Benign Vascular Lesion of Bone | Usually Incidental | Polka-Dot and Corduroy Signs
- Most common benign tumour of the spine but the vast majority are incidental and need no treatment
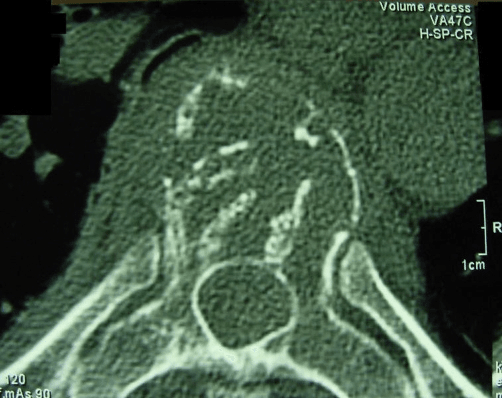
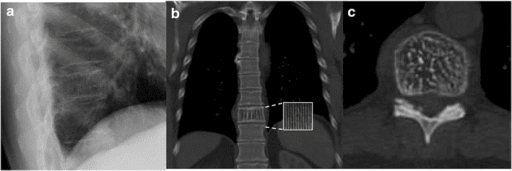
- Polka-dot sign on axial CT and corduroy / jail-bar sign on sagittal views are pathognomonic
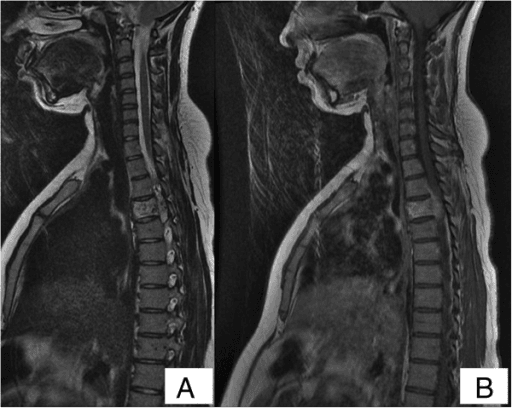
- Fatty (high T1, high T2) lesions are quiescent; low T1 signal flags a more aggressive, vascular lesion
- Aggressive vertebral haemangioma can cause spinal cord compression and a progressive neurological deficit
- Preoperative embolisation is critical before surgery because these are highly vascular and bleed heavily
- “An incidental vertebral haemangioma on MRI needs reassurance, not a biopsy
- “Low T1 signal (replacement of fat by vascular stroma) is the imaging clue to an aggressive lesion
- “Pregnancy can unmask or worsen a haemangioma through venous engorgement and hormonal effect
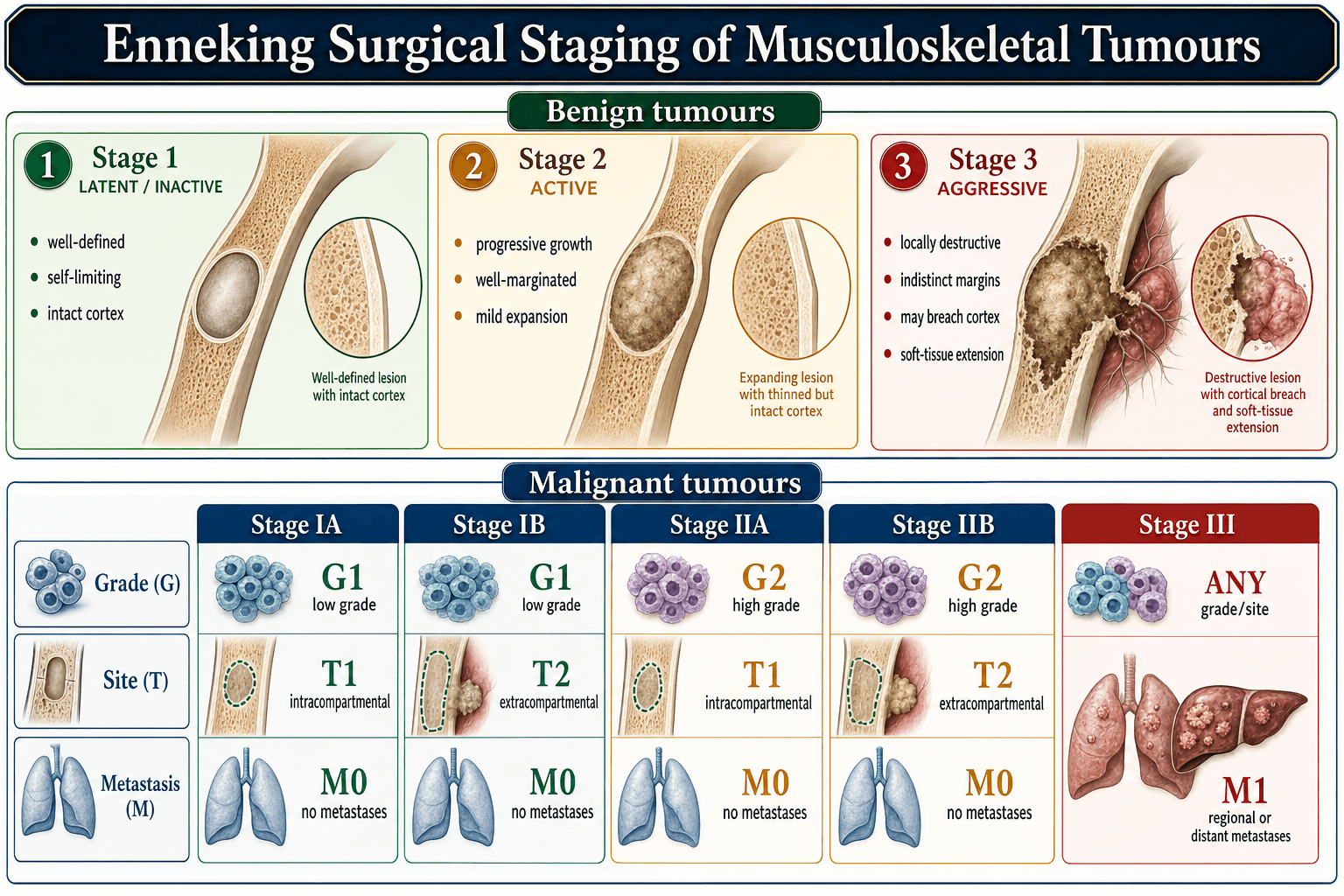
- “Staging uses the Enneking benign system (S1-S3) and the WBB / SINS scores for surgical planning
The vast majority are asymptomatic and found by chance on imaging done for another reason. The exam trap is to over-investigate or biopsy a classic incidental lesion. Recognise the imaging signs and reassure.
