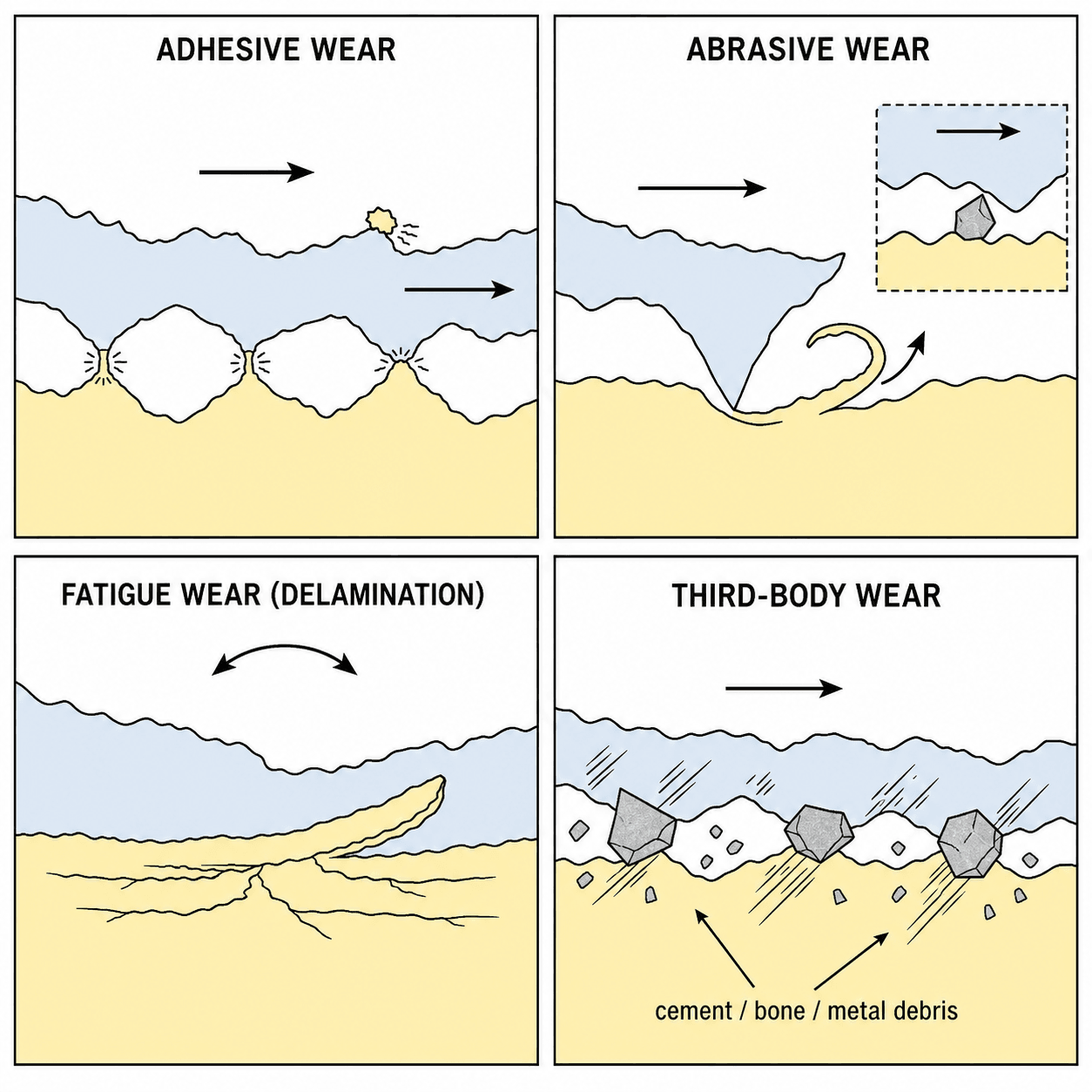
Adhesive | Abrasive | Fatigue | Third-Body
- Polyethylene wear debris causes particle-induced osteolysis via macrophage activation
- Cross-linking reduces polyethylene wear by 50-90% but may reduce mechanical properties
- Ceramic-on-ceramic has lowest volumetric wear but risk of fracture and squeaking
- Third-body wear from cement, bone, or metal particles accelerates bearing damage
- Wear threshold: historic 2mm/year PE wear associated with osteolysis risk
- “Adhesive = cold welding, material transfer
- “Abrasive = harder scratches softer (two-body or three-body)
- “Fatigue (delamination) = subsurface crack propagation
- “Particle size 0.1-1μm most biologically active for osteolysis
Adhesive: Cold welding and transfer. Abrasive: Scratching. Third-body: Trapped particles. Fatigue: Subsurface cracks from cyclic loading (delamination in PE).
