Motion-Preserving Salvage | RA Primary Indication | Distal Loosening Challenge | Low-Demand Essential
- Rheumatoid arthritis is the primary indication - low demands, soft bone, bilateral disease
- Distal component loosening is the most common failure mode (10-30%) - metacarpal stress shielding
- Low-demand patients essential - heavy use accelerates loosening and failure
- Preserves 40-60 degrees motion arc vs arthrodesis which eliminates all motion
- Fusion remains gold standard for high-demand patients due to durability concerns
- “TWA vs fusion: Motion preservation (TWA) vs durability (fusion) - patient selection critical
- “Distal component loosening most common complication - occurs at metacarpal-carpal junction
- “RA patients ideal: low demands, soft bone accepts cement, often bilateral disease
- “Extensor tendon rupture occurs due to dorsal hardware prominence - 5-10% incidence
Rheumatoid arthritis with low demands is the ideal indication. High-demand patients, young age, and heavy manual labor are relative contraindications. Patient selection is the single most important factor determining outcome. Poor selection leads to early loosening and revision.
Distal component loosening is the Achilles heel of TWA (10-30%). Occurs at metacarpal-carpal junction due to stress concentration. Modern third-generation designs address this with improved distal fixation but long-term durability remains inferior to fusion.
Preserves 40-60 degrees arc of motion at wrist. Critical for patients with bilateral disease, contralateral fusion, or occupations requiring wrist motion. However, motion preservation comes at cost of durability - trade-off must be discussed with patient.
Arthrodesis preferred for high-demand patients, young patients, and those requiring durability. Fusion eliminates motion but provides reliable pain relief with 95 percent union. TWA revision rate higher than primary fusion rate.
- Total Wrist Arthroplasty
- RA, low-demand, bilateral disease
- Wrist Arthrodesis
- High-demand, OA, post-traumatic
- Total Wrist Arthroplasty
- Preserves 40-60 degree arc
- Wrist Arthrodesis
- Eliminates all wrist motion
- Total Wrist Arthroplasty
- 80% survival at 5 years
- Wrist Arthrodesis
- 95% union rate, durable long-term
- Total Wrist Arthroplasty
- Distal component loosening (10-30%)
- Wrist Arthrodesis
- Nonunion (5-10%)
- Total Wrist Arthroplasty
- 15-25% at 10 years
- Wrist Arthrodesis
- 5-10% at 10 years
- Total Wrist Arthroplasty
- 50-70% of normal
- Wrist Arthrodesis
- 60-80% of normal
- Total Wrist Arthroplasty
- Low-demand activities only
- Wrist Arthrodesis
- Higher-demand activities possible
- Total Wrist Arthroplasty
- Ideal - motion both sides
- Wrist Arthrodesis
- Functional limitation if bilateral
LOWRATWA Patient Selection
Hook:LOWRA selection: Low demand, Older, Widespread RA with Adequate bone - ideal TWA candidate.
HEAVYTWA Contraindications
Hook:HEAVY contraindications: High demand, Extensor deficiency, Active infection, Very young, Youthful activity - choose fusion instead.