Polka-dot sign on axial CT (trabeculae end-on) and corduroy / jail-bar sign on sagittal CT or radiograph (trabeculae lengthwise) are diagnostic. They reflect thickened residual trabeculae among the vascular tissue and fat.
Low T1 signal, soft-tissue / epidural extension, and a progressive neurological deficit define an aggressive lesion. Fat content is low because vascular stroma has replaced marrow fat. These lesions may need surgery.
Vertebral haemangiomas are highly vascular. Preoperative transarterial embolisation reduces catastrophic intraoperative blood loss and is a near-universal step before resection of an aggressive lesion.
Overview and Epidemiology
Vertebral haemangioma is a benign vascular lesion of bone made up of thin-walled blood vessels and fat sitting between thickened residual bony trabeculae. It is the most common benign tumour of the spine, yet it is overwhelmingly silent: it is usually discovered by accident on imaging performed for unrelated back pain or trauma. Only a tiny fraction ever produce symptoms, and an even smaller fraction behave aggressively enough to threaten the spinal cord.
For the exam, the single most useful concept is the spectrum. At one end is the typical fatty incidental lesion that needs nothing more than recognition and reassurance. At the other end is the aggressive lesion with epidural extension and cord compression that needs a coordinated vascular and surgical plan. Everything else, including the painful but neurologically intact lesion, sits in between.
