, it no longer flexes out of the way during radial deviation. The extended distal scaphoid (and the fused trapezium) then abut the radial styloid, producing radial-sided impingement pain on radial deviation - a common cause of persistent pain despite a solid fusion.
- Prevention: prophylactic radial styloidectomy. Many surgeons perform a limited radial styloidectomy (about 3-4mm) at the time of STT fusion to create clearance and prevent styloid-scaphoid/trapezial abutment. Over-resection is avoided because the radioscaphocapitate ligament origin sits on the styloid, and taking too much risks ulnar translation of the carpus.
- When it presents late. If radial-deviation pain develops after a united fusion, image for styloid abutment; a delayed radial styloidectomy is the usual remedy. Distinguish this mechanical impingement from progressive radiocarpal arthritis, which is managed differently (PRC or total wrist fusion).
Q: A patient has radial-sided pain on radial deviation after a solidly united STT fusion - likely cause and prevention? A: Radial styloid impingement. Fusing the scaphoid in extension stops it flexing away during radial deviation, so the distal scaphoid/trapezium abuts the radial styloid. It is prevented by a prophylactic limited radial styloidectomy (about 3-4mm) at the time of fusion and treated late by a delayed styloidectomy - taking care not to over-resect and detach the radioscaphocapitate ligament origin.
How Much Distal Scaphoid to Resect (and the DISI Trade-off)
The exam warning says "do not over-resect the distal scaphoid" and the Garcia-Elias evidence card records a DISI malalignment in most wrists after resection, but the body never quantifies the safe resection or explains why over-resection destabilises the carpus.
- How much. Remove only the arthritic distal pole - about 2-4mm - enough to clear the STT articular surface and osteophytes, leaving the proximal two-thirds of the scaphoid and, critically, its scapholunate ligament attachment intact.
- Why over-resection destabilises. The distal scaphoid is normally buttressed against the trapezium-trapezoid, which resists scaphoid flexion. Resecting the distal pole removes that distal support, so the scaphoid tends to extend/dorsiflex and the proximal row rotates into a DISI (dorsal intercalated segment instability) pattern (see the carpal-instability topic for the general mechanism). Taking too much, or violating the SL attachment, exaggerates this and risks a symptomatic instability.
- Does the DISI matter? In Garcia-Elias's series a DISI pattern appeared in most wrists after distal-pole resection yet caused no further joint deterioration at short-to-medium follow-up, so a mild radiographic DISI is generally accepted. Whether it accelerates radiocarpal arthritis over decades is unresolved - which is why the resection is kept minimal and the SL attachment preserved.
Q: How much distal scaphoid do you excise for STT arthritis, and what is the consequence of taking too much? A: Resect only the arthritic distal pole (about 2-4mm), clearing the STT surface and osteophytes while preserving the proximal two-thirds and the scapholunate ligament attachment. Removing the distal buttress lets the scaphoid extend and the proximal row rotate into a DISI pattern; a mild DISI is common (Garcia-Elias) and usually tolerated without further short-term deterioration, but over-resection or loss of the SL attachment risks a symptomatic instability - so keep the resection minimal.