Overview and Epidemiology
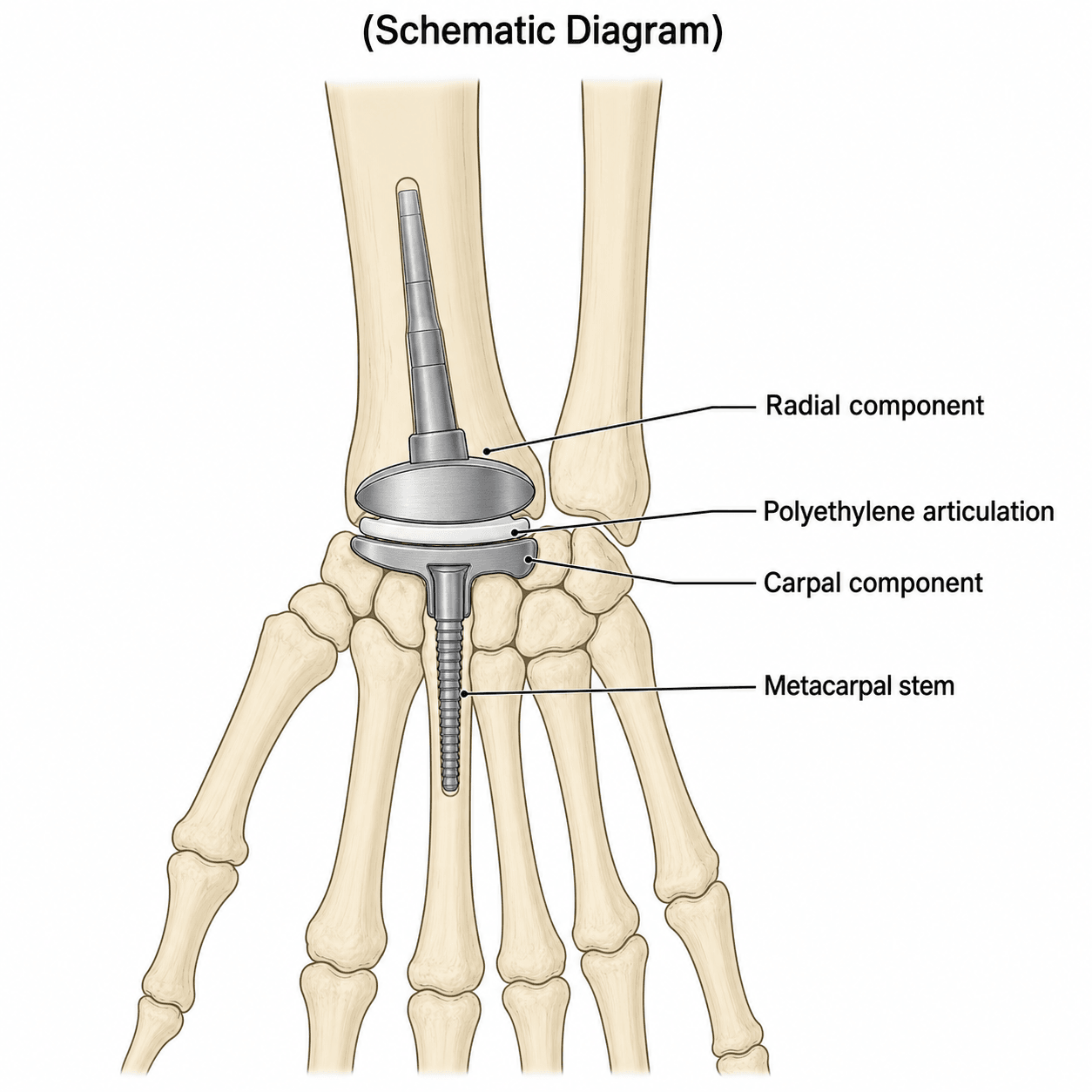
Total wrist arthroplasty (TWA) is a motion-preserving salvage procedure for end-stage wrist arthritis. It replaces the radiocarpal and midcarpal joints with prosthetic components, maintaining wrist motion unlike arthrodesis which eliminates all motion.
Wrist arthroplasty has evolved through three generations. First-generation designs (1970s-1980s) had high failure rates due to poor fixation and excessive constraint. Second-generation designs (1980s-1990s) introduced improved fixation but still had significant loosening. Third-generation designs (2000s-present) including Universal 2, Maestro, and ReMotion use ellipsoidal articulation, improved distal fixation, and better bone preservation with improved but still concerning long-term survival.