- Prevalence: present in roughly 10-12% of adults at autopsy
- Symptomatic disease: under 1% of all vertebral haemangiomas
- Age: typically detected in the 4th to 6th decades
- Sex: aggressive symptomatic lesions show a female predominance
- Thoracic spine: most common site for symptomatic and aggressive lesions
- Lumbar spine: common, often the painful (non-aggressive) type
- Cervical spine: less common but can cause early myelopathy
- Multiplicity: lesions are frequently multiple within the spine
Why Most Are Harmless
The behaviour of a vertebral haemangioma tracks its tissue make-up. A lesion rich in fat with widely spaced trabeculae is metabolically quiet and mechanically stable, which is why the typical incidental lesion never declares itself. When vascular stroma replaces that fat, the lesion becomes more cellular, more vascular and more prone to expand, erode cortex and push into the spinal canal. This is the basis for the imaging distinction between quiescent (fatty, high T1) and aggressive (low T1) lesions.
Common lesion, rare problem. The skill being tested is not how to operate on every haemangioma; it is knowing which lesion to leave alone, which to treat for pain, and which to take to theatre for cord compression.
Pathophysiology and Pathology
A soft, reddish-brown, blood-filled lesion within cancellous bone. The vertebral body shows coarse vertical trabeculae that have thickened in compensation for the loss of horizontal trabeculae replaced by vascular tissue. This is the structural basis of the corduroy and polka-dot signs.
Thin-walled, dilated capillary and cavernous vascular channels lined by a single layer of bland endothelium, interspersed with mature adipose tissue and the thickened bony trabeculae. There is no cellular atypia and no mitotic activity; this is a benign vascular proliferation, not a malignant tumour.
From Quiescent To Aggressive
Predominant adipose tissue and slow-flow vessels, sparse trabeculae. High T1 and high T2 signal on MRI. Mechanically stable and asymptomatic.
More vascular stroma, less fat. Lower T1 signal. May cause mechanical back pain and is the typical target for vertebroplasty.
Vascular stroma dominates, cortical expansion and erosion, soft-tissue or epidural extension. Low T1 with avid enhancement. May compress the cord and cause neurological deficit.
Drivers Of Aggression
The change from a quiet lesion to an aggressive one is associated with increased vascular stroma at the expense of fat, expansion beyond the vertebral body, and sometimes a physiological trigger. Pregnancy is a recognised trigger: increased circulating blood volume, venous engorgement of the epidural plexus, and hormonal softening of vessel walls can unmask or worsen a previously silent lesion, sometimes producing rapid deficit in the third trimester.
A pregnant patient who develops a progressive lower-limb neurological deficit and back pain may have an aggressive vertebral haemangioma. Increased epidural venous engorgement and hormonal change can decompensate a previously silent lesion. This is a high-yield viva scenario and demands urgent multidisciplinary imaging and management.
Classification and Staging
The most practical day-to-day classification separates lesions by their clinical behaviour, because this drives management.
- Symptoms
- None
- Imaging
- Fatty, high T1 and T2, polka-dot CT
- Typical Management
- Observe and reassure
- Symptoms
- Mechanical back pain, no deficit
- Imaging
- Lower fat, no epidural extension
- Typical Management
- Vertebroplasty or radiotherapy
- Symptoms
- Deficit, cord or root compression
- Imaging
- Low T1, epidural extension, expansion
- Typical Management
- Embolisation plus surgery
If asked how you would stage a spinal haemangioma, name three tools and say what each adds: Enneking benign (S1-S3) for biological activity, WBB for the anatomical zone map that decides resectability, and SINS for mechanical instability. This structured answer scores well.
Clinical Presentation
- Asymptomatic: discovered incidentally on imaging
- No tenderness, no deficit, normal examination
- Reported as an aside on a scan for unrelated back pain or trauma
- Localised back pain: mechanical, often the only symptom
- Radiculopathy: nerve root irritation from expansion
- Myelopathy: gait disturbance, weakness, sphincter change
- Acute deficit: rare, from haemorrhage or rapid expansion
Typical Presentations
No symptoms. The lesion is reported on MRI or CT done for another reason. The task is recognition and reassurance, not work-up.
Persistent, mechanical pain localised to the affected level, without neurological signs. Other causes of back pain must be excluded before attributing pain to the lesion.
Gradual onset of leg weakness, gait imbalance, sensory level and bladder or bowel change from cord compression by epidural extension. A neurosurgical and oncological emergency when progressive.
Rapid neurological deterioration in the later stages of pregnancy from a previously silent lesion, driven by venous engorgement and hormonal change.