Complications
Surgical Complications
- Persistent pain (10-15%)
- Scaphoid instability (rare, if over-resected)
- Progressive radiocarpal arthritis (long-term)
- Nonunion (5-15%)
- Hardware prominence/irritation
- Motion loss (10-15 degrees expected)
- Radiocarpal arthritis progression
- Superficial radial nerve injury (dysesthesias, neuroma)
- Wound infection
- Complex regional pain syndrome (less than 2%)
Postoperative Care
Postoperative Protocol
- Thumb spica splint: 2 weeks
- Progressive ROM exercises: 2-6 weeks
- Strengthening: 6 weeks onwards
- Full activity: 6-8 weeks
- Thumb spica cast: 6-8 weeks
- Radiographic fusion assessment at 8-10 weeks
- Progressive ROM after fusion confirmed
- Full activity: 12-14 weeks
Outcomes
Outcome Summary
- Satisfaction
- 80-85%
- Pain Relief
- 80-90%
- Motion
- Preserved
- Satisfaction
- 85-90%
- Pain Relief
- 85-90%
- Motion
- 10-15 degree loss
- Satisfaction
- 80-85%
- Pain Relief
- 80-85%
- Motion
- 50-60% of normal
- Satisfaction
- Greater than 90%
- Pain Relief
- Excellent
- Motion
- None
Functional Recovery:
- Return to work: 85-90% (3-6 months)
- Grip strength: 75-90% of contralateral
- Return to recreational activities: 70-80%
Guidelines, Registries & Global Practice
Global Epidemiology and Evidence Base
- Triscaphe arthritis is the second most common degenerative wrist pattern after SLAC, accounting for ~26% of degenerative wrists in Watson's classic series
- Strong female predominance in primary osteoarthritis; frequently bilateral
- Coexists with thumb basilar (trapeziometacarpal) arthritis in 30-40%, and CPPD (chondrocalcinosis) is a recognised secondary cause
- No randomised trials; recommendations rest on Level IV case series and Level III systematic reviews
- No dedicated society guideline exists for STT arthritis specifically; management follows general degenerative-wrist principles from hand-surgery societies
- Relevance to STT Arthritis
- No STT-specific guideline; endorse staged conservative-then-surgical care and motion-preserving options where feasible
- Relevance to STT Arthritis
- Support core OA principles: activity modification, NSAIDs (oral or topical), judicious intra-articular corticosteroid
- Relevance to STT Arthritis
- Capture large-joint implants, NOT carpal fusions or carpectomy - so STT outcome data come from case series, not registries
Controversies and Areas of Uncertainty
-
Excision versus arthrodesis for isolated Grade I-II disease. No randomised data exist. Distal scaphoid excision preserves motion with faster recovery but induces a DISI carpal malalignment; STT fusion gives stronger, more predictable grip but loses arc and carries a real nonunion risk. Selection remains demand- and surgeon-dependent.
-
Does distal scaphoid excision matter long-term? Garcia-Elias showed a DISI pattern develops in most wrists after distal pole resection, yet without measurable further deterioration at short-to-medium follow-up. Whether this malalignment accelerates radiocarpal arthritis over decades is unresolved, so over-resection is avoided and the proximal scaphoid-SL attachment is preserved.
-
Interposition or not? Both interposition (FCR slip, capsule, allograft) and simple excision are described with broadly comparable outcomes; some series report greater retained motion without interposition. Interposition is not clearly superior.
-
Open versus arthroscopic STT fusion / excision. Arthroscopic techniques may reduce stiffness from extra-articular adhesions but the evidence is small-series and operator-dependent; open surgery remains the default for most surgeons.
-
Role of the diagnostic injection. Universally recommended yet variably predictive - relief confirms the STT joint as a pain source but does not guarantee complete relief after surgery, especially when CMC arthritis coexists.
-
PRC versus four-corner-type salvage for Grade III. When pancarpal disease is present, the choice between proximal row carpectomy and a midcarpal-fusion-based salvage hinges on the integrity of the capitate head and lunate fossa rather than on STT pathology itself.
Key Mnemonics
CACTUSSTT Arthritis Associated Pathology
Hook:Like a CACTUS in the desert (radial/thumb side), these conditions grow together with STT arthritis
The association between STT arthritis and thumb CMC arthritis is particularly important clinically, as both conditions cause radial-sided hand pain and may require concurrent treatment. Careful examination and imaging of both joints is essential to avoid missing combined pathology and incomplete symptom resolution after treating only one joint.
EFPTSurgery by Watson Grade
Hook:Think 'Every Fellow Picks Treatment' - matching the procedure to the grade and patient demand
MCQ Practice Points
Q: What is the triscaphe joint and what conditions predispose to triscaphe arthritis?
A: The triscaphe (STT) joint is the articulation between the scaphoid, trapezium, and trapezoid. Predisposing conditions include: 1) Primary osteoarthritis (most common, often with thumb CMC OA); 2) SLAC wrist Stage I - scapholunate advanced collapse starts at radioscaphoid joint but STT is commonly involved; 3) Scaphoid malunion/nonunion with altered kinematics; 4) Crystal arthropathy (CPPD commonly affects STT); 5) Inflammatory arthritis (RA). Women are more commonly affected. Often bilateral and associated with thumb basilar joint arthritis.
