Real-Time Dynamic Soft Tissue Assessment
Hyperechoic (bright): Fat, fibrous tissue, cortical bone surface, tendons (perpendicular beam)
Isoechoic (grey): Muscle at rest, peripheral nerves
Hypoechoic (dark): Fluid-filled structures (bursae), cartilage, some tumours
Anechoic (black): Simple fluid (effusion, cyst), blood vessels
Key: The echogenicity of a structure depends on its acoustic impedance relative to surrounding tissues — large impedance differences create strong reflections
- Ultrasound uses high-frequency sound waves (no ionising radiation) reflected by tissue interfaces to create real-time images.
- Higher frequency (12-18MHz) gives better resolution but less penetration. Lower frequency (5-8MHz) penetrates deeper but with lower resolution.
- Ultrasound is the only modality offering dynamic, real-time assessment — invaluable for impingement testing, snapping tendons, and subluxation.
- Ultrasound sensitivity for full-thickness rotator cuff tears (89-95%) approaches MRI, but is operator-dependent.
- Ultrasound-guided injections improve accuracy from approximately 50-70% (blind) to over 90% for most targets.
- “A linear transducer (12-18MHz) is used for superficial structures (tendons, ligaments, nerves). A curvilinear transducer (5-8MHz) is used for deeper structures (hip joint, spine).
- “Tendons appear hyperechoic (bright) and FIBRILLAR on long axis. Loss of this fibrillar pattern indicates pathology.
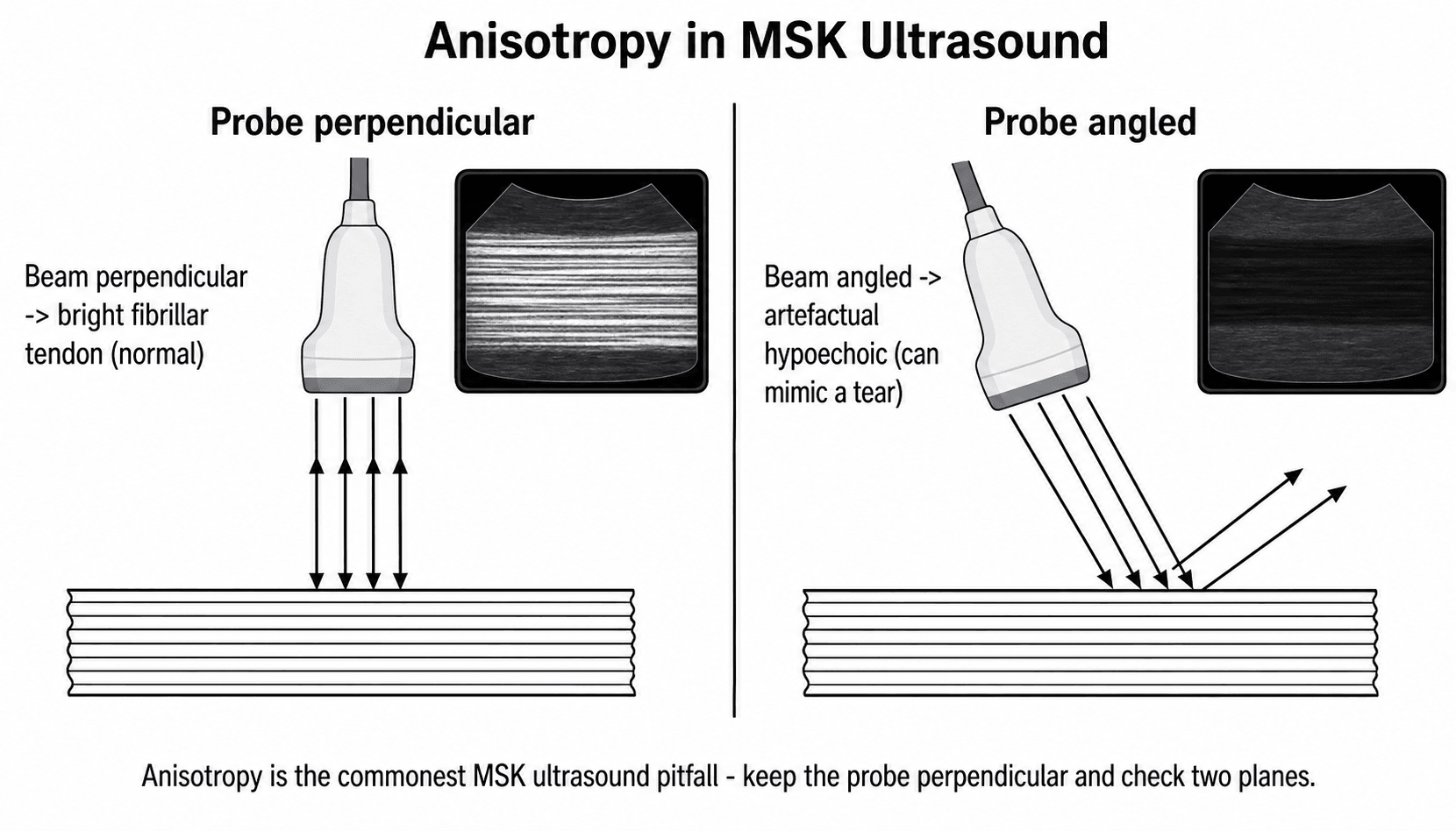
- “Anisotropy artefact: tendons appear falsely dark when the ultrasound beam is not perpendicular — the most common pitfall in MSK ultrasound.