Treat a vertebral haemangioma as potentially aggressive when:
- Pain is progressive rather than mechanical and intermittent
- There are any neurological signs (weakness, sensory level, sphincter change)
- Imaging shows low T1 signal, cortical expansion or epidural extension
- Symptoms appear or worsen during pregnancy
Do NOT attribute a neurological deficit to an incidental fatty haemangioma without first excluding a more aggressive component or a separate pathology.
Investigations and Imaging
Imaging makes the diagnosis. The combination of CT and MRI is usually conclusive and a biopsy is rarely needed for a classic lesion.
Imaging Modalities
Coarse vertical striations within the vertebral body, the corduroy or jail-bar sign. Many lesions are invisible on plain films until they are large.
Axial slices show the polka-dot sign, thickened trabeculae seen end-on as discrete dots. CT also defines cortical integrity, expansion and any posterior-element involvement for surgical planning.
Defines fat content (signal) and, crucially, epidural extension and cord compression. High T1 and high T2 signal indicates a fatty, quiescent lesion; low T1 signal indicates an aggressive, vascular lesion.
Maps the feeding vessels and allows preoperative embolisation to reduce intraoperative blood loss.
- Quiescent (typical)
- High (fatty)
- Aggressive
- Low (fat replaced by stroma)
- Quiescent (typical)
- High
- Aggressive
- High, often heterogeneous
- Quiescent (typical)
- Mild
- Aggressive
- Avid
- Quiescent (typical)
- Confined to body
- Aggressive
- Epidural or paravertebral extension
The most useful single MRI discriminator is T1 signal. A bright (fatty) T1 lesion is almost always a quiescent, leave-alone haemangioma. A T1-dark lesion has lost its fat to vascular stroma and is the one that may be aggressive and may need treatment.
Biopsy Principles
A classic fatty incidental lesion does not need a biopsy - the imaging is diagnostic. Biopsy is reserved for atypical or aggressive lesions where the differential includes a more sinister pathology such as metastasis, myeloma or another primary tumour.
Because these lesions are highly vascular, percutaneous biopsy can bleed. Biopsy of a spinal column tumour should follow oncological principles: planned by the treating surgeon, along a tract that can be excised at definitive surgery, and ideally in a unit able to manage haemorrhage.
Never treat a spinal haemangioma like a routine soft-tissue mass. The vascular nature means an ill-planned biopsy can cause significant bleeding and an ill-placed tract can compromise a future en bloc resection. When in doubt, refer to a specialist spinal oncology unit before any tissue is taken.
Differential Diagnosis
The classic fatty lesion is unmistakable, but the atypical (low-fat) haemangioma is the one that causes diagnostic difficulty because, like a metastasis, it is T1-hypointense. The single most useful discriminator is the trabecular pattern on CT: a haemangioma THICKENS and preserves residual vertical trabeculae (the polka-dot/corduroy pattern), whereas a metastasis DESTROYS trabeculae and is lytic (or sclerotic) without that pattern.
- Discriminating features
- T1-dark like a metastasis, BUT retains thickened vertical trabeculae (polka-dot/corduroy) on CT and often some intralesional fat; no cortical destruction or soft-tissue mass when non-aggressive
- Key clue
- CT trabecular pattern is preserved/coarsened
- Discriminating features
- T1-dark marrow replacement that DESTROYS trabeculae; lytic or sclerotic without a polka-dot pattern; may have a paravertebral/epidural soft-tissue mass, pedicle destruction and cortical breach; usually hot on bone scan
- Key clue
- Trabeculae destroyed, pedicle involved, known primary
- Discriminating features
- T1-bright and T2-bright like a quiescent haemangioma, BUT NO thickened trabeculae and NO polka-dot; suppresses on fat-saturated sequences and drops on opposed-phase (chemical-shift) imaging
- Key clue
- No trabecular thickening; drops with fat suppression
- Discriminating features
- Enlarged vertebral body with cortical thickening ("picture-frame" vertebra) and coarse trabeculae, or a sclerotic "ivory" vertebra; trabecular coarsening is generalised rather than the fine vertical striations of corduroy
- Key clue
- Bony enlargement + picture-frame cortex
- Discriminating features
- Marrow-replacing, T1-dark, often with a soft-tissue component and trabecular/cortical destruction; lack the polka-dot pattern; myeloma classically lytic with low osteoblastic activity
- Key clue
- Marrow replacement, no polka-dot, clinical/serology
Bone scintigraphy helps when the picture is equivocal: most haemangiomas show only normal or mildly increased uptake (and may be photopenic), whereas most metastases are markedly hot — though an aggressive haemangioma can itself be active, so a positive scan does not exclude it. When doubt remains after CT and MRI (particularly for a T1-dark, atypical or aggressive-looking lesion in a patient with a known or suspected primary), the issue is settled by image-guided biopsy along an excisable tract in a specialist unit (see Biopsy Principles above) rather than by imaging alone.