Wear particles activate macrophages → release cytokines (IL-1, TNF-α) → stimulate osteoclasts → bone resorption around implant → loosening. Particle size 0.1-1μm most inflammatory.
Highly cross-linked polyethylene (radiation, remelting/annealing) reduces wear 50-90%. Trade-off: reduced toughness and fracture resistance. Standard for hip, gaining use in knee.
MoP: Metal-on-poly, standard, improved with HXLPE. CoC: Ceramic-on-ceramic, lowest wear but fracture/squeak risk. MoM: Abandoned due to metal ions. CoP: Ceramic-on-poly, low wear.
Overview
Wear is the progressive loss of material from articulating surfaces due to mechanical action. In orthopaedic joint replacement, wear generates debris that can cause adverse biological reactions (osteolysis) leading to implant loosening and revision surgery.
Clinical Significance
- Primary cause of long-term arthroplasty failure
- Polyethylene wear debris triggers osteolysis
- Drives bearing surface material development
- HXLPE has dramatically improved outcomes
Mechanisms and Types
Adhesive Wear
Definition: Wear resulting from adhesion (cold welding) between asperities of two surfaces, followed by material transfer.
Mechanism:
- High local pressure at asperity contact points
- Local adhesion (micro-welding) between surfaces
- Relative motion shears the junction
- Material transfers from weaker to stronger surface
- Transferred material may detach as debris
Factors:
- Surface finish quality
- Lubrication (synovial fluid)
- Material hardness mismatch
- Contact pressure
Clinical Examples:
- Metal-on-metal bearings (historic)
- Poorly lubricated interfaces
- Run-in wear in new implants
Prevention:
- Good surface finish
- Adequate lubrication
- Material selection (CoCr or ceramic heads)
Volumetric vs Linear Wear (and the Head-Size Paradox)
The topic quotes wear as both "mm/year" (linear) and "volumetric", and repeatedly flags large heads — the relationship between them is a classic basic-science point.
- Two ways to measure wear. Linear wear is the penetration depth of the head into the liner (mm/year, measured radiographically — the clinical number, and what the historic 2 mm/year osteolysis threshold refers to). Volumetric wear is the actual volume of material removed (mm cubed/year), which determines the number of particles and hence the biological burden.
- The head-size paradox. For a polyethylene bearing, volumetric wear rises with head diameter (a larger head sweeps a greater sliding distance, so more material is removed per year) even though the linear penetration may be similar or lower. This is why very large-head metal-on-metal and large-diameter bearings, despite low linear wear, generated a large volumetric (and ionic) debris burden.
- Why it matters biologically. Because osteolysis is driven by the number of submicron particles, volumetric wear — not linear penetration alone — best predicts osteolytic potential. HXLPE reduces both, which is why it cut osteolysis so dramatically.
- Run-in vs steady-state. Wear is typically higher in the first year or so (run-in, as surface asperities bed in) then settles to a lower steady-state rate — relevant when interpreting early radiographic wear measurements.