- “Power Doppler detects neovascularisation in tendinopathy — increased Doppler signal correlates with active disease.
- “Ultrasound cannot penetrate cortical bone — it sees the bone surface only, not internal bone pathology.
Musculoskeletal ultrasound is examined in both clinical and viva settings. You must understand: the physics of ultrasound (frequency-resolution-penetration trade-off), transducer selection, anisotropy artefact, the appearance of normal tendons (fibrillar, hyperechoic), rotator cuff examination technique, and the advantages of ultrasound-guided interventions. A common viva trap is not mentioning the operator-dependent nature of ultrasound as a limitation.
ANGLEAnisotropy Artefact
Hook:ANGLE: the most common pitfall in MSK ultrasound. Always keep the beam perpendicular to the tendon.
Overview
Musculoskeletal (MSK) ultrasound has evolved from a niche technique to an essential tool in modern orthopaedic and sports medicine practice. Unlike other imaging modalities, ultrasound provides real-time, dynamic imaging that allows the examiner to visualise structures during movement, provoke pathology with dynamic tests, and guide diagnostic and therapeutic interventions — all without ionising radiation and at the point of care.
The key advantages of ultrasound over MRI include: real-time dynamic assessment, portability, lower cost, absence of contraindications (no magnetic field, no contrast usually required), and the ability to guide interventional procedures. The key disadvantages are: operator dependence (the single greatest limitation), inability to image through bone, limited field of view, and inability to assess bone marrow or deep intra-articular structures.
Dynamic assessment of tendon subluxation or impingement. Guided injections and aspirations. Rotator cuff assessment (comparable to MRI in experienced hands). Evaluation of superficial soft tissue masses. Assessment of neonatal hip (DDH screening). Foreign body localisation. Evaluation of muscle injuries (haematoma, tears) with dynamic contraction. Monitoring of tendon healing.
Bone marrow pathology (oedema, AVN, tumour). Intra-articular structures (menisci, labrum, cruciate ligaments). Deep structures behind bone. Comprehensive joint assessment (ultrasound cannot see all areas). Preoperative tumour staging. Spinal cord and nerve root assessment. When a permanent, reviewer-independent dataset is required.
Systematic Approach
Systematic MSK Ultrasound Examination
- Assessment
- Choose appropriate probe for depth and resolution requirements
- Key Principles
- Linear 12-18MHz for superficial (tendons, nerves). Curvilinear 5-8MHz for deep (hip joint, deep muscles)
- Assessment
- Follow established scanning protocols for the region
- Key Principles
- Always scan in BOTH long axis and short axis. Use the contralateral side for comparison
- Assessment
- Evaluate echogenicity, echotexture, size, vascularity (Doppler)
- Key Principles
- Compare findings to the normal contralateral side. Document measurements
- Assessment
- Perform specific dynamic tests for the region
- Key Principles
- Movement during scanning reveals snapping, subluxation, impingement that are invisible on static imaging
- Assessment
- Apply colour and power Doppler to assess vascularity
- Key Principles
- Increased Doppler signal indicates active inflammation, neovascularisation, or tumour vascularity
- Assessment
- Scan the contralateral side for comparison when findings are equivocal
- Key Principles
- Bilateral scanning helps distinguish normal variants from pathology and quantifies asymmetry
Ultrasound Physics
Sound Wave Principles
Ultrasound uses sound waves with frequencies above the audible range (more than 20kHz). In MSK imaging, frequencies of 5-18MHz are standard. These high-frequency waves are generated by piezoelectric crystals in the transducer, transmitted into tissue, reflected at tissue interfaces, and received by the same transducer to construct the image.
Key relationships:
- Frequency and resolution: Higher frequency gives better axial resolution (ability to distinguish structures along the beam axis). At 15MHz, axial resolution is approximately 0.1mm.
- Frequency and penetration: Higher frequency waves are absorbed more rapidly by tissue, limiting depth of penetration. At 15MHz, useful penetration is approximately 3-4cm. At 5MHz, penetration reaches 15-20cm.
- This trade-off is the fundamental physics concept: you cannot have both maximum resolution and maximum depth simultaneously.