Q: How do you clinically differentiate triscaphe arthritis from other causes of radial wrist pain?
A: STT arthritis: Tenderness distal to radial styloid over the triscaphe joint, pain with axial loading of thumb metacarpal (CMC grind test may be positive), pain with wrist flexion/radial deviation. De Quervain's: Tenderness over 1st dorsal compartment, positive Finkelstein test. Scaphoid pathology: Tenderness in anatomic snuffbox and scaphoid tubercle. CMC arthritis: Grind test positive, tenderness at thumb base. STT arthritis often coexists with CMC arthritis - examine both joints carefully.
Q: What are the imaging findings of triscaphe (STT) arthritis?
A: Radiographs (PA, lateral, scaphoid views): Joint space narrowing at STT articulation, subchondral sclerosis, osteophytes (particularly dorsal). Key radiograph: The STT joint is best seen on PA view with slight ulnar deviation. Look for associated scapholunate widening (SLAC pattern) or thumb CMC OA. CT scan: Better defines extent of arthritis, useful for surgical planning. MRI: Shows synovitis, cartilage loss, bone marrow edema. CPPD (calcium pyrophosphate) often deposits at the scapholunate ligament and STT joint - look for chondrocalcinosis.
Q: What are the surgical options for isolated triscaphe arthritis?
A: Non-operative: Splinting, NSAIDs, corticosteroid injections (diagnostic and therapeutic). Surgical options: 1) Triscaphe (STT) arthrodesis - gold standard for isolated STT OA, fuses scaphoid to trapezium and trapezoid; 2) Distal scaphoid excision - removes distal pole of scaphoid, preserves some motion; 3) Resection arthroplasty with soft tissue interposition. Considerations: STT fusion reduces wrist motion by approximately 20-30% (flexion-extension); if combined with thumb CMC arthritis, may need LRTI or trapeziectomy. Avoid STT fusion if radioscaphoid arthritis present.
Q: What is the relationship between scapholunate ligament injury and triscaphe arthritis?
A: Scapholunate advanced collapse (SLAC) progresses in predictable pattern: Stage I: Radioscaphoid arthritis (radial styloid and scaphoid fossa); Stage II: Entire radioscaphoid joint; Stage III: Capitolunate (midcarpal) arthritis. The STT joint becomes involved due to altered scaphoid kinematics - the scaphoid flexes abnormally, increasing load at STT. In SNAC (scaphoid nonunion advanced collapse), similar pattern occurs. When treating SLAC/SNAC, must address STT involvement. Note: The radiolunate joint is spared in both SLAC and SNAC (important for salvage procedures like scaphoid excision and four-corner fusion).
At a Glance