- Rheumatoid arthritis with low functional demands
- Bilateral wrist disease (motion preservation both sides)
- Contralateral wrist fusion (motion preservation essential)
- Elderly patients with limited activity expectations
- Primary osteoarthritis in low-demand patients
- Post-traumatic arthritis in carefully selected patients
- SLAC/SNAC wrist when motion preservation desired
- High-demand patients or heavy manual labor
- Young age with longevity concerns
- Poor bone stock (severe osteopenia)
- Inadequate soft tissue envelope or extensor deficiency
- Active infection
- Frequency: Uncommon compared to fusion (approximately 1:10 ratio)
- Trend: Increasing use due to improved third-generation designs
- Registry data: AOANJRR limited data due to low numbers
Despite motion preservation, TWA remains a niche procedure because durability is inferior to fusion. Distal component loosening at 10-30% is concerning compared to 5-10% nonunion for fusion. Patient selection is critical - RA with low demands is ideal. High-demand patients should have fusion. The trade-off is motion versus durability.
Implant Types and Biomechanics
- Silicone spacers (Swanson)
- Ball-and-socket designs (Meuli)
- High failure rates due to silicone synovitis, constraint, loosening
- Largely abandoned
- Biaxial design (Cooney)
- Improved fixation but still significant loosening
- Constrained designs caused bone loss
Universal 2 (Integra)
- Ellipsoidal articulation (toroidal radial component)
- Titanium porous-coated radial component
- Cobalt-chrome carpal component
- Polyethylene insert (UHMWPE)
- Distal fixation into 2nd and 3rd metacarpals
- Proximal: Press-fit or cemented into radius
- Distal: Carpal plate with metacarpal stems
- Flexion-extension: 40-60 degrees arc
- Radial-ulnar deviation: 15-25 degrees arc
- 80-85% survival at 5 years
- 60-70% survival at 10 years
Most widely used design with longest follow-up data.
Silicone Wrist Arthroplasty and Silicone-Induced Synovitis
The first-generation silicone (Silastic) implants popularised by Swanson were not true articulating replacements but flexible hinged spacers inserted after resection of the proximal carpal row or radiocarpal joint, acting as a dynamic interposition that guided fibrous encapsulation. They gave early pain relief and were technically simple, but their mechanical and biological failure modes are the reason modern total wrist arthroplasty exists - and they remain a favourite examiner theme.
- Implant fracture and fragmentation. Repetitive loading of a flexible polymer across the high-stress wrist led to tearing and fracture of the spacer, with loss of alignment and recurrent deformity.
- Silicone-induced particulate synovitis. Micro-fragmentation shed silicone particulate debris that provoked a foreign-body granulomatous reaction. The resulting proliferative synovitis and macrophage response drove progressive cystic bone erosions (geodes), component subsidence and, occasionally, regional silicone lymphadenopathy. This destructive osteolysis, rather than simple surface wear, is the hallmark lesion.
- Bone loss compromising salvage. The cystic destruction consumed carpal and metacarpal bone stock, making later conversion to arthrodesis technically demanding and graft-dependent.
metal (titanium) grommets were introduced to shield the silicone from sharp resected bone edges, reduce abrasion and delay fracture. They mitigated but did not eliminate the problem.
silicone is now essentially abandoned for total wrist replacement, but silicone interposition retains a limited role in some low-demand settings and remains widely used in metacarpophalangeal arthroplasty for the rheumatoid hand - a distinction worth stating explicitly in the viva.
If asked why early wrist arthroplasty was abandoned, name silicone-induced particulate synovitis specifically: a foreign-body granulomatous reaction to fragmented silicone that produces cystic (geode) bone erosions and progressive bone loss, compounded by implant fracture. Grommets reduced but did not solve it. Contrast this with modern designs, whose dominant late failure is polyethylene wear-driven distal component loosening.