Acoustic impedance: Each tissue has a characteristic acoustic impedance (Z = density × speed of sound). Ultrasound waves are reflected at interfaces between tissues with different impedances. The greater the impedance mismatch, the stronger the reflection — this is why cortical bone (very high impedance) produces an extremely bright surface reflection.
Coupling gel: Air has very different acoustic impedance from tissue. Without gel, nearly all ultrasound energy is reflected at the skin-air interface. Coupling gel eliminates this interface, allowing sound to enter the tissue efficiently.
RAPIDUltrasound Advantages
Hook:RAPID sums up why ultrasound is becoming indispensable in modern orthopaedic practice.
BONEUltrasound Limitations
Hook:BONE: ultrasound cannot see through Bone, is Operator-dependent, has No complete record, and requires Experience.
Differential Diagnosis & Controversies
Hypoechoic Tendon: Differential Diagnosis
A focal dark (hypoechoic) area within a tendon is one of the commonest decision points in MSK ultrasound. Distinguishing artefact from true pathology, and grading true pathology, is examined frequently.
- Echotexture & Behaviour
- Falsely dark area, tendon thickness normal
- Doppler / Dynamic
- No Doppler signal; resolves on tilting
- Key Discriminator
- Disappears when beam made perpendicular — NOT seen on both axes
- Echotexture & Behaviour
- Thickened tendon, disrupted fibrillar pattern, surfaces intact
- Doppler / Dynamic
- Neovascular power Doppler signal often present
- Key Discriminator
- Persists on tilting; visible on both long and short axis
- Echotexture & Behaviour
- Focal anechoic/hypoechoic defect reaching one surface only
- Doppler / Dynamic
- Variable; may track fluid
- Key Discriminator
- Defect involves bursal OR articular surface but not full depth
- Echotexture & Behaviour
- Defect through entire tendon; deltoid may abut humeral head
- Doppler / Dynamic
- Fluid may fill the gap
- Key Discriminator
- Naked tuberosity sign; tendon retraction
- Echotexture & Behaviour
- Hypoechoic or iso-echoic focus, may lack shadow
- Doppler / Dynamic
- No internal Doppler
- Key Discriminator
- Often shadows when dense; clinical calcific tendinitis
Areas of Uncertainty & Controversy
Ultrasound guidance clearly improves needle-placement accuracy for deep targets, but whether this translates into better patient-reported pain and function is target-dependent and still debated. For the relatively superficial subacromial space, randomised data show little or no outcome advantage over landmark injection, and some benefit of corticosteroid may be systemic rather than local.
Countries using the Graf method universally (e.g. Austria, Germany) report fewer late-presenting dislocations but treat more physiologically immature hips. Selective/risk-based screening (UK, US, Australasia) reduces overtreatment but risks late diagnosis. No global consensus exists; cost-effectiveness drives policy.
Neovascular Doppler signal correlates with symptomatic tendinopathy, but its prognostic value and whether targeting neovessels (e.g. with sclerosant or high-volume injection) improves outcomes remains uncertain.
Published accuracy reflects expert centres and may not generalise. Standardised protocols, accreditation, and emerging deep-learning assistance aim to narrow this gap, but AI tools are not yet validated for routine independent reporting.
Clinical Applications

Rotator Cuff Ultrasound
Ultrasound is the primary imaging modality for rotator cuff assessment in many centres, with sensitivity comparable to MRI for full-thickness tears (89-95%) in experienced hands.
Standard shoulder ultrasound protocol:
- Biceps tendon (long head): Transverse and longitudinal views in the bicipital groove. Assess for tenosynovitis (fluid around the tendon), subluxation, dislocation, and tears.
- Subscapularis: Internal rotation brings the tendon to the anterior scanning window. Assess for partial and full-thickness tears. Dynamic assessment with external rotation demonstrates the tendon rolling over the lesser tuberosity.
- Supraspinatus: Modified Crass position (hand on back pocket). Long axis and short axis assessment. Full-thickness tears show a defect through the entire tendon. Partial-thickness tears appear as focal hypoechoic or anechoic areas.
- Infraspinatus/Teres minor: External rotation with the arm adducted. Less commonly torn but assessed as part of the complete protocol.
- AC joint: Superior assessment for osteophytes, effusion, and instability.
Dynamic assessment: Impingement testing under real-time ultrasound allows direct visualisation of subacromial bursal thickening and cuff compression during abduction — this is unique to ultrasound and impossible with MRI.
Guidelines, Registries & Global Practice
Musculoskeletal ultrasound is performed worldwide by radiologists, sonographers, sports and rehabilitation physicians, rheumatologists, and increasingly by orthopaedic surgeons and emergency physicians. Reflecting its operator-dependence, every major society anchors practice in accreditation, standardised protocols, and supervised training rather than in any single national pathway.