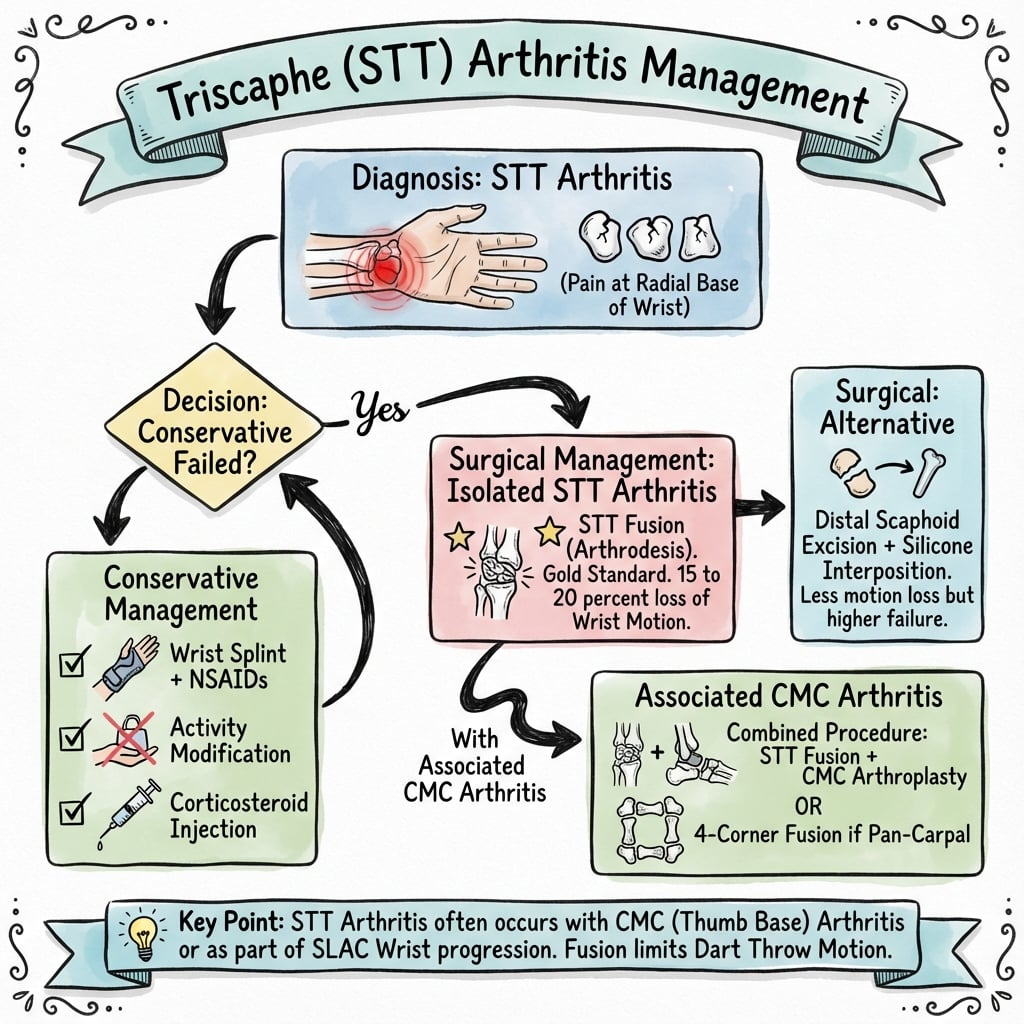
Triscaphe (STT) arthritis affects the scaphotrapeziotrapezoid joint and accounts for 10-15% of degenerative wrist arthritis, presenting with radial-sided wrist pain worse with gripping and wrist extension. It commonly coexists with thumb CMC arthritis (30-40% of cases) and may be associated with scapholunate dissociation. Clinical examination reveals tenderness 1cm distal and radial to the radial styloid, with pain on resisted wrist extension. Conservative management includes activity modification and corticosteroid injection (50-60% temporary relief), while surgical options include distal scaphoid excision for isolated STT, STT fusion for high-demand patients, or proximal row carpectomy for pancarpal involvement.
During wrist motion, the scaphoid rotates about its waist, with the distal pole moving relative to the trapezium and trapezoid. With wrist extension and radial deviation, the STT joint experiences maximum compressive loading. Gripping activities that involve wrist extension substantially increase STT joint reactive forces. These biomechanical factors explain why activities such as push-ups, lifting, and forceful gripping exacerbate symptoms in STT arthritis.
Degenerative Cascade
The pathologic process in STT arthritis follows the typical osteoarthritis cascade. Initial cartilage fibrillation and surface irregularity progress to cartilage loss with exposure of subchondral bone. Attempted healing responses include subchondral sclerosis, marginal osteophyte formation, and synovial inflammation. In advanced cases, complete cartilage loss occurs with bone-on-bone articulation, cyst formation, and deformity. Loose bodies may develop from osteophyte fragmentation.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old office worker presents with radial wrist pain for 18 months, worse with typing and lifting. Examination reveals tenderness directly over the STT joint and pain with resisted wrist extension. Radiographs show Grade II STT arthritis with preserved radiocarpal and midcarpal joints. She has tried NSAIDs and activity modification with minimal benefit. How would you manage this patient?”
“A 58-year-old carpenter with Grade III STT arthritis also shows radioscaphoid joint space narrowing and early capitolunate arthritis on radiographs. He has severe pain limiting his work. What are your treatment options?”
“A 60-year-old woman has radial wrist and thumb-base pain. Radiographs show both STT joint narrowing and trapeziometacarpal arthritis. How do you work out which joint is responsible, and how does that change your operation?”