Answer in one line: the CT trabecular pattern. A haemangioma thickens and preserves the vertical trabeculae (polka-dot end-on, corduroy lengthwise) and often retains some fat; a metastasis destroys trabeculae, is lytic or sclerotic without that pattern, frequently involves the pedicle and may have a soft-tissue mass. If still uncertain on CT and MRI, biopsy.
Management Algorithm
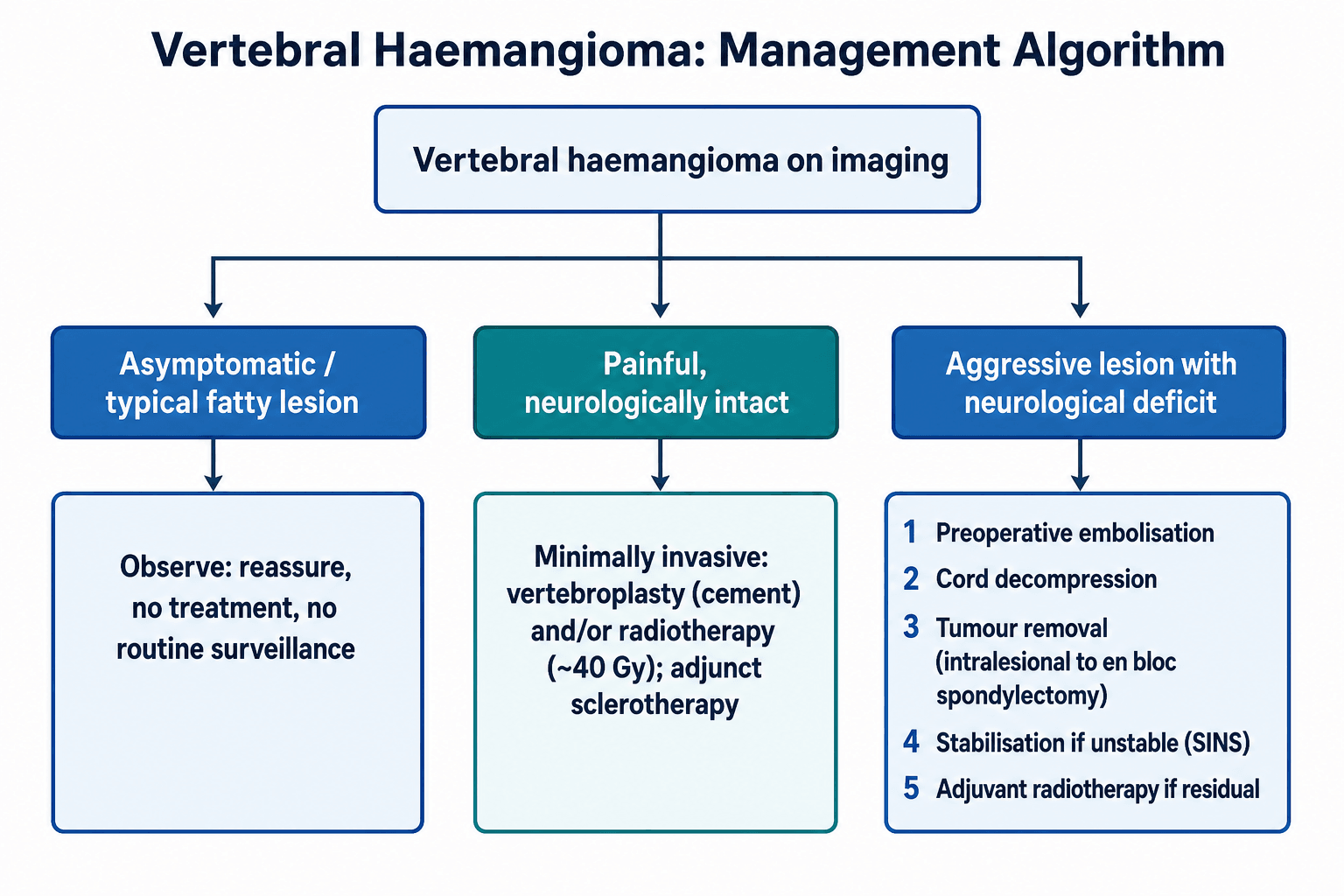
Observation (the default)
The typical incidental fatty lesion needs no treatment. The correct action is to recognise it, document it, and reassure the patient. Routine surveillance imaging of a classic asymptomatic lesion is generally unnecessary. The clinical skill is restraint: not biopsying, not irradiating and not operating on a lesion that is doing no harm.