- Focus
- Technical standards
- Key Position
- Publishes anatomy-specific scanning protocols and graded clinical-indication recommendations; ultrasound first-line for many tendon, nerve and superficial soft-tissue problems
- Focus
- Inflammatory disease & training
- Key Position
- Endorses ultrasound (greyscale plus power Doppler) for synovitis, enthesitis and guided injection; defines structured competency and certification
- Focus
- Practice parameters
- Key Position
- Joint practice parameters for the performance of MSK and interventional ultrasound; accreditation of laboratories and personnel
- Focus
- Accreditation & scope
- Key Position
- Define sonographer/practitioner competence and supervised logbooks; support extended scope MSK ultrasound
- Focus
- Point-of-care use
- Key Position
- Recognise POCUS as an adjunct for fracture detection and reduction monitoring, especially paediatric and resource-limited settings
Global epidemiology and access. MSK ultrasound use has grown faster than any other imaging modality in many health systems because it is inexpensive, portable and radiation-free. There is no implant registry for ultrasound itself; the closest equivalent is national DDH screening data. Approaches diverge: several countries (e.g. Austria, Germany — the home of the Graf method) operate universal newborn hip ultrasound screening, whereas the UK, US and Australasia use selective/targeted screening based on risk factors (breech presentation, family history, clinical instability). The debate centres on cost-effectiveness and overtreatment of physiologically immature hips versus missed late-presenting dysplasia.
High- vs limited-resource practice. In well-resourced centres ultrasound complements MRI and CT and underpins almost all image-guided joint and periarticular injection. In limited-resource and remote settings, portable and handheld ultrasound is often the only available cross-sectional imaging — used for fracture triage, effusion detection, foreign-body localisation, abscess drainage and guided aspiration. The principal global limiting factor is not equipment cost but trained operators, which is why every society pairs guidance with structured accreditation.

Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner asks you about the role of ultrasound in assessing rotator cuff tears, including the advantages and limitations compared to MRI.”
“You are performing an ultrasound of the supraspinatus tendon and notice a dark area in the tendon on the long-axis view.”
“You are asked to perform an ultrasound-guided aspiration and injection of a large knee effusion. Describe your technique and the principles of ultrasound-guided intervention.”
Physics Basics
- Higher frequency = better resolution but less penetration
- 12-18MHz (linear) for superficial structures; 5-8MHz (curvilinear) for deep
- Acoustic impedance differences create reflections — basis of image formation
- Coupling gel eliminates air interface that blocks sound transmission
Advantages (RAPID)
- Real-time dynamic imaging (impingement, subluxation, snapping)
- Accessible, portable — clinic, bedside, theatre
- Procedure guidance (injections more than 90% accurate)
- Inexpensive, no radiation, no contraindications
- Doppler for vascularity (neovascularisation, synovitis)
Key Artefacts
- Anisotropy: tendon appears falsely dark when beam not perpendicular (MOST COMMON pitfall)
- Acoustic shadowing: behind bone, calcification (blocks deeper structures)
- Posterior enhancement: bright signal behind fluid-filled structures (confirms fluid)
- Always tilt probe to check for anisotropy before diagnosing pathology
Rotator Cuff Ultrasound
- Sensitivity 89-95% for full-thickness tears (comparable to MRI)
- Modified Crass position for supraspinatus (hand on back pocket)
- Dynamic impingement testing is unique to ultrasound
- LIMITATION: operator-dependent, cannot assess labrum or fatty infiltration
DDH (Graf Classification)
- Type I: Normal, alpha greater than 60 degrees
- Type II: Immature/Dysplastic, alpha 50-60 degrees
- Type III: Subluxated, alpha less than 43 degrees
- Type IV: Dislocated — labrum displaced inferiorly
Evidence Base
Ultrasound vs MRI vs MR Arthrography for Rotator Cuff Tears
- Pooled analysis of 65 studies using a surgical reference standard (open or arthroscopic).
- No significant difference in sensitivity or specificity between ultrasound and MRI for partial- or full-thickness tears (p greater than 0.05).
- Area under the summary ROC curve: MR arthrography 0.935, ultrasound 0.889, MRI 0.878 — MR arthrography most accurate; ultrasound and MRI comparable.
Ultrasound-Guided vs Landmark-Guided Shoulder Injections
- Systematic review and meta-analysis of 4 cadaveric studies (300 shoulders) and 9 human studies (514 patients).
- Ultrasound-guided injection was significantly more accurate for the AC joint (93.6% vs 68.2%), glenohumeral joint (92.5% vs 72.5%) and biceps tendon sheath (86.7% vs 26.7%).
- For the subacromial space accuracy was similar (65% vs 70%, not significant), but ultrasound guidance improved pain and function at 6 weeks.
Strong evidence supports ultrasound for rotator cuff assessment and guided interventions.