Q: A larger femoral head gives better stability — why can it increase wear? A: Linear and volumetric wear are different. A bigger head sweeps a longer sliding distance, so volumetric wear (and particle number) rises with head diameter even when linear penetration is unchanged — the reason large-head metal-on-metal bearings produced a heavy volumetric/ionic debris load. Osteolysis tracks particle number (volumetric wear), not linear mm/year alone.
Bearing Surface Anatomy
Articulating Surfaces
- Femoral head (CoCr, ceramic, or oxinium)
- Acetabular liner (PE, ceramic, or metal)
- Modular junction (head-neck trunnion)
- Femoral component (CoCr)
- Tibial insert (polyethylene)
- Patellofemoral articulation
- Head
- CoCr or ceramic
- Cup/Insert
- Polyethylene
- Head
- Ceramic
- Cup/Insert
- Ceramic
- Head
- Ceramic
- Cup/Insert
- Polyethylene
- Head
- CoCr
- Cup/Insert
- CoCr (abandoned)
Differential Diagnosis: Causes of Late Arthroplasty Failure
Wear-driven osteolysis is one of several causes of a painful or failing joint replacement. Distinguishing them governs management.
- Typical Features
- Slow, often asymptomatic; eccentric head; lytic lesions
- Key Investigation
- Serial X-ray, CT volume
- Discriminator
- High PE wear rate, scalloped periprosthetic lysis
- Typical Features
- Start-up pain, progressive radiolucent lines
- Key Investigation
- Serial X-ray
- Discriminator
- Migration/subsidence over time
- Typical Features
- Rest pain, early failure, effusion, raised CRP/ESR
- Key Investigation
- Aspiration, alpha-defensin, cultures
- Discriminator
- Positive aspirate, raised inflammatory markers
- Typical Features
- MoM or corroded trunnion; effusion, mass
- Key Investigation
- Cobalt/chromium ions, MARS-MRI
- Discriminator
- Pseudotumour, elevated metal ions
- Typical Features
- Squeak or sudden noise; CoC bearing
- Key Investigation
- X-ray, CT
- Discriminator
- Audible squeak, fracture line, stripe wear
Classification
Wear Mechanism Types (AAFT)
Four Primary Mechanisms:
- Mechanism
- Cold welding, material transfer
- Example
- MoM bearings
- Mechanism
- Scratching by harder surface
- Example
- Damaged CoCr head
- Mechanism
- Subsurface cracks, delamination
- Example
- Gamma-sterilized PE
- Mechanism
- Trapped particles accelerate wear
- Example
- Cement debris
Investigations
Assessment of Wear
- Serial radiographs for PE wear measurement
- Measure from femoral head center to acetabular rim
- Compare to baseline post-op films
- Linear wear rate (mm/year)
- Eccentric head position
- Osteolytic lesions (radiolucent areas)
- Purpose
- Wear measurement
- Findings
- Linear wear, osteolysis