- Best For
- Incidental fatty lesion
- Key Advantage
- No morbidity, correct default
- Key Caution
- Must be confident of diagnosis
- Best For
- Painful lesion, selected aggressive
- Key Advantage
- Rapid pain relief, stabilises body
- Key Caution
- Cement leak, limited for cord disease alone
- Best For
- Painful lesion, residual disease
- Key Advantage
- Durable pain control, re-ossification
- Key Caution
- Slow onset, not for acute cord compression
- Best For
- Aggressive lesion with deficit
- Key Advantage
- Decompresses cord, treats instability
- Key Caution
- Highly vascular, major operation
There is no single correct operation. Reported series show that decompression with vertebroplasty and intralesional resection can give good neurological recovery with low recurrence, while total en bloc spondylectomy gives excellent local control but carries higher morbidity. Match the aggressiveness of the operation to the aggressiveness of the lesion and the patient's fitness.
Complications and Prognosis
- Complication
- Progressive cord compression and deficit
- Mitigation
- Timely imaging and referral
- Complication
- Cement leak, rarely into the canal
- Mitigation
- Image guidance, controlled injection
- Complication
- Massive haemorrhage
- Mitigation
- Preoperative embolisation, cell salvage
- Complication
- Recurrence after subtotal resection
- Mitigation
- Adjuvant radiotherapy, surveillance
Outlook
The prognosis is excellent. The typical incidental lesion never causes a problem. Even in the aggressive group, modern series report that neurological function improves in the great majority of patients after treatment, with low recurrence rates when the blood supply is controlled and the cord is adequately decompressed. Malignant transformation does not occur; a vertebral haemangioma is and remains a benign lesion.
A vertebral haemangioma is a benign lesion with an excellent prognosis. The two ways patients come to harm are an untreated aggressive lesion that compresses the cord and an avoidable complication of over-treatment (unnecessary biopsy or surgery on an incidental lesion). Good judgement avoids both.
Guidelines, Registries and Global Practice
- Widely Accepted Position
- Imaging is diagnostic for classic lesions
- Practical Implication
- Biopsy reserved for atypical or aggressive lesions
- Widely Accepted Position
- T1 signal separates fatty from vascular lesions
- Practical Implication
- Low T1 prompts closer evaluation
- Widely Accepted Position
- Enneking, WBB and SINS used together
- Practical Implication
- Structured planning of resection and stabilisation
- Common Global Practice
- Observation without surveillance imaging
- Variation And Reason
- Some centres image once to confirm stability
- Common Global Practice
- Vertebroplasty or radiotherapy
- Variation And Reason
- Choice depends on local expertise and resources
- Common Global Practice
- Embolisation then decompression and stabilisation
- Variation And Reason
- Extent of resection ranges from intralesional to en bloc by lesion and unit
There is no large randomised evidence base for vertebral haemangioma because symptomatic disease is rare; practice is therefore guided by retrospective series and the principles of benign spinal tumour surgery. Across high- and lower-resource settings the constant themes are recognition of the classic imaging signs, restraint with incidental lesions, embolisation before any major resection, and matching the intensity of treatment to the behaviour of the lesion. Resource-rich units may have ready access to en bloc spondylectomy and interventional radiology, while in other settings decompression with vertebroplasty and radiotherapy are pragmatic and effective alternatives.