Definition and Anatomy
- Degenerative arthritis of scaphotrapeziotrapezoid (STT) joint
- Anatomic location: distal scaphoid articulates with trapezium and trapezoid at radial carpus
- Represents 10-15% of degenerative wrist arthritis
- May be isolated or associated with thumb CMC arthritis (30-40%) or scapholunate dissociation
Clinical Presentation
- Radial-sided wrist pain worse with gripping, wrist extension, radial deviation
- Aggravated by push-ups, lifting, keyboard use
- Tenderness over STT joint (1cm distal and radial to radial styloid)
- STT compression test positive (axial load through thumb with wrist radial/ulnar deviation)
- Grip strength reduced 20-40%
Watson Classification
- Grade I: Joint space narrowing, minimal subchondral changes
- Grade II: Advanced STT arthritis with sclerosis and osteophytes, preserved radiocarpal joint
- Grade III: Radiocarpal or midcarpal arthritis also present (pancarpal disease)
- Grade affects surgical treatment selection
Imaging Protocol
- Standard PA, lateral, oblique radiographs
- ESSENTIAL: Carpal tunnel view (skyline) profiles STT joint, shows joint space narrowing and osteophytes
- CT for surgical planning, assesses bone stock and extent
- MRI assesses cartilage and excludes other pathology
- Diagnostic injection confirms STT as pain source
Conservative Management
- First-line for Grade I and mild Grade II
- Activity modification (avoid wrist extension with loading)
- NSAIDs for symptom relief
- Wrist splinting in neutral or slight flexion
- Corticosteroid injection (60-80% temporary relief, diagnostic and therapeutic)
- Surgery if 3-6 months conservative treatment fails
Surgical Treatment Algorithm
- GRADE I-II ISOLATED: Distal scaphoid excision (2-4mm) with interposition arthroplasty (80-85% satisfaction, preserves motion)
- Alternative: STT fusion (young, high-demand, trades 10-15 degree motion for strength)
- GRADE III PANCARPAL: Proximal row carpectomy (if capitate-lunate fossa preserved)
- Alternative: Total wrist arthrodesis (if capitate-lunate fossa arthritic or failed PRC)
Key Complications
- Distal scaphoid excision: Persistent pain (10-15%), scaphoid instability (rare), progressive radiocarpal arthritis
- STT fusion: Nonunion (5-15%), hardware prominence, motion loss (10-15 degrees expected), radiocarpal arthritis
- General: Superficial radial nerve injury, CRPS (less than 2%), wound complications
Viva Talking Points
- Emphasize carpal tunnel view for diagnosis
- Know Watson classification and treatment by grade
- Understand biomechanics (STT loads with extension and radial deviation)
- Distal scaphoid excision for isolated Grade I-II
- STT fusion for high-demand young patients
- PRC for Grade III if capitate-lunate fossa preserved
- Always assess thumb CMC joint (30-40% coexist)
- Diagnostic injection confirms pain source
Evidence Base
Key Evidence
- Watson & Hempton (1980): Original description of STT fusion technique
- Crosby et al (1978): Long-term outcomes of distal scaphoid excision
- Evidence level predominantly Level IV (case series)
- Conservative management provides 50-60% temporary relief
- Distal scaphoid excision: 80-85% satisfaction at 5-10 years
- STT fusion: 85-95% fusion rate with rigid fixation
- PRC: Reliable salvage with 50-60% motion preservation
Additional Resources and Further Reading
The literature on STT arthritis treatment demonstrates that surgical outcomes are generally favorable for appropriately selected patients. Distal scaphoid excision and STT arthrodesis are both well-supported for isolated STT arthritis - excision preserving motion and arthrodesis maximising grip in higher-demand patients - while proximal row carpectomy serves as an excellent salvage for pancarpal arthritis when the capitate head and lunate fossa are preserved. Hand therapy is integral to both conservative and postoperative care, and any coexisting thumb carpometacarpal arthritis should be assessed and treated on its own merits to avoid incomplete symptom relief.
This topic provides comprehensive coverage of triscaphe (STT) arthritis aligned with FRACS examination requirements, emphasizing clinical diagnosis, radiographic assessment, and evidence-based surgical treatment options tailored to disease severity and patient functional demands.