- Purpose
- Osteolysis quantification
- Findings
- 3D bone loss assessment
- Purpose
- Soft tissue assessment
- Findings
- ALVAL, pseudotumor
Management
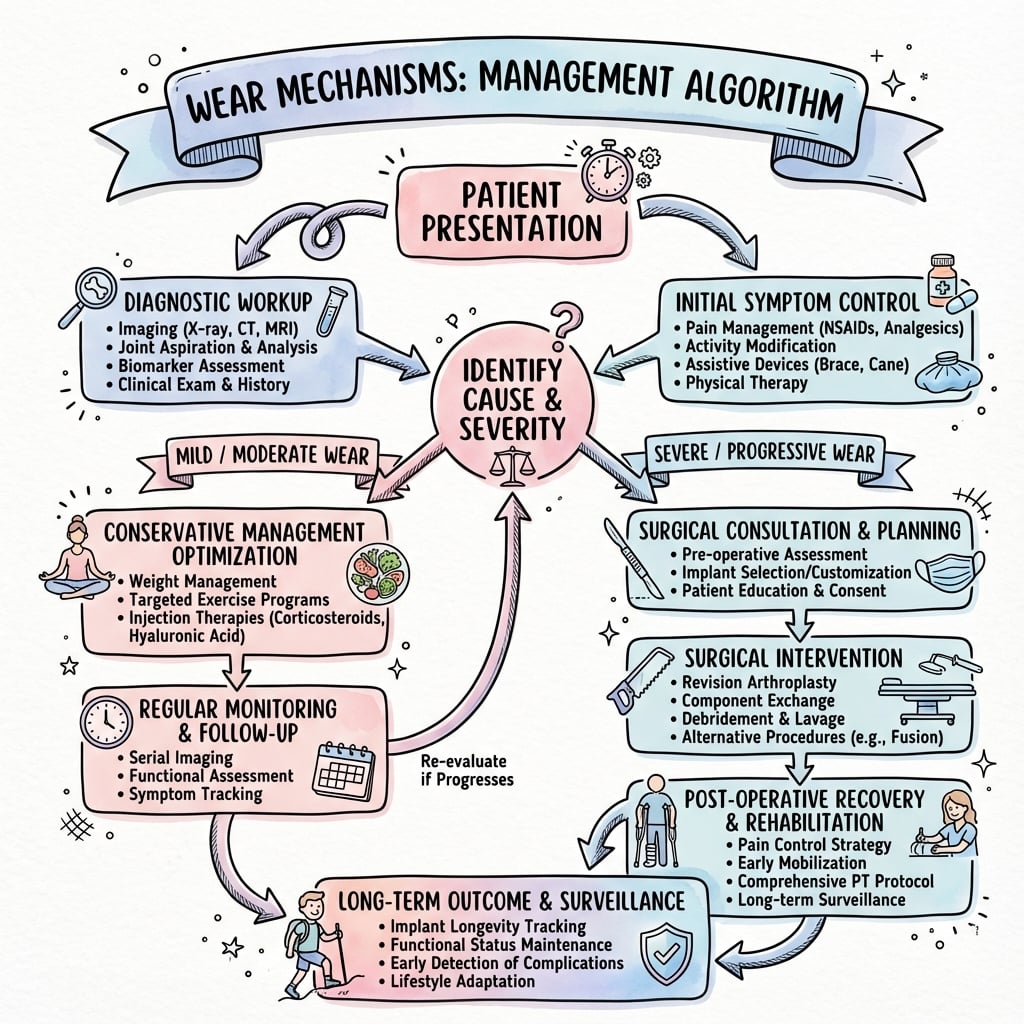
Management Approach
- Asymptomatic wear: Serial monitoring
- Annual or biannual radiographs
- Assess for progressive osteolysis
- Symptomatic loosening
- Progressive osteolysis
- High wear rate with HXLPE available
- Approach
- Observe, serial X-rays
- Rationale
- May stabilize
- Approach
- Plan revision
- Rationale
- Prevent bone loss
- Approach
- Revision arthroplasty
- Rationale
- Address failure
Revision Surgical Technique
Revision Approach
- Isolated liner exchange: Well-fixed cup, adequate bone
- Cup revision: Loose cup or insufficient bone
- Stem revision: If loose or corroded trunnion
- Remove liner, debride membrane
- Bone graft osteolytic lesions
- Insert new HXLPE liner
- Indication
- Well-fixed cup, good bone
- Complexity
- Moderate
- Indication
- Loose or poor bone stock
- Complexity
- Major
- Indication
- Both components involved
- Complexity
- Complex
Complications
Wear-Related Complications
- Particle-induced osteolysis
- Aseptic loosening
- Periprosthetic fracture
- Polyethylene: Osteolysis, loosening
- Metal: ALVAL, pseudotumor, metallosis
- Ceramic: Fracture, squeaking
- Complication
- Osteolysis
- Incidence
- 10-20% at 10 years
- Complication
- Osteolysis
- Incidence
- Less than 5% at 10 years
- Complication
- Fracture
- Incidence
- Less than 0.1%
- Complication
- ALVAL
- Incidence
- 5-10% (abandoned)
Postoperative Care
After Revision Surgery
- Standard THA precautions
- Protected weight-bearing if bone grafted
- VTE prophylaxis
- Serial radiographs to assess bone healing
- Monitor for osteolysis resolution
- Long-term surveillance
- Weight-Bearing
- Protected if bone graft
- Activity
- Hip precautions
- Weight-Bearing
- Progress to full
- Activity
- Rehabilitation
- Weight-Bearing
- Full activities
- Activity
- Long-term monitoring
Outcomes
Modern Bearing Outcomes
- 95-98% survivorship at 10-15 years
- Dramatic reduction in osteolysis
- Lower revision rates than conventional PE
- 97-99% survivorship at 10 years
- Lowest wear rates
- Rare fracture/squeaking
- 10-Year Survival
- 95-98%
- Key Advantage
- Low wear, proven
- 10-Year Survival
- 97-99%
- Key Advantage
- Lowest wear
- 10-Year Survival
- 96-98%
- Key Advantage
- Low wear, no squeak
- 10-Year Survival
- 85-90%
- Key Advantage
- Abandoned for HXLPE
Clinical Relevance - Particle Disease
Particle-Induced Osteolysis
Pathophysiology:
- Wear particles generated at bearing surfaces
- Macrophages attempt to phagocytose particles