Surgical Technique
Pre-operative Planning Steps
- Confirm low-demand lifestyle
- Assess functional requirements
- Evaluate bilateral disease status
- Discuss expectations and limitations
- Confirm end-stage arthritis
- Assess bone quality (RA often osteopenic)
- Evaluate soft tissue envelope
- Assess extensor tendon integrity
- PA and lateral wrist X-rays
- Templating for component sizing
- CT if bone stock concerns
- MRI if soft tissue concerns
- TWA system (Universal 2, Maestro, or ReMotion)
- Multiple sizes available
- Cement if needed (RA with soft bone)
- Fluoroscopy for intraoperative imaging
- Motion preservation benefit versus durability concerns
- Revision rate higher than fusion
- Activity restrictions permanent
- Alternative of fusion discussed
Proper planning ensures appropriate patient selection and realistic expectations.
Complications
- Incidence
- 10-30%
- Risk Factors
- High demand, poor bone quality, malalignment
- Management
- Revision arthroplasty or conversion to fusion
- Incidence
- 10-15%
- Risk Factors
- Component malposition, inadequate resection
- Management
- Debridement, component revision if severe
- Incidence
- 5-10%
- Risk Factors
- Dorsal hardware prominence, RA (weakened tendons)
- Management
- Tendon reconstruction or transfer
- Incidence
- 5-10%
- Risk Factors
- Soft tissue deficiency, component malalignment
- Management
- Thicker polyethylene, ligament repair, revision
- Incidence
- 3-5%
- Risk Factors
- Osteopenic bone, trauma, stress risers
- Management
- ORIF if stable, revision if loose
- Incidence
- 2-5%
- Risk Factors
- RA (immunosuppression), diabetes, poor nutrition
- Management
- Debridement, antibiotics, may need explant
- Incidence
- 5-10%
- Risk Factors
- Superficial radial nerve at risk dorsally
- Management
- Usually neuropraxia - observe, neuroma excision if persistent
Distal component loosening is the Achilles heel of wrist arthroplasty, occurring in 10-30% of cases. It occurs at the carpal-metacarpal junction due to stress concentration, inadequate fixation, and stress shielding. Third-generation designs address this with improved metacarpal stems or central screw fixation, but long-term durability remains inferior to fusion. Patient selection (low demand) is critical for minimizing this complication.
Extensor tendon rupture (5-10%) occurs due to dorsal hardware prominence and is more common in RA patients who have weakened tendons. Prevention includes ensuring smooth dorsal profile, adequate soft tissue coverage, and early hardware removal if prominent. Management requires tendon reconstruction or transfer (EIP to EPL for EPL rupture).
LITERTWA Complications
Hook:LITER of problems: Loosening, Impingement, Tendon rupture, Erosion, Revision - distal loosening is the key failure mode.
Diagnosing and Monitoring Component Loosening
The topic repeatedly hinges on "loosening", "radiographic lucency" and "subsidence" as the defining failure of total wrist arthroplasty, yet these signs must be interpreted carefully - the single most examined nuance is that radiolucency does not automatically equal a failed implant needing revision.
Radiographic features of loosening (always compared with the immediate post-operative film):
- Progressive radiolucent lines at the bone-implant or bone-cement interface. A thin (fewer than 2 mm), non-progressive lucent line may represent stable fibrous fixation; a lucency greater than 2 mm that widens across serial films suggests true loosening.
- Component migration or subsidence - the carpal/distal component sinking into the metacarpal, or the radial component tilting or shifting position.
- Change in component alignment or tilt, cement-mantle fracture, and focal osteolytic (particle disease) lesions with a scalloped margin.
- Zonal analysis. The Wrightington zonal classification (used by Newton and colleagues for the Universal 2) systematically scores lucency around defined radial and carpal component zones, improving reproducibility over a subjective global impression.
Interpreting the findings:
- Sagerfors and colleagues showed radiographic loosening did not reliably predict revision, and satisfaction remained high despite lucent lines - so imaging is read alongside symptoms, never in isolation.
- The combination that warrants intervention is progressive lucency plus subsidence plus activity-related pain, as in the classic loosening viva.
- Serial plain films are the workhorse; CT better defines bone stock and osteolysis for revision planning.