MCQ Practice Points
At a Glance
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An MRI reported for low back pain incidentally shows a T1-bright, T2-bright lesion in an L2 vertebral body with a polka-dot pattern on the accompanying CT. The patient has no neurological signs. What is it and what would you do?”
“A 30-year-old woman in the third trimester of pregnancy develops progressive weakness of both legs and a sensory level. MRI shows a thoracic vertebral lesion with epidural extension compressing the cord. How do you approach this?”
“What staging and assessment tools would you use to plan surgery for an aggressive vertebral haemangioma, and what does each contribute?”
Key Facts
- Most common benign tumour of the spine; vascular lesion of bone
- Present in roughly 10-12% of adults at autopsy; under 1% symptomatic
- Thoracic spine is the most common symptomatic and aggressive site
- Benign lesion - no malignant transformation
Pathognomonic Imaging
- Polka-dot sign on axial CT (trabeculae end-on)
- Corduroy / jail-bar sign on sagittal CT or radiograph
- High T1 and T2 signal = fatty, quiescent lesion
- Low T1 signal = vascular stroma, potentially aggressive
Aggressive Features
- Low T1 signal with avid enhancement
- Cortical expansion and bony destruction
- Epidural or paravertebral soft-tissue extension
- Progressive neurological deficit; pregnancy can trigger
Staging Tools
- Enneking benign: S1 latent, S2 active, S3 aggressive
- WBB: 12 zones and 5 layers to plan resection
- SINS: grades mechanical instability
- ASIA scale for neurological status
Management
- Incidental fatty lesion: observe and reassure, no biopsy
- Painful, intact: vertebroplasty or radiotherapy
- Aggressive with deficit: embolisation then decompression and stabilisation
- Adjuvant radiotherapy for residual tumour after subtotal resection
Surgical Pearls
- Always embolise before resecting - highly vascular, heavy bleeding
- Match extent of surgery to lesion behaviour and patient fitness
- Less extensive surgery can give good recovery with low recurrence
- Biopsy only atypical lesions, along an excisable tract, in a specialist unit
Evidence Base and Key Studies
Total En Bloc Spondylectomy For Enneking Stage 3 Aggressive Lesions
- Series of 23 Enneking stage 3 aggressive vertebral haemangiomas with neurological deficit treated by one-stage posterior total en bloc spondylectomy
- 17 thoracic and 6 lumbar lesions; all had cord compression with or without instability (mean SINS 9.78)
- Mean operative blood loss 1883 mL after preoperative embolisation, with no serious complications reported
- All patients recovered to ASIA-E (normal) neurological status after surgery
- Mean pain score fell from 8.0 to 2.8 out of 10
Is A Less Extensive Approach Adequate For Aggressive Lesions With Deficit
- 21 patients with aggressive vertebral haemangioma and neurological deficit, staged by Enneking and WBB systems with SINS
- All underwent preoperative embolisation; procedures ranged from intralesional spondylectomy to decompression with vertebroplasty and stabilisation
- Neurology improved in all patients over a mean follow-up of about 56 months
- Only one recurrence across the cohort
- Less extensive procedures achieved good clinical, neurological and radiological outcomes
Role Of Radiotherapy And Surgery In Aggressive Vertebral Haemangioma
- 20 patients with aggressive vertebral haemangioma and mild or slowly progressive deficit treated with radiotherapy as first-line therapy (40-50 Gy)
- 65% (13 of 20) were symptom-free without recurrence or malignant transformation at last follow-up (mean 75 months)
- Seven patients needed subsequent surgery for increasing or persistent deficit
- No malignant transformation was observed in any patient
- Radiotherapy was concluded to be safe and effective for mild or slowly progressive disease
Combined Surgical And Endovascular Treatment Of Aggressive Lesions
- 10 patients with aggressive vertebral haemangioma over 17 years, undergoing 13 procedures
- All but one had preoperative procedures to minimise intraoperative blood loss
- All eight patients presenting with neurological deficit improved postoperatively
- Most underwent subtotal resection; one had en bloc resection, with one recurrence requiring staged surgery
- Combined embolisation, resection and stabilisation was safe and effective