- Particles too large or resistant to digestion
- Frustrated phagocytosis activates macrophages
- Release of pro-inflammatory cytokines (IL-1, TNF-α, IL-6)
- Cytokines stimulate osteoclast differentiation (RANK-RANKL)
- Osteoclastic bone resorption around implant
- Progressive osteolysis leads to loosening
Particle Characteristics:
- Size 0.1-1μm most biologically active
- Larger particles less inflammatory (cannot be phagocytosed)
- Smaller particles - billions generated, cumulative effect
- Material volume of debris: PE greater than metal greater than ceramic
Clinical Manifestations:
- Often asymptomatic until advanced
- Radiolucent lesions on radiographs
- Progressive loosening
- Pathological periprosthetic fracture
The Effective Joint Space: Why Osteolysis Occurs at a Distance
The evidence base notes that "solid fixation limits particle migration" — the unifying concept is the effective joint space.
- The concept (Schmalzried). The effective joint space is the entire region a prosthetic joint's fluid — and therefore its wear debris — can reach, which is far larger than the articulation itself. Pressurised joint fluid pumps particles along any accessible interface.
- Why lysis appears remote from the bearing. Debris tracks down the bone-implant (or bone-cement) interface and along the stem and — classically — through empty acetabular screw holes and around screws, producing focal (scalloped) osteolytic lesions remote from the bearing surface. This is why periacetabular or peri-stem lysis can appear where the bearing itself is not.
- Fixation controls migration. A well-bonded, circumferentially porous-coated or fully cemented interface limits the effective joint space and confines debris — hence the observation that solid fixation reduces particle migration and osteolysis, and the move away from non-circumferential coatings and unnecessary screw holes.
- Clinical corollary. Osteolysis is often silent and periprosthetic rather than at the joint line, so surveillance radiographs (and CT) must be read along the whole length of the implant, not just at the bearing.
Q: Why does periprosthetic osteolysis appear around acetabular screw holes or down the stem, away from the bearing? A: The effective joint space (Schmalzried) — pressurised joint fluid carries submicron wear debris along every accessible interface, including through empty screw holes and down the bone-implant interface, causing scalloped lysis remote from the articulation. Solid, circumferential fixation limits the effective joint space and confines debris, which is why fixation quality protects against osteolysis.