- Before attributing symptoms to aseptic loosening, exclude low-grade infection with ESR, CRP and, where indicated, joint aspiration - an infected loose implant is managed entirely differently.
Score marks by distinguishing a stable, non-progressive lucent line (fewer than 2 mm) from progressive lucency with subsidence and pain. Always compare with the immediate post-operative radiograph, use a zonal system for reproducibility, and exclude infection with inflammatory markers before calling it aseptic loosening.
Postoperative Care and Rehabilitation
Immediate Postoperative Care (0-2 weeks)
- Volar splint in neutral position
- Elevation above heart level
- Neurovascular checks every 4 hours
- Finger ROM encouraged immediately
- Maintain splint continuously
- Active finger ROM exercises
- Wound check at 7-10 days
- Suture removal at 10-14 days
- Convert to removable splint at 2 weeks
- Multimodal analgesia (paracetamol, NSAIDs if appropriate)
- Opioids for breakthrough pain
- Ice elevation for swelling
Early finger motion maintains tendon gliding and prevents stiffness.
Guidelines, Registries & Global Practice
Global Epidemiology
- Wrist arthroplasty is uncommon worldwide - performed roughly an order of magnitude less often than wrist fusion. Most published series are single-centre or national-registry cohorts of a few hundred cases.
- Historically rheumatoid arthritis dominated indications. With widespread DMARD and biologic therapy, the incidence of severe destructive RA wrists requiring surgery has fallen, and the proportion of cases performed for osteoarthritis and post-traumatic disease has risen (Norwegian register trend).
- Typical patient: low-demand, often older than 60, frequently with bilateral or contralateral wrist disease.
Registry Evidence (side by side)
- Cohort
- 189 wrists (Biax, Elos, Gibbon)
- Key Survivorship Signal
- 78% at 5 yr, 71% at 10 yr; Biax 85% vs Elos 57% at 5 yr
- Cohort
- 219 wrists
- Key Survivorship Signal
- 8-yr survival: Maestro 95%, ReMotion 94%, Biax 81%
- Cohort
- Low annual wrist-replacement volumes
- Key Survivorship Signal
- Numbers too small for robust implant ranking - underlines niche status
Society and Practice Guidance
- No major society (AAOS, BOA, EFORT, AO) issues a dedicated stand-alone wrist-arthroplasty guideline; recommendations derive from hand-surgery consensus and registry data.
- Consensus across regions: arthrodesis remains the durable benchmark, particularly for high-demand and younger patients; arthroplasty is reserved for selected low-demand patients prioritising motion, especially with bilateral disease or contralateral fusion.
- Shared decision-making and explicit counselling on revision risk and permanent activity restriction are universally emphasised.
High- vs Limited-Resource Practice Variation
- High-resource settings: third- and fourth-generation modular implants, intraoperative fluoroscopy, and dedicated hand-therapy rehabilitation are standard; revisability and conversion-to-fusion planning influence implant choice.
- Limited-resource settings: implant cost and availability, lack of revision inventory, and limited hand-therapy access shift practice strongly toward arthrodesis, which is cheaper, more durable, and technically more forgiving.
- Worldwide, TWA is concentrated in tertiary units with subspecialty hand-surgery training because low case volumes make maintaining proficiency difficult.
Controversies and Areas of Uncertainty
The evidence base for wrist arthroplasty remains predominantly Level III-IV with no high-quality randomised comparison against arthrodesis, leaving several genuine areas of debate.
1. Arthroplasty versus arthrodesis - the core unresolved question. Cavaliere and Chung concluded existing data did not support widespread TWA over fusion in the rheumatoid wrist. No adequately powered randomised trial has since overturned this. Proponents argue motion preservation is functionally important (especially with contralateral fusion or bilateral disease); sceptics counter that fusion delivers more reliable, durable pain relief. Current practice individualises the decision rather than applying a blanket rule.