Guidelines, Registries & Global Practice
Global epidemiology: Particle-induced osteolysis and aseptic loosening were historically the leading causes of late revision in metal-on-conventional-polyethylene hips. The widespread shift to HXLPE has substantially reduced wear-related revision worldwide, while metal-on-metal bearings were largely abandoned after 2010 following adverse-reaction-to-metal-debris signals.
- Position on bearings & wear
- Supports HXLPE as standard bearing; evidence-based work-up for painful MoM hips
- Position on bearings & wear
- Bearing selection guidance with registry-informed implant benchmarks (ODEP ratings)
- Position on bearings & wear
- Emphasises tribology principles, component positioning to limit edge loading
- Position on bearings & wear
- Endorse HXLPE and ceramic bearings; structured MoM surveillance
- Position on bearings & wear
- Issued alerts mandating surveillance of metal-on-metal hips (ion levels, MARS-MRI)
Registry evidence: National joint registries (NJR England/Wales, AJRR US, AOANJRR Australia, Swedish SHAR, Norwegian, NZJR) consistently show lower revision rates for HXLPE versus conventional polyethylene and the highest revision rates for large-head metal-on-metal bearings, driving global practice change. Registries also underpin implant benchmarking schemes (e.g. ODEP) used internationally.
High- vs limited-resource practice: In high-resource settings HXLPE and ceramic bearings are routine, with CT and MARS-MRI available for surveillance. In limited-resource settings conventional polyethylene and metal-on-poly remain common due to cost, and surveillance relies mainly on serial plain radiographs; metal ion assays and metal-artefact-reduction MRI may be unavailable.
Controversies & Areas of Uncertainty
Remelting (above the melt transition) eliminates free radicals most completely but lowers crystallinity and mechanical strength. Annealing (below melt) preserves mechanical properties but leaves residual free radicals and a residual oxidation risk. The optimal trade-off remains debated; vitamin E stabilisation is an attempt to sidestep it.
HXLPE is the clear standard at the hip, but the knee sees higher contact stress, multidirectional motion and thinner inserts where reduced toughness could matter. Registry signals are favourable but long-term superiority over conventional PE in TKA is not yet definitively proven.
The commonly cited ~7 ppb cobalt/chromium action level is a guide, not a hard cut-off. Symptoms, imaging and trends matter more than a single value, and authorities differ on exact thresholds and surveillance intervals.
CoC offers the lowest wear and is attractive in young, active patients, but fracture risk (rare with fourth-generation delta ceramic), squeaking and cost temper enthusiasm versus ceramic-on-HXLPE. Best bearing for the young patient is unresolved.
MCQ Practice Points
Q: What are the four main types of wear in orthopaedic implants? A: Adhesive (cold welding), Abrasive (scratching), Fatigue (delamination), and Third-body (trapped particles). Remember AAFT.
Q: What is the mechanism of particle-induced osteolysis? A: Wear particles are phagocytosed by macrophages → activated macrophages release cytokines (IL-1, TNF-α) → cytokines stimulate RANK-RANKL pathway → osteoclast activation → bone resorption.
Q: How does highly cross-linked polyethylene reduce wear? A: Cross-linking by irradiation creates bonds between polymer chains, reducing plastic deformation and adhesive/abrasive wear by 50-90%. Post-irradiation treatment (remelting/annealing/vit E) removes free radicals to prevent oxidation.
At a Glance
Four primary wear mechanisms affect orthopaedic bearings: adhesive (cold welding and material transfer), abrasive (harder surface scratches softer), fatigue/delamination (subsurface crack propagation from cyclic loading), and third-body (trapped particles accelerate wear). Polyethylene wear debris causes particle-induced osteolysis via macrophage activation and cytokine release (IL-1, TNF-α) stimulating osteoclasts—particles 0.1-1μm are most biologically active. Highly cross-linked polyethylene (HXLPE) reduces wear by 50-90% but with reduced toughness. Bearing combinations: MoP (metal-on-poly, improved with HXLPE), CoC (ceramic-on-ceramic, lowest wear but fracture/squeak risk), CoP (ceramic-on-poly), and MoM (abandoned due to metal ion concerns). Historic threshold: over 2mm/year PE wear associated with osteolysis risk.