2. Expanding indications to osteoarthritis and post-traumatic disease. Historically RA was the near-exclusive indication. Registry and cohort data (Norwegian register, ReMotion multicentre series) show increasing use in non-inflammatory disease, with comparable midterm survival in some series. Whether higher-demand OA and post-traumatic patients will erode long-term survivorship remains uncertain - the lower bone quality of RA paradoxically reduces mechanical loading.
3. Cause of late failure - loosening versus polyethylene wear. Distal/carpal component loosening is consistently the dominant failure mode, but its mechanism is contested. Newton et al implicate polyethylene wear-driven osteolysis on explant analysis, shifting attention from purely mechanical fixation toward bearing-surface durability and material science.
4. Radiographic lucency as a revision trigger. Sagerfors et al found radiographic loosening did not reliably predict revision, with high satisfaction despite lucent lines. This challenges the use of radiolucency alone to justify reoperation - clinical symptoms and progressive subsidence matter more than a single radiograph.
5. Implant selection and the absence of head-to-head trials. Marked implant-specific survival differences exist (e.g. second-generation Biax markedly inferior to Maestro/ReMotion), yet randomised comparisons between modern designs are lacking. Choice is driven by surgeon familiarity, registry signals, and revisability rather than Level I evidence.
Examiners reward candidates who acknowledge that TWA evidence is low-level and that fusion remains the durable benchmark, while articulating the specific scenarios (low-demand RA, bilateral disease, contralateral fusion) where motion preservation justifies the trade-off. Avoid dogmatism in either direction.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old woman with bilateral rheumatoid arthritis affecting both wrists presents with end-stage disease. Her left wrist was fused 3 years ago and she now has progressive pain in her right wrist. She works as a retired librarian and has low physical demands. Discuss your management options and justify your recommendation.”
“A 68-year-old man presents 4 years after total wrist arthroplasty with progressive wrist pain. X-rays show lucency around the distal component with subsidence. He has low demands and good bone stock. How do you manage this?”
“A 70-year-old woman with RA presents 2 years after TWA with inability to extend her thumb. On examination she has loss of thumb IP extension. X-rays show well-fixed components. What is your diagnosis and management?”
Indications
- Primary: RA with low demands (ideal candidate)
- Bilateral disease - motion preservation both sides
- Contralateral fusion - avoid bilateral fusion
- Elderly with limited activity expectations
Contraindications
- High-demand or manual labor - choose fusion
- Young age - durability concerns
- Poor bone stock - inadequate fixation
- Active infection - eradicate first
Key Numbers
- Motion: 40-60 degree arc preserved
- 5-year survival: 80%
- Distal loosening: 10-30%
- Revision rate: 15-25% at 10 years
Implant Types
- Universal 2 - most widely used, longest follow-up
- Maestro - bone-preserving, easier revision
- ReMotion - newest, anatomic design
- All third-generation ellipsoidal articulation
Complications
- Distal loosening - KEY failure mode (10-30%)
- Extensor tendon rupture (5-10%) - dorsal hardware
- Impingement (10-15%)
- Revision to fusion if failed
TWA vs Fusion
- TWA: motion preserved but less durable
- Fusion: no motion but 95% union
- Fusion revision rate 5-10% vs TWA 15-25%
- Fusion gold standard for high-demand
Evidence Base and Key Trials
TWA vs Arthrodesis - Landmark Systematic Review
- 18 TWA studies (~500 procedures) vs 20 fusion studies (over 800 procedures) in rheumatoid wrists
- Total wrist fusion provided more reliable pain relief than arthroplasty
- Complication and revision rates were higher for TWA than fusion
- Only 3 of 14 studies showed a mean active arc within the functional range; satisfaction high in both groups
Norwegian Arthroplasty Register - 189 Wrist Replacements
- 189 primary wrist replacements (Biax, Elos, Gibbon) over 16 years
- 5-year survival 78% (95% CI 70-85); 10-year survival 71% (95% CI 59-80)
- Biax 85% at 5 years vs Elos only 57% at 5 years - large implant-specific differences
- Survival inferior to hip/knee arthroplasty, but a failed TWA still leaves the option of a well-functioning arthrodesis
ReMotion International Multicentre Study (215 wrists)
- 215 ReMotion wrists across 7 centres (129 rheumatoid, 86 non-rheumatoid)
- Survival 96% (RA) and 92% (non-RA) at mean 4-year follow-up
- Mean postoperative flexion-extension arc 58 degrees (RA) and 63 degrees (non-RA)
- Implant loosening 4% (RA) and 3% (non-RA); only one dislocation in the whole series
Swedish Single-Centre Cohort - 219 Wrists, Implant-Specific Survival
- 219 wrists (189 patients), mean follow-up 7 years (range 2-13)
- 8-year survival 81% Biax, 94% ReMotion, 95% Maestro
- Radiographic loosening 26% Biax, 18% ReMotion, only 2% Maestro
- Radiographic loosening did not reliably correlate with revision; satisfaction high across all implants
Universal 2 - Long-Term (11-Year) Survival
- 26 Universal 2 wrists, mean follow-up 11 years
- 81% implant survival; 92% of patients satisfied
- 5 failures converted to fusion (distal component loosening in 3, recurrent dislocation 1, synovitis 1)
- Distal component loosening was the dominant mode of long-term failure
Universal 2 - Revision and Loosening Beyond 10 Years
- 78 rheumatoid wrists, longest follow-up 16 years; 29 wrists beyond 10 years
- Overall revision rate 22%; 10-year survivorship 78%
- Late revision commonly for periprosthetic loosening with pain and component subsidence
- Explant analysis showed polyethylene wear as the postulated driver of component loosening
References
-
Cavaliere CM, Chung KC. A systematic review of total wrist arthroplasty compared with total wrist arthrodesis for rheumatoid arthritis. Plast Reconstr Surg. 2008;122(3):813-825. PMID: 18766045. doi:10.1097/PRS.0b013e318180ece3
-
Krukhaug Y, Lie SA, Havelin LI, Furnes O, Hove LM. Results of 189 wrist replacements. A report from the Norwegian Arthroplasty Register. Acta Orthop. 2011;82(4):405-409. PMID: 21657971. doi:10.3109/17453674.2011.588858
-
Herzberg G, Boeckstyns M, Sorensen AI, et al. "ReMotion" total wrist arthroplasty: preliminary results of a prospective international multicenter study of 215 cases. J Wrist Surg. 2012;1(1):17-22. PMID: 23904975. doi:10.1055/s-0032-1323642
-
Sagerfors M, Gupta A, Brus O, Pettersson K. Total wrist arthroplasty: a single-center study of 219 cases with 5-year follow-up. J Hand Surg Am. 2015;40(12):2380-2387. PMID: 26612635. doi:10.1016/j.jhsa.2015.09.016
-
Zijlker HJA, Ritt MJPF, IJsselstein CB. Long-term results of Universal 2 total wrist arthroplasty. J Wrist Surg. 2019;8(4):317-320. PMID: 31404363. doi:10.1055/s-0039-1685469
-
Newton A, Kandemir G, Joyce T, Murali R, Hayton M, Talwalkar S, Trail I. Long-term outcomes of the Universal 2 total wrist replacement: revision and loosening at 10 years and beyond. J Hand Surg Eur Vol. 2023;48(7):641-647. PMID: 36927271. doi:10.1177/17531934231160380
-
Yeoh D, Tourret L. Total wrist arthroplasty: a systematic review of the evidence from the last 5 years. J Hand Surg Eur Vol. 2014;40(5):458-468. PMID: 24963082. doi:10.1177/1753193414539796
-
Tham A, Ross A, Wright J, et al. Long-term outcomes of the Universal 2 total wrist arthroplasty. J Orthop. 2024;61:103-108. PMID: 40051785. doi:10.1016/j.jor.2024.10.004