AAFTWear Types
Hook:AAFT = Adhesive, Abrasive, Fatigue, Third-body - the four wear mechanisms!
POMOOsteolysis Pathway
Hook:POMO = Particles → macrophages (Opsonize) → Mediators → Osteolysis!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old man presents with progressive periacetabular osteolysis 12 years after primary cemented THA. PE wear measures 3mm. He is minimally symptomatic. How do you manage him?”
“A retrieved polyethylene liner shows sheet-like surface delamination with a subsurface white band. The examiner asks you to classify the wear mechanisms acting on a bearing surface and explain what this retrieval demonstrates.”
“A 58-year-old woman has groin pain three years after a large-head metal-on-metal THA. Radiographs show well-fixed components. How do you investigate and manage her?”
Wear Types (AAFT)
- Adhesive: Cold welding and transfer
- Abrasive: Scratching (two-body or three-body)
- Fatigue: Subsurface cracks, delamination
- Third-body: Trapped particles accelerate wear
Osteolysis Pathway
- Particles → Macrophage phagocytosis
- Cytokine release (IL-1, TNF-α)
- RANK-RANKL → Osteoclast activation
- Particle size 0.1-1μm most active
HXLPE
- Cross-linking by irradiation
- Remelting/annealing removes free radicals
- Wear reduction 50-90%
- Standard for hip, increasing in knee
Bearing Selection
- MoP with HXLPE: Standard, proven
- CoC: Lowest wear, fracture/squeak risk
- CoP: Low wear, ceramic benefits
- MoM: Abandoned (metal ions, ALVAL)
Evidence Base
- Double-blinded RCT, 122 patients, minimum 10-year follow-up
- 3-D wear rate 0.03 mm/yr (XLPE) versus 0.27 mm/yr (conventional UHMWPE), p less than 0.001
- Osteolysis prevalence 8% (XLPE) versus 38% (conventional), p less than 0.005
- Revision rate 1.9% (XLPE) versus 14.6% (conventional), p = 0.012
- It is the concentration of particles in the critical size range, not total wear volume, that drives the biological response
- Critical size range for macrophage activation is 0.2-0.8 micron
- Pre-clinical testing of any bearing must characterise particle size and reactivity, not just wear volume
- Predicted nanometre-scale metal-on-metal debris would raise new biological concerns
- Polyethylene particle NUMBER (not size) differed between osteolysis-positive and -negative cases
- Critical threshold around 1 x 10^10 particles per gram of tissue for osteolysis
- Macrophages identified as the cells primarily responsible for bone loss
- Solid bone-implant fixation limits particle migration and osteolysis
- First RCT reporting 7-year RSA results for vitamin E-diffused HXLPE (VEPE)
- Mean 7-year proximal head penetration -0.07 mm (VEPE) versus 0.00 mm (moderately XLPE), not significant
- All wear rates below the 0.1 mm/yr osteolysis threshold
- No implants revised for aseptic loosening; acetabular radiolucency linked to greater shell migration
- 235 fourth-generation (BIOLOX delta) CoC THAs, mean 12-year follow-up
- All-cause survivorship 96.7% at 12 years
- Squeaking reported in 9 hips; only 1 required revision for squeaking
- No ceramic liner or head fractures in the cohort
- Reviews development and clinical results of HXLPE in hip and knee arthroplasty
- Polyethylene wear and osteolysis identified as principal long-term failure modes
- Second-generation (vitamin E) HXLPE introduced to address oxidative degradation
- Ongoing retrieval and clinical studies needed for longest-term durability